
Comparative Assessment of Robotic versus Classical Physical Therapy Using Muscle Strength and Ranges of Motion Testing in Neurological Diseases


 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
Evaluation Protocol
3. Results
4. Discussion
- (1)
- General benefits of physical therapy in neuromotor diseases: besides the Vascular group, which is known to benefit from physical therapy, there are also promising results in the other study groups that could improve the quality of life of chronic patients and delay the effect of degenerative diseases;
- (2)
- Comparative assessment of robotic versus manual physical therapy: our results illustrate that robotic therapy can be used for the treatment of neuromotor diseases with similar results as manual therapy, which, in the face of the upcoming crisis caused by the ageing of the population, represents a valid option to enable the treatment of more patients requiring physical therapy;
- (3)
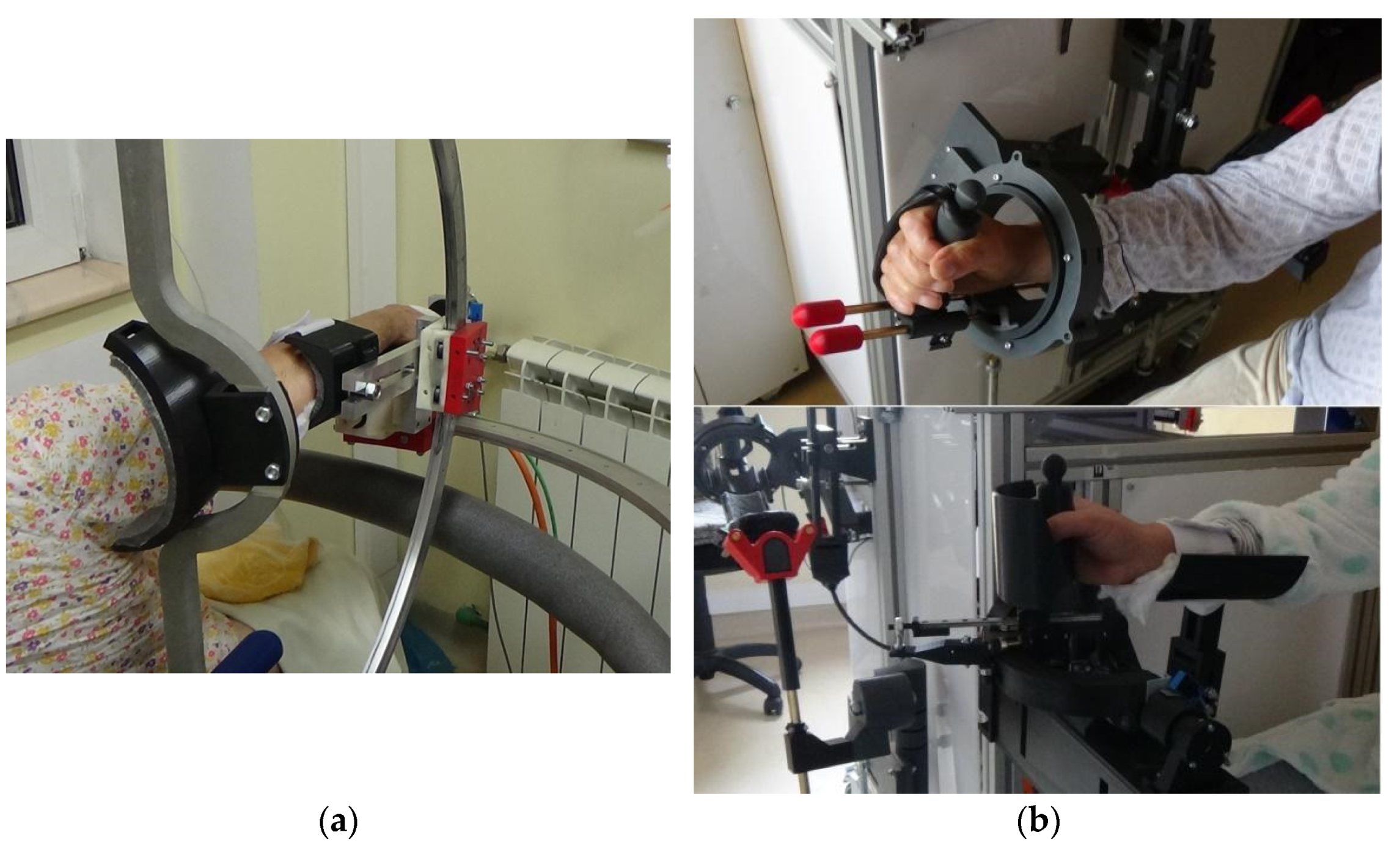
- Possible improvements of the robotic devices: each module of the upper limb robotic system has been carefully analyzed based on clinical data, and our team is working on improving the overall system. For the shoulder rehabilitation device, ASPIRE, our team has recently completed processing the clinical data [31], while ParReEx is expected to be ready in the coming months.
