
Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge


Abstract
:1. Introduction
2. Materials and Methods
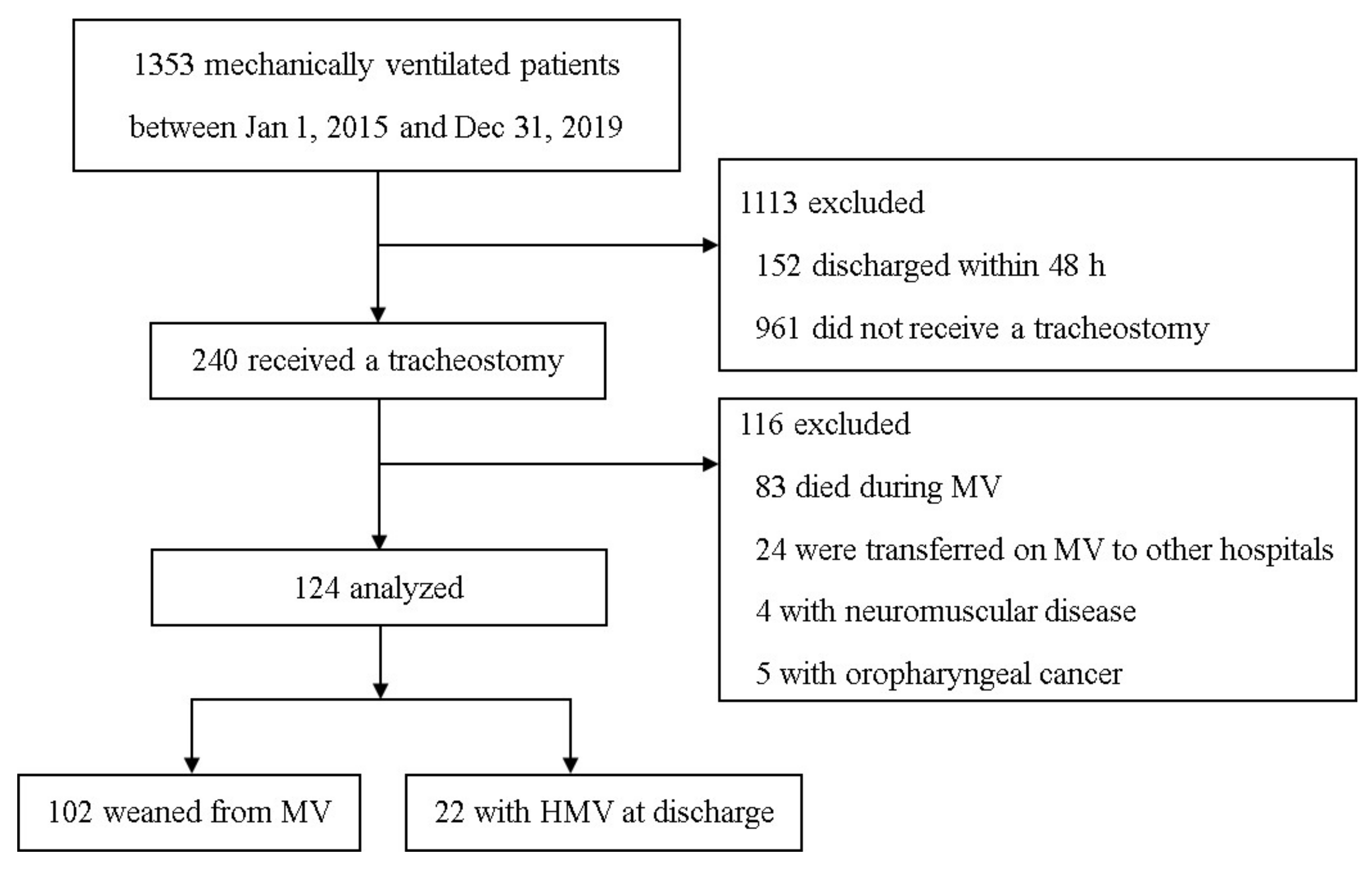
2.1. Study Design and Patients
2.2. Data Collection and Definitions
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
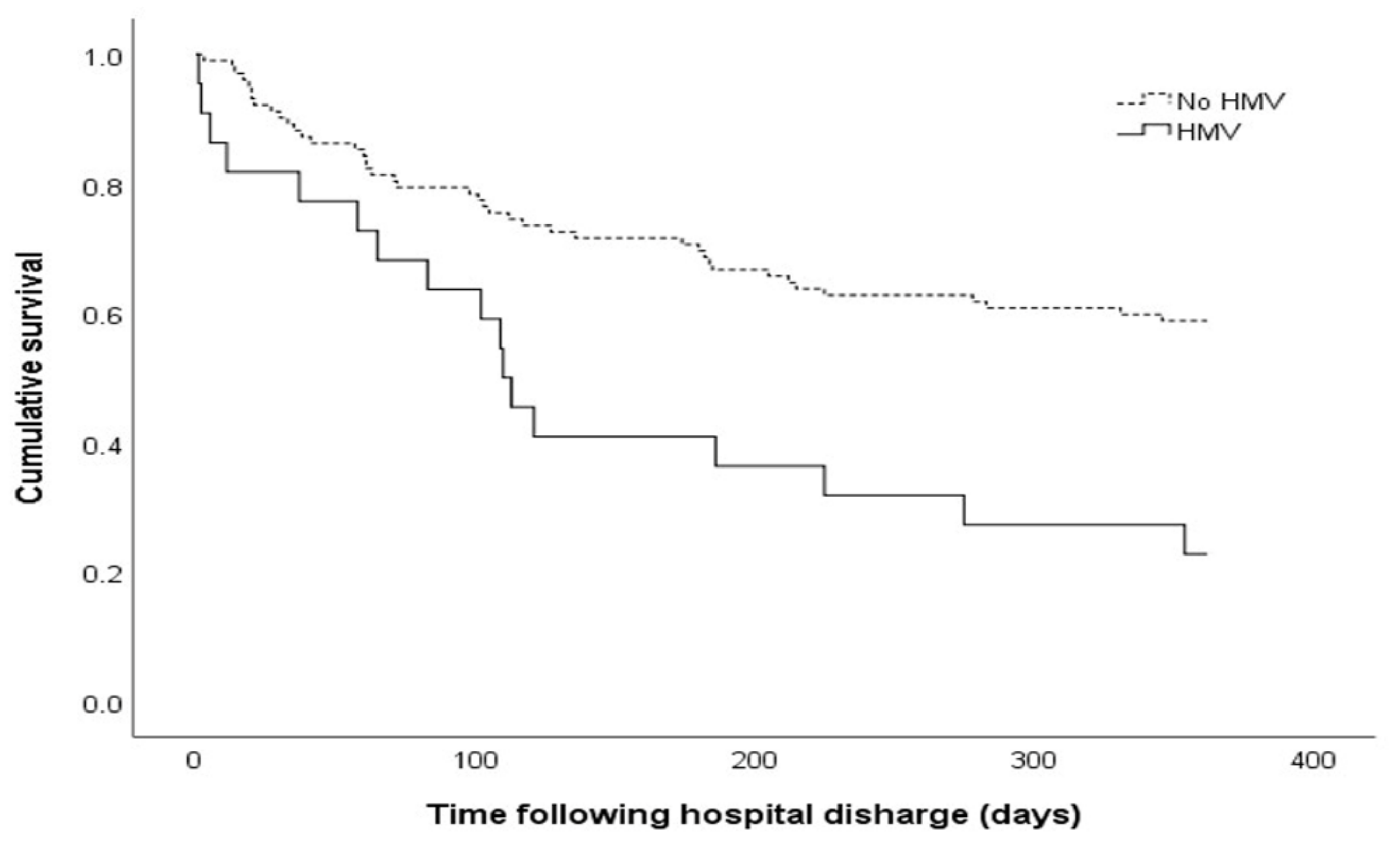
3.2. Outcomes of Patients Who Received a Tracheostomy
3.3. Predictive Factors for 1-Year Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simonds, A.K. Home Mechanical Ventilation: An Overview. Ann. Am. Thorac. Soc. 2016, 13, 2035–2044. [Google Scholar] [CrossRef] [Green Version]
- Hind, M.; Polkey, M.I.; Simonds, A.K. AJRCCM: 100-Year Anniversary. Homeward Bound: A Centenary of Home Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2017, 195, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Cho, J.H.; Park, S.Y.; Lee, Y.S.; Chang, Y.; Choi, W.I.; Sim, Y.S.; Moon, J.Y.; Lee, K.; Jung, K.S.; et al. Home Mechanical Ventilation Use in South Korea Based on National Health Insurance Service Data. Respir. Care 2019, 64, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, K.; Wahidi, M.M. The Changing Role for Tracheostomy in Patients Requiring Mechanical Ventilation. Clin. Chest Med. 2016, 37, 741–751. [Google Scholar] [CrossRef]
- Ambrosino, N.; Gabbrielli, L. The difficult-to-wean patient. Exp. Rev. Respir. Med. 2010, 4, 685–692. [Google Scholar] [CrossRef]
- Li, J.; Zhan, Q.Y.; Wang, C. Survey of Prolonged Mechanical Ventilation in Intensive Care Units in Mainland China. Respiratory Care 2016, 61, 1224–1231. [Google Scholar] [CrossRef] [Green Version]
- Damuth, E.; Mitchell, J.A.; Bartock, J.L.; Roberts, B.W.; Trzeciak, S. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: A systematic review and meta-analysis. Lancet. Respir. Med. 2015, 3, 544–553. [Google Scholar] [CrossRef]
