
Determinants of Treatment Benefit and Post-Treatment Survival for Patients with Hepatocellular Carcinoma Enrolled in Second-Line Trials after the Failure of Sorafenib Treatment

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
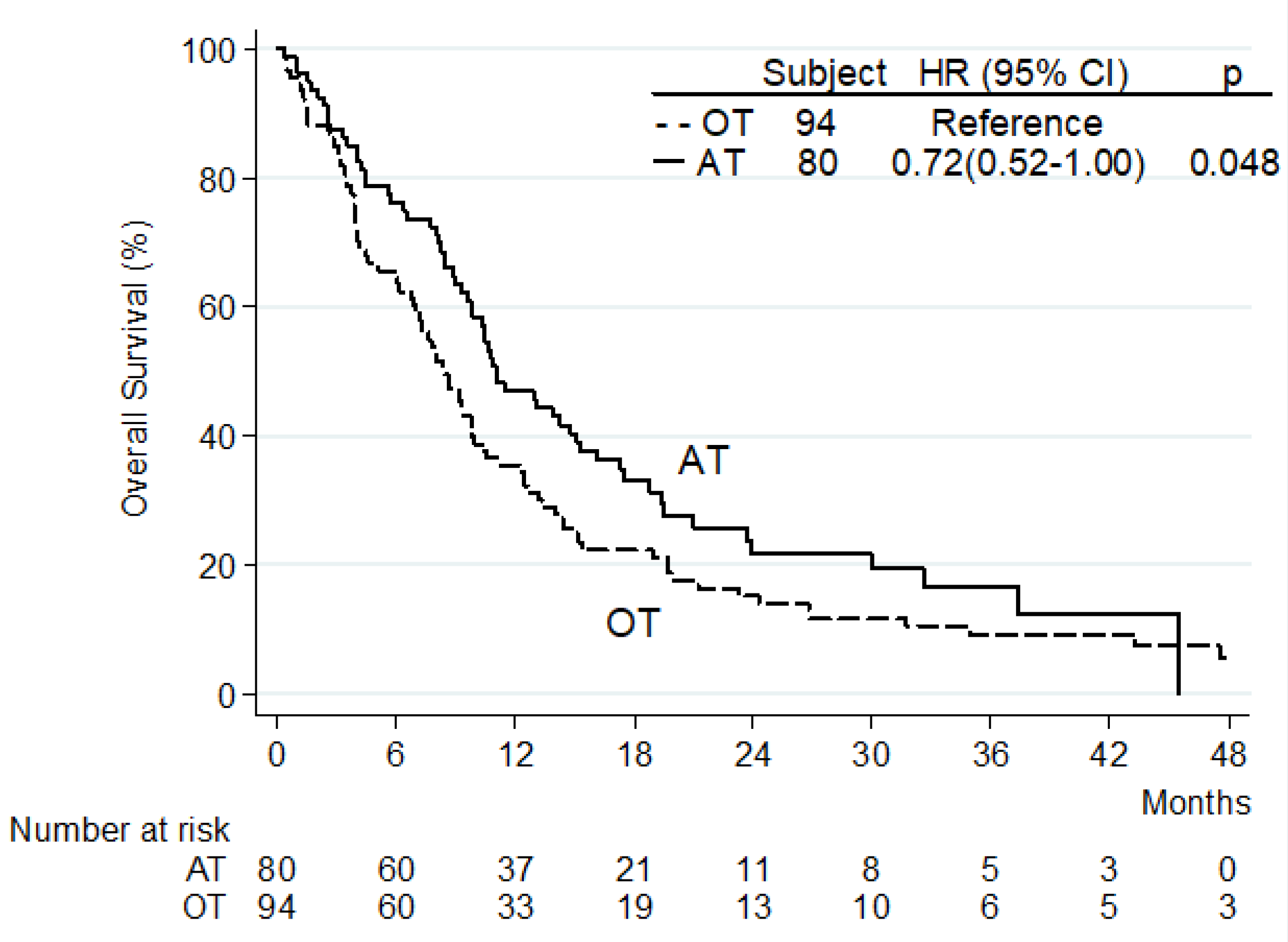
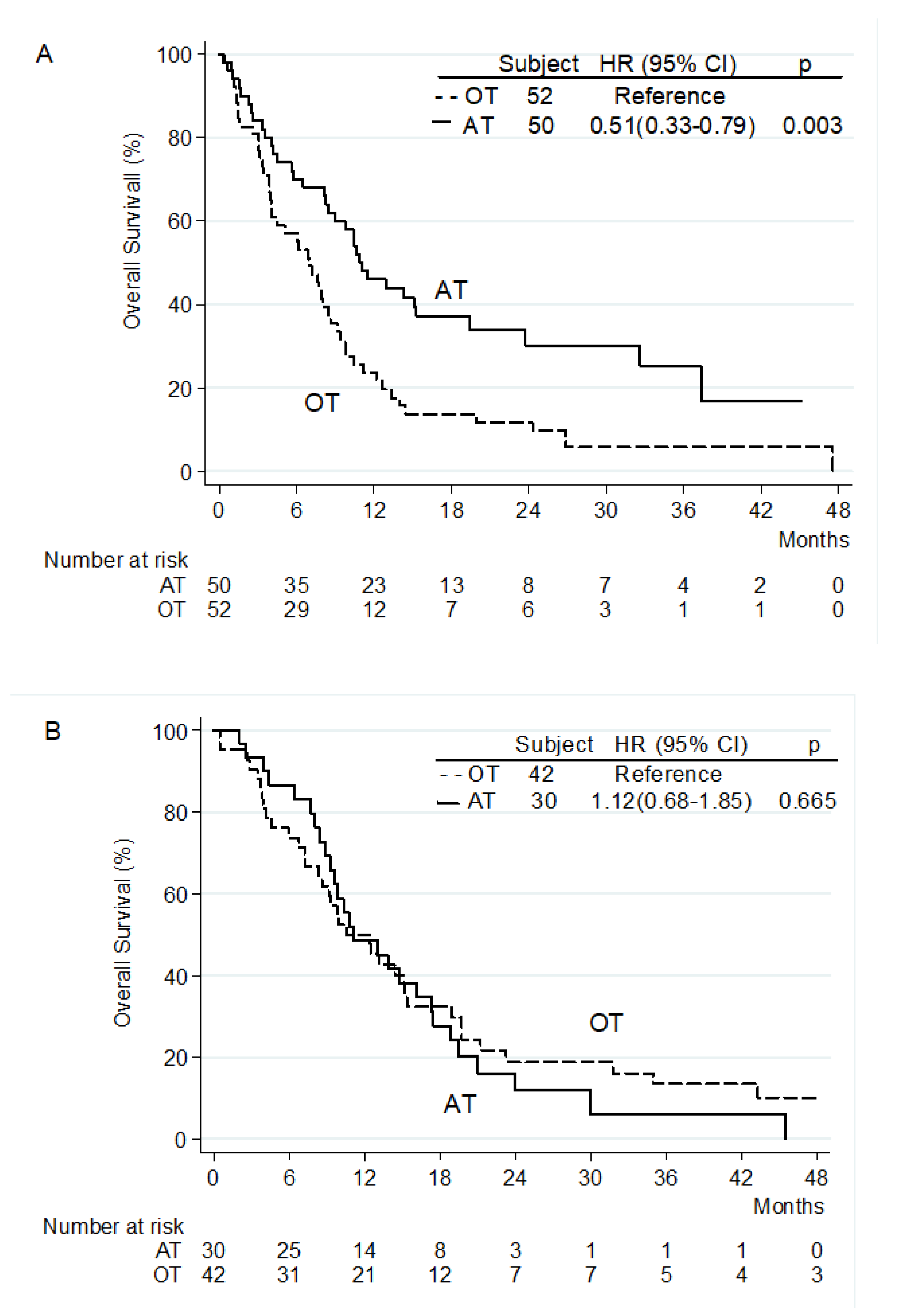
3.2. Overall Survival from the Beginning of Second-Line Treatment
3.3. Overall Survival from Start of Sorafenib
3.4. Time to Treatment Failure from Start of Second-Line Treatment
3.5. Post-Second-Line Treatment Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vogel, A.; Meyer, T.; Sapisochin, G. Hepatocellular carcinoma. Lancet 2022. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Finn, R.S.; Qin, S. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Qin, S.; Merle, P. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cheng, A.L.; Qin, S.; Ikeda, M. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.; Xu, J.; Bai, Y. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): A randomised, open-label, phase 2-3 study. Lancet Oncol. 2021, 22, 977–990. [Google Scholar] [CrossRef]
- Qin, S.; Chan, L.S.; Gu, S. Camrelizumab (C) plus rivoceranib (R) vs. sorafenib (S) as first-line therapy for unresectable hepatocellular carcinoma (uHCC): A randomized, phase III trial. Ann. Oncol. 2022, 33 (Suppl. 7), S808–S869. [Google Scholar] [CrossRef]
- Qin, S.; Kudo, M.; Meyer, T. Final analysis of RATIONALE-301: Randomized, phase III study of tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Ann. Oncol. 2022, 33 (Suppl. 7), S808–S869. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evid. 2022. [Google Scholar] [CrossRef]
- Kelley, R.K.; Rimassa, L.; Cheng, A.L. Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2022, 23, 995–1008. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Yau, T.; Kang, Y.K.; Kim, T.Y. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients With Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib: The CheckMate 040 Randomized Clinical Trial. JAMA Oncol. 2020, 6, e204564. [Google Scholar] [CrossRef]
