
P16-CD8-Ki67 Triple Algorithm for Prediction of CDKN2A Mutations in Patients with Multiple Primary and Familial Melanoma


 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
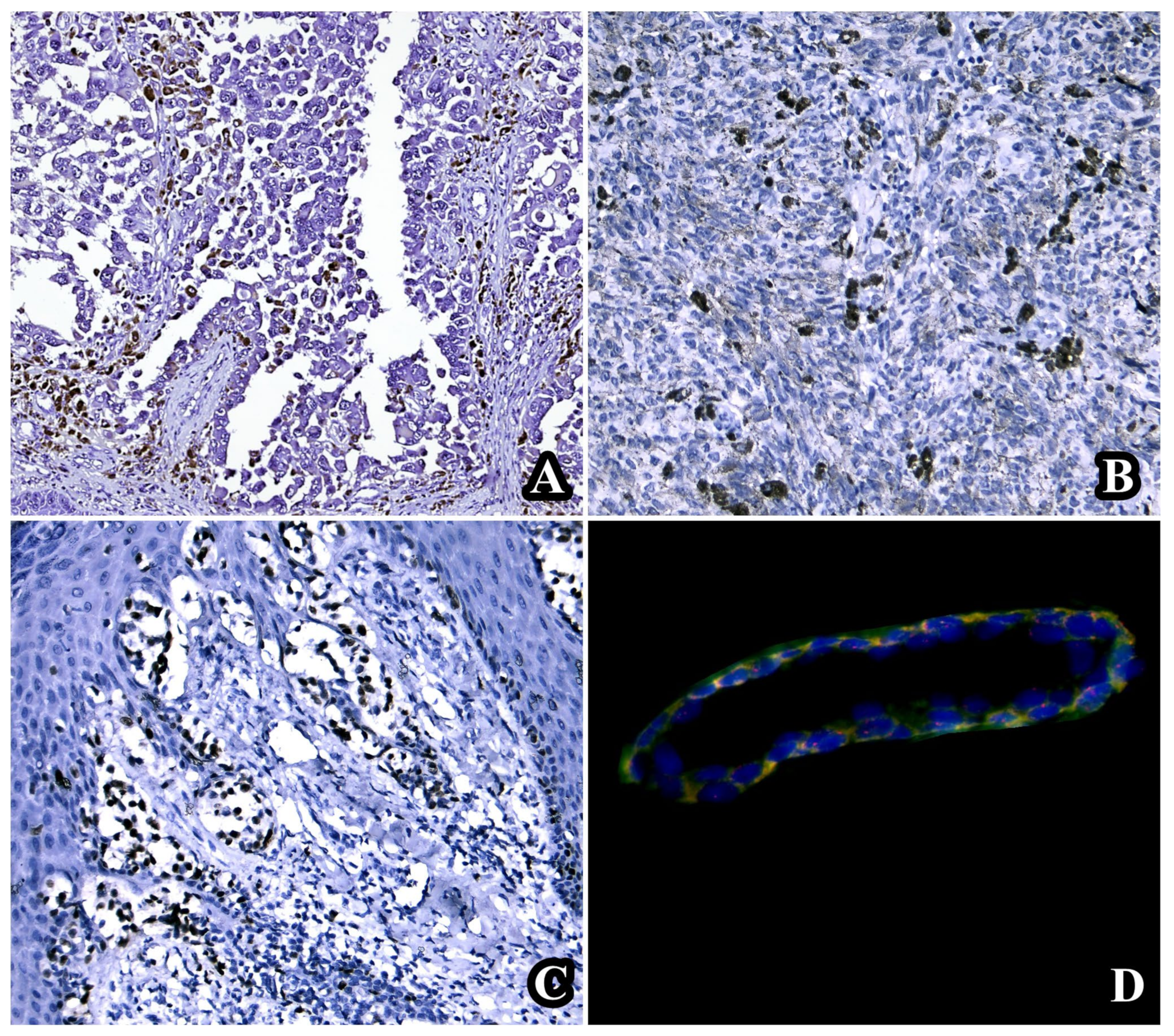
3.1. Individual Evaluation of p16, CD8, and Ki67
3.2. Assessment of Clinical and Genetic Correlations in the Analyzed Cohort
3.3. The Triple p16-CD8-Ki67 Scoring Algorithm for the Distinction between Familial and Multiple Primary Melanomas with and without CDKN2A Mutations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karimkhani, C.; Green, A.C.; Nijsten, T.; Weinstock, M.A.; Dellavalle, R.P.; Naghavi, M.; Fitzmaurice, C. The global burden of melanoma: Results from the Global Burden of Disease Study 2015. Br. J. Dermatol. 2017, 177, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Wehner, M.R.; Matrisian, L.M.; Nead, K.T. Estimated Projection of US Cancer Incidence and Death to 2040. JAMA Netw. Open 2021, 4, e214708. [Google Scholar] [CrossRef] [PubMed]
- Kamb, A.; Gruis, N.A.; Weaver-Feldhaus, J.; Liu, Q.; Harshman, K.; Tavtigian, S.V.; Stockert, E.; Day, R.S.; Johnson, B.E.; Skolnick, M.H. A cell cycle regulator potentially involved in genesis of many tumor types. Science 1994, 264, 436–440. [Google Scholar] [CrossRef]
- Nobori, T.; Miura, K.; Wu, D.J.; Lois, A.; Takabayashi, K.; Carson, D.A. Deletions of the cyclin-dependent kinase-4 inhibitor gene in multiple human cancers. Nature 1994, 368, 753–756. [Google Scholar] [CrossRef] [PubMed]
- Bartkova, J.; Lukas, J.; Guldberg, P.; Alsner, J.; Kirkin, A.F.; Zeuthen, J.; Bartek, J. The p16-cyclin D/Cdk4-pRb pathway as a functional unit frequently altered in melanoma pathogenesis. Cancer Res. 1996, 56, 5475–5483. [Google Scholar] [PubMed]
- Zeng, H.; Jorapur, A.; Shain, A.H.; Lang, U.E.; Torres, R.; Zhang, Y.; McNeal, A.S.; Botton, T.; Lin, J.; Donne, M.; et al. Bi-allelic Loss of CDKN2A Initiates Melanoma Invasion via BRN2 Activation. Cancer Cell 2018, 34, 56–68.e9. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, S.S.; Pramio, D.T.; Kashiwabara, A.Y.; Pennacchi, P.C.; Maria-Engler, S.S.; Achatz, M.I.; Campos, A.H.J.F.M.; Duprat, J.P.; Rosenberg, C.; Carraro, D.M.; et al. DNA Methylation Levels of Melanoma Risk Genes Are Associated with Clinical Characteristics of Melanoma Patients. BioMed Res. Int. 2015, 2015, 376423. [Google Scholar] [CrossRef] [PubMed]
- Hussussian, C.J.; Struewing, J.P.; Goldstein, A.M.; Higgins, P.A.T.; Ally, D.S.; Sheahan, M.D.; Clark, W.H.; Tucker, M.A.; Dracopoli, N.C. Germline p16 mutations in familial melanoma. Nat. Genet. 1994, 8, 15–21. [Google Scholar] [CrossRef]