- Hill, A.D.; Fowler, R.A.; Burns, K.E.; Rose, L.; Pinto, R.L.; Scales, D.C. Long-Term Outcomes and Health Care Utilization after Prolonged Mechanical Ventilation. Ann. Am. Thorac. Soc. 2017, 14, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Vagheggini, G.; Vlad, E.P.; Mazzoleni, S.; Bortolotti, U.; Guarracino, F.; Ambrosino, N. Outcomes for difficult-to-wean subjects after cardiac surgery. Respir. Care 2015, 60, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hough, C.L.; Caldwell, E.S.; Cox, C.E.; Douglas, I.S.; Kahn, J.M.; White, D.B.; Seeley, E.J.; Bangdiwala, S.I.; Rubenfeld, G.D.; Angus, D.C.; et al. Development and Validation of a Mortality Prediction Model for Patients Receiving 14 Days of Mechanical Ventilation. Crit. Care Med. 2015, 43, 2339–2345. [Google Scholar] [CrossRef] [Green Version]
- Carson, S.S.; Kahn, J.M.; Hough, C.L.; Seeley, E.J.; White, D.B.; Douglas, I.S.; Cox, C.E.; Caldwell, E.; Bangdiwala, S.I.; Garrett, J.M.; et al. A multicenter mortality prediction model for patients receiving prolonged mechanical ventilation. Crit. Care Med. 2012, 40, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Vieillard-Baron, A.; et al. Weaning from mechanical ventilation. Eur. Respir. J. 2007, 29, 1033–1056. [Google Scholar] [CrossRef] [PubMed]
- Dettmer, M.R.; Damuth, E.; Zarbiv, S.; Mitchell, J.A.; Bartock, J.L.; Trzeciak, S. Prognostic Factors for Long-Term Mortality in Critically Ill Patients Treated With Prolonged Mechanical Ventilation: A Systematic Review. Crit. Care Med. 2017, 45, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, R.; Voicu, S.; Jaber, S.; Chousterman, B.; Paugam-Burtz, C.; Oueslati, H.; Damoisel, C.; Caillard, A.; Roquilly, A.; Feuillet, F.; et al. Tracheostomy and long-term mortality in ICU patients undergoing prolonged mechanical ventilation. PLoS ONE 2019, 14, e0220399. [Google Scholar] [CrossRef] [Green Version]
- Kojicic, M.; Li, G.; Ahmed, A.; Thakur, L.; Trillo-Alvarez, C.; Cartin-Ceba, R.; Gay, P.C.; Gajic, O. Long-term survival in patients with tracheostomy and prolonged mechanical ventilation in Olmsted County, Minnesota. Respiratory Care 2011, 56, 1765–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, O.; Shapira-Galitz, Y.; Shnipper, R.; Stavi, D.; Halperin, D.; Adi, N.; Lahav, Y. Outcome and survival following tracheostomy in patients ≥ 85 years old. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 1837–1844. [Google Scholar] [CrossRef]