- The improvement of the graphical user interface to investigate the possibility of working with more patients simultaneously under the supervision of a single therapist;
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parre, M.D.; Sujatha, B. Novel Human-Centered Robotics: Towards an Automated Process for Neurorehabilitation. Neurol. Res. Int. 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Braun, R.G.; Wittenberg, G.F. Motor Recovery: How Rehabilitation Techniques and Technologies Can Enhance Recovery and Neuroplasticity. Semin. Neurol. 2021, 41, 167–176. [Google Scholar] [CrossRef]
- Masiero, S.; Celia, A.; Rosati, G.; Armani, M. Robotic-Assisted Rehabilitation of the Upper Limb after Acute Stroke. Arch. Phys. Med. Rehabil. 2007, 88, 142–149. [Google Scholar] [CrossRef]
- Singh, N.; Saini, M.; Kumar, N.; Srivastava, M.V.P.; Mehndiratta, A. Evidence of neuroplasticity with robotic hand exoskel-eton for post-stroke rehabilitation: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 1–15. [Google Scholar] [CrossRef]
- Taravati, S.; Capaci, K.; Uzumcugil, H.; Tanigor, G. Evaluation of an upper limb robotic rehabilitation program on motor functions, quality of life, cognition, and emotional status in patients with stroke: A randomized controlled study. Neurol. Sci. 2021, 1–12. [Google Scholar] [CrossRef]
- Androwis, G.J.; Sandroff, B.M.; Niewrzol, P.; Fakhoury, F.; Wylie, G.R.; Yue, G.; DeLuca, J. A Pilot Randomized Controlled Trial of Robotic Exoskeleton-Assisted Exercise Rehabilitation in Multiple Sclerosis. Mult. Scler. Relat. Disord. 2021, 51, 102936. [Google Scholar] [CrossRef]
- Paolucci, T.; Agostini, F.; Mangone, M.; Bernetti, A.; Pezzi, L.; Liotti, V.; Recubini, E.; Cantarella, C.; Bellomo, R.G.; D’Aurizio, C.; et al. Robotic rehabilitation for end-effector device and botulinum toxin in upper limb rehabilitation in chronic post-stroke patients: An integrated rehabilitative approach. Neurol. Sci. 2021, 1–11. [Google Scholar] [CrossRef]
- Budhota, A.; Chua, K.S.G.; Hussain, A.; Kager, S.; Cherpin, A.; Contu, S.; Vishwanath, D.; Kuah, C.W.K.; Ng, C.Y.; Yam, L.H.L.; et al. Robotic assisted upper limb training post-stroke: A randomized control trial using combinatory approach towards reducing workforce demands. Front. Neurol. 2021, 12, 622014. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, E.; Gasperini, G.; Zajc, J.; Immick, N.; Augsten, A.; Rossini, M.; Ballarati, R.; Russold, M.; Ferrante, S.; Ferrigno, G.; et al. A robotic system with EMG-triggered functional electrical stimulation for restoring arm func-tions in stroke survivors. Neurorehabilit. Neural Repair 2021, 35, 334–345. [Google Scholar] [CrossRef]