- Healy, E.; Sikkink, S.; Rees, J.L. Infrequent mutation of p16INK4 in sporadic melanoma. J. Investig. Dermatol. 1996, 107, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Shain, A.H.; Bastian, B.C. From melanocytes to melanomas. Nat. Rev. Cancer 2016, 16, 345–358, Correction in Nat. Rev. Cancer 2020, 20, 355. [Google Scholar] [CrossRef]
- Davis, L.E.; Shalin, S.C.; Tackett, A.J. Current state of melanoma diagnosis and treatment. Cancer Biol. Ther. 2019, 20, 1366–1379. [Google Scholar] [CrossRef]
- Mehnert, J.M.; Kluger, H.M. Driver mutations in melanoma: Lessons learned from bench-to-bedside studies. Curr. Oncol. Rep. 2012, 14, 449–457. [Google Scholar] [CrossRef]
- Galon, J.; Bruni, D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat. Rev. Drug Discov. 2019, 18, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Straume, O.; Akslen, L.A. Alterations and prognostic significance of p16 and p53 protein expression in subgroups of cutaneous melanoma. Int. J. Cancer 1997, 74, 535–539. [Google Scholar] [CrossRef]
- Hu, Y.X.; Watanabe, H.; Ohtsubo, K.; Yamaguchi, Y.; Ha, A.; Okai, T.; Sawabu, N. Frequent loss of p16 expression and its correlation with clinicopathological parameters in pancreatic carcinoma. Clin. Cancer Res. 1997, 3, 1473–1477. [Google Scholar]
- Yamada, Y.; Hatta, Y.; Murata, K.; Sugawara, K.; Ikeda, S.; Mine, M.; Maeda, T.; Hirakata, Y.; Kamihira, S.; Tsukasaki, K.; et al. Deletions of p15 and/or p16 genes as a poor-prognosis factor in adult T-cell leukemia. J. Clin. Oncol. 1997, 15, 1778–1785. [Google Scholar] [CrossRef] [PubMed]
- Kawabuchi, B.; Moriyama, S.; Hironaka, M.; Fujii, T.; Koike, M.; Moriyama, H.; Nishimura, Y.; Mizuno, S.; Fukayama, M. p16 inactivation in small-sized lung adenocarcinoma: Its association with poor prognosis. Int. J. Cancer 1999, 84, 49–53. [Google Scholar] [CrossRef]
- Straume, O.; Sviland, L.; A Akslen, L. Loss of nuclear p16 protein expression correlates with increased tumor cell proliferation (Ki-67) and poor prognosis in patients with vertical growth phase melanoma. Clin. Cancer Res. 2000, 6, 1845–1853. [Google Scholar] [PubMed]
- Mihic-Probst, D.; Mnich, C.D.; Oberholzer, P.A.; Seifert, B.; Sasse, B.; Moch, H.; Dummer, R. p16 expression in primary malignant melanoma is associated with prognosis and lymph node status. Int. J. Cancer 2005, 118, 2262–2268. [Google Scholar] [CrossRef]
- Gerdes, J.; Schwab, U.; Lemke, H.; Stein, H. Production of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferation. Int. J. Cancer 1983, 31, 13–20. [Google Scholar] [CrossRef]
