Weight Gain and Increased Body Mass Index in Patients with Hepatitis C after Eradication Using Direct-Acting Antiviral Therapy in Taiwan

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
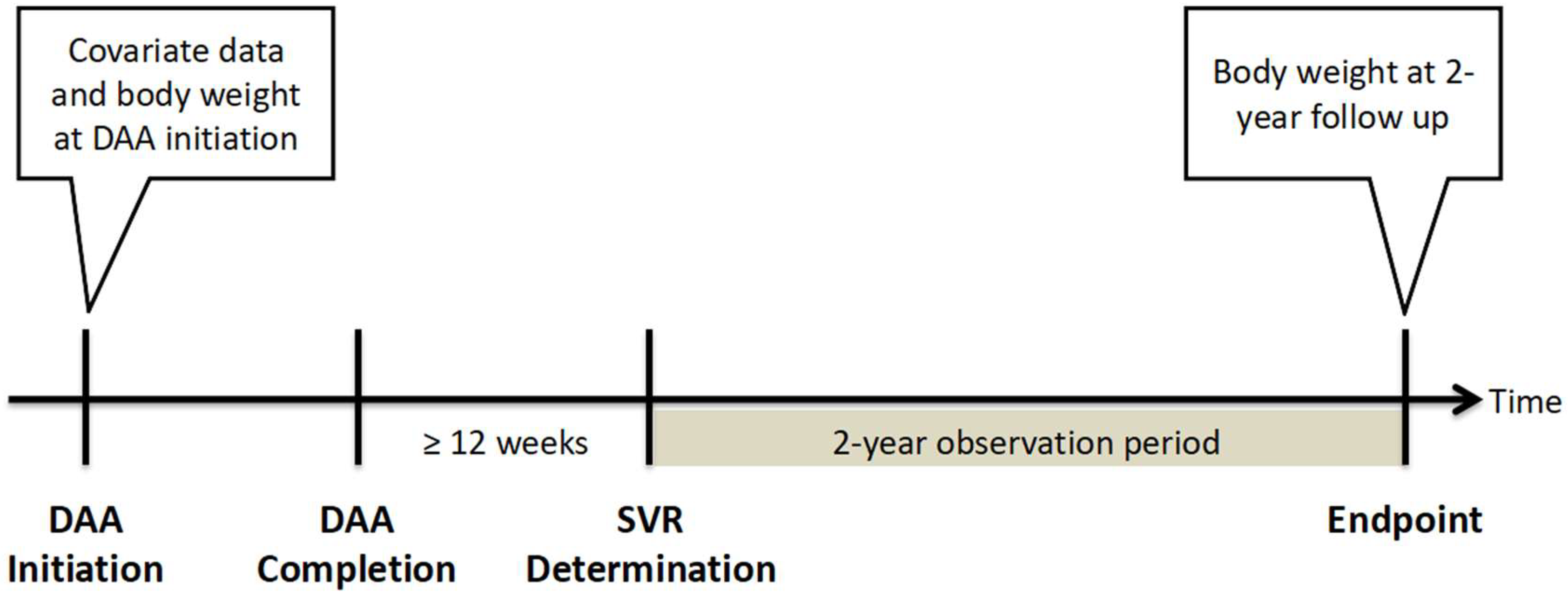
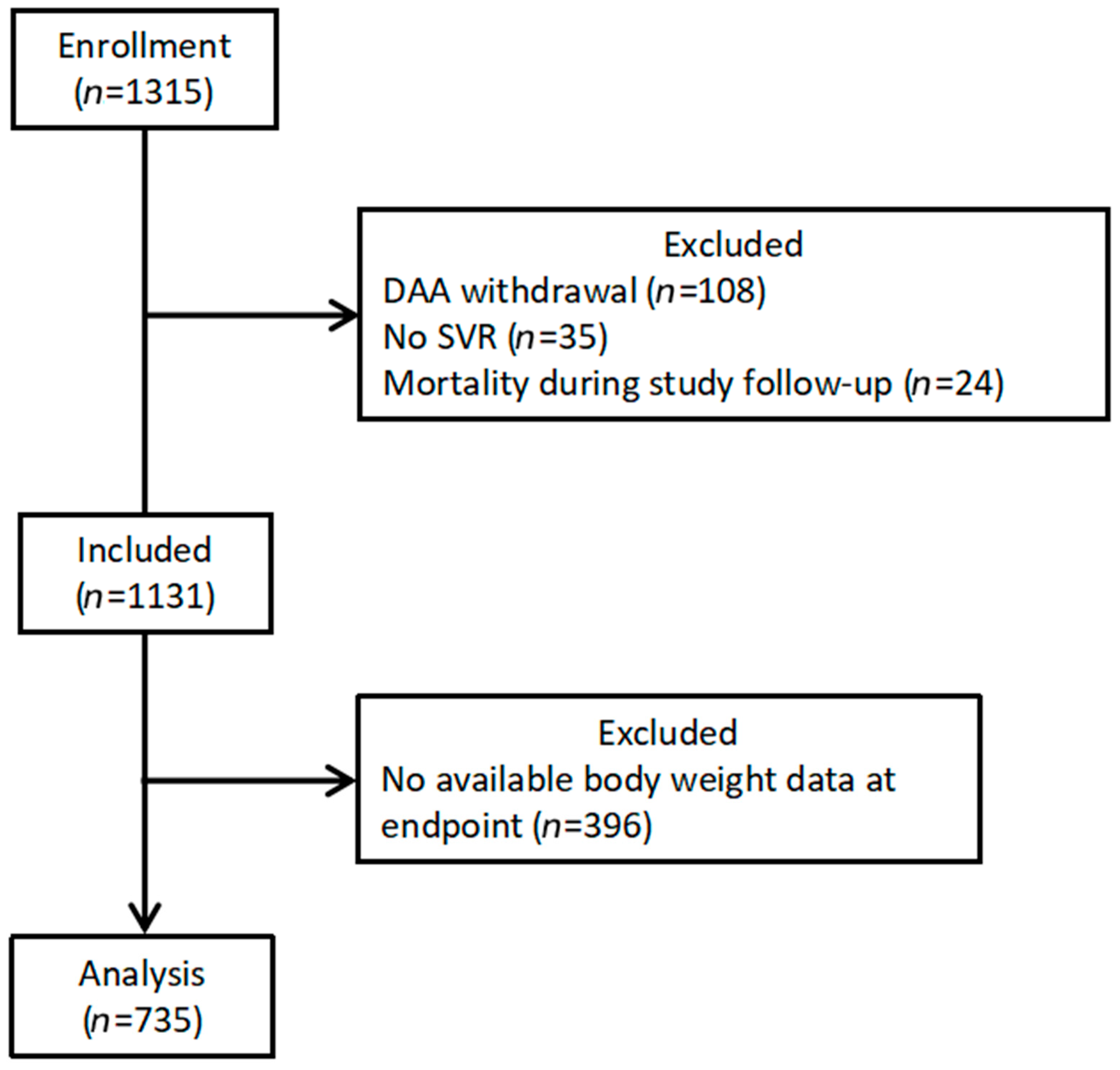
2.1. Study Design and Patient Population
2.2. Assessment of Clinical Parameters
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
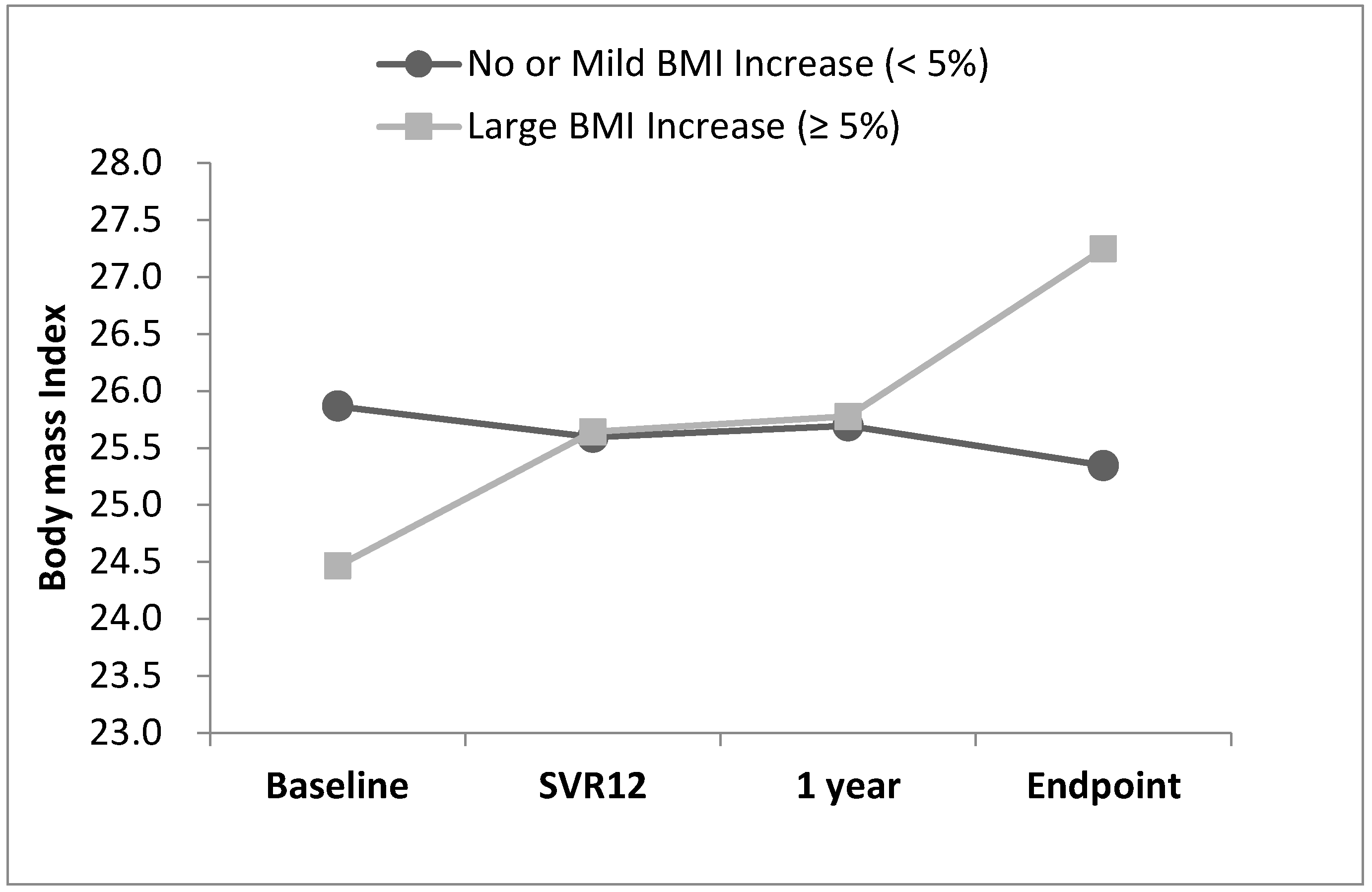
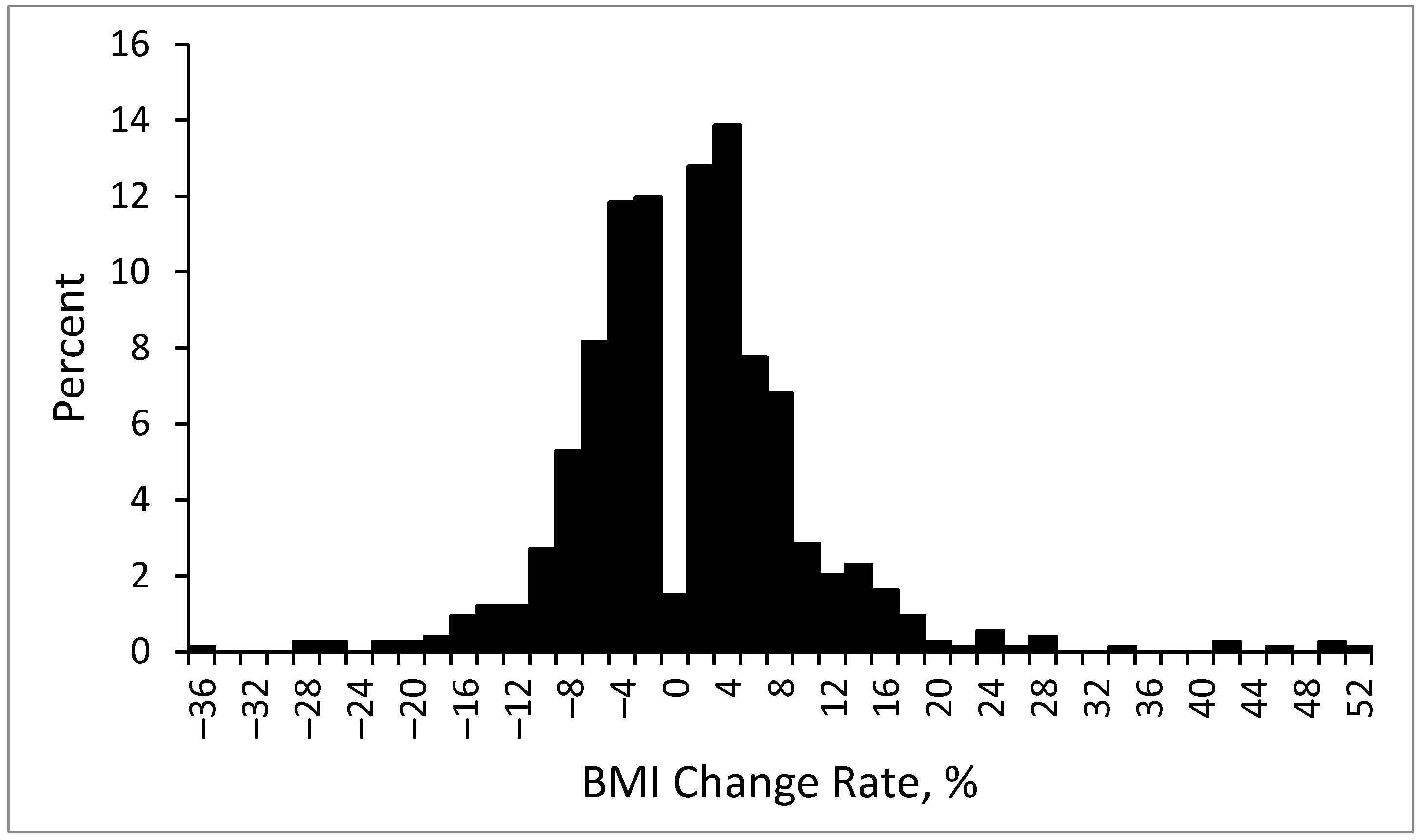
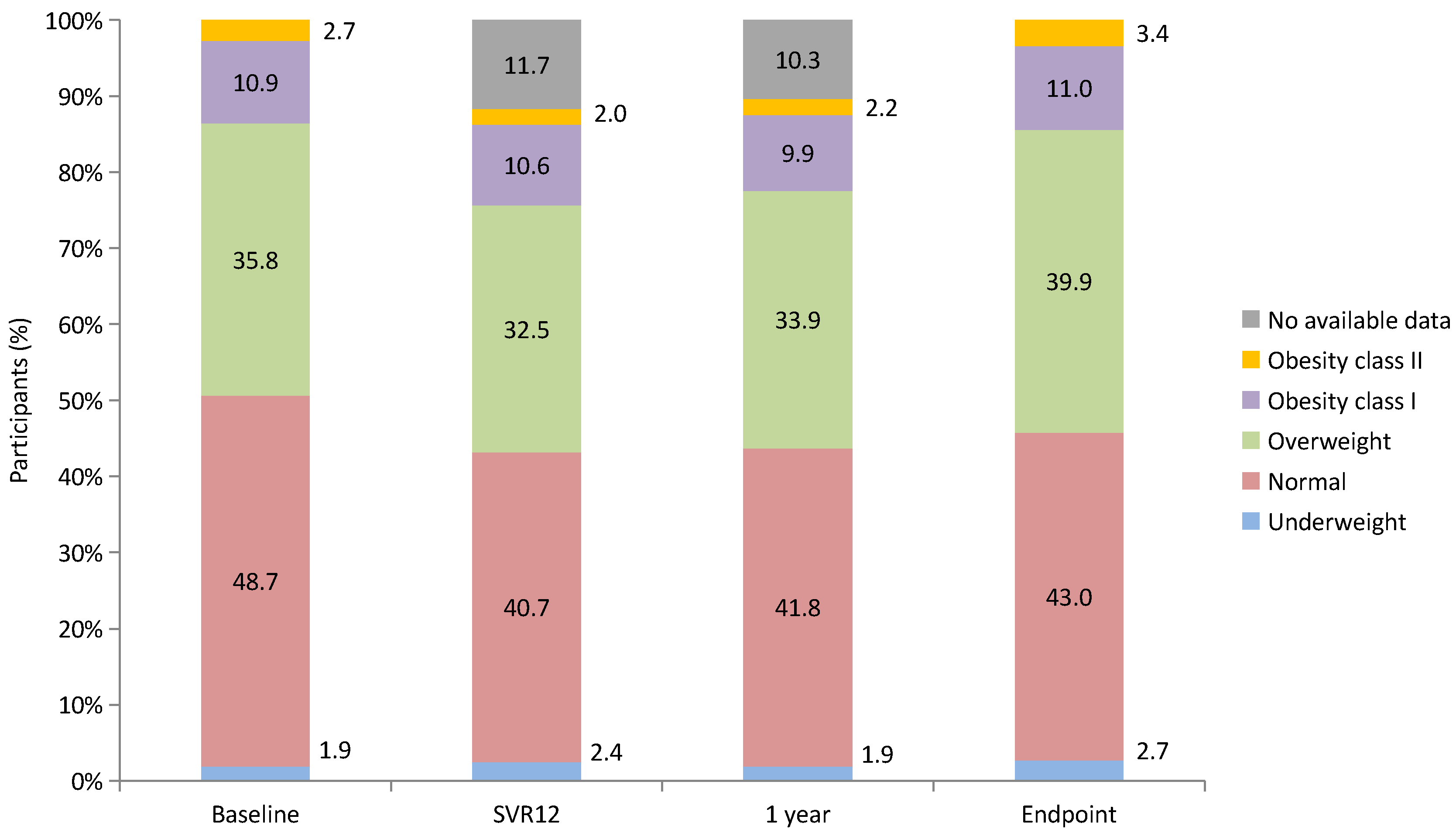
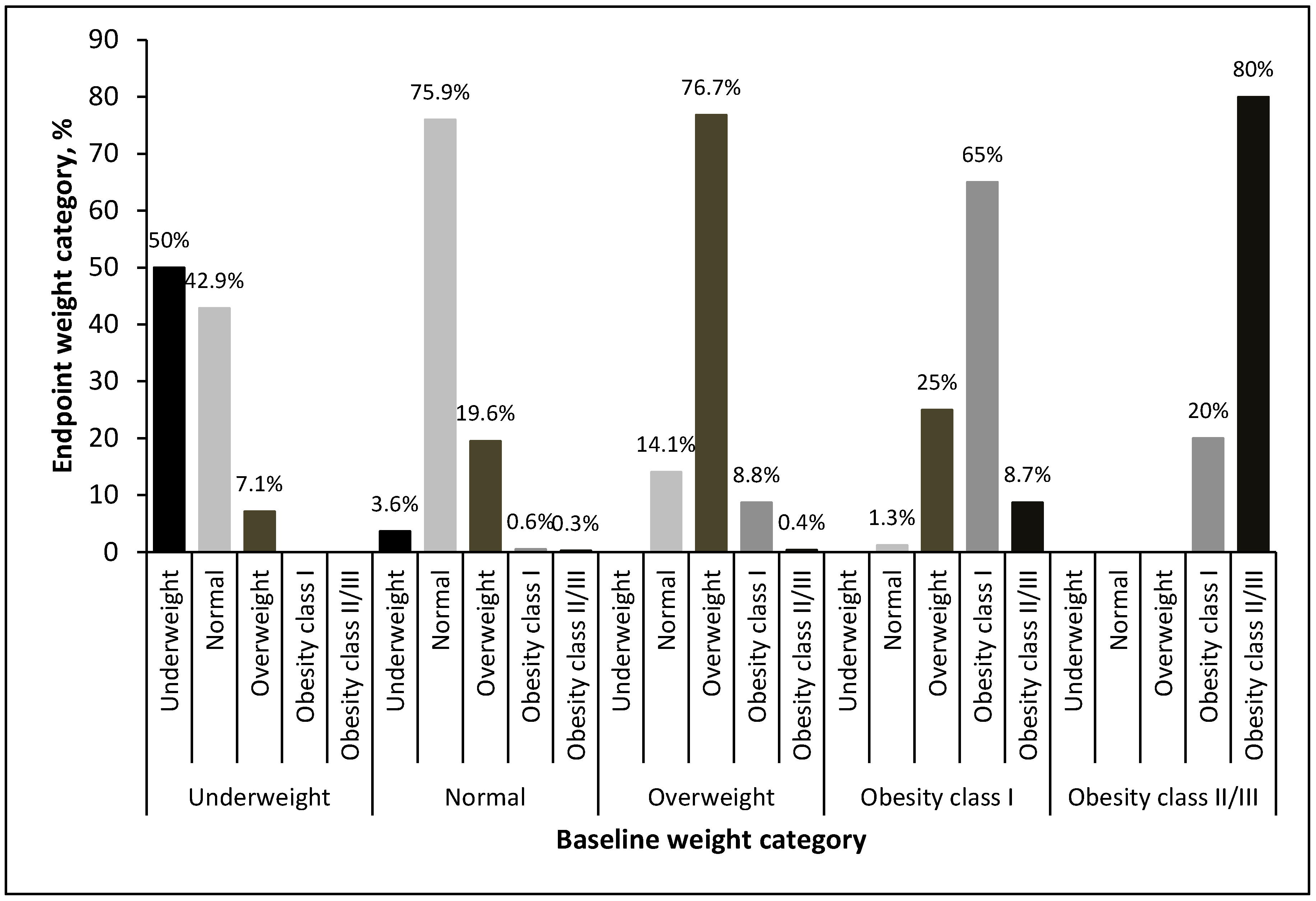
3.2. BMI Change
3.3. Multivariate Regression Analysis for Notable BMI Increase
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohanty, A.; Salameh, S.; Butt, A.A. Impact of direct acting antiviral agent therapy upon extrahepatic manifestations of hepatitis C virus infection. Curr. HIV/AIDS Rep. 2019, 16, 389–394. [Google Scholar] [CrossRef]
- Lanini, S.; Scognamiglio, P.; Pisapia, R.; Minosse, C.; Agresta, A.; Ippolito, G. Recovery of metabolic impairment in patients who cleared chronic hepatitis C infection after direct-acting antiviral therapy. Int. J. Antimicrob. Agents 2019, 53, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Sandmann, L.; Schulte, B.; Manns, M.P.; Maasoumy, B. Treatment of chronic hepatitis C: Efficacy, side effects and complications. Visc. Med. 2019, 35, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Miyanari, Y.; Atsuzawa, K.; Usuda, N.; Watashi, K.; Hishiki, T.; Zayas, M.; Bartenschlager, R.; Wakita, T.; Hijikata, M.; Shimotohno, K. The lipid droplet is an important organelle for hepatitis C virus production. Nat. Cell Biol. 2007, 9, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.V.; Cortez-Pinto, H. Insulin resistance and steatosis in chronic hepatitis C. Ann. Hepatol. 2009, 8, S67–S75. [Google Scholar] [CrossRef] [PubMed]