- Waller, S.M.; Whithall, J. Hand dominance and side of stroke affect rehabilitation in chronic stroke. Clin. Rehabil. 2005, 15, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.E.; Eng, J.J. Individuals with the dominant hand affected following stroke demonstrate less impairment than those with non-dominant hand affected. Neurorehabil. Neural Repair 2006, 20, 380–389. [Google Scholar] [CrossRef] [Green Version]
- Nam, H.U.; Huh, J.S.; Na Yoo, J.; Hwang, J.M.; Lee, B.J.; Min, Y.-S.; Kim, C.-H.; Jung, T.-D. Effect of Dominant Hand Paralysis on Quality of Life in Patients With Subacute Stroke. Ann. Rehabil. Med. 2014, 38, 450–457. [Google Scholar] [CrossRef] [Green Version]
- Major, Z.Z.; Vaida, C.; Major, K.A.; Tucan, P.; Simori, G.; Banica, A.; Brusturean, E.; Burz, A.; Craciunas, R.; Ulinici, I.; et al. The Impact of Robotic Rehabilitation on the Motor System in Neurological Diseases. A Multimodal Neurophysiological Approach. Int. J. Environ. Res. Public Health 2020, 17, 6557. [Google Scholar] [CrossRef]
- Reis, S.B.; Bernardo, W.M.; Oshiro, C.A.; Krebs, H.I.; Conforto, A.B. Effects of Robotic Therapy Associated With Noninvasive Brain Stimulation on Upper-Limb Rehabilitation After Stroke: Systematic Review and Meta-analysis of Randomized Clinical Trials. Neurorehabilit. Neural Repair 2021, 35, 256–266. [Google Scholar] [CrossRef]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef]
- Hatem, S.M.; Saussez, G.; Della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrazzoli, D.; Ortelli, P.; Zivi, I.; Cian, V.; Urso, E.; Ghilardi, M.F.; Maestri, R.; Frazzitta, G. Efficacy of intensive multidisciplinary rehabilitation in Parkinson’s disease: A randomised controlled study. J. Neurol. Neurosurg. Psychiatry 2018, 89, 828–835. [Google Scholar] [CrossRef]
- Prodoehl, J.; Rafferty, M.; David, F.; Poon, C.; Vaillancourt, D.E.; Comella, C.L.; Leurgans, S.E.; Kohrt, W.M.; Corcos, D.M.; Robichaud, J.A. Two-Year Exercise Program Improves Physical Function in Parkinson’s Disease: A randomised controlled study. Neurorehabilit. Neural Repair 2015, 29, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Paganoni, S.; Karam, C.; Joyce, N.; Bedlack, R.; Carter, G.T. Comprehensive rehabilitative care across the spectrum of amyotrophic lateral sclerosis. NeuroRehabilitation 2015, 37, 53–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bello-Haas, V.D. Physical therapy for individuals with amyotrophic lateral sclerosis: Current insights. Degener. Neurol. Neuromuscul. Dis. 2018, 8, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Major, Z.Z.; Văcăraș, V.; Mariș, E.; Crișan, I.; Florea, B.; Major, K.A.; Mureșanu, D.F. The electrophysiological changes after 1 Hz rTMS in ALS patients. A pilot study. Ideggyógyászati Szemle 2016, 69. [Google Scholar] [CrossRef]
