
Broad Electrocardiogram Syndromes Spectrum: From Common Emergencies to Particular Electrical Heart Disorders

 ,
,  ,
, 
 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Wellen’s Syndrome
- Previous history of angina.
- Normal or slightly increased cardiac enzymes.
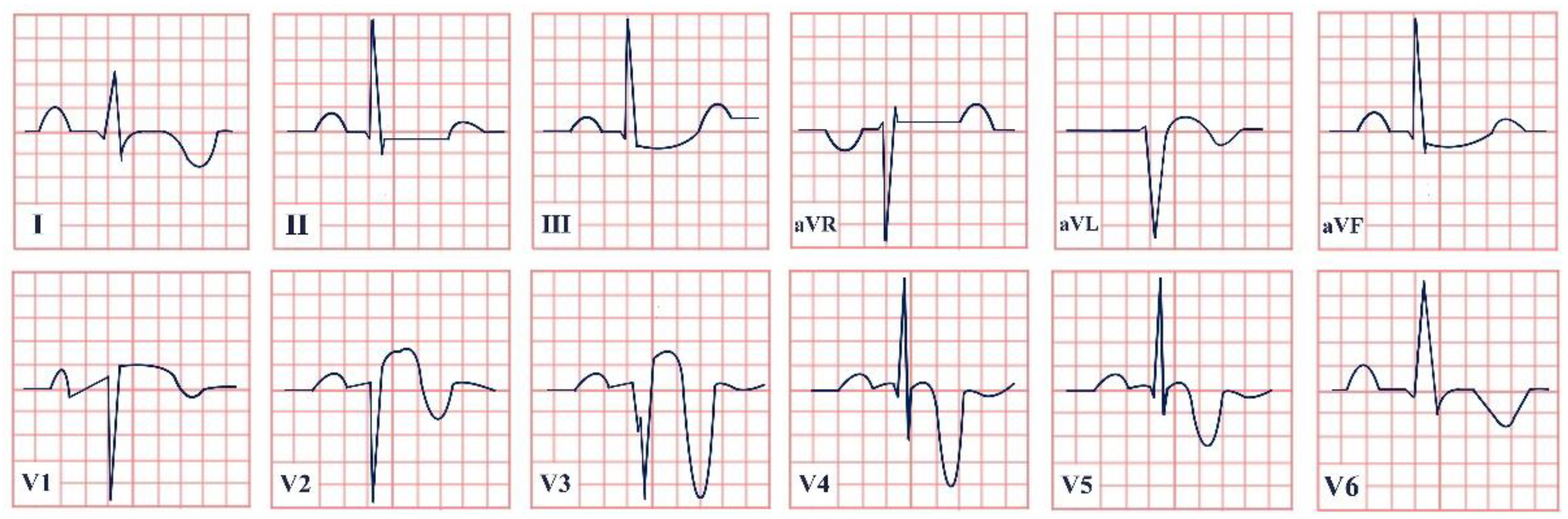
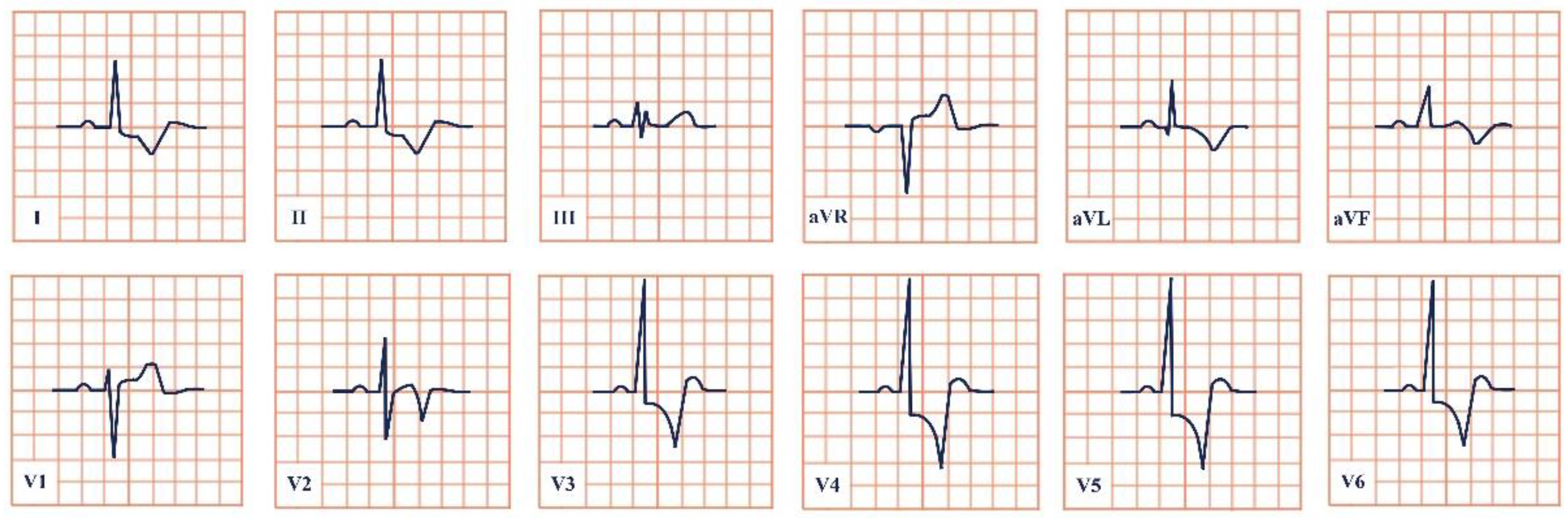
- Normal ECG during angina and T wave abnormalities when pain-free in V2–V3 (deeply inverted in Type A or biphasic in Type B).
- No pathological Q waves.
- No R wave loss [9].
- –
- T wave inversion or biphasic T wave due to ischemia.
- –
- T wave inversion, in most leads, due to Takotsubo cardiomyopathy.
- –
- ST-segment depression and T wave flattening, best seen in V2–V4, due to hypokalemia.
- –
- T wave inversion in V1–V6 due to acute pulmonary embolism.
- –
- T wave inversion due to cardiac memory, such as in LBBB, pacemakers, or transient tachycardia.
- –
- T wave inversion in V1–V3 physiologically in prepubertal patients.
- –
- T wave inversion in most leads due to pericarditis, myocarditis, or advanced AV block [10].
