

Identification of Patients with Potential Atrial Fibrillation during Sinus Rhythm Using Isolated P Wave Characteristics from 12-Lead ECGs

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
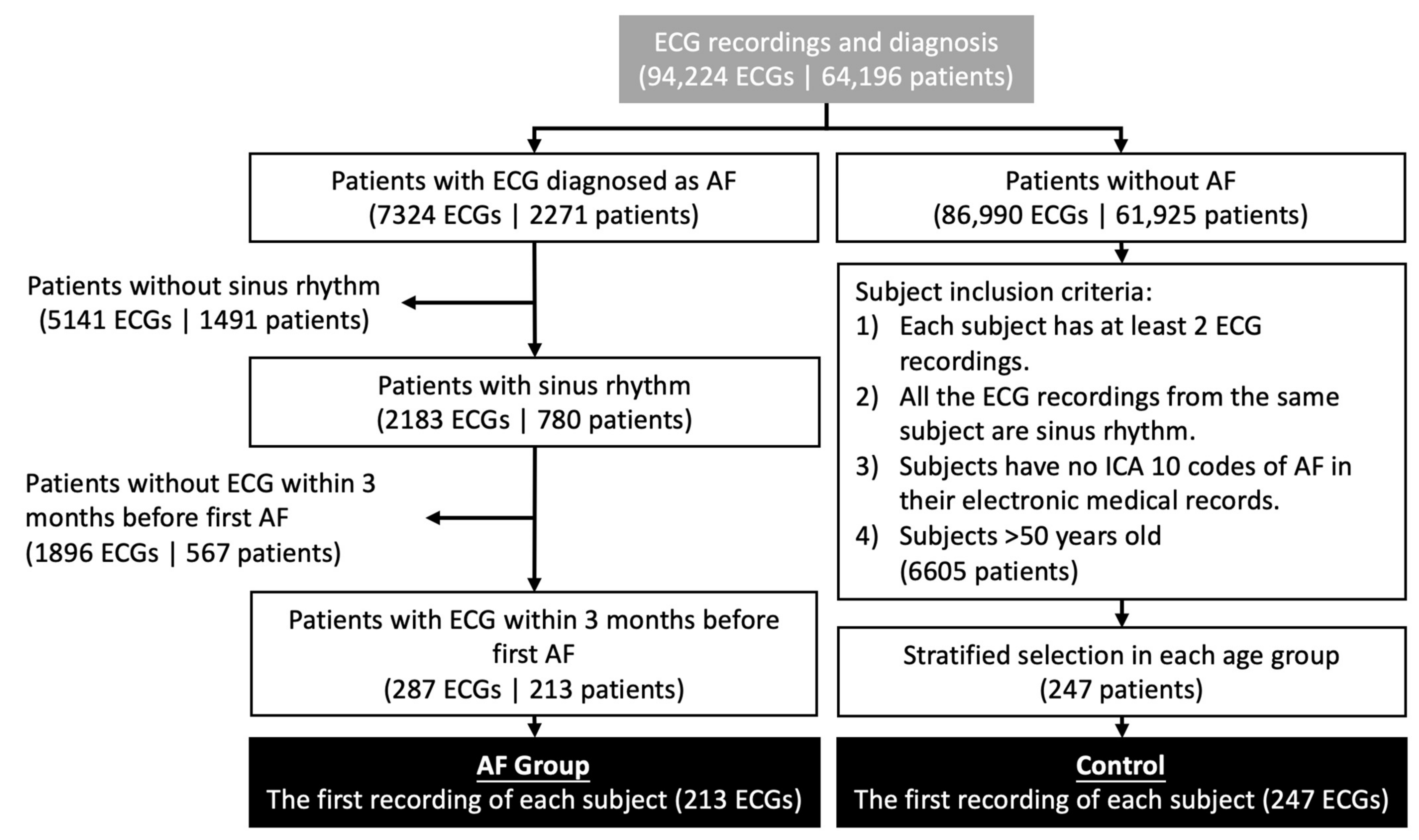
2.1. Subject Selection
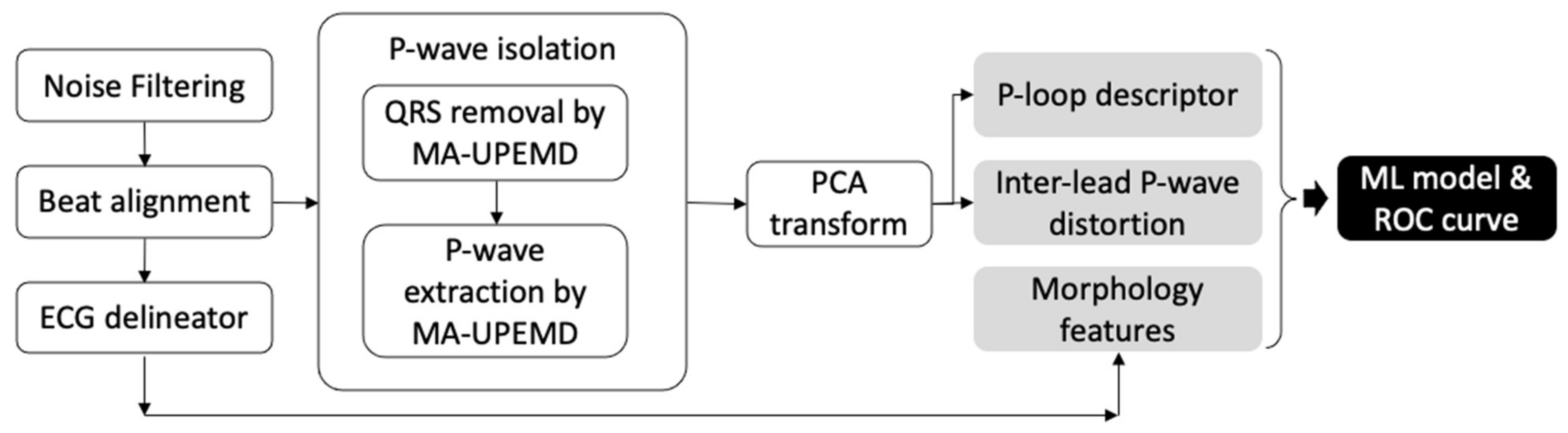
2.2. ECG Signal Processing
2.2.1. Noise Filtering
2.2.2. ECG Delineation
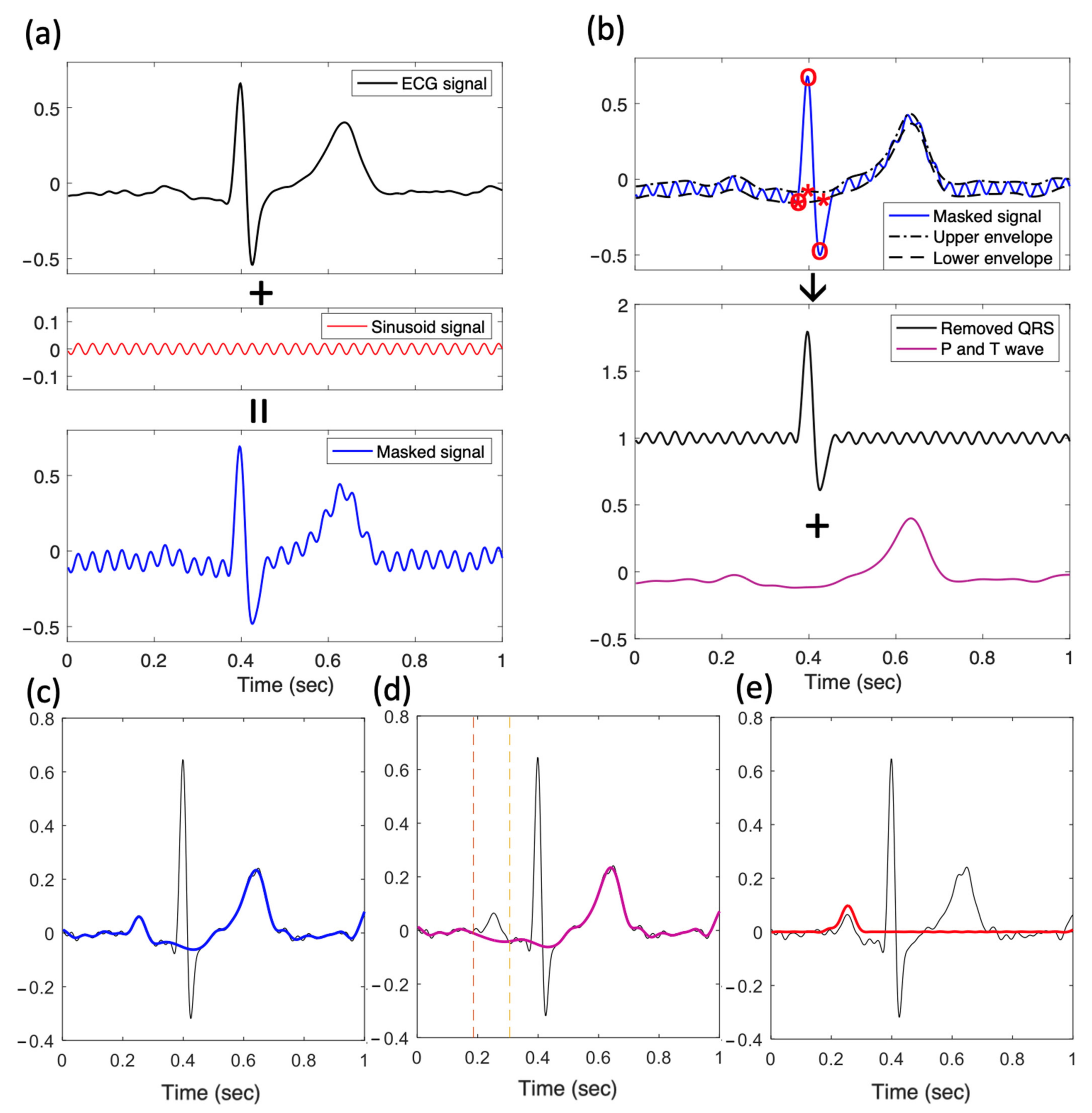
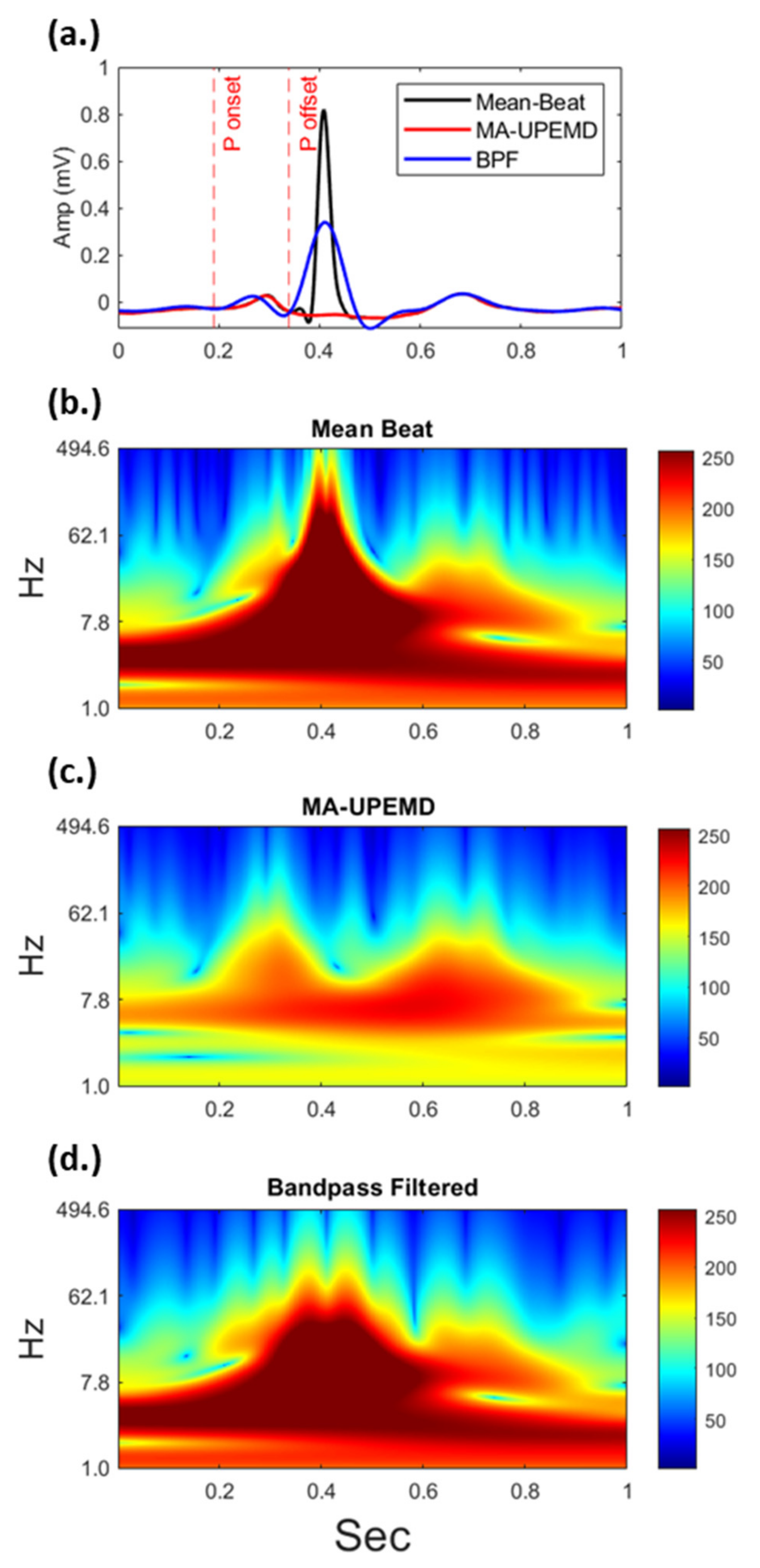
2.2.3. P Wave Extraction Using Minimum-Arclength Uniform Phase Empirical Mode Decomposition (MA-UPEMD)
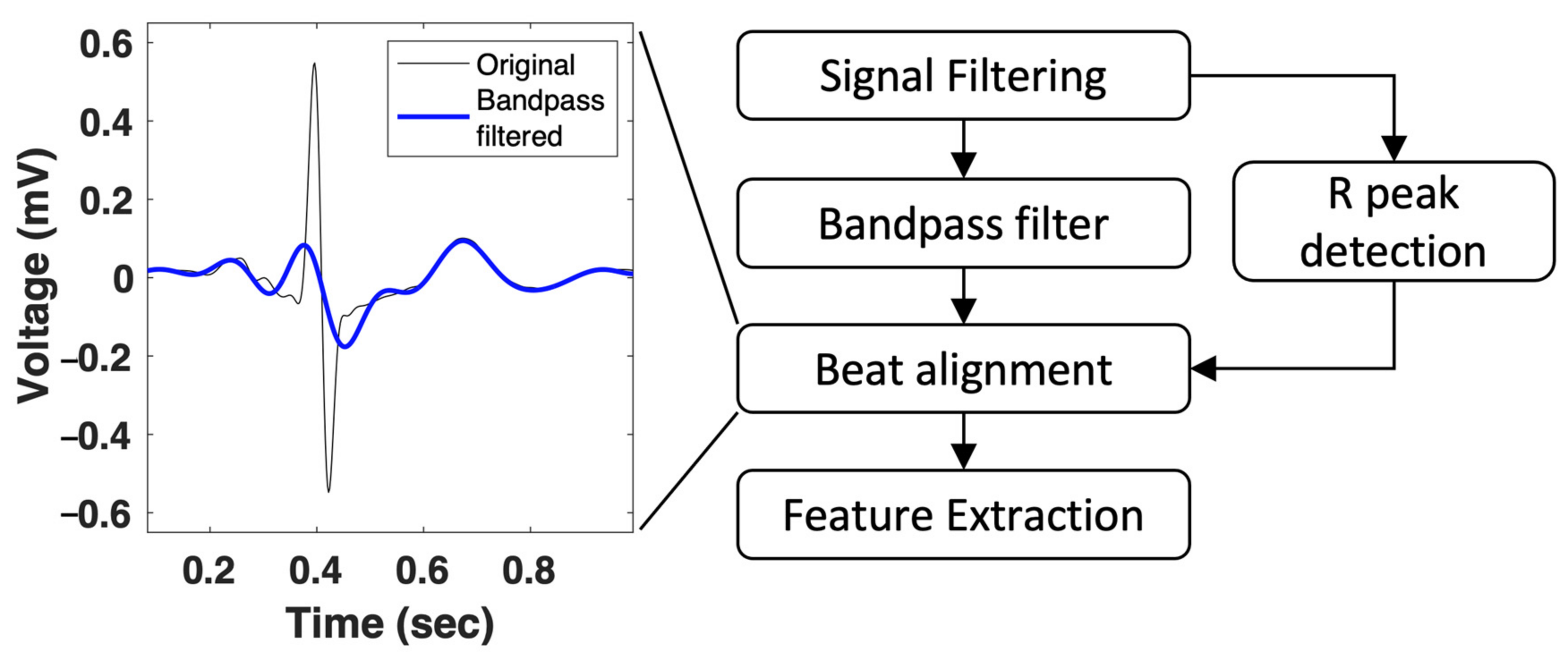
2.2.4. P Wave Extraction Using Bandpass Filter
2.3. Feature Extraction
2.3.1. ECG Morphology Features
- Wave amplitude: the amplitudes of the P, Q, S, and T waves were defined by their peaks.
- P duration: we calculated the duration of the P wave as the time between onset and offset.
- Intervals: traditionally, ECG features are calculated and include the duration between P-onset and R-onset (PR interval), that between Q onset and J point (QRS duration), and that between Q onset and T offset (QT interval).