- Major, K.A.; Major, Z.Z.; Craciunas, R.; Carbone, G.; Vaida, C.; Pîslă, D.L. Efficiency of Transcranial Magnetic Stimulation in Progressive Supranuclear Palsy: Estimation Using Goniometry and Dinamometry. Neurophysiology 2019, 51, 57–62. [Google Scholar] [CrossRef]
- Tucan, P.; Vaida, C.; Ulinici, I.; Banica, A.; Burz, A.; Pop, N.; Birlescu, I.; Gherman, B.; Plitea, N.; Antal, T.; et al. Optimization of the ASPIRE Spherical Parallel Rehabilitation Robot Based on Its Clinical Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 3281. [Google Scholar] [CrossRef] [PubMed]
- Plitea, N.; Vaida, C.; Carbone, G.; Pisla, A.; Ulinici, I.; Pisla, D. On the Kinematics of an Innovative Spherical Parallel Robot for Shoulder Rehabilitation. Mech. Eng. Mater. 2018, 54, 464–473. [Google Scholar] [CrossRef]
- Vaida, C.; Ulinici, I.; Banica, A.; Burz, A.; Gherman, B.; Tucan, P.; Pisla, A.; Carbone, G.; Pisla, D. First Clinical Evalu-ation of a Spherical Robotic system for Shoulder Rehabilitation. In Proceedings of the International Workshop on Medical and Service Robots, Basel, Switzerland, 8–10 July 2020; Volume 93. [Google Scholar]
- Vaida, C.; Plitea, N.; Pisla, D.; Carbone, G.; Gherman, B.; Ulinici, I.; Pisla, A. Spherical Robot for Medical Rehabilitation of Proximal Area of Upper Limb. Patent No. RO-132233, 30 March 2020. [Google Scholar]
- Tucan, P.; Gherman, B.; Major, K.; Vaida, C.; Major, Z.; Plitea, N.; Carbone, G.; Pisla, D. Fuzzy Logic-Based Risk Assessment of a Parallel Robot for Elbow and Wrist Rehabilitation. Int. J. Environ. Res. Public Health 2020, 17, 654. [Google Scholar] [CrossRef] [Green Version]
- Gherman, B.; Carbone, G.; Plitea, N.; Ceccarelli, M.; Banica, A.; Pisla, D. Kinematic Design of a Parallel Robot for Elbow and Wrist Rehabilitation. In Mechanical Engineering and Materials; Springer Science and Business Media LLC: Cham, Switzerland, 2018; Volume 57, pp. 147–154. [Google Scholar]
- Gherman, B.; Pisla, D.; Plitea, N.; Vaida, C.; Carbone, G.; Pisla, A.; Banica, A. Parallel Robotic System for Medical Reha-bilitation of Upper Limb. Patent No. RO-132234, 30 March 2020. [Google Scholar]
- Wortman-Jutt, S.; Edwards, D. Poststroke Aphasia Rehabilitation: Why All Talk and No Action? Neurorehabilit. Neural Repair 2019, 33, 235–244. [Google Scholar] [CrossRef]
- Tramontano, M.; Morone, G.; Palomba, A.; De Angelis, S.; Mercuro, A.; Caltagirone, C.; Grasso, M.G. Effectiveness of a sensor-based technology in upper limb motor recovery in post-acute stroke neurorehabilitation: A randomized con-trolled trial. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 3), 165–174. [Google Scholar]