- Menon, S.S.; Guruvayoorappan, C.; Sakthivel, K.M.; Rasmi, R.R. Ki-67 protein as a tumour proliferation marker. Clin. Chim. Acta 2019, 491, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Liu, P.; Da, J.; Hao, J.; Peng, W.; Sun, G. Prognostic value of Ki-67 in stage I non-small-cell lung cancer: A meta-analysis involving 1931 patients. Pathol.-Res. Pract. 2019, 215, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.-S.; Kang, G.; Sohn, J.H. Ki-67 labeling index can be used as a prognostic marker in gastrointestinal stromal tumor: A systematic review and meta-analysis. Int. J. Biol. Markers 2016, 31, e204–e210. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-J.; He, D.-S.; Tang, R.-X.; Ren, F.-H.; Chen, G. Ki-67 is a valuable prognostic factor in gliomas: Evidence from a systematic review and meta-analysis. Asian Pac. J. Cancer Prev. 2015, 16, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.-H.; Wen, D.-Y.; Luo, Y.-H.; Chen, G.; Yang, H.; Chen, J.-Q.; He, Y. The diagnostic and prognostic values of Ki-67/MIB-1 expression in thyroid cancer: A meta-analysis with 6,051 cases. Onco Targets Ther. 2017, 10, 3261–3276. [Google Scholar] [CrossRef]
- Robinson, E.M.; Rosenbaum, B.E.; Zhang, Y.; Rogers, R.; Tchack, J.; Berman, R.S.; Darvishian, F.; Osman, I.; Shapiro, R.L.; Shao, Y.; et al. Association between Ki-67 expression and clinical outcomes among patients with clinically node-negative, thick primary melanoma who underwent nodal staging. J. Surg. Oncol. 2018, 118, 150–156. [Google Scholar] [CrossRef]
- Udovicic-Gagula, D.; Ahmovic, A.; Bilalovic, N.; Doric, M. Expression of Ki-67 and Estrogen Receptor Beta in Primary Cutaneous Melanoma as a Potential Indicator of Regional Lymph Node Positivity. Appl. Immunohistochem. Mol. Morphol. 2019, 27, 27–32. [Google Scholar] [CrossRef]
- Sabbatino, F.; Scognamiglio, G.; Liguori, L.; Marra, A.; Anniciello, A.M.; Polcaro, G.; Col, J.D.; Caputo, A.; Peluso, A.L.; Botti, G.; et al. Peritumoral Immune Infiltrate as a Prognostic Biomarker in Thin Melanoma. Front. Immunol. 2020, 11, 561390. [Google Scholar] [CrossRef] [PubMed]
- Fortes, C.; Mastroeni, S.; Mannooranparampil, T.J.; Passarelli, F.; Zappalà, A.; Annessi, G.; Marino, C.; Caggiati, A.; Russo, N.; Michelozzi, P. Tumor-infiltrating lymphocytes predict cutaneous melanoma survival. Melanoma Res. 2015, 25, 306–311. [Google Scholar] [CrossRef]
- Eriksson, H.; Frohm-Nilsson, M.; Järås, J.; Kanter-Lewensohn, L.; Kjellman, P.; Månsson-Brahme, E.; Vassilaki, I.; Hansson, J. Prognostic factors in localized invasive primary cutaneous malignant melanoma: Results of a large population-based study. Br. J. Dermatol. 2014, 172, 175–186. [Google Scholar] [CrossRef]