- Depuydt, P.; Oeyen, S.; De Smet, S.; De Raedt, S.; Benoit, D.; Decruyenaere, J.; Derom, E. Long-term outcome and health-related quality of life in difficult-to-wean patients with and without ventilator dependency at ICU discharge: A retrospective cohort study. BMC Pulm. Med. 2016, 16, 133. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Lee, S.M.; Song, J.H.; Kim, Y.S. Clinical outcomes of difficult-to-wean patients with ventilator dependency at intensive care unit discharge. Acute Crit. Care 2020, 35, 156–163. [Google Scholar] [CrossRef] [PubMed]
- O'Connor, H.H.; White, A.C. Tracheostomy decannulation. Respir. Care 2010, 55, 1076–1081. [Google Scholar]
- Kim, H.; Yoon, J.L.; Lee, A.; Jung, Y.; Kim, M.Y.; Cho, J.J.; Ju, Y.S. Prognostic effect of body mass index to mortality in Korean older persons. Geriatr. Gerontol. Int. 2018, 18, 538–546. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, D.H.; Park, J.H.; Kim, S.; Choi, M.; Kim, H.; Seul, D.E.; Park, S.G.; Jung, J.H.; Han, K.; et al. Association between body mass index and mortality in the Korean elderly: A nationwide cohort study. PLoS ONE 2018, 13, e0207508. [Google Scholar] [CrossRef] [Green Version]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kissova, V.; Rosenberger, J.; Goboova, M.; Kiss, A. Ten-year all-cause mortality in hospitalized non-surgical patients based on nutritional status screening. Public Health Nutr. 2015, 18, 2609–2614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasimi, N.; Dabbaghmanesh, M.H.; Sohrabi, Z. Nutritional status and body fat mass: Determinants of sarcopenia in community-dwelling older adults. Exp. Gerontol. 2019, 122, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.M.; Chen, D.; Xie, X.H.; Zhang, J.E.; Zeng, Y.; Cheng, A.S. Sarcopenia as a predictor of mortality among the critically ill in an intensive care unit: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 339. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, N.; Vitacca, M. The patient needing prolonged mechanical ventilation: A narrative review. Multidiscip. Respir. Med. 2018, 13, 6. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Total (n = 124) | No HMV (n = 102) | HMV (n = 22) | p Value |