- ST-voltage: the height of the ECG segment between the J point and T onset, which is usually used for the diagnosis of myocardial infarction, was used. The average voltage between the two points was calculated (STvol_R).
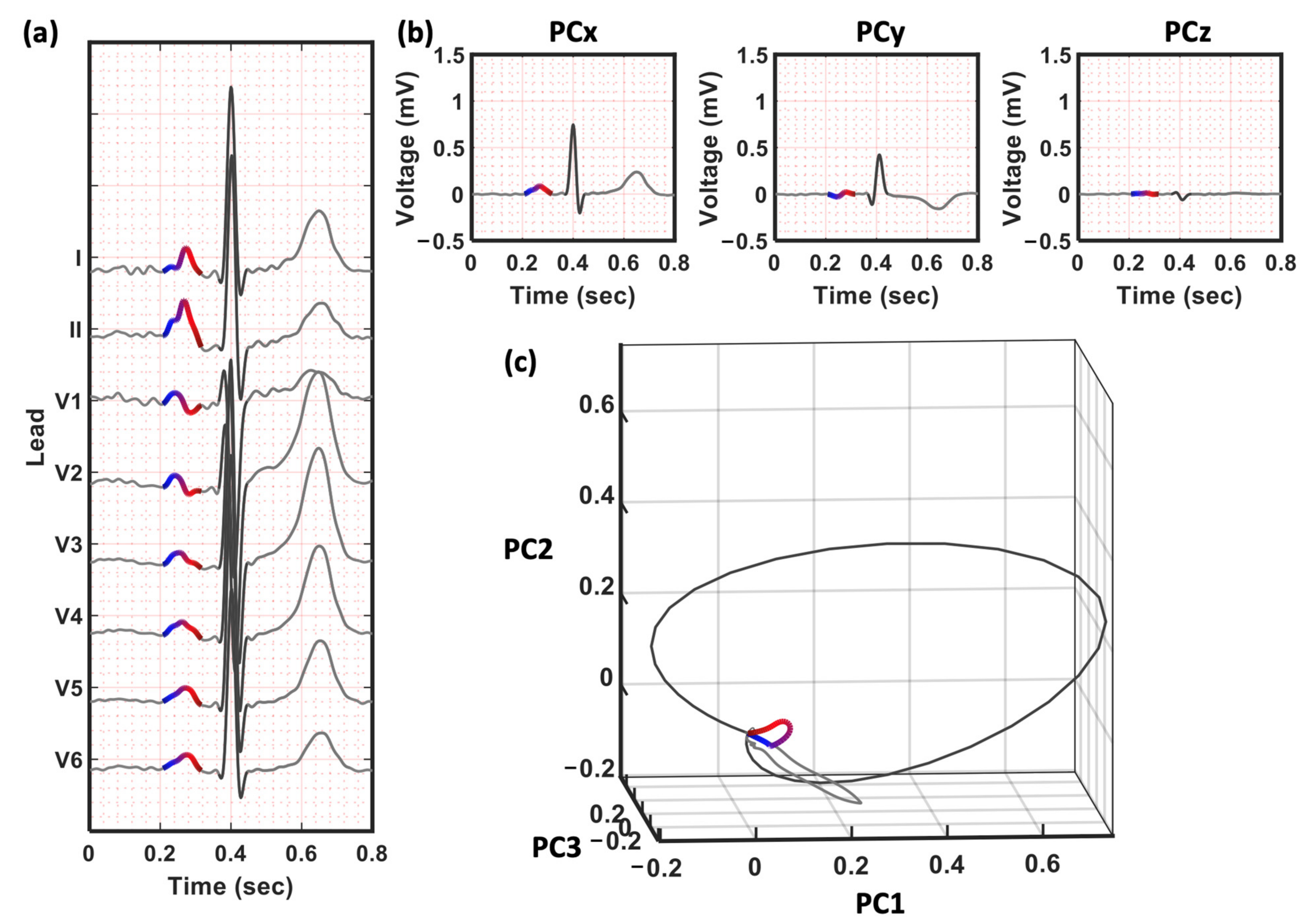
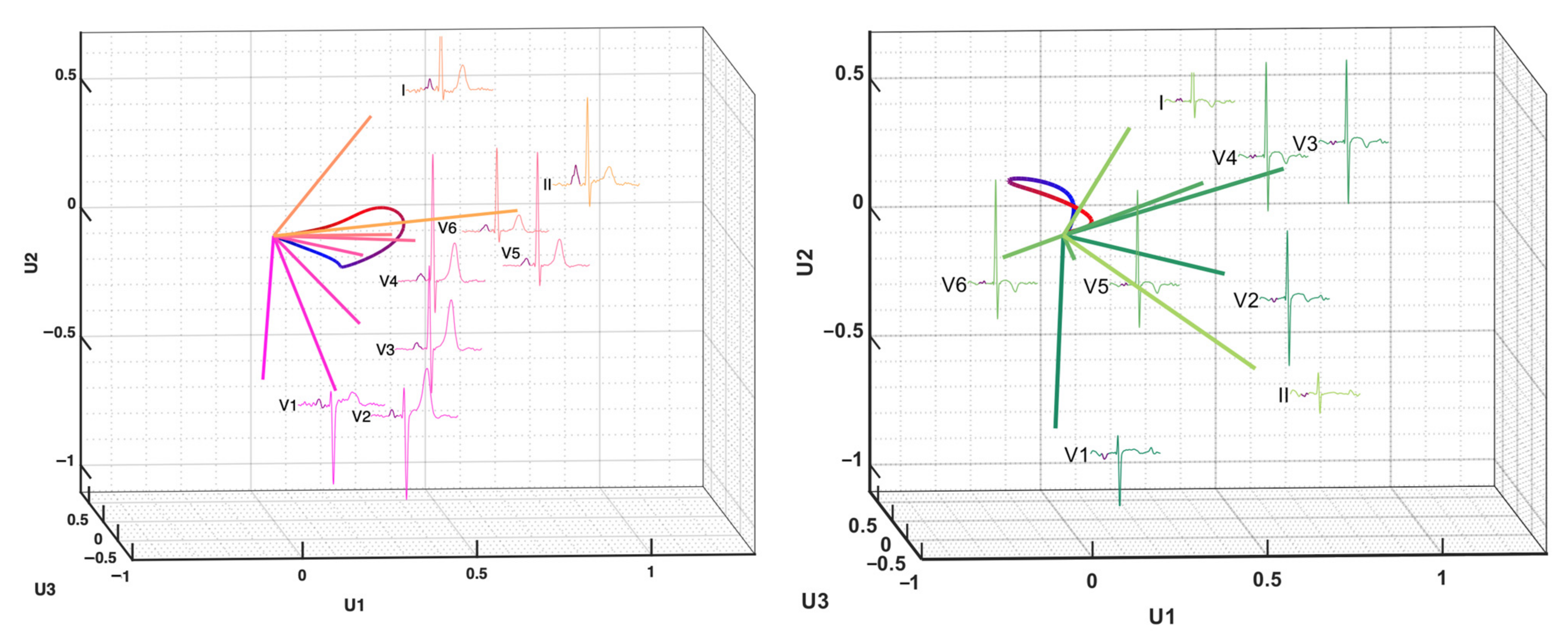
2.3.2. P Wave Projection by Principal Component Analysis (PCA)
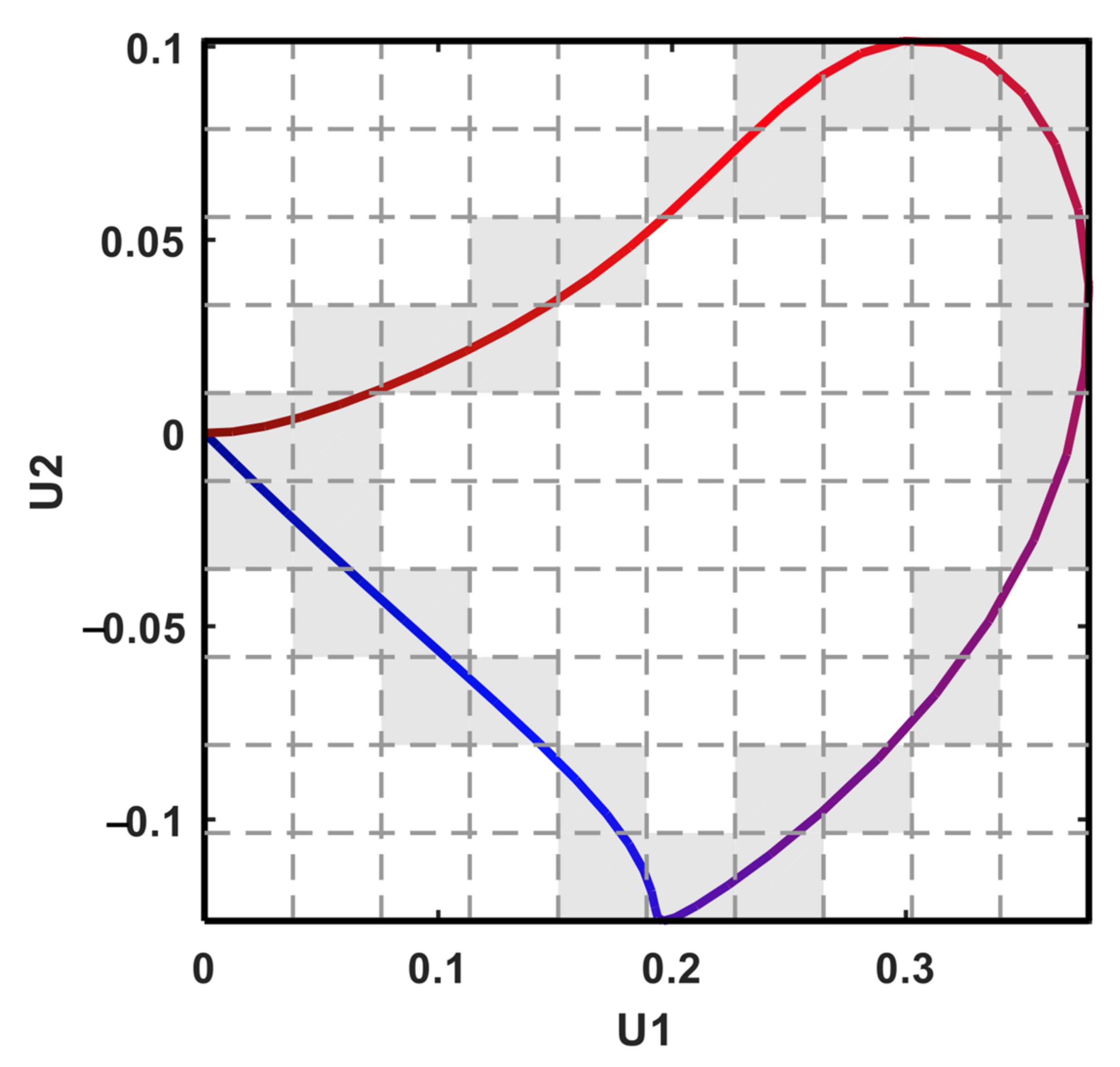
2.3.3. P-Loop Descriptors
2.3.4. Inter-Lead P Wave Dispersion
2.4. Classification of Patients with AF
2.4.1. ML Model in AF Prediction
2.4.2. Feature Importance
2.4.3. Comparison with DL
3. Results
3.1. Comparison of P Wave Signals Extracted by MA-UPEMD and Band-Pass Filter
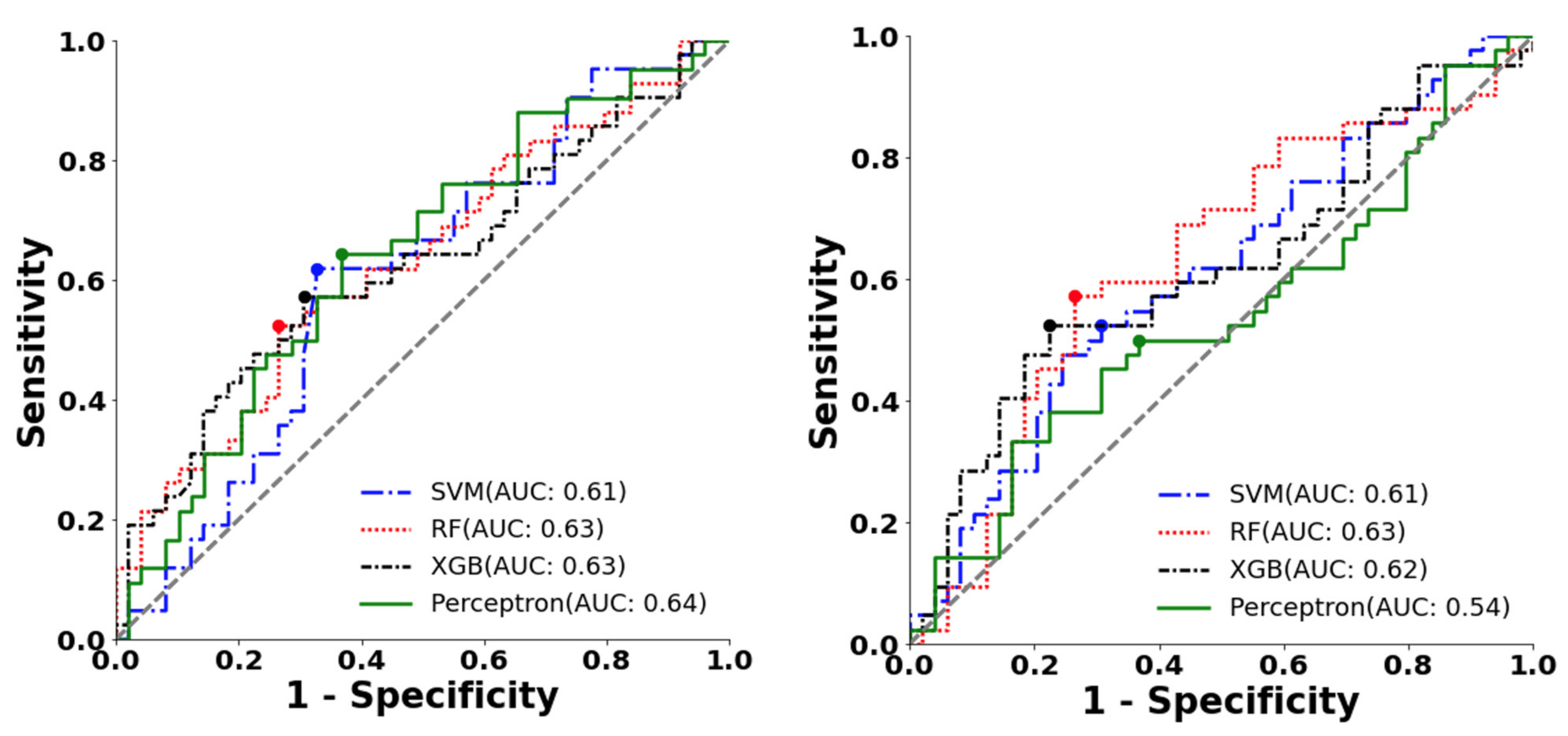
3.2. Prediction of AF Using Different P Wave Extraction and ML Models
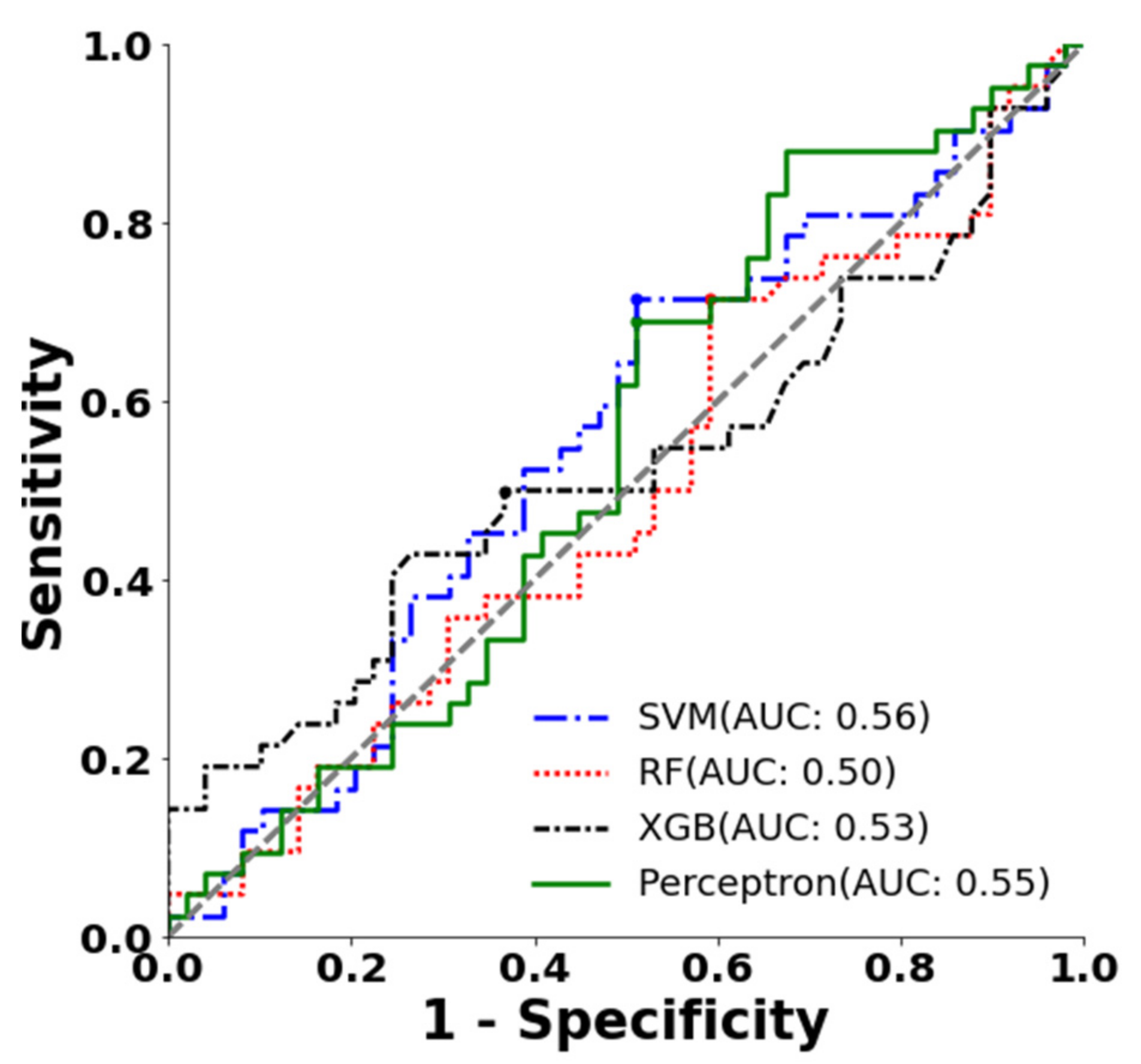
3.3. Classification with Only P Wave Amplitude and Duration
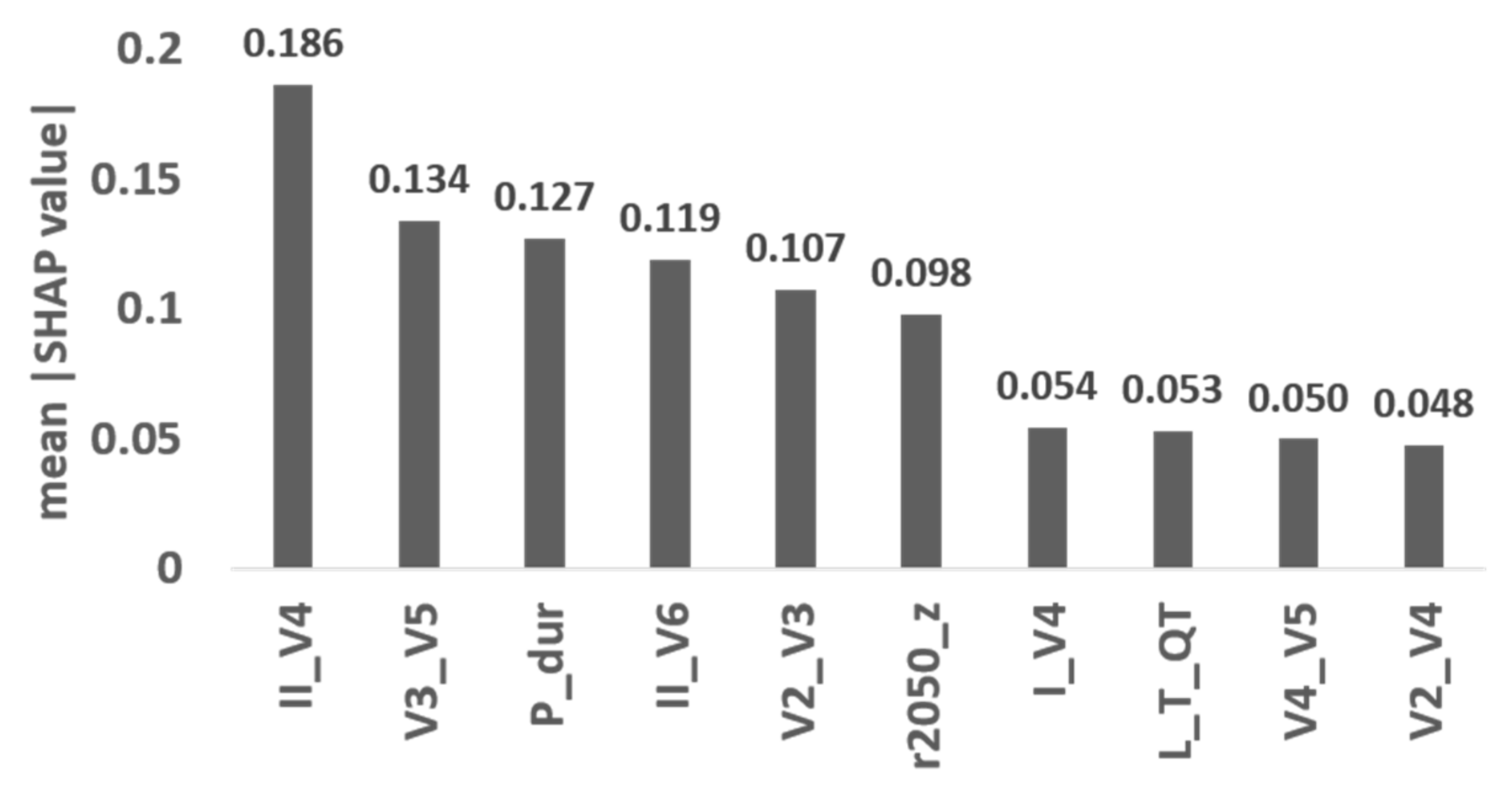
3.4. Feature Importance
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zulkifly, H.; Lip, G.Y.H.; Lane, D.A. Epidemiology of Atrial Fibrillation. Int. J. Clin. Pract. 2018, 72, e13070. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Wolf, P.A.; D’Agostino, R.B.; Silbershatz, H.; Kannel, W.B.; Levy, D. Impact of Atrial Fibrillation on the Risk of Death. Circulation 1998, 98, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Oladiran, O.; Nwosu, I. Stroke Risk Stratification in Atrial Fibrillation: A Review of Common Risk Factors. J. Commun. Hosp. Intern. Med. Perspect. 2019, 9, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial Fibrillation as an Independent Risk Factor for Stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef]
- Chiang, C.-E.; Wu, T.-J.; Ueng, K.-C.; Chao, T.-F.; Chang, K.-C.; Wang, C.-C.; Lin, Y.-J.; Yin, W.-H.; Kuo, J.-Y.; Lin, W.-S.; et al. 2016 Guidelines of the Taiwan Heart Rhythm Society and the Taiwan Society of Cardiology for the Management of Atrial Fibrillation. J. Formos. Med. Assoc. 2016, 115, 893–952. [Google Scholar] [CrossRef]
- Turakhia, M.P.; Ullal, A.J.; Hoang, D.D.; Than, C.T.; Miller, J.D.; Friday, K.J.; Perez, M.V.; Freeman, J.V.; Wang, P.J.; Heidenreich, P.A. Feasibility of Extended Ambulatory Electrocardiogram Monitoring to Identify Silent Atrial Fibrillation in High-Risk Patients: The Screening Study for Undiagnosed Atrial Fibrillation (STUDY-AF). Clin. Cardiol. 