- Vidali, M.; Tripodi, M.-F.; Ivaldi, A.; Zampino, R.; Occhino, G.; Restivo, L.; Sutti, S.; Marrone, A.; Ruggiero, G.; Albano, E.; et al. Interplay between oxidative stress and hepatic steatosis in the progression of chronic hepatitis C. J. Hepatol. 2008, 48, 399–406. [Google Scholar] [CrossRef]
- Moriishi, K.; Mochizuki, R.; Moriya, K.; Miyamoto, H.; Mori, Y.; Abe, T.; Murata, S.; Tanaka, K.; Miyamura, T.; Suzuki, T.; et al. Critical role of PA28γ in hepatitis C virus-associated steatogenesis and hepatocarcinogenesis. Proc. Natl. Acad. Sci. USA 2007, 104, 1661–1666. [Google Scholar] [CrossRef]
- Kahn, B.B.; Flier, J.S. Obesity and insulin resistance. J. Clin. Investig. 2000, 106, 473–481. [Google Scholar] [CrossRef]
- El Kassas, M.; Alboraie, M.; Naguib, M.; Omar, H.; El Tahan, A.; Moaz, I.; Abdellah, M.; Ezzat, S.; Wifi, M.-N.; Sherief, A.F.; et al. A significant upsurge of body mass index in patients with chronic hepatitis C successfully treated with direct-acting antiviral regimens. Turk. J. Gastroenterol. 2019, 30, 708–713. [Google Scholar] [CrossRef]
- Do, A.; Esserman, D.A.; Krishnan, S.; Lim, J.K.; Taddei, T.H.; Hauser, R.G.; Tate, J.P.; Re, V.L.; Justice, A.C. Excess weight gain after cure of hepatitis C infection with direct-acting antivirals. J. Gen. Intern. Med. 2020, 35, 2025–2034. [Google Scholar] [CrossRef]
- Schlevogt, B.; Boeker, K.H.W.; Mauss, S.; Klinker, H.; Heyne, R.; Link, R.; Simon, K.-G.; Sarrazin, C.; Serfert, Y.; Manns, M.P.; et al. Weight Gain after Interferon-Free Treatment of Chronic Hepatitis C—Results from the German Hepatitis C-Registry (DHC-R). Biomedicines 2021, 9, 1495. [Google Scholar] [CrossRef] [PubMed]
- Nkwocha, C.L.; Carter, P.S.; Blair, S.; Blackwell, J.M.; Fasanmi, E.O. Understanding the effect of direct-acting antiviral therapy on weight in patients with chronic hepatitis C. Antivir. Ther. 2022, 27, 13596535221115253. [Google Scholar] [CrossRef]
- Dutton, G.R.; Kim, Y.; Jacobs Jr, D.R.; Li, X.; Loria, C.M.; Reis, J.P.; Carnethon, M.; Durant, N.H.; Gordon-Larsen, P.; Shikany, J.M.; et al. 25-year weight gain in a racially balanced sample of US adults: The CARDIA study. Obesity 2016, 24, 1962–1968. [Google Scholar] [CrossRef]