3. De Winter Syndrome
4. Kounis Syndrome
5. Takotsubo (Broken Heart) Syndrome
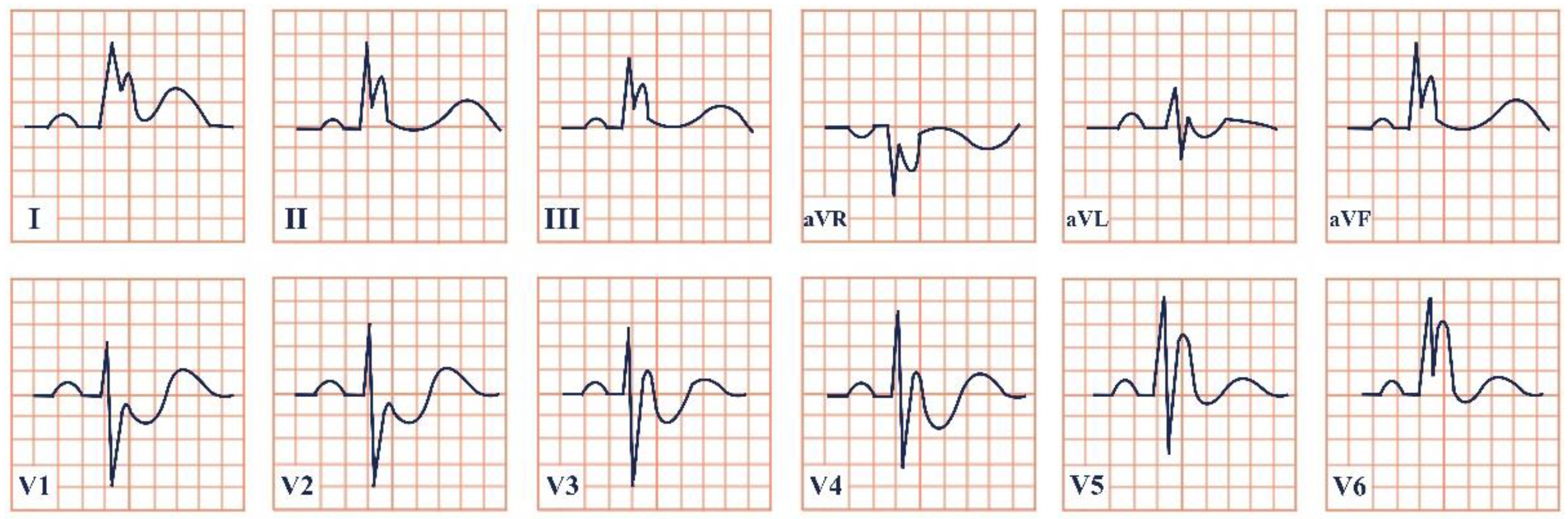
6. Yamaguchi Syndrome
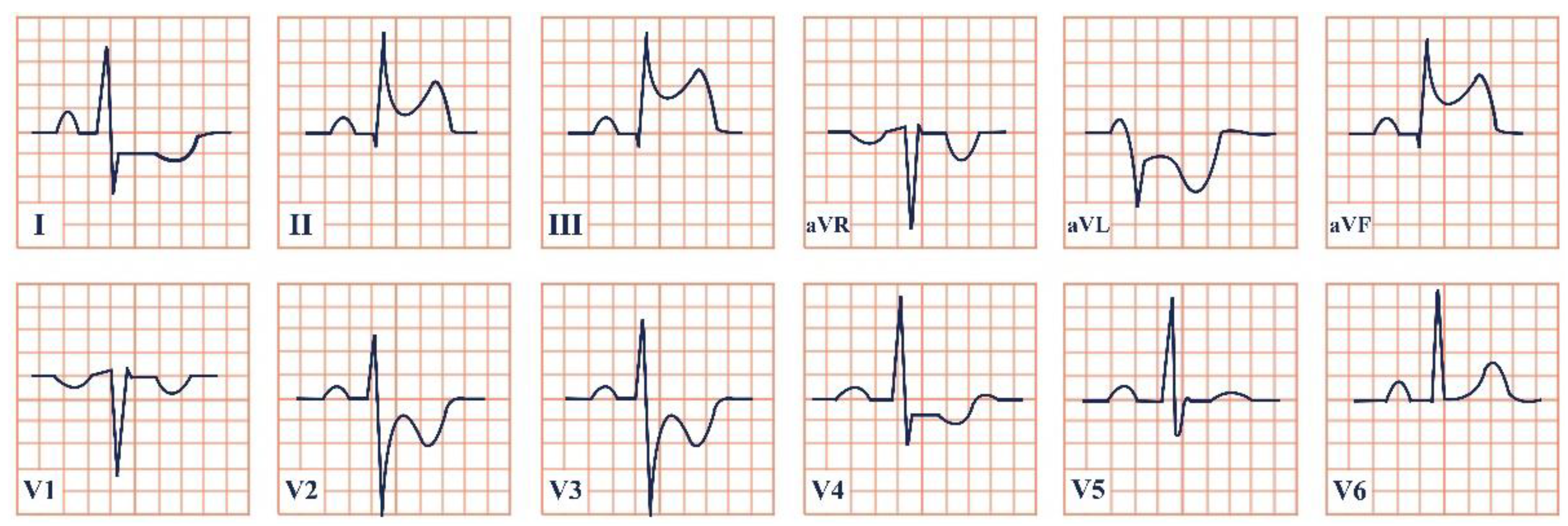
- Presence of asymmetric left ventricular hypertrophy.
- Left apex thicker than 15 mm.
- Ratio of apical wall thickness to posterior wall thickness higher than 1,5 [48].
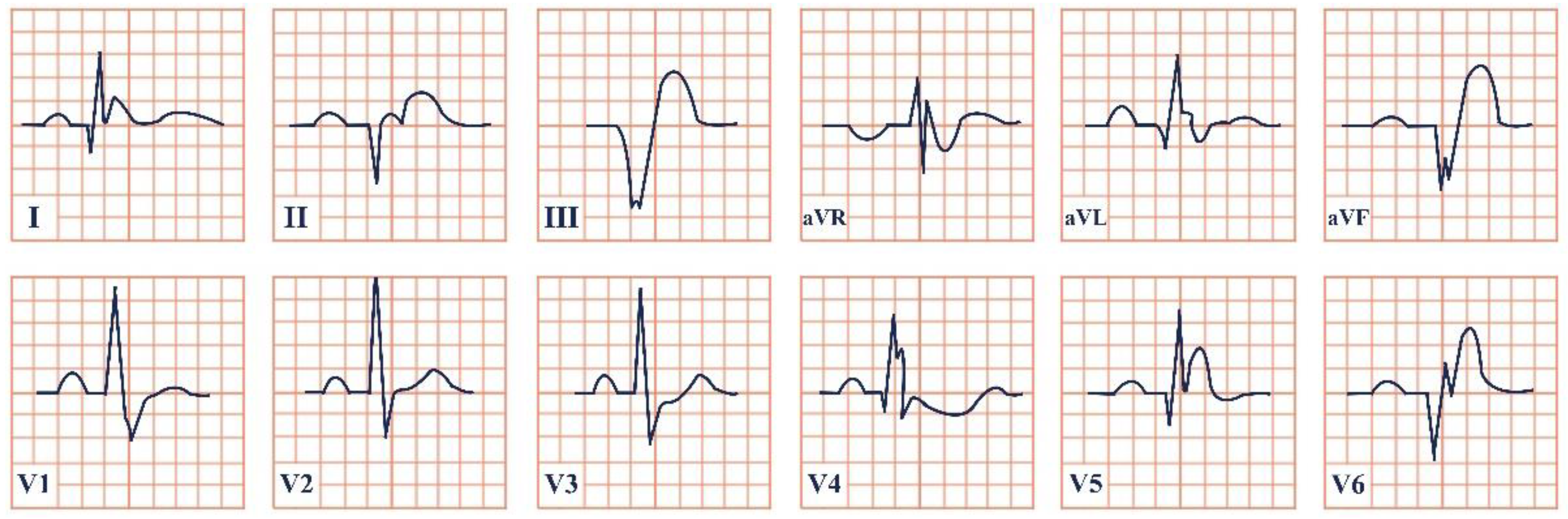
7. Wolff–Parkinson–White Syndrome
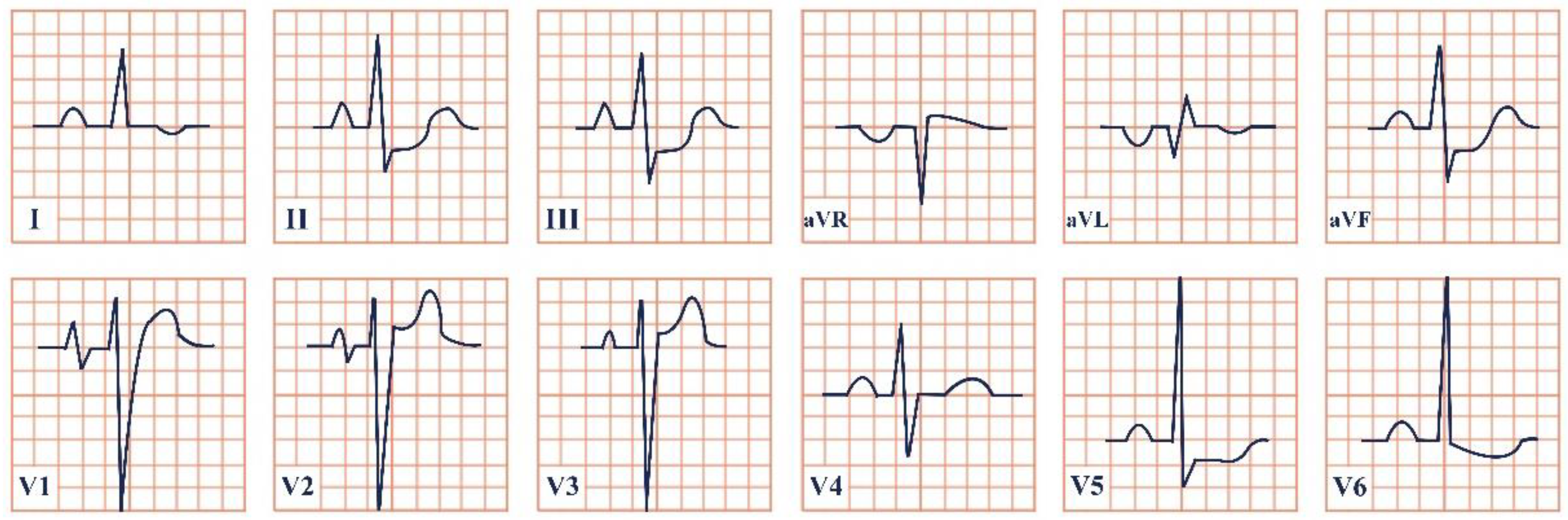
8. Lown–Ganong–Levine Syndrome
9. Brugada Syndrome
10. Frederick’s Syndrome
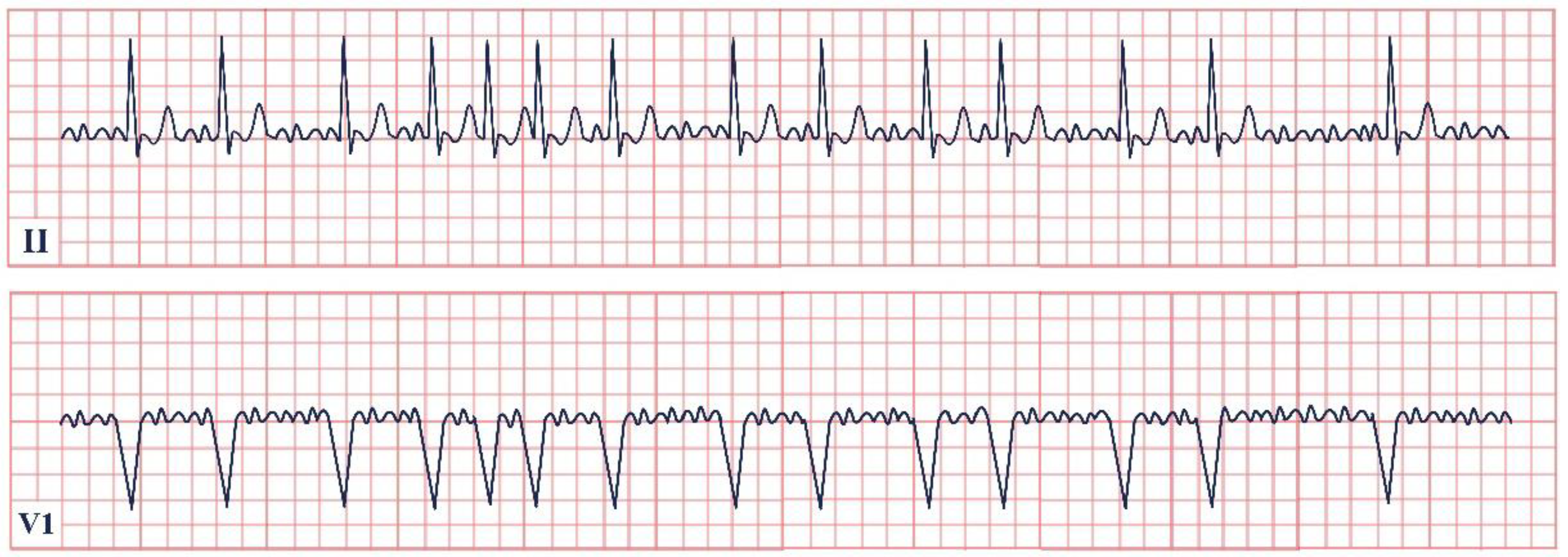
11. PAFIYAMA Syndrome
12. Haïssaguerre Syndrome
- Haïssaguerre syndrome diagnosis is confirmed by a J-point elevation larger than 1 mm in two or more contiguous inferior and/or lateral leads in a patient with a history of resuscitation from otherwise unexplained ventricular fibrillation or polymorphic ventricular tachycardia.
- Haïssaguerre syndrome can be diagnosed in a deceased patient due to sudden cardiac death who has no cardiac structural defects upon autopsy and a previous ECG with a J-point elevation larger than 1 mm in two or more contiguous inferior and/or lateral leads.
- Haïssaguerre syndrome can be diagnosed with the presence of a J-point elevation larger than 1 mm in two or more contiguous inferior and/or lateral leads on ECG [103].
13. Osborn Syndrome
14. LEOPARD Syndrome
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Zwaan, C.; Bär, F.W.H.M.; Wellens, H.J.J. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am. Heart J. 1982, 103, 730–736. [Google Scholar] [CrossRef]
- Miner, B.; Grigg, W.S.; Hart, E.H. Wellens Syndrome. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Balasubramanian, K.; Balasubramanian, R.; Subramanian, A. A dangerous twist of the ‘T’ wave: A case of Wellens’ Syndrome. Australas. Med. J. 2013, 6, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Hovland, A.; Bjornstad, H.; Staub, U.; Vik-Mo, H. Reversible ischemia in Wellens’ syndrome. J. Nucl. Cardiol. 2006, 13, e13-5. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Vyas, S.; Kumar, R. Wellen’s syndrome: Challenges in diagnosis. Malays. Fam. Physician 2015, 10, 35. [Google Scholar]
- Ajibawo, T.; Andreev, A.; Sahni, S. Wellens’ syndrome presenting as epigastric pain and syncope: An unusual presentation. Cureus 2020, 12, e6877. [Google Scholar] [CrossRef] [Green Version]
- Schears, M.R.; Sleigh, B.C.; Ganti, L. Wellen’s syndrome: Is one electrocardiogram good and plenty? Cureus 2019, 11, e4394. [Google Scholar] [CrossRef] [Green Version]
- Muharam, M.Y.; Ahmad, R.; Harmy, M. The ‘widow maker’: Electrocardiogram features that should not be missed. Malays. Fam. Physician 2013, 8, 45. [Google Scholar]
- Tandy, T.K.; Bottomy, D.P.; Lewis, J.G. Wellens’ syndrome. Ann. Emerg. Med. 1999, 33, 347–351. [Google Scholar] [CrossRef] [Green Version]
- Hanna, E.B.; Glancy, D.L. ST-segment depression and T-wave inversion: Classification, differential diagnosis, and caveats. Clevel. Clin. J. Med. 2011, 78, 404. [Google Scholar] [CrossRef]
- Nisbet, B.C.; Zlupko, G. Repeat Wellens’ syndrome: Case report of critical proximal left anterior descending artery restenosis. J. Emerg. Med. 2010, 39, 305–308. [Google Scholar] [CrossRef]
- Yan, J.; Wang, Q.; Zhang, Z.; Shi, G.; Hua, J.; Ying, R.; Kang, T.; Zheng, Z.; Zheng, Z.; Peng, X.; et al. De Winter syndrome as an emergency electrocardiogram sign of ST-elevation myocardial infarction: A case report. ESC Heart Fail. 2020, 7, 4353–4356. [Google Scholar] [CrossRef] [PubMed]
- Dressler, W.; Hugo, R. High T waves in the earliest stage of myocardial infarction. Am. Heart J. 1947, 34, 627–645. [Google Scholar] [CrossRef]