2015, 38, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Waalen, J.; Edwards, A.M.; Ariniello, L.M.; Mehta, R.R.; Ebner, G.S.; Carter, C.; Baca-Motes, K.; Felicione, E.; Sarich, T.; et al. Effect of a Home-Based Wearable Continuous ECG Monitoring Patch on Detection of Undiagnosed Atrial Fibrillation: The MSToPS Randomized Clinical Trial. JAMA 2018, 320, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-H.; Lin, C.; Chang, H.-C.; Liu, C.-C.; Serafico, B.M.F.; Wu, L.-C.; Lin, C.-T.; Hsu, T.; Huang, C.-Y.; Lo, M.-T. Cloud-Based Artificial Intelligence System for Large-Scale Arrhythmia Screening. Computer 2019, 52, 40–51. [Google Scholar] [CrossRef]
- Turakhia, M.P.; Desai, M.; Hedlin, H.; Rajmane, A.; Talati, N.; Ferris, T.; Desai, S.; Nag, D.; Patel, M.; Kowey, P.; et al. Rationale and Design of a Large-Scale, App-Based Study to Identify Cardiac Arrhythmias Using a Smartwatch: The Apple Heart Study. Am. Heart J. 2019, 207, 66–75. [Google Scholar] [CrossRef]
- Savelieva, I.; Camm, A.J. Clinical Relevance of Silent Atrial Fibrillation: Prevalence, Prognosis, Quality of Life, and Management. J. Interv. Card Electrophysiol. 2000, 4, 369–382. [Google Scholar] [CrossRef]