- Everson, S.; Glodberg, D.E.; Helmrich, S.P.; Lakka, T.A.; Lynch, J.W.; Kaplan, G.A.; Salonen, J.T. Weight gain and the risk of developing insulin resistance syndrome. Diabetes Care 1998, 21, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Chen, J.D.; Chen, P.C. Excessive 5-year weight gain predicts metabolic syndrome development in healthy middle-aged adults. World J. Diabetes 2011, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Seyam, M.S.; Freshwater, D.A.; O’Donnell, K.; Mutimer, D.J. Weight loss during pegylated interferon and ribavirin treatment of chronic hepatitis C. J. Viral Hepat. 2005, 12, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Zampino, R.; Marrone, A.; Restivo, L.; Guerrera, B.; Sellitto, A.; Rinaldi, L.; Romano, C.; E Adinolfi, L. Chronic HCV infection and inflammation: Clinical impact on hepatic and extra-hepatic manifestations. World J. Hepatol. 2013, 5, 528–540. [Google Scholar] [CrossRef]
- Foster, G.R.; Goldin, R.D.; Thomas, H.C. Chronic hepatitis C virus infection causes a significant reduction in quality of life in the absence of cirrhosis. Hepatology 1998, 27, 209–212. [Google Scholar] [CrossRef]
- Musialik, J.; Suchecka, W.; Klimacka-Nawrot, E.; Petelenz, M.; Hartman, M.; Błońska-Fajfrowska, B. Taste and appetite disorders of chronic hepatitis C patients. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1400–1405. [Google Scholar] [CrossRef]
- Kumar, S.; Samaras, K. The impact of weight gain during HIV treatment on risk of pre-diabetes, diabetes mellitus, cardiovascular disease, and mortality. Front. Endocrinol. 2018, 9, 705. [Google Scholar] [CrossRef]
- Erlandson, K.M.; Carter, C.C.; Melbourne, K.; Brown, T.T.; Cohen, C.; Das, M.; Esser, S.; Huang, H.; Koethe, J.R.; Martin, H.; et al. Weight change following antiretroviral therapy switch in people with viral suppression: Pooled data from randomized clinical trials. Clin. Infect. Dis. 2021, 73, 1440–1451. [Google Scholar] [CrossRef] [PubMed]