- de Winter, R.J.; Verouden, N.J.; Wellens, H.J.; Wilde, A.A. A new ECG sign of proximal LAD occlusion. N. Engl. J. Med. 2008, 359, 2071–2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verouden, N.J.; Koch, K.T.; Peters, R.J.; Henriques, J.P.; Baan, J.; van der Schaaf, R.J.; Vis, M.M.; Tijssen, J.G.; Piek, J.J.; Wellens, H.J.; et al. Persistent precordial “hyperacute” T-waves signify proximal left anterior descending artery occlusion. Heart 2009, 95, 1701–1706. [Google Scholar] [CrossRef] [Green Version]
- Barbati, G.; Caprioglio, F. de Winter’s Pattern: An Unusual but Very Important Electrocardiographic Sign to Recognize. CJC Open 2020, 2, 22–25. [Google Scholar] [CrossRef]
- Vilela, E.M.; Braga, J.P. DeWinter Pattern. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Bruyninckx, R.; Aertgeerts, B.; Bruyninckx, P.; Buntinx, F. Signs and symptoms in diagnosing acute myocardial infarction and acute coronary syndrome: A diagnostic meta-analysis. Br. J. Gen. Pract. 2008, 58, e1–e8. [Google Scholar] [CrossRef] [Green Version]
- Goebel, M.; Bledsoe, J.; Orford, J.L.; Mattu, A.; Brady, W.J. A new ST-segment elevation myocardial infarction equivalent pattern? Prominent T wave and J-point depression in the precordial leads associated with ST-segment elevation in lead aVr. Am. J. Emerg. Med. 2014, 32, 287.e285–287.e288. [Google Scholar] [CrossRef]
- XIAO, Y.; FAN, Z.; XU, B.; HE, S. de Winter syndrome, an easily ignored but life-threatening disease: A case report. J. South Med. Univ. 2020, 40, 919. [Google Scholar]
- Lin, Y.-Y.; Wen, Y.-D.; Wu, G.-L.; Xu, X.-D. De Winter syndrome and ST-segment elevation myocardial infarction can evolve into one another: Report of two cases. World J. Clin. Cases 2019, 7, 3296. [Google Scholar] [CrossRef]
- Puha, G.; Lionte, C.; Bologa, C.; Sorodoc, L. An unusual cause of myocardial ischemia in young adults. Rom. J. Cardiol. 2016, 26, 471–475. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.; Crea, F.; Goudevenos, J.A.; Halvorsen, S. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Kounis, N.G. Kounis syndrome (allergic angina and allergic myocardial infarction): A natural paradigm? Eur. J. Cardiol. 2006, 110, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Kounis, N.; Zavras, G. Histamine-induced coronary artery spasm: The concept of allergic angina. Br. J. Clin. Pract. 1991, 45, 121–128. [Google Scholar] [PubMed]
- Fourie, P. Kounis syndrome: A narrative review. South African J. Anaesth. Analg. 2016, 22, 72–80. [Google Scholar] [CrossRef]
- Dewachter, P.; Mouton-Faivre, C.; Emala, C.W.; Riou, B. Anaphylaxis and anesthesia: Controversies and new insights. Anesthesiology 2009, 111, 1141–1150. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.P.; Hou, D.; Pendyala, L.; Goudevenos, J.A.; Kounis, N.G. Drug-eluting stent thrombosis: The Kounis hypersensitivity-associated acute coronary syndrome revisited. JACC Cardiovasc. Interv. 2009, 2, 583–593. [Google Scholar] [CrossRef] [Green Version]
- Kounis, N.G.; Koniari, I.; Velissaris, D.; Tzanis, G.; Hahalis, G. Kounis syndrome—Not a single-organ arterial disorder but a multisystem and multidisciplinary disease. Balkan Med. J. 2019, 36, 212. [Google Scholar] [CrossRef]
- Lopez, P.R.; Peiris, A.N. Kounis syndrome. South Med. J. 2010, 103, 1148–1155. [Google Scholar] [CrossRef]
- Kounis, N.G. Kounis syndrome: An update on epidemiology, pathogenesis, diagnosis and therapeutic management. Clin. Chem. Lab. Med. 2016, 54, 1545–1559. [Google Scholar] [CrossRef] [Green Version]
- Ntuli, P.M.; Makambwa, E. Kounis syndrome. S. Afr. Med. J. 2015, 105, 878. [Google Scholar] [CrossRef] [Green Version]
- Lionte, C. An unusual cause of hypotension and abnormal electrocardiogram (ECG)—Scombroid poisoning. Cent. Eur. J. Med. 2010, 5, 292–297. [Google Scholar] [CrossRef]
- Haliga, R.E.; Morarasu, B.C.; Sorodoc, V.; Lionte, C.; Sirbu, O.; Stoica, A.; Ceasovschih, A.; Constantin, M.; Sorodoc, L. Rare Causes of Acute Coronary Syndrome: Carbon Monoxide Poisoning. Life 2022, 12, 1158. [Google Scholar] [CrossRef]
