


Clustering Molecular Subtypes in Breast Cancer, Immunohistochemical Parameters and Risk of Axillary Nodal Involvement

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Population
2.2. Pathological Assessment
2.3. Statistical Analysis
2.4. Cluster Analysis (CA)
2.4.1. Approach to CA
2.4.2. Types of Data and Measures of Distance
2.4.3. Hierarchical Agglomerative Method
2.4.4. Selecting the Optimum Number of Clusters
3. Results
3.1. Patients’ Characteristics
3.2. Statistical Analysis
3.3. Cluster Analysis
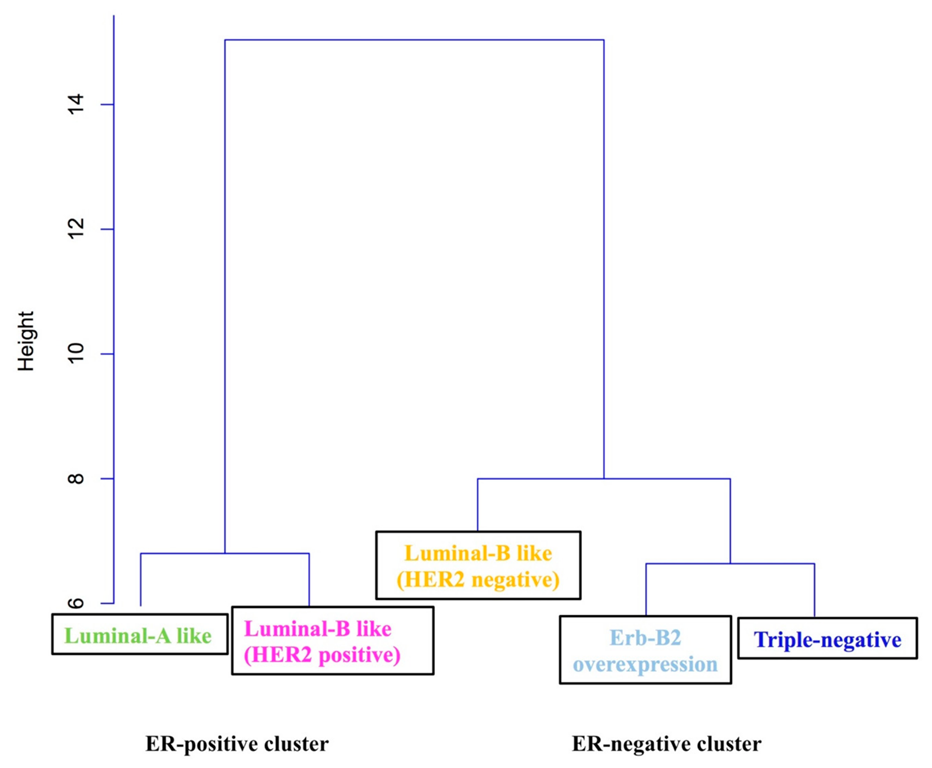
3.3.1. First CA
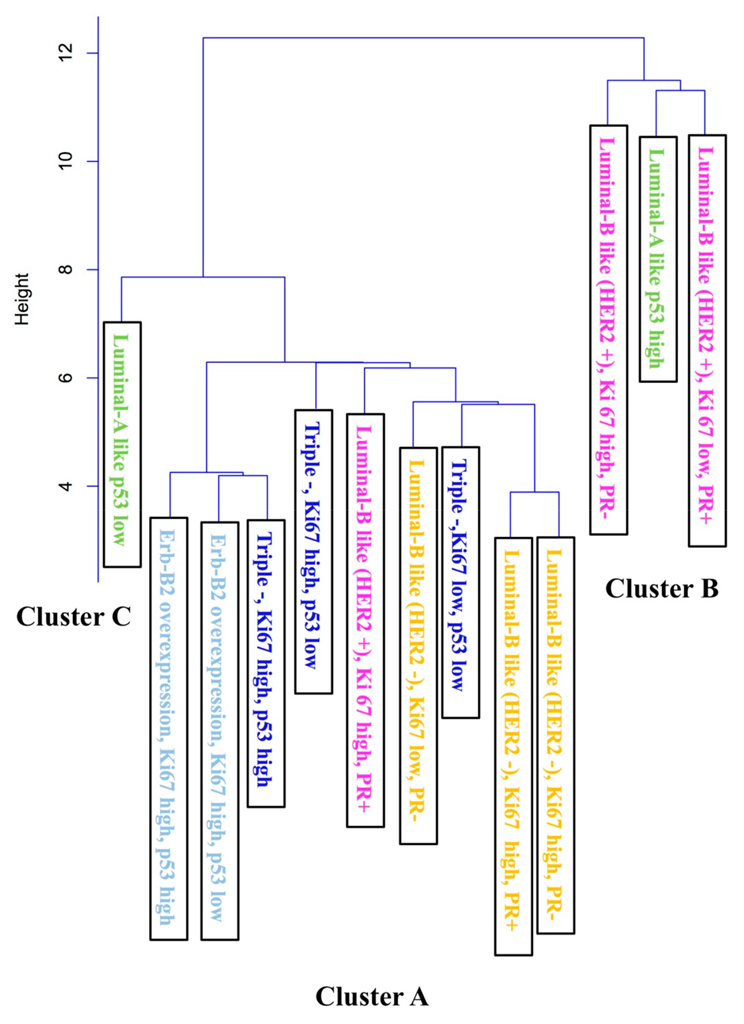
3.3.2. Second CA
- Based on the HER2 negative quality (6 observations): Luminal B, HER2-, high Ki67, PR+ or PR-; Luminal B, HER2-, low Ki67, PR-; TN, with low Ki67 and p53; TN, with high Ki67 and low or high p53.
- Based on high Ki67 quality (7 observations): TN, high Ki67 and low or high p53; Luminal B, HER2+, high Ki67 and PR+; Luminal B, HER2-, high Ki67, PR+ or PR-; Erb-B2 overexpression, high Ki67 and low or high p53. Results are shown in Figure 2.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The 2013 St. Gallen International Breast Cancer Consensus Conference. St Gallen 2013 Proceedings Book. The Breast Supplement. 2013, 22, S1–S184.
- Sørlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Bastien, R.R.; Rodríguez-Lescure, Á.; Ebbert, M.T.; Prat, A.; Munárriz, B.; Rowe, L.; Miller, P.; Ruiz-Borrego, M.; Anderson, D.; Lyons, B.; et al. PAM50 breast cancer subtyping by RT-qPCR and concordance with standard clinical molecular markers. BMC Med. Genom. 2012, 5, 44. [Google Scholar] [CrossRef] [PubMed]
- Fein, D.A.; Fowble, B.L.; Hanlon, A.L.; Hooks, M.A.; Hoffman, J.P.; Sigurdson, E.R.; Jardines, L.A.; Eisenberg, B.L. Identification of women with T1-T2 breast cancer at low risk of positive axillary nodes. J. Surg. Oncol. 1997, 65, 34–39. [Google Scholar] [CrossRef]
- McGee, J.M.; Youmans, R.; Clingan, F.; Malnar, K.; Bellefeuille, C.; Berry, B. The value of axillary dissection in T1a breast cancer. Am. J. Surg. 1996, 172, 501–504. [Google Scholar] [CrossRef]
- Cetintaş, S.K.; Kurt, M.; Ozkan, L.; Engin, K.; Gökgöz, S.; Taşdelen, I. Factors influencing axillary node metastasis in breast cancer. Tumori 2006, 92, 416–422. [Google Scholar] [CrossRef]
- Harvey, J.M.; Clark, G.M.; Osborne, C.K.; Allred, D.C. Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J. Clin. Oncol. 1999, 17, 1474–1481. [Google Scholar] [CrossRef]