- Alam, I.; Ali, I.; Ali, S.; Alam, I.; Naseem, F.; Naseem, Z. Impact of combination interferon therapy on the body weight, body fat and lean body mass of chronic HCV infected patients. J. Antivir. Antiretrovir. 2013, 6, 1–5. [Google Scholar]
- Chen, Y.-Y.; Fang, W.-H.; Wang, C.-C.; Kao, T.-W.; Chang, Y.-W.; Yang, H.-F.; Wu, C.-J.; Sun, Y.-S.; Chen, W.-L. Increased body fat percentage in patients with hepatitis B and C virus infection. PLoS ONE 2018, 13, e0200164. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, R.; Iwasa, M.; Hara, N.; Tamai, Y.; Yoshikawa, K.; Ogura, S.; Tanaka, H.; Eguchi, A.; Yamamoto, N.; Kobayashi, Y.; et al. Changes in liver function and body composition by direct-acting antiviral therapy for hepatitis C virus infection. Hepatol. Res. 2018, 48, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Ghoneim, S.; Butt, M.U.; Trujillo, S.; Asaad, I. FIB-4 regression with direct-acting antiviral therapy in patients with hepatitis C infection: A safety-net hospital experience. Front. Med. 2020, 7, 359. [Google Scholar] [CrossRef]
- Lau, B.; Sharrett, A.R.; Kingsley, L.A.; Post, W.; Palella, F.J.; Visscher, B.; Gange, S.J. C-reactive protein is a marker for human immunodeficiency virus disease progression. Arch. Intern. Med. 2006, 166, 64–70. [Google Scholar] [CrossRef]
- Mave, V.; Erlandson, K.M.; Gupte, N.; Balagopal, A.; Asmuth, D.M.; Campbell, T.B.; Smeaton, L.; Kumarasamy, N.; Hakim, J.; Santos, B.; et al. Inflammation and change in body weight with antiretroviral therapy initiation in a multinational cohort of HIV-infected adults. J. Infect. Dis. 2016, 214, 65–72. [Google Scholar] [CrossRef]
- Wada, R.; Tekin, E. Body composition and wages. Econ. Hum. Biol. 2010, 8, 242–254. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients (n = 735) | No or Mild BMI Increase (<5%) | n | Large BMI Increase (≥5%) | n | p Value | |
|---|---|---|---|---|---|---|
| Age, year | 66.1 (11.8) | 66.3 (11.5) | 572 | 65.6 (12.7) | 163 | 0.525 |