- Kottkamp, H.; Hügl, B.; Krauss, B.; Wetzel, U.; Fleck, A.; Schuler, G.; Hindricks, G. Electromagnetic Versus Fluoroscopic Mapping of the Inferior Isthmus for Ablation of Typical Atrial Flutter. Circulation 2000, 102, 2082–2086. [Google Scholar] [CrossRef] [PubMed]
- Raghunath, S.; Pfeifer, J.M.; Ulloa-Cerna, A.E.; Nemani, A.; Carbonati, T.; Jing, L.; vanMaanen, D.P.; Hartzel, D.N.; Ruhl, J.A.; Lagerman, B.F.; et al. Deep Neural Networks Can Predict New-Onset Atrial Fibrillation from the 12-Lead ECG and Help Identify Those at Risk of Atrial Fibrillation–Related Stroke. Circulation 2021, 143, 1287–1298. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An Artificial Intelligence-Enabled ECG Algorithm for the Identification of Patients with Atrial Fibrillation during Sinus Rhythm: A Retrospective Analysis of Outcome Prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef]
- Khurshid, S.; Friedman, S.; Reeder, C.; Di Achille, P.; Diamant, N.; Singh, P.; Harrington, L.X.; Wang, X.; Al-Alusi, M.A.; Sarma, G.; et al. ECG-Based Deep Learning and Clinical Risk Factors to Predict Atrial Fibrillation. Circulation 2022, 145, 122–133. [Google Scholar] [CrossRef]