- Finn, R.S.; Ryoo, B.Y.; Merle, P. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Chen, Z.; Fang, W. Pembrolizumab plus best supportive care versus placebo plus best supportive care as second-line therapy in patients in Asia with advanced hepatocellular carcinoma (HCC): Phase 3 KEYNOTE-394 study. J. Clin. Oncol. 2022, 40 (Suppl. 4). [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Hepatobiliary Cancers. Version 1.2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf (accessed on 1 September 2022).
- Johnson, P.J.; Berhane, S.; Kagebayashi, C. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Alsina, A.; Kudo, M.; Vogel, A. Effects of Subsequent Systemic Anticancer Medication Following First-Line Lenvatinib: A Post Hoc Responder Analysis from the Phase 3 REFLECT Study in Unresectable Hepatocellular Carcinoma. Liver Cancer. 2020, 9, 93–104. [Google Scholar] [CrossRef]
- Iavarone, M.; Cabibbo, G.; Biolato, M. Predictors of survival in patients with advanced hepatocellular carcinoma who permanently discontinued sorafenib. Hepatology 2015, 62, 784–791. [Google Scholar] [CrossRef]
- Facciorusso, A.; Abd El Aziz, M.A.; Sacco, R. Efficacy of Regorafenib in Hepatocellular Carcinoma Patients: A Systematic Review and Meta-Analysis. Cancers (Basel) 2019, 12, 36. [Google Scholar] [CrossRef] [Green Version]
- Pfister, D.; Núñez, N.G.; Pinyol, R. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature 2021, 592, 450–456. [Google Scholar] [CrossRef]
- Kirstein, M.M.; Scheiner, B.; Marwede, T. Sequential systemic treatment in patients with hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2020, 52, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.Y.; Wu, C.H.; Lu, L.C. Prognosis of patients with advanced hepatocellular carcinoma who failed first-line systemic therapy. J. Hepatol. 2014, 60, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Personeni, N.; Giordano, L.; Abbadessa, G. Prognostic value of the neutrophil-to-lymphocyte ratio in the ARQ 197-215 second-line study for advanced hepatocellular carcinoma. Oncotarget 2017, 8, 14408–14415. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Cheng, A.L.; Meinhardt, G. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Gong, Y.; Zhang, Q. Prognostic Roles of Blood Inflammatory Markers in Hepatocellular Carcinoma Patients Taking Sorafenib. A Systematic Review and Meta-Analysis. Front. Oncol. 2020, 9, 1557. [Google Scholar] [CrossRef]
- Choi, W.M.; Kim, J.Y.; Choi, J. Kinetics of the neutrophil-lymphocyte ratio during PD-1 inhibition as a prognostic factor in advanced hepatocellular carcinoma. Liver Int. 2021, 41, 2189–2199. [Google Scholar] [CrossRef]