- Pertschuk, L.P.; Kim, D.S.; Nayer, K.; Feldman, J.G.; Eisenberg, K.B.; Carter, A.C.; Rong, Z.T.; Thelmo, W.L.; Fleisher, J.; Greene, G.L. Immunocytochemical estrogen and progestin receptor assays in breast cancer with monoclonal antibodies. Histopathologic, demographic, and biochemical correlations and relationship to endocrine response and survival. Cancer 1990, 66, 1663–1670. [Google Scholar] [CrossRef]
- Bartlett, J.M.; Brookes, C.L.; Robson, T.; van de Velde, C.J.; Billingham, L.J.; Campbell, F.M.; Grant, M.; Hasenburg, A.; Hille, E.T.; Kay, C.; et al. Estrogen receptor and progesterone receptor as predictive biomarkers of response to endocrine therapy: A prospectively powered pathology study in the Tamoxifen and Exemestane Adjuvant Multinational trial. J. Clin. Oncol. 2011, 29, 1531–1538. [Google Scholar] [CrossRef]
- Colzani, E.; Liljegren, A.; Johansson, A.L.; Adolfsson, J.; Hellborg, H.; Hall, P.F.; Czene, K. Prognosis of patients with breast cancer: Causes of death and effects of time since diagnosis, age, and tumor characteristics. J. Clin. Oncol. 2011, 29, 4014–4021. [Google Scholar] [CrossRef] [PubMed]
- Colleoni, M.; Sun, Z.; Price, K.N.; Karlsson, P.; Forbes, J.F.; Thürlimann, B.; Gianni, L.; Castiglione, M.; Gelber, R.D.; Coates, A.S.; et al. Annual Hazard Rates of Recurrence for Breast Cancer During 24 Years of Follow-Up: Results from the International Breast Cancer Study Group Trials I to V. J. Clin. Oncol. 2016, 34, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Andrulis, I.L.; Bull, S.B.; Blackstein, M.E.; Sutherland, D.; Mak, C.; Sidlofsky, S.; Pritzker, K.P.; Hartwick, R.W.; Hanna, W.; Lickley, L.; et al. neu/erbB-2 amplification identifies a poor-prognosis group of women with node-negative breast cancer. Toronto Breast Cancer Study Group. J. Clin. Oncol. 1998, 16, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Tandon, A.K.; Clark, G.M.; Chamness, G.C.; Ullrich, A.; McGuire, W.L. HER-2/neu oncogene protein and prognosis in breast cancer. J. Clin. Oncol. 1989, 7, 1120–1128. [Google Scholar] [CrossRef]
- Ferrero-Poüs, M.; Hacène, K.; Bouchet, C.; Le Doussal, V.; Tubiana-Hulin, M.; Spyratos, F. Relationship between c-erbB-2 and other tumor characteristics in breast cancer prognosis. Clin. Cancer Res. 2000, 6, 4745–4754. [Google Scholar]