- Sharkey, S.W.; Lesser, J.R.; Maron, M.S.; Maron, B.J. Why not just call it tako-tsubo cardiomyopathy: A discussion of nomenclature. J. Am. Coll. Cardiol. 2011, 57, 1496–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossone, E.; Savarese, G.; Ferrara, F.; Citro, R.; Mosca, S.; Musella, F.; Limongelli, G.; Manfredini, R.; Cittadini, A.; Filardi, P.P. Takotsubo cardiomyopathy: Overview. Heart Fail. Clin. 2013, 9, 249–266. [Google Scholar] [CrossRef]
- Rodríguez, M.; Rzechorzek, W.; Herzog, E.; Lüscher, T.F. Misconceptions and facts about Takotsubo syndrome. Am. J. Med. 2019, 132, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; Bossone, E.; Schneider, B.; Sechtem, U.; Citro, R.; Underwood, S.R.; Sheppard, M.N.; Figtree, G.A.; Parodi, G.; Akashi, Y.J. Current state of knowledge on Takotsubo syndrome: A Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2016, 18, 8–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, H.; Tateishi, H.; Uchida, T. Takotsubo-type cardiomyophaty due to multivessel spasm. Clinical aspects of myocardial injury: From ischemia to heart failure. Tokyo Kagakuhyouounsha 1990, 2, 54–64. [Google Scholar]
- Dote, K.; Sato, H.; Tateishi, H.; Uchida, T.; Ishihara, M. Myocardial stunning due to simultaneous multivessel coronary spasms: A review of 5 cases. J. Cardiol. 1991, 21, 203–214. [Google Scholar]
- Kato, K.; Lyon, A.R.; Ghadri, J.-R.; Templin, C. Takotsubo syndrome: Aetiology, presentation and treatment. Heart 2017, 103, 1461–1469. [Google Scholar] [CrossRef]
- Sharkey, S.W. A clinical perspective of the takotsubo syndrome. Heart Fail. Clin. 2016, 12, 507–520. [Google Scholar] [CrossRef]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International expert consensus document on Takotsubo syndrome (part I): Clinical characteristics, diagnostic criteria, and pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Piña, I.L. Stress-induced cardiomyopathy. Heart Fail. Clin. 2019, 15, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, T.; TEI, C.; MURAYAMA, M.; ICHIYASU, H.; HADA, Y.; HAYASHI, T.; AMANO, K. Giant T wave inversion as a manifestation of asymmetrical apical hypertrophy (AAH) of the left ventricle echocardiographic and ultrasono-cardiotomographic study. Jpn. Heart J. 1976, 17, 611–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, H.; Ishimura, T.; Nishiyama, S.; Nagasaki, F.; Nakanishi, S.; Takatsu, F.; Nishijo, T.; Umeda, T.; Machii, K. Hypertrophic nonobstructive cardiomyopathy with giant negative T waves (apical hypertrophy): Ventriculographic and echocardiographic features in 30 patients. Am. J. Cardiol. 1979, 44, 401–412. [Google Scholar] [CrossRef]
- Varma, P.K.; Neema, P.K. Hypertrophic cardiomyopathy: Part 1-introduction, pathology and pathophysiology. Ann. Card. Anaesth. 2014, 17, 118. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.J.; Sonnenberg, B.; Woo, A.; Rakowski, P.; Parker, T.G.; Wigle, E.D.; Rakowski, H. Long-term outcome in patients with apical hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2002, 39, 638–645. [Google Scholar] [CrossRef]
- Shah, F.A.; Fujikawa, P.; Miller, J.B.; Singh, H. A Novel Case of Yamaguchi Syndrome in a Hispanic Male. Cureus 2021, 13, e17651. [Google Scholar] [CrossRef]
- Candelario, N.; Penalver, J.; Sen, M. Yamaguchi syndrome presenting as atrioventricular nodal re-entrant tachycardia in an African-American patient. BMJ Case Rep. 2017, 2017, bcr2016218051. [Google Scholar] [CrossRef]
- Al Lawati, H.; Al Habsi, M.; Al Riyami, A.B. Left ventricular apical hypertrophy (Yamaguchi disease). Eur. Heart J. Case Rep. 2021, 5, ytab330. [Google Scholar] [CrossRef]