- Song, W.; Tian, C.; Wang, K. The pretreatment lymphocyte to monocyte ratio predicts clinical outcome for patients with hepatocellular carcinoma: A meta-analysis. Sci. Rep. 2017, 7, 46601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, T.; Zhu, J.; Zhao, L. Lymphocyte to monocyte ratio and neutrophil to lymphocyte ratio are superior inflammation-based predictors of recurrence in patients with hepatocellular carcinoma after hepatic resection. J. Surg. Oncol. 2017, 115, 718–728. [Google Scholar] [CrossRef]
- Wang, W.; Tsuchiya, K.; Kurosaki, M. Sorafenib-regorafenib sequential therapy in Japanese patients with unresectable hepatocellular carcinoma—Relative dose intensity and post-regorafenib therapies in real world practice. Cancers (Basel) 2019, 11, 1517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finn, R.S.; Merle, P.; Granito, A. Outcomes of sequential treatment with sorafenib followed by regorafenib for HCC: Additional analyses from the phase III RESORCE trial. J. Hepatol. 2018, 69, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Ryoo, B.Y.; Merle, P. Second-line cabozantinib after sorafenib treatment for advanced hepatocellular carcinoma: A subgroup analysis of the phase 3 CELESTIAL trial. ESMO Open. 2020, 5, e000714. [Google Scholar] [CrossRef]
- Llovet, J.M.; Decaens, T.; Raoul, J.L. Brivanib in patients with advanced hepatocellular carcinoma who were intolerant to sorafenib or for whom sorafenib failed: Results from the randomized phase III BRISK-PS study. J. Clin. Oncol. 2013, 31, 3509–3516. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kudo, M.; Assenat, E. Effect of everolimus on survival in advanced hepatocellular carcinoma after failure of sorafenib: The EVOLVE-1 randomized clinical trial. JAMA 2014, 312, 57–67. [Google Scholar] [CrossRef]
- Zhu, A.X.; Park, J.O.; Ryoo, B.Y. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Rimassa, L.; Assenat, E.; Peck-Radosavljevic, M. Tivantinib for second-line treatment of MET-high, advanced hepatocellular carcinoma (METIV-HCC): A final analysis of a phase 3, randomised, placebo-controlled study. Lancet Oncol. 2018, 19, 682–693. [Google Scholar] [CrossRef]