- Abd El-Rehim, D.M.; Pinder, S.E.; Paish, C.E.; Bell, J.; Blamey, R.W.; Robertson, J.F.; Nicholson, R.I.; Ellis, I.O. Expression of luminal and basal cytokeratins in human breast carcinoma. J. Pathol. 2004, 203, 661–671. [Google Scholar] [CrossRef]
- Perreard, L.; Fan, C.; Quackenbush, J.F.; Mullins, M.; Gauthier, N.P.; Nelson, E.; Mone, M.; Hansen, H.; Buys, S.S.; Rasmussen, K.; et al. Classification and risk stratification of invasive breast carcinomas using a real-time quantitative RT-PCR assay. Breast Cancer Res. 2006, 8, R23. [Google Scholar] [CrossRef]
- Sorlie, T.; Tibshirani, R.; Parker, J.; Hastie, T.; Marron, J.S.; Nobel, A.; Deng, S.; Johnsen, H.; Pesich, R.; Geisler, S.; et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. USA 2003, 100, 8418–8423. [Google Scholar] [CrossRef]
- Sotiriou, C.; Neo, S.Y.; McShane, L.M.; Korn, E.L.; Long, P.M.; Jazaeri, A.; Martiat, P.; Fox, S.B.; Harris, A.L.; Liu, E.T. Breast cancer classification and prognosis based on gene expression profiles from a population-based study. Proc. Natl. Acad. Sci. USA 2003, 100, 10393–10398. [Google Scholar] [CrossRef]
- Yu, K.; Lee, C.H.; Tan, P.H.; Tan, P. Conservation of breast cancer molecular subtypes and transcriptional patterns of tumor progression across distinct ethnic populations. Clin. Cancer Res. 2004, 10, 5508–5517. [Google Scholar] [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Cheang, M.C.; Chia, S.K.; Voduc, D.; Gao, D.; Leung, S.; Snider, J.; Watson, M.; Davies, S.; Bernard, P.S.; Parker, J.S.; et al. Ki67 index, HER2 status, and prognosis of patients with luminal B breast cancer. J. Natl. Cancer Inst. 2009, 101, 736–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, C.; Oh, D.S.; Wessels, L.; Weigelt, B.; Nuyten, D.S.; Nobel, A.B.; van’t Veer, L.J.; Perou, C.M. Concordance among gene-expression-based predictors for breast cancer. N. Engl. J. Med. 2006, 355, 560–569. [Google Scholar] [CrossRef]
- Hu, Z.; Fan, C.; Oh, D.S.; Marron, J.S.; He, X.; Qaqish, B.F.; Livasy, C.; Carey, L.A.; Reynolds, E.; Dressler, L.; et al. The molecular portraits of breast tumors are conserved across microarray platforms. BMC Genom. 2006, 7, 96. [Google Scholar] [CrossRef]
- King, C.R.; Kraus, M.H.; Aaronson, S.A. Amplification of a novel v-erbB-related gene in a human mammary carcinoma. Science 1985, 229, 974–976. [Google Scholar] [CrossRef] [PubMed]