- Ahmed, I.; Loudon, B.L.; Abozguia, K.; Cameron, D.; Shivu, G.N.; Phan, T.T.; Maher, A.; Stegemann, B.; Chow, A.; Marshall, H.; et al. Biventricular pacemaker therapy improves exercise capacity in patients with non-obstructive hypertrophic cardiomyopathy via augmented diastolic filling on exercise. Eur. J. Heart Fail. 2020, 22, 1263–1272. [Google Scholar] [CrossRef] [Green Version]
- Chrispin, J.; Calkins, H. Accessory pathways-related tachycardias: Wolff–Parkinson–White syndrome and atrioventricular reentrant tachycardias. In The ESC Textbook of Cardiovascular Medicine; Camm, A.J., Lüscher, T.F., Maurer, G., Serruys, P.W., Eds.; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Wolff, L.; Parkinson, J.; White, P.D. Bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia. 1930. Ann. Noninvasive Electrocardiol. 2006, 11, 340–353. [Google Scholar] [CrossRef] [PubMed]
- Holzmann, M.; Scherf, D. Über elektrokardiogramme mit verkürzter Vorhof-Kammer-Distanz und positiven P-Zacken. Z. Kiln. Med. 1932, 121, 404. [Google Scholar]
- Al-Khatib, S.M.; Pritchett, E.L. Clinical features of wolff-parkinson-white syndrome. Am. Heart J. 1999, 138, 403–413. [Google Scholar] [CrossRef]
- Sethi, K.; Dhall, A.; Chadha, D.; Garg, S.; Malani, S.; Mathew, O. WPW and preexcitation syndromes. J. Assoc. Physicians India 2007, 55, 10. [Google Scholar] [PubMed]
- Gallagher, J.J.; Pritchett, E.L.; Sealy, W.C.; Kasell, J.; Wallace, A.G. The preexcitation syndromes. Prog. Cardiovasc. Dis. 1978, 20, 285–327. [Google Scholar] [CrossRef]
- Sapra, A.; Albers, J.; Bhandari, P.; Davis, D.; Ranjit, E. Wolff-Parkinson-White Syndrome: A Master of Disguise. Cureus 2020, 12, e8672. [Google Scholar] [CrossRef]
- McINTIRE, M.S.; Freed, A. THE WOLFF-PARKINSON-WHITE SYNDROME: Report of a Case Occurring in a Mother and Infant. Am. J. Dis. Child. 1955, 89, 743–747. [Google Scholar]
- Valderrama, A.L. Wolff-Parkinson-White syndrome: Essentials for the primary care nurse practitioner. J. Am. Acad. Nurse Pract. 2004, 16, 378–383. [Google Scholar] [CrossRef]
- Larson, N.P.; Rosenthal, J.B.; Bridwell, R.E.; Tannenbaum, L.; Cibrario, A. Hide and Seek: Intermittent Preexcitation Wolff-Parkinson-White Syndrome Case Report and Management Overview. Cureus 2020, 12, e8971. [Google Scholar] [CrossRef] [PubMed]
- Benson, D.W.; Cohen, M.I. Wolff-Parkinson-White syndrome: Lessons learnt and lessons remaining. Cardiol. Young 2017, 27, S62–S67. [Google Scholar] [CrossRef]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram. J. Am. Coll. Cardiol. 2009, 53, 976–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mark, D.G.; Brady, W.J.; Pines, J.M. Preexcitation syndromes: Diagnostic consideration in the ED. Am. J. Emerg. Med. 2009, 27, 878–888. [Google Scholar] [CrossRef] [PubMed]
- Clerc, A.; Levy, R.; Critesco, C. A propos du raccourcissement permanent de l’espace PR de l’electrocardiogramme sans deformation du complex ventriculaire. Arch Mal. Coeur. 1938, 31, 569. [Google Scholar]
- LOWN, B.; GANONG, W.F.; LEVINE, S.A. The syndrome of short PR interval normal QRS complex and paroxysmal rapid heart action. Circulation 1952, 5, 693–706. [Google Scholar] [CrossRef] [Green Version]
- Basso, C.; Corrado, D.; Rossi, L.; Thiene, G. Ventricular preexcitation in children and young adults: Atrial myocarditis as a possible trigger of sudden death. Circulation 2001, 103, 269–275. [Google Scholar] [CrossRef]
- Hunter, J.; Tsounias, E.; Cogan, J.; Young, M.L. A Case of Lown-Ganong-Levine Syndrome: Due to an Accessory Pathway of James Fibers or Enhanced Atrioventricular Nodal Conduction (EAVNC)? Am. J. Case Rep. 2018, 19, 309–313. [Google Scholar] [CrossRef] [Green Version]
- Soos, M.P.; McComb, D. Lown Ganong Levine Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- MYERBURG, R.J.; SUNG, R.J.; CASTELLANOS, A. Ventricular Tachycardia and Ventricular Fibrillation in Patients with Short P-R Intervals and Narrow QRS Complexes. Pacing. Clin. Electrophysiol. 1979, 2, 568–578. [Google Scholar] [CrossRef]