- Lee, H.-C.; Kuo, F.-L.; Lin, Y.-N.; Liou, T.-H.; Lin, J.-C.; Huang, S.-W. Effects of Robot-Assisted Rehabilitation on Hand Function of People With Stroke: A Randomized, Crossover-Controlled, Assessor-Blinded Study. Am. J. Occup. Ther. 2021, 75, 7501205020p1–7501205020p11. [Google Scholar] [CrossRef]
- Major, K.; Major, Z.; Carbone, G.; Pisla, A.; Vaida, C.; Gherman, B.; Pisla, D. Ranges of Motion as Basis for Robot-Assisted Post-Stroke Rehabilitation. Hum. Vet. Med. Int. J. Bioflux Soc. 2016, 8, 200–204. [Google Scholar]
- Rodriguez-Sabate, C.; Morales, I.; Lorenzo, J.N.; Rodriguez, M. The organization of the basal ganglia functional connectivity network is non-linear in Parkinson’s disease. NeuroImage Clin. 2019, 22, 101708. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Fu, Z.; Le, W. Exercise and Parkinson’s disease. Int. Rev. Neurobiol. 2019, 147, 45–74. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, C.; Clarke, C.; Stowe, R.; Shah, L.; Sackley, C.; Deane, K.; Wheatley, K.; et al. Physiotherapy versus placebo or no intervention in Parkinson’s disease. Cochrane Database Syst. Rev. 2013, 2013, CD002817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longatelli, V.; Antonietti, A.; Biffi, E.; Diella, E.; D’Angelo, M.G.; Rossini, M.; Molteni, F.; Bocciolone, M.; Pedrocchi, A.; Gandolla, M. User-centred assistive SystEm for arm Functions in neUromuscuLar subjects (USEFUL): A randomized controlled study. J. Neuroeng. Rehabil. 2021, 18, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wang, C.; Fan, W.; Gu, M.; Yasin, G.; Xiao, S.; Huang, J.; Huang, X. Robot-Assisted Arm Training versus Therapist-Mediated Training after Stroke: A Systematic Review and Meta-Analysis. J. Health Eng. 2020, 2020, 8810867. [Google Scholar] [CrossRef] [PubMed]
- Pop, N.; Vaida, C.; Carbone, G.; Craciun, F.; Major, K.; Abrudan, C.; Puskas, F.; Pisla, D. The Analysis of Bio-Signals and Sensors for Robotic Assisted Rehabilitation. In Proceedings of the 6th International Conference on Advancements of Medicine and Health Care through Technology, Cluj-Napoca, Romania, 17–20 October 2018; Springer: Singapore, 2019; Volume 71, pp. 229–235. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Vascular Disease | Extrapyramidal Disease | Neuromuscular Disease |
|---|---|---|
| Passive motions, 2 sessions/day 10–12 repetitions: (Conventional and robotic therapy) | Passive motions, 2 sessions/day 10–12 repetitions: (Conventional and robotic therapy) | Passive motions, 2 sessions/day 8–10 repetitions: (Conventional and robotic therapy) |