- Klapper, L.N.; Glathe, S.; Vaisman, N.; Hynes, N.E.; Andrews, G.C.; Sela, M.; Yarden, Y. The ErbB-2/HER2 oncoprotein of human carcinomas may function solely as a shared coreceptor for multiple stroma-derived growth factors. Proc. Natl. Acad. Sci. USA 1999, 96, 4995–5000. [Google Scholar] [CrossRef]
- Karunagaran, D.; Tzahar, E.; Beerli, R.R.; Chen, X.; Graus-Porta, D.; Ratzkin, B.J.; Seger, R.; Hynes, N.E.; Yarden, Y. ErbB-2 is a common auxiliary subunit of NDF and EGF receptors: Implications for breast cancer. EMBO J. 1996, 15, 254–264. [Google Scholar] [CrossRef]
- Petit, A.M.; Rak, J.; Hung, M.C.; Rockwell, P.; Goldstein, N.; Fendly, B.; Kerbel, R.S. Neutralizing antibodies against epidermal growth factor and ErbB-2/neu receptor tyrosine kinases down-regulate vascular endothelial growth factor production by tumor cells in vitro and in vivo: Angiogenic implications for signal transduction therapy of solid tumors. Am. J. Pathol. 1997, 151, 1523–1530. [Google Scholar]
- Giatromanolaki, A.; Koukourakis, M.I.; Simopoulos, C.; Polychronidis, A.; Gatter, K.C.; Harris, A.L.; Harris, A.L.; Sivridis, E. c-erbB-2 related aggressiveness in breast cancer is hypoxia inducible factor-1alpha dependent. Clin. Cancer Res. 2004, 10, 7972. [Google Scholar] [CrossRef]
- Prat, A.; Parker, J.S.; Karginova, O.; Fan, C.; Livasy, C.; Herschkowitz, J.I.; He, X.; Perou, C.M. Phenotypic and molecular characterization of the claudin-low intrinsic subtype of breast cancer. Breast Cancer Res. 2010, 12, R68. [Google Scholar] [CrossRef]
- Teschendorff, A.E.; Miremadi, A.; Pinder, S.E.; Ellis, I.O.; Caldas, C. An immune response gene expression module identifies a good prognosis subtype in estrogen receptor negative breast cancer. Genome Biol. 2007, 8, R157. [Google Scholar] [CrossRef] [PubMed]
- Kreike, B.; van Kouwenhove, M.; Horlings, H.; Weigelt, B.; Peterse, H.; Bartelink, H.; van de Vijver, M.J. Gene expression profiling and histopathological characterization of triple-negative/basal-like breast carcinomas. Breast Cancer Res. 2007, 9, R65. [Google Scholar] [CrossRef]
- Nielsen, T.O.; Hsu, F.D.; Jensen, K.; Cheang, M.; Karaca, G.; Hu, Z.; Hernandez-Boussard, T.; Livasy, C.; Cowan, D.; Dressler, L.; et al. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin. Cancer Res. 2004, 10, 5367–5374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, T.; Iwaya, K.; Moriya, T.; Yamasaki, T.; Tsuda, H.; Yamamoto, J.; Matsubara, O. A simple immunohistochemical panel comprising 2 conventional markers, Ki67 and p53, is a powerful tool for predicting patient outcome in luminal-type breast cancer. BMC Clin. Pathol. 2013, 13, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Age at Diagnosis | N (%) | Total | |