| Male gender, n (%) | 336 (45.7%) | 258 (45.1%) | 572 | 78 (47.9%) | 163 | 0.534 |
| Body weight, kg | 64.7 (12.4) | 65.4 (12.1) | 572 | 62.3 (13.0) | 163 | 0.005 |
| BMI, kg/m2 | 25.6 (4.1) | 25.9 (4.0) | 572 | 24.5 (4.0) | 163 | <0.001 |
| Weight category, n (%) | 572 | 163 | ||||
| Underweight: <18.5 kg/m2 | 14 (1.9%) | 9 (1.6%) | 5 (3.1%) | 0.208 | ||
| Normal: 18.5–24.9 kg/m2 | 358 (48.7%) | 257 (44.9%) | 101 (62.0%) | <0.001 | ||
| Overweight: 25.0–29.9 kg/m2 | 263 (35.8%) | 218 (38.1%) | 45 (27.6%) | 0.014 | ||
| Obesity class I: 30.0–34.9 kg/m2 | 80 (10.9%) | 72 (12.6%) | 8 (4.9%) | 0.004 | ||
| Obesity class II and III: >35.0 kg/m2 | 20 (2.7%) | 16 (2.8%) | 4 (2.5%) | 1.000 | ||
| Current smoking, n (%) | 138 (18.8%) | 105 (18.4%) | 572 | 33 (20.2%) | 163 | 0.586 |
| Diabetes mellitus, n (%) | 199 (27.1%) | 148 (25.9%) | 572 | 51 (31.3%) | 163 | 0.170 |
| Hypertension, n (%) | 367 (49.9%) | 284 (49.7%) | 572 | 83 (50.9%) | 163 | 0.775 |
| Dyslipidemia, n (%) | 153 (20.8%) | 114 (19.9%) | 572 | 39 (23.9%) | 163 | 0.268 |
| HBsAg positive, n (%) | 98 (13.3%) | 79 (13.8%) | 572 | 19 (11.7%) | 163 | 0.475 |
| HCC, n (%) | 50 (6.8%) | 41 (7.2%) | 572 | 9 (5.5%) | 163 | 0.597 |
| Prior IFN, n (%) | 155 (21.1%) | 121 (21.2%) | 254 | 34 (20.9%) | 65 | 0.501 |
| AST, U/L | 58.0 (46.5) | 55.7 (45.7) | 572 | 66.0 (48.6) | 163 | 0.013 |
| ALT, U/L | 72.1 (68.7) | 70.5 (71.1) | 572 | 77.8 (59.3) | 163 | 0.228 |
| Albumin, g/dL | 4.3 (0.4) | 4.3 (0.4) | 572 | 4.2 (0.4) | 163 | 0.030 |
| Albumin ≤ 3.5 g/dL, n (%) | 23 (3.1%) | 12 (2.1%) | 572 | 11 (6.7%) | 163 | 0.003 |
| Total bilirubin, mg/dL | 0.8 (0.4) | 0.7 (0.4) | 572 | 0.8 (0.6) | 163 | 0.173 |
| Platelet, 103/μL | 178.0 (65.6) | 182.0 (67.0) | 572 | 163.8 (58.5) | 163 | 0.002 |
| PT INR | 1.0 (0.1) | 1.0 (0.1) | 572 | 1.0 (0.2) | 163 | 0.040 |
| FIB-4 score | 3.17 (2.45) | 3.03 (2.36) | 572 | 3.68 (2.74) | 163 | 0.006 |
| FIB-4 score, n (%) | 572 | 163 | ||||