- Reig, M.; Galle, P.R.; Kudo, M. Pattern of progression in advanced hepatocellular carcinoma treated with ramucirumab. Liver Int. 2021, 41, 598–607. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n = 174 (%) |
|---|---|
| Median Age | |
| Years (range) | 69 (24–85) |
| Gender | |
| Male | 157 (90.2) |
| Female | 17 (9.8) |
| Diagnosis | |
| Histology | 117 (67.2) |
| AASLD criteria | 57 (32.8) |
| ECOG PS † | |
| 0 | 103 (59.5) |
| 1 | 70 (40.5) |
| Barcelona Clinic Liver Cancer stage | |
| B | 37 (21.3) |
| C | 137 (78.7) |
| Etiology | |
| Hepatitis C Infection | 70 (40.2) |
| Hepatitis B Infection | 23 (13.2) |
| Alcohol | 34 (19.5) |
| Non-alcoholic fatty liver disease | 15 (9.0) |
| Others | 32 (18.3) |
| Child–Pugh Class | |
| A | 172 (98.9) |
| B7 | 2 (1.1) |
| Prior surgery | |
| Yes | 71 (40.9) |
| No | 103 (59.1) |
| Prior locoregional treatments | |
| Yes | 112 (64.4) |
| No | 62 (35.6) |
| Reason for sorafenib discontinuation | |
| Disease progression | 141 (81.0) |
| Adverse events | 33 (19.0) |
| Disease Extent | |
| EHS | 102 (58.6) |
| Intrahepatic only | 72 (41.4) |
| Portal Vein Thrombosis | |
| Yes | 50 (28.8) |
| No | 124 (71.2) |
| Median AFP | |
| ng/dL (range) | 86 (1–436300) |
| Median neutrophils to lymphocyte ratio (range) | 3 (0–17) |
| Second-line treatment | |
| Targeted agents | 40 (23.0) |
| ICI +/– targeted agents | 40 (23.0) |
| Other treatments not approved for HCC | 52 (29.9) |
| Placebo | 42 (24.1) |
| Reasons for second-line treatment discontinuation ‡ | |
| Disease progression | 125 (73.1) |
| Adverse events | 14 (8.1) |
| Liver failure or ECOG PS worsening | 32 (18.8) |
| Albumin-Bilirubin grade after second-line treatment § | |
| 1 | 16 (22.9) |
| 2 | 41 (58.5) |
| 3 | 13 (18.6) |
| Class of Drug | Median OS (Months) | HR (95% CI) | p-Value |
|---|---|---|---|
| Placebo | 8.9 | Reference | |
| Other treatments not approved for HCC | 8.4 | 1.27 (0.83–1.96) | 0.27 |
| Targeted agents approved for HCC | 10.9 | 0.89 (0.55–1.43) | 0.63 |
| Anti-PD1 antibodies +/– anti-CTLA4 antibodies | 11.3 | 0.83 (0.45–1.51) | 0.53 |
| Anti-PD1 antibodies + targeted agents +/– anti-CTLA4 antibodies | 14.7 | 0.68 (0.36–1.29) | 0.24 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (continuous trait) | 1.00 (0.98–1.01) | 0.58 | ||
| Sex | ||||
| Male/Female | 1.55 (0.86–2.80) | 0.15 | ||
| ECOG PS | ||||