|---|---|---|---|
| ≤50 yr | 353 (33.4%) | - | |
| >50 yr | 705 (66.6%) | - | 1058 |
| Menopausal status | N (%) | Total | |
| Premenopausal | 297 (28.1%) | - | |
| Postmenopausal | 756 (71.4%) | - | |
| Unknown | 5 (0.5%) | - | 1058 |
| Histopathology | N (%) | Total | |
| Invasive ductal | 887 (83.8%) | - | |
| Invasive lobular | 118 (11.2%) | - | |
| Mixed | 53 (5%) | - | 1058 |
| Grade | N (%) | Total | |
| I | 26 (2.4%) | - | |
| II | 765 (72.3%) | - | |
| III | 263 (24.9%) | - | |
| Unknown | 4 (0.4%) | - | 1058 |
| Tumor size | N (%) | Total | |
| T1 | 695 (65.7%) | - | |
| T2 | 323 (30.5%) | - | |
| T3 | 22 (2.1%) | - | |
| Unknown | 18 (1.7%) | - | 1058 |
| Axillary involvement | No | Yes | Total |
| Any axillary involvement | 628 (59.5%) | 428 (40.5%) | 1056 |
| ≥pN1 (macroscopic involvement) | 711 (67.3%) | 345 (32.7%) | 1056 |
| ≥pN2 | 893 (84.6%) | 163 (15.4%) | 1056 |
| BC location | Unilateral | Bilateral | Total |
| 1043 (98.6%) | 15 (1.4%) | 1058 | |
| IHC parameters | Negative | Positive | Total |
| ER | 222 (21%) | 836 (79%) | |
| PR | 429 (40.5%) | 629 (59.5%) | |
| HER2 | 829 (78.4%) | 229 (21.6%) | |
| Ki67 | 285 (26.9%) | 773 (73.1%) | |
| p53 | 561 (53%) | 497 (47%) | 1058 |
| Clinico-pathologic surrogate of the intrinsic subtypes (St. Gallen 2013) | N (%) | Rest (%) | Total |
| Luminal A | 285 (26.9%) | 773 (73.1%) | |
| Luminal B (HER2 negative) | 404 (38.2%) | 654 (61.8%) | |
| Luminal B (HER2 positive) | 147 (13.9%) | 911 (86.1%) | |
| HER 2 Non luminal | 82 (7.8%) | 976 (92.2%) | |
| Triple negative (ductal) | 140 (13.2%) | 918 (86.8%) | 1058 |
| St. Gallen Consensus Categories and Subcategories | Distribution of BC Patients N (%) | Any axillary Involvement. N (%) | Axillary Macroscopic Involvement. N (%) | Axillary Involvement pN2 or More. N (%) |
|---|---|---|---|---|
| Luminal-A like | 285 (26.9) | 103 (36.1) | 73 (25.6) | 21 (7.4) |
| p53 low | 262 (24.8) | 99 (37.8) | 71 (27.1) | 19 (7.3) |
| p53 high | 17 (1.6) | 4 (23.5) | 2 (11.8) | 2 (11.8) |
| Luminal-B like (HER2 negative) | 404 (38.2) | 185 (45.8) | 153 (37.9) | 68 (16.8) |