- Erdag, G.; Schaefer, J.T.; Smolkin, M.E.; Deacon, D.H.; Shea, S.M.; Dengel, L.T.; Patterson, J.W.; Slingluff, C.L. Immunotype and immunohistologic characteristics of tumor-infiltrating immune cells are associated with clinical outcome in metastatic melanoma. Cancer Res. 2012, 72, 1070–1080. [Google Scholar] [CrossRef] [PubMed]
- Uguen, A.; Talagas, M.; Costa, S.; Duigou, S.; Bouvier, S.; De Braekeleer, M.; Marcorelles, P. A p16-Ki-67-HMB45 immunohistochemistry scoring system as an ancillary diagnostic tool in the diagnosis of melanoma. Diagn. Pathol. 2015, 10, 195. [Google Scholar] [CrossRef] [PubMed]
- Kavvadas, D.; Karachrysafi, S.; Anastasiadou, P.; Kavvada, A.; Fotiadou, S.; Papachristodoulou, A.; Papamitsou, T.; Sioga, A. Immunohistochemical Evaluation of CD3, CD4, CD8, and CD20 in Decidual and Trophoblastic Tissue Specimens of Patients with Recurrent Pregnancy Loss. Clin. Pract. 2022, 12, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Avilés-Izquierdo, J.A.; García-Piqueras, P.; Ciudad-Blanco, C.; Lozano-Masdemont, B.; Lázaro-Ochaita, P.; Bellón-Cano, J.M.; Rodríguez-Lomba, E. Do not PASS any melanoma without diagnosis: A new simplified dermoscopic algorithm. Int. J. Dermatol. 2023, 62, 518–523. [Google Scholar] [CrossRef]
- Dolianitis, C.; Kelly, J.; Wolfe, R.; Simpson, P. Comparative performance of 4 dermoscopic algorithms by nonexperts for the diagnosis of melanocytic lesions. Arch. Dermatol. 2005, 141, 1008–1014. [Google Scholar] [CrossRef] [PubMed]
- Reed, J.A.; Loganzo, F., Jr.; Shea, C.R.; Walker, G.J.; Flores, J.F.; Glendening, J.M.; Bogdany, J.K.; Shiel, M.J.; Haluska, F.G.; Fountain, J.W.; et al. Loss of expression of the p16/cyclin-dependent kinase inhibitor 2 tumor suppressor gene in melanocytic lesions correlates with invasive stage of tumor progression. Cancer Res. 1995, 55, 2713–2718. [Google Scholar] [PubMed]
- Liu, D.; Yang, X.; Wu, X. Tumor Immune Microenvironment Characterization Identifies Prognosis and Immunotherapy-Related Gene Signatures in Melanoma. Front. Immunol. 2021, 12, 663495. [Google Scholar] [CrossRef] [PubMed]
- Soo, J.K.; Castle, J.T.; Bennett, D.C. Preferential killing of melanoma cells by a p16-related peptide. Biol. Open 2023, 12, bio059965. [Google Scholar] [CrossRef] [PubMed]
- Catacchio, I.; Silvestris, N.; Scarpi, E.; Schirosi, L.; Scattone, A.; Mangia, A. Intratumoral, rather than stromal, CD8+ T cells could be a potential negative prognostic marker in invasive breast cancer patients. Transl. Oncol. 2019, 12, 585–595. [Google Scholar] [CrossRef]
- Tanaka, A.; Sakaguchi, S. Regulatory T cells in cancer immunotherapy. Cell Res. 2017, 27, 109–118. [Google Scholar] [CrossRef]
- Yuan, Y.; Zhu, Z.; Lan, Y.; Duan, S.; Zhu, Z.; Zhang, X.; Li, G.; Qu, H.; Feng, Y.; Cai, H.; et al. DDevelopment and Validation of a CD8+ T Cell Infiltration-Related Signature for Melanoma Patients. Front. Immunol. 2021, 12, 659444. [Google Scholar] [CrossRef]