- Christopoulos, G.; Graff-Radford, J.; Lopez, C.L.; Yao, X.; Attia, Z.I.; Rabinstein, A.A.; Petersen, R.C.; Knopman, D.S.; Mielke, M.M.; Kremers, W.; et al. Artificial Intelligence–Electrocardiography to Predict Incident Atrial Fibrillation. Circ. Arrhythm. Electrophysiol. 2020, 13, e009355. [Google Scholar] [CrossRef]
- Yang, H.-W.; Jeng, S.-K.; Young, H.-W.V.; Lin, C.; Wang, Y.-H.; Hu, K.; Lo, M.-T. A Minimum Arclength Method for Removing Spikes in Empirical Mode Decomposition. IEEE Access 2019, 7, 13284–13294. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Yeh, C.-H.; Young, H.-W.V.; Hu, K.; Lo, M.-T. On the Computational Complexity of the Empirical Mode Decomposition Algorithm. Phys. A Stat. Mech. Its Appl. 2014, 400, 159–167. [Google Scholar] [CrossRef]
- Laguna, P.; Jané, R.; Caminal, P. Automatic Detection of Wave Boundaries in Multilead ECG Signals: Validation with the CSE Database. Comput. Biomed. Res. 1994, 27, 45–60. [Google Scholar] [CrossRef]
- Deering, R.; Kaiser, J.F. The Use of a Masking Signal to Improve Empirical Mode Decomposition. In Proceedings of the IEEE International Conference on Acoustics, Speech, and Signal Processing, (ICASSP’05), Philadelphia, PA, USA, 23 March 2005; Volume 484, pp. iv/485–iv/488. [Google Scholar]