| <1.45 | 170 (23.1%) | 142 (24.8%) | 28 (17.2%) | 0.041 | ||
| 1.45–3.25 | 306 (41.6%) | 246 (43.0%) | 60 (36.8%) | 0.157 | ||
| >3.25 | 259 (35.2%) | 184 (32.2%) | 75 (46.0%) | 0.001 | ||
| FIB-4 score reduction * | 0.8 (1.7) | 0.6 (1.6) | 566 | 1.1 (1.8) | 161 | 0.002 |
| AFP, ng/mL | 8.0 (28.3) | 7.4 (26.8) | 572 | 10.3 (33.0) | 163 | 0.247 |
| HCV-RNA, 106 IU/mL | 10.9 (208.4) | 13.5 (236.2) | 572 | 2.0 (2.7) | 163 | 0.538 |
| HCV-RNA, log-transformed | 6.0 (1.0) | 6.0 (0.9) | 572 | 5.7 (1.0) | 163 | <0.001 |
| HCV genotype, n (%) | 572 | 163 | ||||
| 1a | 9 (1.2%) | 6 (1.0%) | 3 (1.8%) | 0.423 | ||
| 1b | 493 (67.1%) | 383 (67.0%) | 110 (67.5%) | 0.900 | ||
| 2 | 201 (27.3%) | 162 (28.3%) | 39 (23.9%) | 0.267 | ||
| 3 | 2 (0.3%) | 1 (0.2%) | 1 (0.6%) | 0.395 | ||
| 6 | 8 (1.1%) | 7 (1.2%) | 1 (0.6%) | 0.692 | ||
| mixed | 22 (3.0%) | 13 (2.3%) | 9 (5.5%) | 0.039 | ||
| DAAs, n (%) | 572 | 163 | ||||
| DCV/ASV | 41 (5.6%) | 29 (5.1%) | 12 (7.4%) | 0.261 | ||
| ProD | 98 (13.3%) | 76 (13.3%) | 22 (13.5%) | 0.944 | ||
| Zepatier | 271 (36.9%) | 220 (38.5%) | 51 (31.3%) | 0.094 | ||
| Maviret | 105 (14.3%) | 81 (14.2%) | 24 (14.7%) | 0.856 | ||
| SOF-based | 220 (29.9%) | 166 (29.0%) | 54 (33.1%) | 0.312 | ||
| Ribavirin use, n (%) | 84 (11.4%) | 61 (10.7%) | 572 | 23 (14.1%) | 163 | 0.222 |
| Hemoglobin, g/dL | 13.8 (1.7) | 13.9 (1.7) | 572 | 13.6 (1.8) | 163 | 0.034 |
| Fasting plasma glucose, mg/dL | 115.4 (39.66) | 113.9 (39.4) | 318 | 120.7 (40.4) | 90 | 0.149 |
| Creatinine, mg/dL | 0.91 (0.36) | 0.91 (0.37) | 572 | 0.89 (0.29) | 163 | 0.493 |
| eGFR, mL/min/1.73 m2 | 84.35 (23.99) | 83.88 (23.94) | 572 | 85.99 (24.18) | 163 | 0.323 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variables | OR (95%CI) | p Value | OR (95%CI) | p Value |
| Age (year) | 0.995 (0.981–1.010) | 0.525 | 0.979 (0.963–0.996) | 0.013 |
| Gender (Male vs. Female) | 1.117 (0.788–1.583) | 0.535 | 1.120 (0.743–1.689) | 0.587 |
| Body weight (kg) | 0.979 (0.964–0.993) | 0.005 | ||