- Liu, Q.; Peng, Z.; Shen, L.; Shen, L. Prognostic and Clinicopathological Value of Ki-67 in Melanoma: A Meta-Analysis. Front. Oncol. 2021, 11, 737760. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, M.; Lee, Y.; Simpson, D.; Moran, U.; Darvishian, F.; Kim, R.H.; Hernando, E.; Polsky, D.; Hanniford, D.; Shapiro, R.; et al. Primary Melanoma Histologic Subtype: Impact on Survival and Response to Therapy. J. Natl. Cancer Inst. 2018, 111, 180–188. [Google Scholar] [CrossRef]
- Lodha, S.; Saggar, S.; Celebi, J.T.; Silvers, D.N. Discordance in the histopathologic diagnosis of difficult melanocytic neoplasms in the clinical setting. J. Cutan. Pathol. 2008, 35, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Hekler, A.; Utikal, J.S.; Enk, A.H.; Berking, C.; Klode, J.; Schadendorf, D.; Jansen, P.; Franklin, C.; Holland-Letz, T.; Krahl, D.; et al. Pathologist-level classification of histopathological melanoma images with deep neural networks. Eur. J. Cancer 2019, 115, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-H.; Ali, N.S.; Vidal, N.Y. Social media use in residency recruitment during the COVID-19 pandemic. Dermatol. Online J. 2021, 27, 1–3. [Google Scholar] [CrossRef]
- Humphries, M.P.; Maxwell, P.; Salto-Tellez, M. QuPath: The global impact of an open source digital pathology system. Comput. Struct. Biotechnol. J. 2021, 19, 852–859. [Google Scholar] [CrossRef]
- Bishop, D.T.; Demenais, F.; Goldstein, A.M.; Bergman, W.; Bishop, J.N.; Bressac-de Paillerets, B.; Chompret, A.; Ghiorzo, P.; Gruis, N.; Hansson, J.; et al. Geographical variation in the penetrance of CDKN2A mutations for melanoma. J. Natl. Cancer Inst. 2002, 94, 894–903. [Google Scholar] [CrossRef]
- Talantov, D.; Mazumder, A.; Yu, J.X.; Briggs, T.; Jiang, Y.; Backus, J.; Atkins, D.; Wang, Y. Novel genes associated with malignant melanoma but not benign melanocytic lesions. Clin. Cancer Res. 2005, 11, 7234–7242. [Google Scholar] [CrossRef]
- Puig-Butille, J.A.; Escámez, M.J.; Garcia-Garcia, F.; Tell-Marti, G.; Fabra, À.; Martínez-Santamaría, L.; Badenas, C.; Aguilera, P.; Pevida, M.; Dopazo, J.; et al. Capturing the biological impact of CDKN2A and MC1R genes as an early predisposing event in melanoma and non melanoma skin cancer. Oncotarget 2013, 5, 1439–1451. [Google Scholar] [CrossRef]
- Levanat, S.; Situm, M.; Crnić, I.; Marasović, D.; Puizina-Ivić, N.; Pokupcić, N.; Musani, V.; Komar, A.; Kubat, M.; Furac, I.; et al. Alterations in CDKN2A locus as potential indicator of melanoma predisposition in relatives of non-familial melanoma cases. Croat. Med. J. 2003, 44, 418–424. [Google Scholar] [PubMed]