| Ki67 high, PR positive | 248 (23.4) | 116 (46.8) | 98 (39.5) | 40 (16.1) |
| Ki67 low, PR negative | 75 (7.1) | 31 (41.3) | 24 (32.0) | 12 (16.0) |
| Ki67 high, PR negative | 81 (7.7) | 38 (46.9) | 31 (38.3) | 16 (19.8) |
| Luminal-B like (HER2 positive) | 147 (13.9) | 49 (33.8) | 37 (25.5) | 20 (13.8) |
| Ki67 high, PR positive | 70 (6.6) | 25 (35.7) | 21 (30.0) | 10 (14.3) |
| Ki67 low, PR negative | 11 (1.0) | 5 (45.5) | 4 (36.4) | 3 (27.3) |
| Ki67 high, PR negative | 40 (3.8) | 13 (34.2) | 6 (15.8) | 4 (10.5) |
| Ki67 low, PR positive | 26 (2.5) | 6 (23.1) | 6 (23.1) | 3 (11.5) |
| HER2 overexpression | 82 (7.8) | 35 (42.7) | 31 (37.8) | 23 (28.0) |
| Ki67 low, p53 low | 6 (0.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Ki67 high, p53 low | 36 (3.4) | 17 (47.2) | 15 (41.7) | 10 (27.8) |
| Ki67 high, p53 high | 35 (3.3) | 16 (45.7) | 14 (40.0) | 11 (31.4) |
| Ki67 low, p53 high | 3 (0.3) | 1 (33.3) | 1 (33.3) | 1 (33.3) |
| Triple-negative | 140 (13.2) | 56 (40.0) | 51 (36.4) | 31 (22.1) |
| Ki67 low, p53 low | 24 (2.3) | 10 (41.7) | 9 (37.5) | 4 (16.7) |
| Ki67 high, p53 low | 45 (4.3) | 15 (33.3) | 14 (31.1) | 9 (20.0) |
| Ki67 high, p53 high | 63 (6) | 28 (44.4) | 25 (39.7) | 16 (25.4) |
| Ki67 low, p53 high | 6 (0.6) | 2 (33.3) | 2 (33.3) | 2 (33.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, A.; Siegrist, J.; Lizarraga, S.; Pérez-Medina, T. Clustering Molecular Subtypes in Breast Cancer, Immunohistochemical Parameters and Risk of Axillary Nodal Involvement. J. Pers. Med. 2022, 12, 1404. https://doi.org/10.3390/jpm12091404
Pereira A, Siegrist J, Lizarraga S, Pérez-Medina T. Clustering Molecular Subtypes in Breast Cancer, Immunohistochemical Parameters and Risk of Axillary Nodal Involvement. Journal of Personalized Medicine. 2022; 12(9):1404. https://doi.org/10.3390/jpm12091404
Chicago/Turabian StylePereira, Augusto, Jaime Siegrist, Santiago Lizarraga, and Tirso Pérez-Medina. 2022. "Clustering Molecular Subtypes in Breast Cancer, Immunohistochemical Parameters and Risk of Axillary Nodal Involvement" Journal of Personalized Medicine 12, no. 9: 1404. https://doi.org/10.3390/jpm12091404
APA StylePereira, A., Siegrist, J., Lizarraga, S., & Pérez-Medina, T. (2022). Clustering Molecular Subtypes in Breast Cancer, Immunohistochemical Parameters and Risk of Axillary Nodal Involvement. Journal of Personalized Medicine, 12(9), 1404. https://doi.org/10.3390/jpm12091404