|---|---|---|---|---|
| Age (years) | 77 (68–82) | 76 (69–82) | 78 (66–83) | 0.094 |
| Male (%) | 69 (55.6) | 55 (53.9) | 14 (63.6) | 0.405 |
| Body mass index (kg/m2) | 20.8 (18.4–24.4) | 20.8 (18.5–24.3) | 20.5 (17.7–24.5) | 0.014 |
| Before admission (%) | ||||
| Nursing home or hospital | 29 (23.4) | 26 (25.5) | 3 (13.6) | 0.234 |
| Bedridden status | 29 (23.4) | 26 (25.5) | 3 (13.6) | 0.234 |
| Tube feeding | 29 (23.4) | 24 (23.5) | 5 (22.7) | 0.936 |
| SOFA score | 8.5 (6–11) | 8 (5–11) | 9 (7–11) | 0.014 |
| ProVent 14 score | 2 (2–2) | 2 (2–2) | 2 (2–3) | 0.096 |
| Charlson Comorbidity Index | 4 (3–5) | 4 (3–5) | 3.5 (3–5) | 0.383 |
| Comorbidities (%) | ||||
| Diabetes | 11 (8.9) | 7 (6.9) | 4 (18.2) | 0.105 |
| Hypertension | 12 (9.7) | 9 (8.8) | 3 (13.6) | 0.445 |
| Chronic lung disease | 12 (9.7) | 6 (5.9) | 6 (27.3) | 0.007 |
| Chronic kidney disease | 6 (4.8) | 3 (2.9) | 3 (13.6) | 0.068 |
| Chronic liver disease | 2 (1.6) | 2 (2.0) | 0 (0.0) | 1.000 |
| Cardiovascular disorder | 24 (19.4) | 19 (18.6) | 5 (22.7) | 0.766 |
| Neurological disorder | 30 (24.2) | 25 (24.5) | 5 (22.7) | 1.000 |
| Malignancy | 6 (4.8) | 6 (5.9) | 0 (0.0) | 0.590 |
| Admission via ER (%) | 109 (87.9) | 92 (90.2) | 17 (77.3) | 0.141 |
| Reason for ICU admission (%) | 0.163 | |||
| Sepsis/septic shock | 18 (14.5) | 16 (15.7) | 2 (9.1) | |
| Pneumonia | 42 (33.9) | 38 (37.3) | 4 (18.2) | |
| Cardiovascular disease | 5 (4.0) | 5 (4.9) | 0 (0.0) | |
| ARDS/acute respiratory failure | 13 (10.5) | 10 (9.8) | 3 (13.6) | |
| Post-cardiac arrest care | 35 (28.2) | 26 (25.5) | 9 (40.9) | |
| Other | 11 (8.9) | 7 (6.9) | 4 (18.2) | |
| Tracheostomy type (%) | 0.184 | |||
| Surgical tracheostomy | 91 (73.4) | 72 (70.6) | 19 (86.4) | |
| Percutaneous dilatational tracheostomy | 33 (26.6) | 30 (29.4) | 3 (13.6) | |
| Initial vital signs | ||||
| Systolic blood pressure (mmHg) | 94 (87–107) | 94 (87–106) | 95.5 (90–110) | 0.739 |
| Diastolic blood pressure (mmHg) | 54 (48–60) | 54 (48–59) | 54 (46–65) | 0.622 |