| Radio-carpal joint flexion and extension Radio-carpal joint rotation Forearm supination and pronation Elbow flexion Shoulder flexion and extension Shoulder adduction and adduction | Radio-carpal joint flexion and extension Radio-carpal joint rotation Forearm supination and pronation Elbow flexion Shoulder flexion and extension Shoulder adduction and adduction | Radio-carpal joint flexion and extension Radio-carpal joint rotation Forearm supination/pronation Elbow flexion with 10–20% resistance, stretching program, positioning in extension Shoulder adduction and adduction |
| MRC Scale for Muscle Power | |
|---|---|
| 0 | No muscle contraction is visible. |
| 1 | Muscle contraction is visible but there is no movement of the joint. |
| 2 | Active joint movement is possible with gravity eliminated. |
| 3 | Movement can overcome gravity but not resistance from the examiner. |
| 4 | The muscle group can overcome gravity and move against some resistance. |
| 5 | Full and normal power against resistance. |
| Vascular | Extrapyramidal | Neuromuscular | |
|---|---|---|---|
| Age [years] [10] | 75.92 ± 1.77 | 71.17 ± 4.13 | 66.00 ± 3.85 |
| M | 6 (50%) | 3 (50%) | 3 (60%) |
| F | 6 (50%) | 3 (50%) | 2 (40%) |
| Left side deficit | 6 (50%) | 6 (100%) | 5 (100%) |
| Right side deficit | 6 (50%) | 6 (100%) | 5 (100%) |
| Dominant hand | L 2 (16.66%) | L 2 (33.33%) | L 1 (20%) |
| R 10 (83.34%) | R 4 (66.67%) | R 4 (80%) | |
| MMS score | 26.52 ± 1.283 | 27.11 ± 1.304 | 26.79 ± 1.391 |
| Time from neurological disease [months] | 9.08 ± 5.07 | 12.33 ± 6.54 | 9.20 ± 4.35 |
| Motion | Vascular (Degrees) | Result (%) | Extrapyramidal (Degrees) | Result (%) | Neuromuscular (Degrees) | Result (%) | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Final | Baseline | Final | Baseline | Final | ||||
| Shoulder Flexion | 82.04 ± 3.40 | 93.34 ± 4.42 | 13.77 | 109.11 ± 7.11 | 121.42 ± 3.55 | 11.28 | 107.31 ± 10.2 | 92.11 ± 1.21 | −14.16 |
| Shoulder Extension | 34.51 ± 5.31 | 49.31 ± 2.75 | 42.89 | 42.63 ± 6.12 | 43.44 ± 4.45 | 1.90 | 44.18 ± 4.56 | 45.66 ± 5.65 | 3.35 |
| Shoulder Abduction | 59.12 ± 6.78 | 54.24 ± 2.38 | −8.25 | 61.24 ± 3.24 | 64.16 ± 3.21 | 4.77 | 61.37 ± 3.12 | 63.32 ± 2.77 | 3.18 |
| Shoulder Adduction | 32.73 ± 3.15 | 48.13 ± 4.33 | 47.05 | 63.15 ± 3.14 | 71.84 ± 2.55 | 13.76 | 50.64 ± 2.64 | 51.56 ± 8.22 | 1.82 |
| Elbow Flexion | 121.16 ± 4.32 | 132.07 ± 8.22 | 9.00 | 138.21 ± 6.98 | 140.76 ± 8.2 | 1.85 | 137.84 ± 4.24 | 138.21 ± 9.98 | 0.27 |
| Elbow pronation | 62.36 ± 4.11 | 71.17 ± 5.24 | 14.13 | 72.79 ± 4.37 | 84.32 ± 5.12 | 15.84 | 78.10 ± 3.51 | 80.65 ± 6.24 | 3.27 |
| Elbow Supination | 63.95 ± 6.98 | 77.67 ± 2.22 | 21.45 | 81.34 ± 5.15 | 84.54 ± 4.22 | 3.93 | 81.67 ± 1.61 | 86.61 ± 2.55 | 6.05 |
| Radio-carpal flexion | 41.24 ± 4.35 | 49.22 ± 2.35 | 19.35 | 58.36 ± 4.61 | 64.13 ± 2.28 | 9.89 | 58.46 ± 7.21 | 57.31 ± 5.36 | −1.97 |