| BMI (kg/m2) | 0.910 (0.868–0.955) | <0.001 | 0.907 (0.863–0.954) | <0.001 |
| Weight category | ||||
| Underweight: <18.5 kg/m2 | 1.414 (0.463–4.320) | 0.544 | ||
| Normal: 18.5–24.9 kg/m2 | Reference | |||
| Overweight: 25.0–29.9 kg/m2 | 0.525 (0.354–0.780) | 0.001 | ||
| Obesity class I: 30.0–34.9 kg/m2 | 0.283 (0.131–0.608) | 0.001 | ||
| Obesity class II and III: ≧35.0 kg/m2 | 0.636 (0.208–1.949) | 0.428 | ||
| Current smoking (Yes vs. No) | 1.129 (0.729–1.747) | 0.586 | ||
| Diabetes Mellitus (Yes vs. No) | 1.305 (0.892–1.908) | 0.171 | 1.092 (0.693–1.720) | 0.0704 |
| Hypertension (Yes vs. No) | 1.052 (0.743–1.490) | 0.775 | 1.317 (0.867–2.002) | 0.197 |
| Dyslipidemia (Yes vs. No) | 1.264 (0.835–1.912) | 0.268 | 1.355 (0.841–2.184) | 0.212 |
| HBsAg positive (Yes vs. No) | 0.823 (0.483–1.405) | 0.476 | ||
| HCC (Yes vs. No) | 0.757 (0.360–1.592) | 0.463 | ||
| AST (U/L) | 1.004 (1.001–1.008) | 0.014 | ||
| ALT (U/L) | 1.001 (0.999–1.004) | 0.231 | ||
| Albumin (g/dL) | 0.582 (0.373–0.907) | 0.017 | 0.819 (0.491–1.367) | 0.445 |
| Total bilirubin (mg/dL) | 1.280 (0.886–1.849) | 0.189 | ||
| Platelet (103/μL) | 0.995 (0.993–0.998) | 0.002 | 0.996 (0.993–0.999) | 0.022 |
| FIB-4 score (Baseline) | 1.102 (1.033–1.176) | 0.003 | ||
| <1.45 | Reference | |||
| 1.45–3.25 | 1.237 (0.755–2.027) | 0.399 | ||
| >3.25 | 2.067 (1.271–3.361) | 0.003 | ||
| FIB-4 score (SVR12) | 1.054 (0.966–1.149) | 0.236 | ||
| <1.45 | Reference | |||
| 1.45–3.25 | 0.847 (0.561–1.281) | 0.432 | ||
| >3.25 | 1.390 (0.847–2.282) | 0.193 | ||
| FIB-4 score reduction a | 1.189 (1.072–1.319) | 0.001 | 1.168 (1.047–1.304) | 0.006 |
| AFP (ng/mL) | 1.003 (0.998–1.008) | 0.283 | ||
| HCV-RNA (106 IU/mL) | 0.892 (0.837–0.950) | <0.001 | 1.000 (1.000–1.000) | 0.006 |
| HCV genotype | ||||
| 1a | NA b | |||
| 1b | Reference | |||
| 2 | 0.838 (0.557–1.262) | 0.398 | ||
| 3 | NA b | |||
| 6 | NA b | |||
| mixed | NA b | |||
| DAAs | ||||
| DCV/ASV | 1.272 (0.607–2.665) | 0.524 | ||
| ProD | 0.890 (0.506–1.566) | 0.686 | ||