| Heart rate (/min) | 94 (82–110) | 94 (80–106) | 108 (88–126) | 0.499 |
| Respiratory rate (/min) | 22.5 (20–26) | 22 (20–26) | 24 (19–28) | 0.725 |
| Body temperature (°C) | 36.7 (36.4–37.2) | 36.7 (36.5–37.2) | 36.7 (36.2–37.2) | 0.068 |
| Oxygen saturation (%) | 97 (95–99) | 97 (95–99) | 97 (94–99) | 0.762 |
| Glasgow coma scale | 7 (5–10) | 7 (5–10) | 7 (5–10) | 0.834 |
| PaO2/FiO2 | 171 (94–254) | 177 (99–258) | 153 (74–274) | 0.149 |
| Time of MV to tracheostomy (days) | 13 (8–17) | 13 (8–18) | 13 (10–15) | 0.272 |
| Vasopressor (%) | 63 (50.8) | 50 (49.0) | 13 (59.1) | 0.391 |
| CRRT (%) | 18 (14.5) | 12 (11.8) | 6 (27.3) | 0.090 |
| Neuromuscular blocker (%) | 10 (8.1) | 7 (6.9) | 3 (13.6) | 0.383 |
| Laboratory findings | ||||
| White blood cells (×109/L) | 12.4 (8.3–17.0) | 13.1 (8.4–16.9) | 10.3 (8.3–20.6) | 0.296 |
| Platelet (×109/L) | 226 (161–308) | 225 (162–295) | 228 (132–355) | 0.647 |
| Albumin (g/dL) | 3.0 (2.6–3.5) | 3.0 (2.5–3.5) | 3.2 (2.8–3.4) | 0.029 |
| Creatinine (mg/dL) | 0.91 (0.57–1.47) | 0.87 (0.55–1.46) | 1.04 (0.70–2.25) | 0.079 |
| C-reactive protein (mg/dL) | 94 (16–182) | 87 (17–177) | 110 (11–229) | 0.074 |
| Lactic acid (mmol/L) | 1.9 (1.0–3.5) | 1.9 (1.0–3.8) | 1.6 (1.1–2.4) | 0.371 |
| At discharge (%) | ||||
| Nursing home or hospital | 100 (80.6) | 78 (76.5) | 22 (100.0) | 0.007 |
| Tube feeding | 94 (75.8) | 72 (70.6) | 22 (100.0) | 0.003 |
| Decannulation of tracheostomy tube | 25 (20.2) | 25 (24.5) | 0 (0.0) | 0.007 |
| Length of hospital stay (days) | 68 (42–106) | 72 (42–106) | 62 (40–112) | 0.136 |
| Duration of ICU stay (days) | 29 (21–52) | 26 (18–43) | 52 (31–67) | 0.228 |
| Duration of MV (days) | 22 (13–34) | 19 (12–29) | 33 (26–52) | 0.082 |
| Duration of MV and HMV (days) | 23 (13–46) | 19 (12–29) | 75 (52–102) | 0.034 |
| Variables | Total (n = 124) | No HMV (n = 102) | HMV (n = 22) | p Value |
|---|---|---|---|---|
| Primary outcome | ||||
| 1-yr mortality (%) | 59 (47.6) | 42 (41.2) | 17 (77.3) | 0.002 |
| Secondary outcomes | ||||
| 3-m mortality (%) | 29 (23.4) | 21 (20.6) | 8 (36.4) | 0.162 |
| 6-m mortality (%) | 44 (35.5) | 31 (30.4) | 13 (59.1) | 0.014 |