| Radio-carpal extension | 40.61 ± 3.21 | 50.45 ± 4.78 | 24.23 | 52.47 ± 2.07 | 59.77 ± 6.32 | 13.91 | 58.22 ± 5.23 | 58.65 ± 4.12 | 0.74 |
| Motion | Vascular | Result (%) | Extrapyramidal | Result (%) | Neuromuscular | Result (%) | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Final | Baseline | Final | Baseline | Final | ||||
| Shoulder Flexion | 4.04 ± 0.21 | 4.12 ± 0.70 | 1.98 | 4.41 ± 0.23 | 4.94 ± 0.01 | 12.02 | 4.06 ± 0.15 | 3.95 ± 1.01 | −2.71 |
| Shoulder Extension | 3.91 ± 0.13 | 4.32 ± 0.33 | 10.49 | 4.35 ± 0.31 | 4.67 ± 0.13 | 7.36 | 4.45 ± 0.23 | 3.93 ± 0.52 | −11.69 |
| Shoulder Abduction | 4.22 ± 0.60 | 4.43 ± 0.12 | 4.98 | 4.74 ± 0.12 | 4.97 ± 0.01 | 4.85 | 4.16 ± 0.36 | 4.06 ± 0.36 | −2.40 |
| Shoulder Adduction | 4.27 ± 0.33 | 4.41 ± 0.21 | 3.28 | 4.83 ± 0.08 | 4.94 ± 0.02 | 2.28 | 4.19 ± 0.44 | 4.15 ± 0.18 | −0.95 |
| Elbow Flexion | 3.73 ± 0.90 | 4.39 ± 0.33 | 17.69 | 4.75 ± 0.10 | 4.92 ± 0.02 | 3.58 | 4.21 ± 0.18 | 4.29 ± 0.16 | 1.90 |
| Elbow pronation | 4.18 ± 0.60 | 4.47 ± 0.44 | 6.94 | 4.46 ± 0.12 | 4.93 ± 0.05 | 10.54 | 4.08 ± 0.22 | 4.08 ± 0.25 | 0.00 |
| Elbow Supination | 3.72 ± 1.10 | 3.92 ± 0.99 | 5.38 | 4.48 ± 0.40 | 4.76 ± 0.10 | 6.25 | 3.81 ± 0.91 | 3.83 ± 0.39 | 0.52 |
| Radio-carpal flexion | 4.19 ± 0.56 | 3.71 ± 1.01 | −11.46 | 4.75 ± 0.13 | 4.81 ± 0.16 | 1.26 | 4.16 ± 0.28 | 3.95 ± 0.46 | −5.05 |
| Radio-carpal extension | 3.92 ± 0.81 | 4.23 ± 0.22 | 7.91 | 4.78 ± 0.09 | 4.87 ± 0.10 | 1.88 | 4.17 ± 0.39 | 3.95 ± 0.38 | −5.28 |
| Motion | Vascular (kgf) | Result (%) | Extrapyramidal (kgf) | Result (%) | Neuromuscular (kgf) | Result (%) | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Final | Baseline | Final | Baseline | Final | ||||
| Shoulder Flexion | 4.05 ± 0.25 | 4.03 ± 1.12 | −0.49 | 6.11 ± 0.66 | 6.42 ± 0.25 | 5.07 | 4.23 ± 1.01 | 4.83 ± 1.03 | 14.18 |
| Shoulder Extension | 4.14 ± 0.38 | 4.15 ± 0.87 | 0.24 | 5.72 ± 0.29 | 5.86 ± 0.55 | 2.45 | 4.42 ± 0.28 | 4.54 ± 0.78 | 2.71 |
| Shoulder Abduction | 3.92 ± 0.68 | 3.91 ± 1.11 | −0.26 | 5.98 ± 0.27 | 6.14 ± 0.24 | 2.68 | 4.39 ± 0.55 | 4.45 ± 0.88 | 1.37 |
| Shoulder Adduction | 3.96 ± 0.17 | 4.04 ± 0.88 | 2.02 | 5.91 ± 0.34 | 6.19 ± 0.35 | 4.74 | 4.46 ± 0.98 | 4.53 ± 0.47 | 1.57 |
| Elbow Flexion | 5.14 ± 1.20 | 6.12 ± 0.16 | 19.07 | 7.81 ± 0.10 | 7.91 ± 0.08 | 1.28 | 5.93 ± 0.19 | 6.31 ± 0.98 | 6.41 |
| Elbow pronation | 2.44 ± 1.80 | 2.72 ± 1.25 | 11.48 | 3.87 ± 1.12 | 4.24 ± 1.02 | 9.56 | 2.70 ± 1.97 | 2.77 ± 1.12 | 2.59 |
| Elbow Supination | 5.47 ± 0.98 | 5.52 ± 1.16 | 0.91 | 7.76 ± 0.11 | 7.85 ± 0.02 | 1.16 | 5.81 ± 0.88 | 6.06 ± 0.28 | 4.30 |
| Radio-carpal flexion | 2.86 ± 1.30 | 3.29 ± 1.23 | 15.03 | 3.93 ± 0.99 | 4.73 ± 0.25 | 20.36 | 2.67 ± 1.21 | 2.65 ± 1.09 | −0.75 |