- Wang, Y.-H.; Hu, K.; Lo, M.-T. Uniform Phase Empirical Mode Decomposition: An Optimal Hybridization of Masking Signal and Ensemble Approaches. IEEE Access 2018, 6, 34819–34833. [Google Scholar] [CrossRef]
- Rilling, G.; Flandrin, P. One or Two Frequencies? The Empirical Mode Decomposition Answers. IEEE Trans. Signal. Process. 2008, 56, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.-H.; Young, H.-W.V.; Lo, M.-T. The Inner Structure of Empirical Mode Decomposition. Phys. Stat. Mech. Its Appl. 2016, 462, 1003–1017. [Google Scholar] [CrossRef]
- Hsieh, W.-H.; Lin, C.-Y.; Te, A.L.D.; Lo, M.-T.; Wu, C.-I.; Chung, F.-P.; Chang, Y.-C.; Chang, S.-L.; Lin, C.; Lo, L.-W.; et al. A Novel Noninvasive Surface ECG Analysis Using Interlead QRS Dispersion in Arrhythmogenic Right Ventricular Cardiomyopathy. PLoS ONE 2017, 12, e0182364. [Google Scholar] [CrossRef] [PubMed]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. arXiv 2018, arXiv:1201.0490. Available online: https://doi.org/10.48550/arXiv.1201.0490 (accessed on 13 May 2022).