| 1/0 | 1.48 (1.06–2.07) | 0.020 | ||
| Barcelona Clinic Liver Cancer stage | ||||
| B/C | 0.76 (0.51–1.13) | 0.17 | ||
| HCC etiology | ||||
| Non-viral/Viral (HBV or HCV-related) | 0.88 (0.63–1.22) | 0.42 | ||
| Previous surgery | ||||
| Yes/No | 0.60 (0.43–0.84) | 0.03 | ||
| Sorafenib duration (continuous trait) | 1.00 (0.97–1.02) | 0.67 | ||
| Reason for sorafenib discontinuation | ||||
| AEs/Disease Progression | 0.69 (0.46–1.05) | 0.08 | ||
| Pattern of progression during first-line sorafenib | ||||
| EHS/Intrahepatic | 1.21 (0.84–1.74) | 0.30 | ||
| Time from sorafenib discontinuation to second-line start (continuous trait) | 1.01 (0.98–1.04) | 0.56 | ||
| Disease extent at the start of second-line treatment | ||||
| EHS/Intrahepatic | 1.21 (0.87–1.68) | 0.26 | 2.14 (1.36–3.37) | 0.001 |
| Portal vein thrombosis | ||||
| Yes/No | 1.91 (1.35–2.72) | <0.001 | 1.85 (1.28–2.69) | 0.001 |
| AFP levels at start of second-line treatment (ng/dL) | ||||
| ≥400/<400 | 1.19 (0.82–1.73) | 0.36 | ||
| NLR (continuous trait) | ||||
| High vs. low | 1.51 (1.08–1.23) | <0.001 | ||
| Second line treatment | 0.72 (0.52–1.00) | 0.048 | 0.24 (0.12–0.47) | <0.001 |
| AT/OT |
| Survival Rate | Sorafenib → AT (n = 94) | Sorafenib → OT (n = 80) |
|---|---|---|
| 6 months | 100% | 97% |
| 12 months | 81% | 79% |
| 24 months | 46% | 42% |
| 36 months | 29% | 17% |
| 48 months | 19% | 11% |
| 60 months | 12% | 6% |
| Type of Treatment | |||
|---|---|---|---|
| Targeted Agents (n = 40) | Anti-PD1 Antibodies, Alone or in Combination (n = 40) | OT (n = 94) | |
| Disease progression | 25 (62%) | 28 (70%) | 72 (77%) |
| AEs | 5 (13%) | 2 (5%) | 7 (7%) |
| Liver failure or ECOG PS worsening | 10 (25%) | 7 (18%) | 15 (16%) |
| Ongoing treatment | - | 3 (7%) | - |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Prior second-line treatment | 0.80 (0.58–1.12) | 0.20 | ||
| AT/OT | ||||
| Reason for second-line treatment discontinuation | ||||
| Disease Progression/Liver Failure or PS worsening | 0.38 (0.25–0.57) | <0.001 | ||
| AEs/Liver Failure or ECOG PS worsening | 0.45 (0.23–0.87) | 0.02 | ||
| Enrolment onto third-line trial | ||||
| Yes/No | 0.31 (0.19–0.51) | <0.001 | 0.34 (0.15–0.78) | 0.01 |
| AFP levels at second-line treatment discontinuation (ng/dL) | ||||