| Zepatier | 0.713 (0.462–1.098) | 0.125 | ||
| GP | 0.911(0.526–1.578) | 0.739 | ||
| SOF-based | Reference | |||
| SOF-based (Yes vs. No) | 1.212 (0.835–1.759) | 0.313 | ||
| Ribavirin use (Yes vs. No) | 1.376 (0.823–2.303) | 0.224 | ||
| Hemoglobin (g/dL) | 0.896 (0.809–0.992) | 0.035 | 0.908 (0.801–1.030) | 0.133 |
| Fasting plasma glucose (mg/dL) | 1.004 (0.999–1.009) | 0.154 | ||
| HbA1c (%) | 1.036 (0.858–1.251) | 0.713 | ||
| Creatinine (mg/dL) | 0.831 (0.490–1.411) | 0.494 | ||
| eGFR (mL/min/1.73 m2) | 1.004 (0.996–1.011) | 0.323 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Hsieh, Y.-Y.; Chen, W.-M.; Shen, C.-H.; Wei, K.-L.; Chang, K.-C.; Ding, Y.-J.; Lu, S.-N.; Hung, C.-H.; Chang, T.-S. Weight Gain and Increased Body Mass Index in Patients with Hepatitis C after Eradication Using Direct-Acting Antiviral Therapy in Taiwan. Diagnostics 2024, 14, 213. https://doi.org/10.3390/diagnostics14020213
Chen C-H, Hsieh Y-Y, Chen W-M, Shen C-H, Wei K-L, Chang K-C, Ding Y-J, Lu S-N, Hung C-H, Chang T-S. Weight Gain and Increased Body Mass Index in Patients with Hepatitis C after Eradication Using Direct-Acting Antiviral Therapy in Taiwan. Diagnostics. 2024; 14(2):213. https://doi.org/10.3390/diagnostics14020213
Chicago/Turabian StyleChen, Chun-Hsien, Yung-Yu Hsieh, Wei-Ming Chen, Chien-Heng Shen, Kuo-Liang Wei, Kao-Chi Chang, Yuan-Jie Ding, Sheng-Nan Lu, Chao-Hung Hung, and Te-Sheng Chang. 2024. "Weight Gain and Increased Body Mass Index in Patients with Hepatitis C after Eradication Using Direct-Acting Antiviral Therapy in Taiwan" Diagnostics 14, no. 2: 213. https://doi.org/10.3390/diagnostics14020213
APA StyleChen, C. -H., Hsieh, Y. -Y., Chen, W. -M., Shen, C. -H., Wei, K. -L., Chang, K. -C., Ding, Y. -J., Lu, S. -N., Hung, C. -H., & Chang, T. -S. (2024). Weight Gain and Increased Body Mass Index in Patients with Hepatitis C after Eradication Using Direct-Acting Antiviral Therapy in Taiwan. Diagnostics, 14(2), 213. https://doi.org/10.3390/diagnostics14020213