- Benditt, D.G.; Pritchett, L.; Smith, W.M.; Wallace, A.G.; Gallagher, J.J. Characteristics of atrioventricular conduction and the spectrum of arrhythmias in lown-ganong-levine syndrome. Circulation 1978, 57, 454–465. [Google Scholar] [CrossRef] [Green Version]
- Ometto, R.; Thiene, G.; Corrado, D.; Vincenzi, M.; Rossi, L. Enhanced AV nodal conduction (Lown-Ganong-Levine syndrome) by congenitally hypoplastic AV node. Eur. Heart J. 1992, 13, 1579–1584. [Google Scholar] [CrossRef]
- Khan, N. A Glimpse into the Rare Find of Lown-Ganong-Levine Syndrome. EP Lab. Dig. 2015, 15. [Google Scholar]
- Sieira, J.; Dendramis, G.; Brugada, P. Pathogenesis and management of Brugada syndrome. Nat. Rev. Cardiol. 2016, 13, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Guazon, M.P. Algunas notas sobre bangungut. Revista Filipina de Medicina Y Farmacia 1917, 8, 437–442. [Google Scholar]
- Brugada, P.; Brugada, J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: A distinct clinical and electrocardiographic syndrome: A multicenter report. J. Am. Coll. Cardiol. 1992, 20, 1391–1396. [Google Scholar] [CrossRef]
- Gehshan, J.M.; Rizzolo, D. Understanding Brugada syndrome. JAAPA 2015, 28, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Wilde, A.A.; Postema, P.G.; Di Diego, J.M.; Viskin, S.; Morita, H.; Fish, J.M.; Antzelevitch, C. The pathophysiological mechanism underlying Brugada syndrome: Depolarization versus repolarization. J. Mol. Cell. Cardiol. 2010, 49, 543–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brugada, R.; Campuzano, O.; Sarquella-Brugada, G.; Brugada, J.; Brugada, P. Brugada syndrome. Methodist Debakey Cardiovasc. J. 2014, 10, 25. [Google Scholar] [CrossRef]
- Rojas, R.; Kaul, R.; Frenkel, D.; Hoch, E.G.; Iwai, S.; Jacobson, J.T.; Aronow, W.S. Brugada syndrome clinical update. Hosp. Pract. 1995 2021, 49, 255–261. [Google Scholar] [CrossRef]
- Lippi, G.; Montagnana, M.; Meschi, T.; Comelli, I.; Cervellin, G. Genetic and clinical aspects of Brugada syndrome: An update. Adv. Clin. Chem. 2012, 56, 197–208. [Google Scholar]
- Brugada, J.; Campuzano, O.; Arbelo, E.; Sarquella-Brugada, G.; Brugada, R. Present Status of Brugada Syndrome: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1046–1059. [Google Scholar] [CrossRef]
- Nademanee, K. Radiofrequency ablation in Brugada syndrome. Heart Rhythm. 2021, 18, 1805–1806. [Google Scholar] [CrossRef]
- Tzur, I.; Izhakian, S.; Gorelik, O. Frederick’s syndrome: A forgotten eponym. Open J. Clin. Med. Case Rep. 2019, 5, 1603. [Google Scholar]
- Fredericq, L. Rythme affolé des ventricules dû à la fibrillation des oreillettes. Physiologie du faisceau auriculo-ventriculaire. Arch Internat. Physiol. 1905, 2, 81. [Google Scholar]
- Fredericq, L. Action de la fibrillation des ventricules sur le rythme des pulsations auriculaires du cœur du chien. Bull. Mem. Acad. R Med. Belg. 1932, 22, 93–97. [Google Scholar]
- Трекина, Н.; Руденко, А.; Урванцева, И.; Саламатина, Л.; Корнеева, Е. Нормо-брадисистолическая форма фибрилляции предсердий (синдром Фредерика): поздняя диагностика и лечение. Клиницист 2014, 8, 58–62. [Google Scholar]
- Štěchovský, C.; Adla, T.; Bonaventura, J. Clinical perspective on the myocarditis and cardiomyopathies. Cesk Patol. 2019, 55, 209–217. [Google Scholar]
- Sanchis-Gomar, F.; Perez-Quilis, C.; Lippi, G.; Cervellin, G.; Leischik, R.; Lollgen, H.; Serrano-Ostariz, E.; Lucia, A. Atrial fibrillation in highly trained endurance athletes—Description of a syndrome. Int. J. Cardiol. 2017, 226, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, M. Atrial fibrillation in endurance athletes. Eur. J. Prev. Cardiol. 2014, 21, 1040–1048. [Google Scholar] [CrossRef]
- Zimetbaum, P. Atrial Fibrillation. Ann. Intern. Med. 2017, 166, ITC33–ITC48. [Google Scholar] [CrossRef]