- Lundberg, S.M.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. Adv. Neural Inf. Process. Syst. 2017, 30, 4768–4777. [Google Scholar]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; Balasubramanian, V.; Russo, A.M.; Rajmane, A.; Cheung, L.; et al. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N. Engl. J. Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef] [PubMed]
- Mant, J.; Edwards, D. Stroke Prevention in Atrial Fibrillation. Drugs Aging 2010, 27, 859–870. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Ziegler, P.D.; Schmitt, S.K.; Chang, Y.; Fan, J.; Than, C.T.; Keung, E.K.; Singer, D.E. Atrial Fibrillation Burden and Short-Term Risk of Stroke. Circ. Arrhythm. Electrophysiol. 2015, 8, 1040–1047. [Google Scholar] [CrossRef]
- Allessie, M.A.; Konings, K.; Kirchhof, C.J.H.J.; Wijffels, M. Electrophysiologic Mechanisms of Perpetuation of Atrial Fibrillation. Am. J. Cardiol. 1996, 77, 10A–23A. [Google Scholar] [CrossRef]
- Hari, K.J.; Nguyen, T.P.; Soliman, E.Z. Relationship between P-Wave Duration and the Risk of Atrial Fibrillation. Expert Rev. Cardiovasc. Ther. 2018, 16, 837–843. [Google Scholar] [CrossRef]
- Chao, T.-F.; Liu, C.-J.; Tuan, T.-C.; Chen, T.-J.; Hsieh, M.-H.; Lip, G.Y.H.; Chen, S.-A. Lifetime Risks, Projected Numbers, and Adverse Outcomes in Asian Patients with Atrial Fibrillation: A Report from the Taiwan Nationwide AF Cohort Study. Chest 2018, 153, 453–466. [Google Scholar] [CrossRef]
- Turakhia, M.P.; Hoang, D.D.; Zimetbaum, P.; Miller, J.D.; Froelicher, V.F.; Kumar, U.N.; Xu, X.; Yang, F.; Heidenreich, P.A. Diagnostic Utility of a Novel Leadless Arrhythmia Monitoring Device. Am. J. Cardiol. 2013, 112, 520–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Feature Name | Description |
|---|---|---|
| P Wave | P_dur | P wave duration. |
| Morphology | L_AMP_X, C_AMP_X X may be P, Q, R, S, or T | Mean of P, Q, R, S, or T wave amplitude on limb leads and chest leads. |
| L_T_X, C_T_X X: PR, QRS or QT | Mean of PR, QRS, or QT interval on limb leads and chest leads. | |
| L_STvol_R, C_STvol_R | Average voltage of ST segment on limb leads and chest leads. | |
| Principal component | PC1w, PC2w, PC3w | Weight of eigenvalues from PC1, PC2 and PC3. |
| Inter-lead P wave dispersion | I_II, II_V1, V1_V2, V2_V3, V3_V4, V4_V5, V5_V6, I_V1, II_V2, V1_V3, V2_V4, V3_V5, V4_V6, I_V2, II_V3, V1_V4, V2_V5, V3_V6, I_V3, II_V4, V1_V5, V2_V6, I_V4, II_V5, V1_V6, I_V5, II_V6, I_V6 | P-loop angle between two leads. |
| Loop analysis | LoopArea | Area of P-loop. |
| LoopLength | Length of P-loop | |
| LAratio | Ratio of P-loop length and area | |
| Frequency analysis | r2050_PC1, r2050_PC2, r2050_PC3 | The ratio between the total power in frequency bands 20–50 Hz and 1–20 Hz |
| Model | Method | AUC | Accuracy | Sensitivity | Specificity | Precision | F1 |
|---|---|---|---|---|---|---|---|
| SVM | MA-UPEMD | 0.61 | 0.58 | 0.67 | 0.51 | 0.55 | 0.60 |
| BP-filter | 0.61 | 0.55 | 0.62 | 0.49 | 0.51 | 0.56 | |
| Random forest | MA-UPEMD | 0.63 | 0.59 | 0.57 | 0.61 | 0.56 | 0.56 |
| BP-filter | 0.63 | 0.60 | 0.64 | 0.57 | 0.56 | 0.60 | |
| XGBoost | MA-UPEMD | 0.63 | 0.62 | 0.48 | 0.74 | 0.61 | 0.53 |
| BP-filter | 0.62 | 0.50 | 0.50 | 0.50 | 0.46 | 0.48 | |
| Perceptron | MA-UPEMD | 0.64 | 0.58 | 0.71 | 0.47 | 0.54 | 0.61 |
| BP-filter | 0.54 | 0.51 | 0.50 | 0.51 | 0.47 | 0.48 | |
| CNN | 0.51 | 0.54 | 0.57 | 0.52 | 0.50 | 0.53 |
| Model | AUC | Accuracy | Sensitivity | Specificity | Precision | F1 |
|---|---|---|---|---|---|---|
| SVM | 0.56 | 0.56 | 0.52 | 0.59 | 0.52 | 0.52 |
| Random forest | 0.50 | 0.48 | 0.43 | 0.53 | 0.44 | 0.43 |
| XGBoost | 0.53 | 0.59 | 0.43 | 0.74 | 0.58 | 0.49 |
| Perceptron | 0.55 | 0.56 | 0.62 | 0.51 | 0.52 | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.-W.; Hsiao, C.-Y.; Peng, Y.-Q.; Lin, T.-Y.; Tsai, L.-W.; Lin, C.; Lo, M.-T.; Shih, C.-M. Identification of Patients with Potential Atrial Fibrillation during Sinus Rhythm Using Isolated P Wave Characteristics from 12-Lead ECGs. J. Pers. Med. 2022, 12, 1608. https://doi.org/10.3390/jpm12101608
Yang H-W, Hsiao C-Y, Peng Y-Q, Lin T-Y, Tsai L-W, Lin C, Lo M-T, Shih C-M. Identification of Patients with Potential Atrial Fibrillation during Sinus Rhythm Using Isolated P Wave Characteristics from 12-Lead ECGs. Journal of Personalized Medicine. 2022; 12(10):1608. https://doi.org/10.3390/jpm12101608
Chicago/Turabian StyleYang, Hui-Wen, Cheng-Yi Hsiao, Yu-Qi Peng, Tse-Yu Lin, Lung-Wen Tsai, Chen Lin, Men-Tzung Lo, and Chun-Ming Shih. 2022. "Identification of Patients with Potential Atrial Fibrillation during Sinus Rhythm Using Isolated P Wave Characteristics from 12-Lead ECGs" Journal of Personalized Medicine 12, no. 10: 1608. https://doi.org/10.3390/jpm12101608
APA StyleYang, H. -W., Hsiao, C. -Y., Peng, Y. -Q., Lin, T. -Y., Tsai, L. -W., Lin, C., Lo, M. -T., & Shih, C. -M. (2022). Identification of Patients with Potential Atrial Fibrillation during Sinus Rhythm Using Isolated P Wave Characteristics from 12-Lead ECGs. Journal of Personalized Medicine, 12(10), 1608. https://doi.org/10.3390/jpm12101608