| ≥400/<400 | 1.67 (1.13–2.47) | 0.010 | 2.01 (1.08–3.74) | 0.029 |
| NLR at second-line treatment discontinuation (continuous trait) | ||||
| 1.15 (1.08–1.22) | 0.034 | |||
| Radiological response (RECIST v 1.1 criteria) during prior second-line treatment | ||||
| PD (or NA)/PR | 2.67 (1.22–5.84) | 0.014 | ||
| SD (or NA)/PR | 1.52 (0.70–3.28) | 0.293 | ||
| ALBI grade at second-line treatment discontinuation | ||||
| 2/1 | 2.99 (1.36–6.54) | 0.006 | 1.85 (0.81–4.21) | 0.14 |
| 3/1 | 20.1 (7.4–54.55) | <0.001 | 7.53 (2.48–22.90) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Personeni, N.; Pressiani, T.; Zanuso, V.; Casadei-Gardini, A.; D’Alessio, A.; Valgiusti, M.; Dadduzio, V.; Bergamo, F.; Soldà, C.; Rizzato, M.D.; et al. Determinants of Treatment Benefit and Post-Treatment Survival for Patients with Hepatocellular Carcinoma Enrolled in Second-Line Trials after the Failure of Sorafenib Treatment. J. Pers. Med. 2022, 12, 1726. https://doi.org/10.3390/jpm12101726
Personeni N, Pressiani T, Zanuso V, Casadei-Gardini A, D’Alessio A, Valgiusti M, Dadduzio V, Bergamo F, Soldà C, Rizzato MD, et al. Determinants of Treatment Benefit and Post-Treatment Survival for Patients with Hepatocellular Carcinoma Enrolled in Second-Line Trials after the Failure of Sorafenib Treatment. Journal of Personalized Medicine. 2022; 12(10):1726. https://doi.org/10.3390/jpm12101726
Chicago/Turabian StylePersoneni, Nicola, Tiziana Pressiani, Valentina Zanuso, Andrea Casadei-Gardini, Antonio D’Alessio, Martina Valgiusti, Vincenzo Dadduzio, Francesca Bergamo, Caterina Soldà, Mario Domenico Rizzato, and et al. 2022. "Determinants of Treatment Benefit and Post-Treatment Survival for Patients with Hepatocellular Carcinoma Enrolled in Second-Line Trials after the Failure of Sorafenib Treatment" Journal of Personalized Medicine 12, no. 10: 1726. https://doi.org/10.3390/jpm12101726
APA StylePersoneni, N., Pressiani, T., Zanuso, V., Casadei-Gardini, A., D’Alessio, A., Valgiusti, M., Dadduzio, V., Bergamo, F., Soldà, C., Rizzato, M. D., Giordano, L., Santoro, A., & Rimassa, L. (2022). Determinants of Treatment Benefit and Post-Treatment Survival for Patients with Hepatocellular Carcinoma Enrolled in Second-Line Trials after the Failure of Sorafenib Treatment. Journal of Personalized Medicine, 12(10), 1726. https://doi.org/10.3390/jpm12101726