| Variables | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p value | HR (95% CI) | p value | |
| Age | 1.009 (0.989–1.029) | 0.388 | ||
| Male | 1.694 (0.993–2.889) | 0.053 | ||
| Body mass index | 0.917 (0.856–0.982) | 0.013 | 0.913 (0.850–0.980) | 0.012 |
| Bedridden status before admission | 1.150 (0.640–2.066) | 0.641 | ||
| Tube feeding before admission | 1.314 (0.740–2.332) | 0.352 | ||
| SOFA score | 1.080 (1.011–1.154) | 0.023 | 1.114 (1.040–1.193) | 0.002 |
| ProVent 14 score | 1.204 (0.881–1.644) | 0.244 | ||
| Charlson Comorbidity Index | 1.115 (0.971–1.279) | 0.123 | ||
| Vasopressor | 1.772 (1.048–2.995) | 0.033 | ||
| CRRT | 2.113 (1.139–3.918) | 0.018 | ||
| Neuromuscular blocker | 1.815 (0.823–4.004) | 0.140 | ||
| Transferred to a nursing facility | 6.156 (1.925–19.684) | 0.002 | 5.055 (1.558–16.400) | 0.007 |
| Tube feeding at discharge | 4.733 (1.891–11.843) | 0.001 | ||
| Decannulation of tracheostomy tube | 0.362 (0.156–0.843) | 0.018 | ||
| HMV at discharge | 2.560 (1.453–4.510) | 0.001 | 1.930 (1.082–3.444) | 0.026 |
| Length of hospital stay | 0.997 (0.993–1.001) | 0.171 | ||
| Duration of ICU stay | 1.006 (0.996–1.015) | 0.227 | ||
| Duration of MV and HMV | 1.004 (1.000–1.008) | 0.032 | ||
| Time from MV to tracheostomy | 0.993 (0.977–1.009) | 0.361 | ||
| PaO2/FiO2 | 0.999 (0.997–1.001) | 0.315 | ||
| Albumin | 0.619 (0.406–0.946) | 0.027 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.-Y.; Baek, M.S. Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge. J. Pers. Med. 2021, 11, 1257. https://doi.org/10.3390/jpm11121257
Kim W-Y, Baek MS. Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge. Journal of Personalized Medicine. 2021; 11(12):1257. https://doi.org/10.3390/jpm11121257
Chicago/Turabian StyleKim, Won-Young, and Moon Seong Baek. 2021. "Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge" Journal of Personalized Medicine 11, no. 12: 1257. https://doi.org/10.3390/jpm11121257
APA StyleKim, W. -Y., & Baek, M. S. (2021). Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge. Journal of Personalized Medicine, 11(12), 1257. https://doi.org/10.3390/jpm11121257