- Wang, L.; Rao, M.; Fang, Y.; Hameed, M.; Viale, A.; Busam, K.; Jhanwar, S.C. A genome-wide high-resolution array-CGH analysis of cutaneous melanoma and comparison of array-CGH to FISH in diagnostic evaluation. J. Mol. Diagn. 2013, 15, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Cesinaro, A.M.; Schirosi, L.; Bettelli, S.; Migaldi, M.; Maiorana, A. Alterations of 9p21 analysed by FISH and MLPA distinguish atypical spitzoid melanocytic tumours from conventional Spitz’s nevi but do not predict their biological behaviour. Histopathology 2010, 57, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Globocan 2020. Melanoma of Skin. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/16-Melanoma-of-skin-fact-sheet.pdf (accessed on 9 April 2024).
- Adler, N.; Kelly, J.; Haydon, A.; McLean, C.; Mar, V. Clinicopathological characteristics and prognosis of patients with multiple primary melanomas. Br. J. Dermatol. 2017, 178, e44–e45. [Google Scholar] [CrossRef]
- Cancer.Net Editorial Board. Familial Malignant Melanoma. Available online: https://www.cancer.net/cancer-types/familial-malignant-melanoma (accessed on 9 April 2024).


{kind=link}
| Marker | Clone | Manufacturer | Dilution | Host, Clonality/Additional Materials |
|---|---|---|---|---|
| P16 | MX007 | Master Diagnostica | Ready-to-use (RTU) 7 mL | Mouse, monoclonal |
| CD8 | SP16 | Master Diagnostica | RTU 7 mL | Rabbit, monoclonal |
| Ki67 | SP6 | Biocare | RTU 6 mL | Rabbit, monoclonal |
| SPEC CDKN2A/CEN 9 Dual Color Probe | ZytoLight® | ZytoVision GmbH, Bremerhaven, Germany | RTU 0.2 mL | ZytoLight FISH Implementation Kit |
| Patient Code | P16 | CD8 | Ki67 | CDKN2A Analysis |
|---|---|---|---|---|
| SV001 | 50% | 0% | 40% | Disomy |
| MS002 | 50% | 20% | 20% | Heterozygous deletion |
| IM003 | 50% | 0% | 25% | Heterozygous deletion |
| HV004 | 0% | 0% | 40% | Homozygous deletion |
| CV005 | 50% | 20% | 60% | Heterozygous deletion |
| RI006 | 0% | 5% | 60% | Homozygous deletion |
| PC007 | 50% | 0% | 10% | Disomy |
| BN008 | 50% | 20% | 10% | Monosomy |
| MR009 | 50% | 70% | 60% | Monosomy |
| MI010 | 0% | 5% | 60% | Homozygous deletion |
| PS011 | 50% | 10% | 10% | Disomy |
| AM012 | 50% | 40% | 70% | Disomy |
| GN013 | 0% | 0% | 40% | Homozygous deletion |
| CM014 | 0% | 0% | 50% | Homozygous deletion |
| CN015 | 50% | 5% | 50% | Disomy |
| GU016 | 50% | 10% | 10% | Disomy |
| SM017 | 50% | 0% | 60% | Monosomy |
| MS018 | 0% | 0% | 20% | Homozygous deletion |
| VS019 | 0% | 0% | 80% | Monosomy |
| LV020 | 0% | 90% | 20% | Monosomy |
| PD021 | 50% | 5% | 30% | Disomy |
| PG022 | 50% | 5% | 10% | Monosomy |