- Romero, I.; Nedios, S.; Kriatselis, C. Diagnosis and management of atrial fibrillation: An overview. Cardiovasc. Ther. 2014, 32, 242–252. [Google Scholar] [CrossRef] [Green Version]
- Sanchis-Gomar, F.; Lippi, G.; Cervellin, G.; Perez-Quilis, C. PAFIYAMA syndrome evidence in highly trained population. Int. J. Cardiol. 2018, 256, 10. [Google Scholar] [CrossRef]
- Kherlopian, A.; Weinshel, S.; Madias, C.; Estes, N.A.M., 3rd. Exercise and Athletic Activity in Atrial Fibrillation. Card. Electrophysiol. Clin. 2021, 13, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Viskin, S. Idiopathic ventricular fibrillation “Le Syndrome d’Haissaguerre” and the fear of J waves. J. Am. Coll. Cardiol. 2009, 53, 620–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomaszewski, W. Changement electrocardiographiques observes chez un homme mort de froid. Arch Mal. Coeur. Vaiss. 1938, 31, 525–528. [Google Scholar]
- Haïssaguerre, M.; Derval, N.; Sacher, F.; Jesel, L.; Deisenhofer, I.; de Roy, L.; Pasquié, J.-L.; Nogami, A.; Babuty, D.; Yli-Mayry, S.; et al. Sudden cardiac arrest associated with early repolarization. N. Engl. J. Med. 2008, 358, 2016–2023. [Google Scholar] [CrossRef] [Green Version]
- Rosso, R.; Kogan, E.; Belhassen, B.; Rozovski, U.; Scheinman, M.M.; Zeltser, D.; Halkin, A.; Steinvil, A.; Heller, K.; Glikson, M.; et al. J-point elevation in survivors of primary ventricular fibrillation and matched control subjects: Incidence and clinical significance. J. Am. Coll. Cardiol. 2008, 52, 1231–1238. [Google Scholar] [CrossRef] [Green Version]
- Hanboly, N.H. Haissaguerre syndrome: The gray area still exists. Nig. J. Cardiol. 2017, 14, 59. [Google Scholar] [CrossRef]
- Miyazaki, S.; Shah, A.J.; Haissaguerre, M. Early repolarization syndrome—A new electrical disorder associated with sudden cardiac death. Circ. J. 2010, 74, 2039–2044. [Google Scholar] [CrossRef] [Green Version]
- Li, G.-L.; Yang, L.; Cui, C.-C.; Sun, C.-F.; Yan, G.-X. J wave syndromes: A decade of progress. Chin. Med. J. 2015, 128, 969–975. [Google Scholar] [CrossRef]
- Priori, S.G.; Wilde, A.A.; Horie, M.; Cho, Y.; Behr, E.R.; Berul, C.; Blom, N.; Brugada, J.; Chiang, C.E.; Huikuri, H.; et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: Document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013. Heart Rhythm. 2013, 10, 1932–1963. [Google Scholar] [CrossRef]
- Chiarini, R.; Duarte, C.E.; Junior, J.D.R.T.M.; de Vasconcelos, J.T.M.; dos Santos Galvão Filho, S. Eletrocardiograma na síndrome de Haissaguerre. J. Card. Arrhythm. 2019, 32, 155–162. [Google Scholar]
- Antzelevitch, C.; Yan, G.X.; Viskin, S. Rationale for the use of the terms J-wave syndromes and early repolarization. J. Am. Coll. Cardiol. 2011, 57, 1587–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourier, F.; Denis, A.; Cheniti, G.; Lam, A.; Vlachos, K.; Takigawa, M.; Kitamura, T.; Frontera, A.; Duchateau, J.; Pambrun, T.; et al. Early Repolarization Syndrome: Diagnostic and Therapeutic Approach. Front. Cardiovasc. Med. 2018, 5, 169. [Google Scholar] [CrossRef] [PubMed]
- Osborn, J.J. Experimental hypothermia: Respiratory and blood pH changes in relation to cardiac function. Am. J. Physiol. 1953, 175, 389–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, M.; Kobayashi, Y.; Kodani, E.; Hirayama, Y.; Atarashi, H.; Katoh, T.; Takano, T. Osborn waves: History and significance. Indian Pacing Electrophysiol. J. 2004, 4, 33. [Google Scholar]
- Omar, H.R. The Osborn wave: What have we learned? Herz 2016, 41, 48–56. [Google Scholar] [CrossRef]
- Gussak, I.; Bjerregaard, P.; Egan, T.M.; Chaitman, B.R. ECG phenomenon called the J wave: History, pathophysiology, and clinical significance. J. Electrocardiol. 1995, 28, 49–58. [Google Scholar] [CrossRef]
- Feldman, A.; Freedberg, N.A.; Antonelli, D.; Rozner, E.; Turgeman, Y. Prognostic Value of J (Osborn) Waves on Surface Electrocardiogram Tracing during Therapeutic Hypothermia in Out-of-Hospital Cardiac Arrest Survivors (JOW trial). Isr. Med. Assoc. J. 2021, 23, 291–296. [Google Scholar]