| Radio-carpal extension | 4.17 ± 0.89 | 4.64 ± 0.88 | 11.27 | 3.22 ± 0.94 | 4.16 ± 0.18 | 29.19 | 4.14 ± 1.71 | 4.63 ± 0.85 | 11.84 |
| Motion | Vascular Group | Extrapyramidal Group | Neuromuscular Group | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Goniometry | MRC | Dynamometry | Goniometry | MRC | Dynamometry | Goniometry | MRC | Dynamometry | |
| Shoulder Flexion | 0.15 | 0.43 | 0.57 | 0.59 | 0.97 | 0.35 | 0.42 | 0.44 | 0.69 |
| Shoulder Extension | 0.71 | 0.35 | 0.46 | 0.46 | 0.25 | 0.21 | 0.32 | 0.33 | 0.13 |
| Shoulder Abduction | 0.18 | 0.84 | 0.87 | 0.71 | 0.27 | 0.35 | 0.37 | 0.68 | 0.47 |
| Shoulder Adduction | 0.36 | 0.81 | 0.48 | 0.98 | 0.61 | 0.68 | 0.73 | 0.44 | 0.76 |
| Elbow Flexion | 0.68 | 0.20 | 0.30 | 0.37 | 0.40 | 0.45 | 0.16 | 0.46 | 0.48 |
| Elbow pronation | 0.36 | 0.72 | 0.67 | 0.29 | 0.86 | 0.74 | 0.73 | 0.45 | 0.23 |
| Elbow Supination | 0.81 | 0.59 | 0.75 | 0.83 | 0.83 | 0.56 | 0.74 | 0.70 | 0.14 |
| Radio-carpal flexion | 0.70 | 0.42 | 0.60 | 0.68 | 0.49 | 0.14 | 0.26 | 0.82 | 0.53 |
| Radio-carpal extension | 0.48 | 0.36 | 0.39 | 0.34 | 0.69 | 0.20 | 0.48 | 0.54 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Major, Z.Z.; Vaida, C.; Major, K.A.; Tucan, P.; Brusturean, E.; Gherman, B.; Birlescu, I.; Craciunaș, R.; Ulinici, I.; Simori, G.; et al. Comparative Assessment of Robotic versus Classical Physical Therapy Using Muscle Strength and Ranges of Motion Testing in Neurological Diseases. J. Pers. Med. 2021, 11, 953. https://doi.org/10.3390/jpm11100953
Major ZZ, Vaida C, Major KA, Tucan P, Brusturean E, Gherman B, Birlescu I, Craciunaș R, Ulinici I, Simori G, et al. Comparative Assessment of Robotic versus Classical Physical Therapy Using Muscle Strength and Ranges of Motion Testing in Neurological Diseases. Journal of Personalized Medicine. 2021; 11(10):953. https://doi.org/10.3390/jpm11100953
Chicago/Turabian StyleMajor, Zoltán Zsigmond, Calin Vaida, Kinga Andrea Major, Paul Tucan, Emanuela Brusturean, Bogdan Gherman, Iosif Birlescu, Raul Craciunaș, Ionut Ulinici, Gábor Simori, and et al. 2021. "Comparative Assessment of Robotic versus Classical Physical Therapy Using Muscle Strength and Ranges of Motion Testing in Neurological Diseases" Journal of Personalized Medicine 11, no. 10: 953. https://doi.org/10.3390/jpm11100953
APA StyleMajor, Z. Z., Vaida, C., Major, K. A., Tucan, P., Brusturean, E., Gherman, B., Birlescu, I., Craciunaș, R., Ulinici, I., Simori, G., Banica, A., Pop, N., Burz, A., Carbone, G., & Pisla, D. (2021). Comparative Assessment of Robotic versus Classical Physical Therapy Using Muscle Strength and Ranges of Motion Testing in Neurological Diseases. Journal of Personalized Medicine, 11(10), 953. https://doi.org/10.3390/jpm11100953