| TV023 | 0% | 0% | 50% | Homozygous deletion |
| Marker | CDKN2A-Wild Type Melanomas (Average Value) | CDKN2A-Mutated Melanomas (Average Value) | p-Value |
|---|---|---|---|
| P16 | 42.30% | 15.00% | 0.009045612 |
| CD8 | 19.61% | 5.00% | 0.118534718 |
| Ki67 | 35.38% | 42.50% | 0.430718946 |
| Parameter | Score 0 | Score 1 | Score 2 | Score 3 | Score 4 | Total Score |
|---|---|---|---|---|---|---|
| P16 (positive cells) | >50% | 11–50% | 1–10% | 0% | - | 0–10 |
| CD8+ peritumoral TILs | >60% | 20–60% | <20% | 0% | - | |
| Ki67 (proliferative index) | <2% | 2–5% | 6–10% | 11–20% | >20% |
| Patient Code | CDKN2A Analysis | Total Value of the Triple p16-CD8-Ki67 Score |
|---|---|---|
| SV001 | Disomy | 8 |
| PC007 | Disomy | 6 |
| BN008 | Monosomy | 4 |
| MR009 | Monosomy | 5 |
| PS011 | Disomy | 5 |
| SM017 | Monosomy | 8 |
| MS002 | Heterozygous deletion | 5 |
| IM003 | Heterozygous deletion | 8 |
| HV004 | Homozygous deletion | 10 |
| CV005 | Heterozygous deletion | 5 |
| RI006 | Homozygous deletion | 9 |
| Patient Code | CDKN2A Analysis | Total Value of the Triple p16-CD8-Ki67 Score |
|---|---|---|
| AM012 | Disomy | 6 |
| CN015 | Disomy | 7 |
| GU016 | Disomy | 5 |
| VS019 | Monosomy | 10 |
| LV020 | Monosomy | 6 |
| PD021 | Disomy | 7 |
| PG022 | Monosomy | 5 |
| MI010 | Homozygous deletion | 9 |
| GN013 | Homozygous deletion | 10 |
| CM014 | Homozygous deletion | 10 |
| MS018 | Homozygous deletion | 9 |
| TV023 | Homozygous deletion | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nurla, L.-A.; Gheorghe, E.; Aşchie, M.; Cozaru, G.C.; Orășanu, C.I.; Boşoteanu, M. P16-CD8-Ki67 Triple Algorithm for Prediction of CDKN2A Mutations in Patients with Multiple Primary and Familial Melanoma. Diagnostics 2024, 14, 813. https://doi.org/10.3390/diagnostics14080813
Nurla L-A, Gheorghe E, Aşchie M, Cozaru GC, Orășanu CI, Boşoteanu M. P16-CD8-Ki67 Triple Algorithm for Prediction of CDKN2A Mutations in Patients with Multiple Primary and Familial Melanoma. Diagnostics. 2024; 14(8):813. https://doi.org/10.3390/diagnostics14080813
Chicago/Turabian StyleNurla, Luana-Andreea, Emma Gheorghe, Mariana Aşchie, Georgeta Camelia Cozaru, Cristian Ionuț Orășanu, and Mǎdǎlina Boşoteanu. 2024. "P16-CD8-Ki67 Triple Algorithm for Prediction of CDKN2A Mutations in Patients with Multiple Primary and Familial Melanoma" Diagnostics 14, no. 8: 813. https://doi.org/10.3390/diagnostics14080813
APA StyleNurla, L. -A., Gheorghe, E., Aşchie, M., Cozaru, G. C., Orășanu, C. I., & Boşoteanu, M. (2024). P16-CD8-Ki67 Triple Algorithm for Prediction of CDKN2A Mutations in Patients with Multiple Primary and Familial Melanoma. Diagnostics, 14(8), 813. https://doi.org/10.3390/diagnostics14080813