- Sarkozy, A.; Digilio, M.C.; Dallapiccola, B. Leopard syndrome. Orphanet J. Rare Dis. 2008, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- ZEISLER, E.P.; BECKER, S.W. Generalized lentigo: Its relation to systemic nonelevated nevi. Arch Derm. Syphilol. 1936, 33, 109–125. [Google Scholar] [CrossRef]
- Gorlin, R.J.; Anderson, R.C.; Blaw, M. Multiple lentigenes syndrome: Complex comprising multiple lentigenes, electrocardiographic conduction abnormalities, ocular hypertelorism, pulmonary stenosis, abnormalities of genitalia, retardation of growth, sensorineural deafness, and autosomal dominant hereditary pattern. Am. J. Dis. Child. 1969, 117, 652–662. [Google Scholar]
- Yue, X.; Zhao, X.; Dai, Y.; Yu, L. Leopard syndrome: The potential cardiac defect underlying skin phenotypes. Hereditas 2021, 158, 34. [Google Scholar] [CrossRef] [PubMed]
- Limongelli, G.; Pacileo, G.; Marino, B.; Digilio, M.C.; Sarkozy, A.; Elliott, P.; Versacci, P.; Calabro, P.; De Zorzi, A.; Di Salvo, G.; et al. Prevalence and clinical significance of cardiovascular abnormalities in patients with the LEOPARD syndrome. Am. J. Cardiol. 2007, 100, 736–741. [Google Scholar] [CrossRef] [PubMed]
- Voron, D.A.; Hatfield, H.H.; Kalkhoff, R.K. Multiple lentigines syndrome: Case report and review of the literature. Am. J. Med. 1976, 60, 447–456. [Google Scholar] [CrossRef]
- Elliott, P.; McKenna, W.J. Hypertrophic cardiomyopathy. Lancet 2004, 363, 1881–1891. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ECG Syndrome | ECG Diagnostic Criteria | ECG Aspect |
|---|---|---|
| Wellen’s syndrome |
|  |
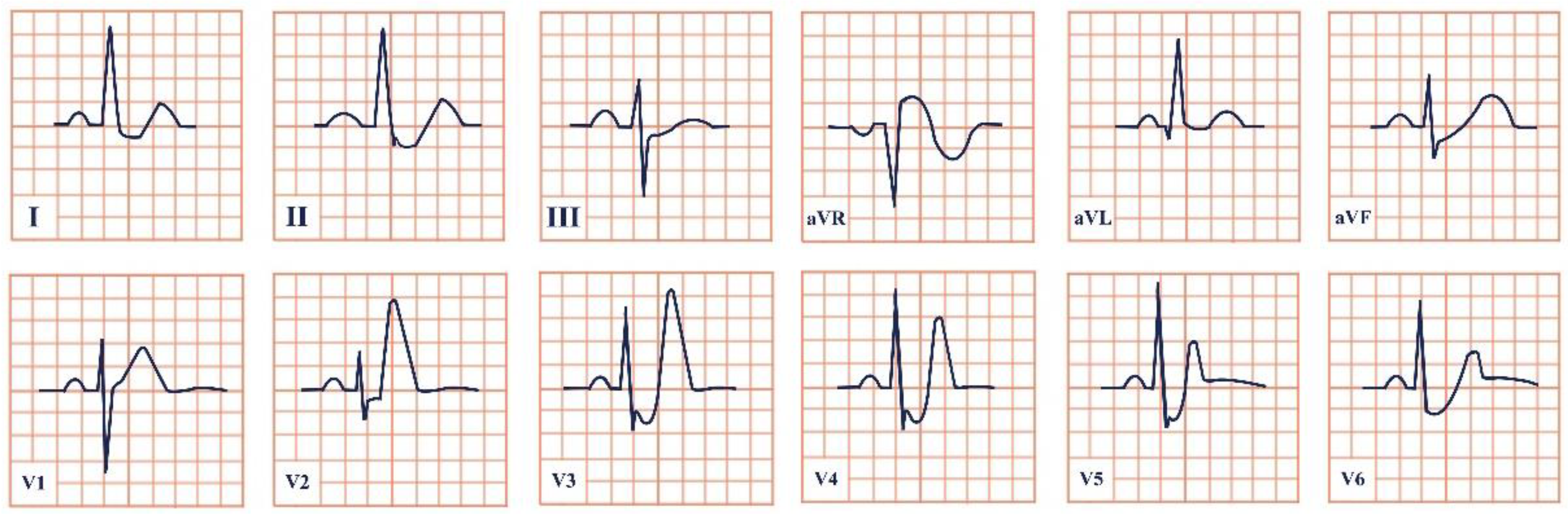
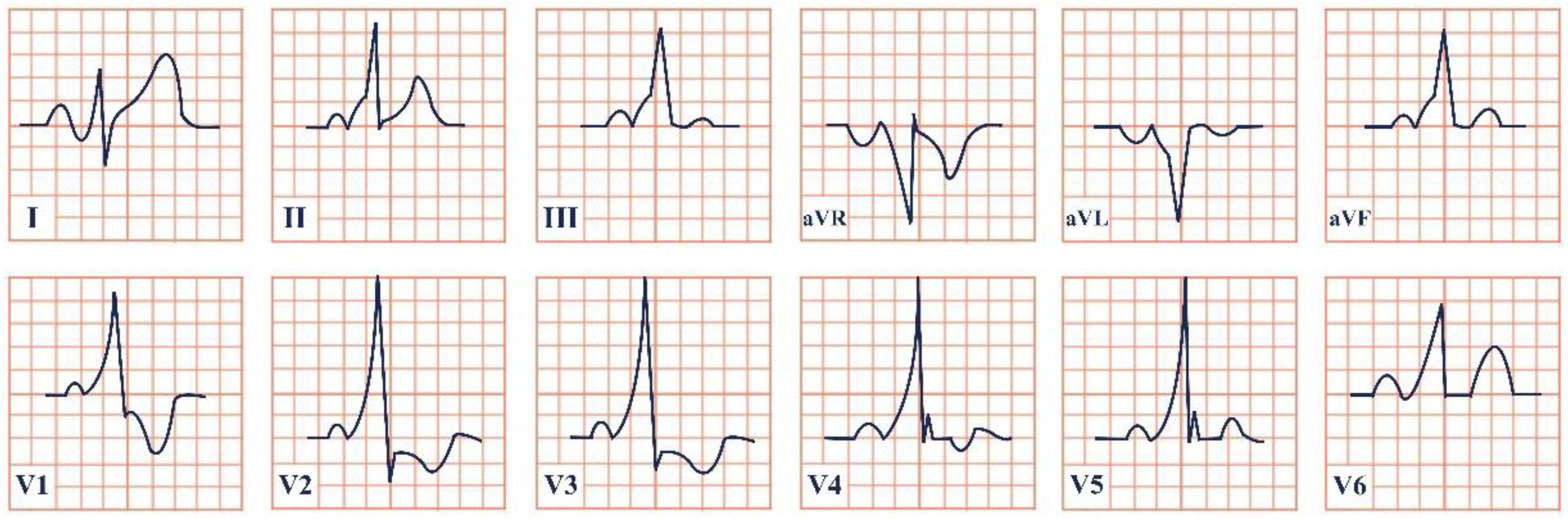
| De Winter syndrome |
|  |
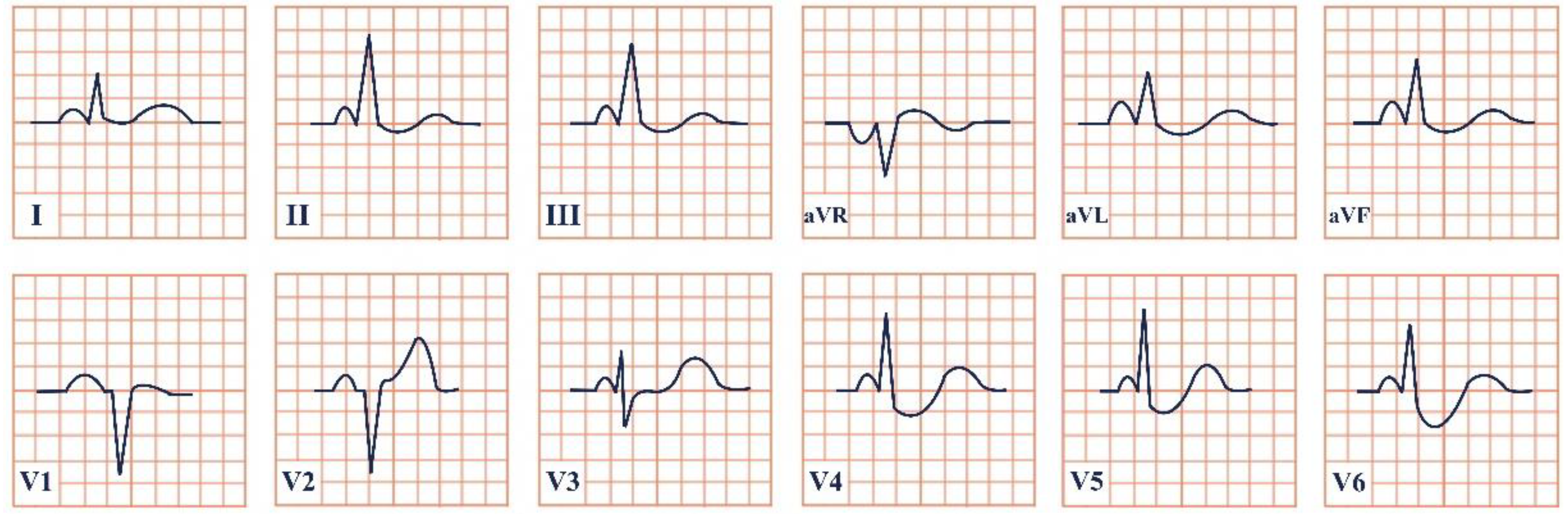
| Kounis syndrome |
|  |
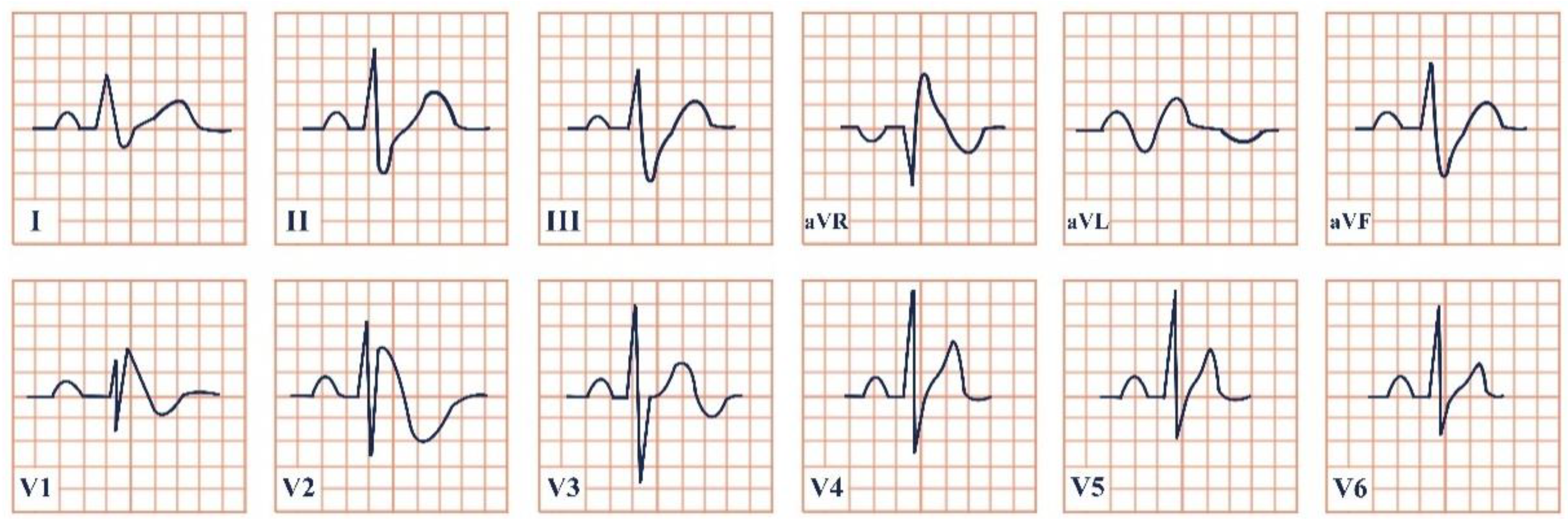
| Takotsubo syndrome |
|  |
| Yamaguchi syndrome |
|  |
| Wolff–Parkinson–White syndrome |
|  |
| Lown–Ganong–Levine syndrome |
|  |
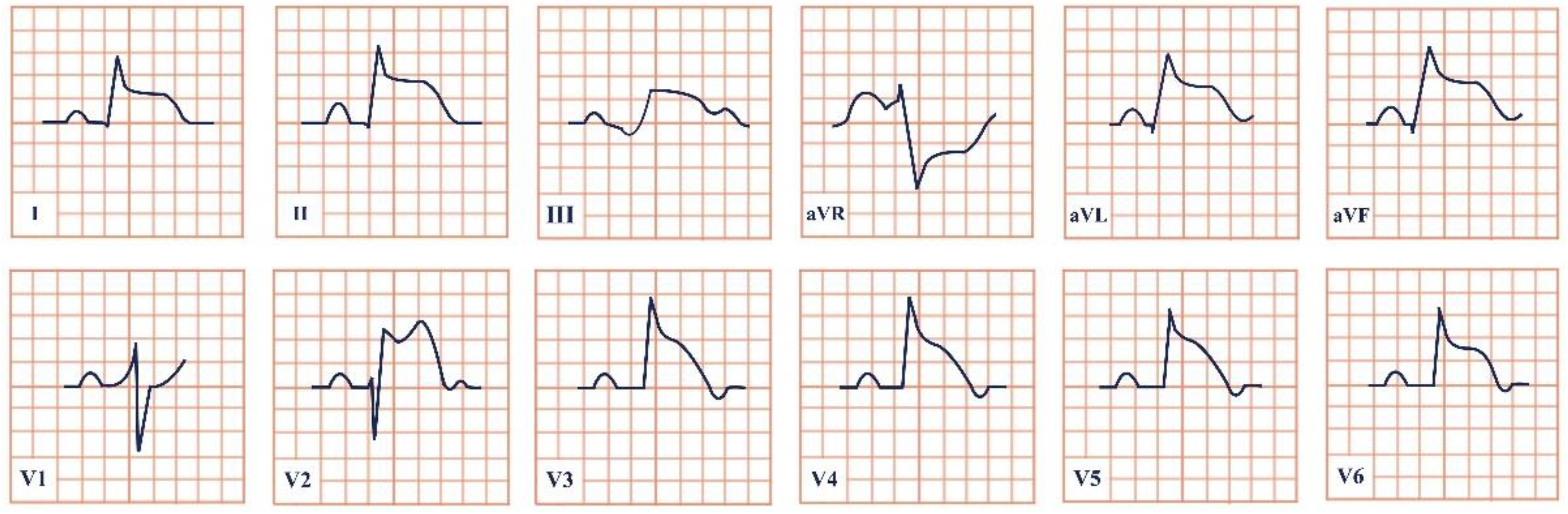
| Brugada syndrome |
|  |
| Frederick’s syndrome |
|  |
| PAFIYAMA syndrome |
|  |
| Haïssaguerre syndrome |
|  |
| Osborn syndrome |
|  |
| LEOPARD syndrome |
|  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balta, A.; Ceasovschih, A.; Șorodoc, V.; Dimitriadis, K.; Güzel, S.; Lionte, C.; Stătescu, C.; Sascău, R.A.; Mantzouranis, E.; Sakalidis, A.; et al. Broad Electrocardiogram Syndromes Spectrum: From Common Emergencies to Particular Electrical Heart Disorders. J. Pers. Med. 2022, 12, 1754. https://doi.org/10.3390/jpm12111754
Balta A, Ceasovschih A, Șorodoc V, Dimitriadis K, Güzel S, Lionte C, Stătescu C, Sascău RA, Mantzouranis E, Sakalidis A, et al. Broad Electrocardiogram Syndromes Spectrum: From Common Emergencies to Particular Electrical Heart Disorders. Journal of Personalized Medicine. 2022; 12(11):1754. https://doi.org/10.3390/jpm12111754
Chicago/Turabian StyleBalta, Anastasia, Alexandr Ceasovschih, Victorița Șorodoc, Kyriakos Dimitriadis, Sara Güzel, Cătălina Lionte, Cristian Stătescu, Radu Andy Sascău, Emmanouil Mantzouranis, Athanasios Sakalidis, and et al. 2022. "Broad Electrocardiogram Syndromes Spectrum: From Common Emergencies to Particular Electrical Heart Disorders" Journal of Personalized Medicine 12, no. 11: 1754. https://doi.org/10.3390/jpm12111754
APA StyleBalta, A., Ceasovschih, A., Șorodoc, V., Dimitriadis, K., Güzel, S., Lionte, C., Stătescu, C., Sascău, R. A., Mantzouranis, E., Sakalidis, A., Vlachakis, P. K., Tsioufis, P., Kordalis, A., Tsiamis, E., Tsioufis, K., & Șorodoc, L. (2022). Broad Electrocardiogram Syndromes Spectrum: From Common Emergencies to Particular Electrical Heart Disorders. Journal of Personalized Medicine, 12(11), 1754. https://doi.org/10.3390/jpm12111754