
Clinical, Imaging and Neurogenetic Features of Patients with Gliomatosis Cerebri Referred to a Tertiary Neuro-Oncology Centre
 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Inclusion Criteria and Study Population
2.2. Demographic Data, Imaging and Pathology
2.3. Imaging Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics and Presenting Symptoms
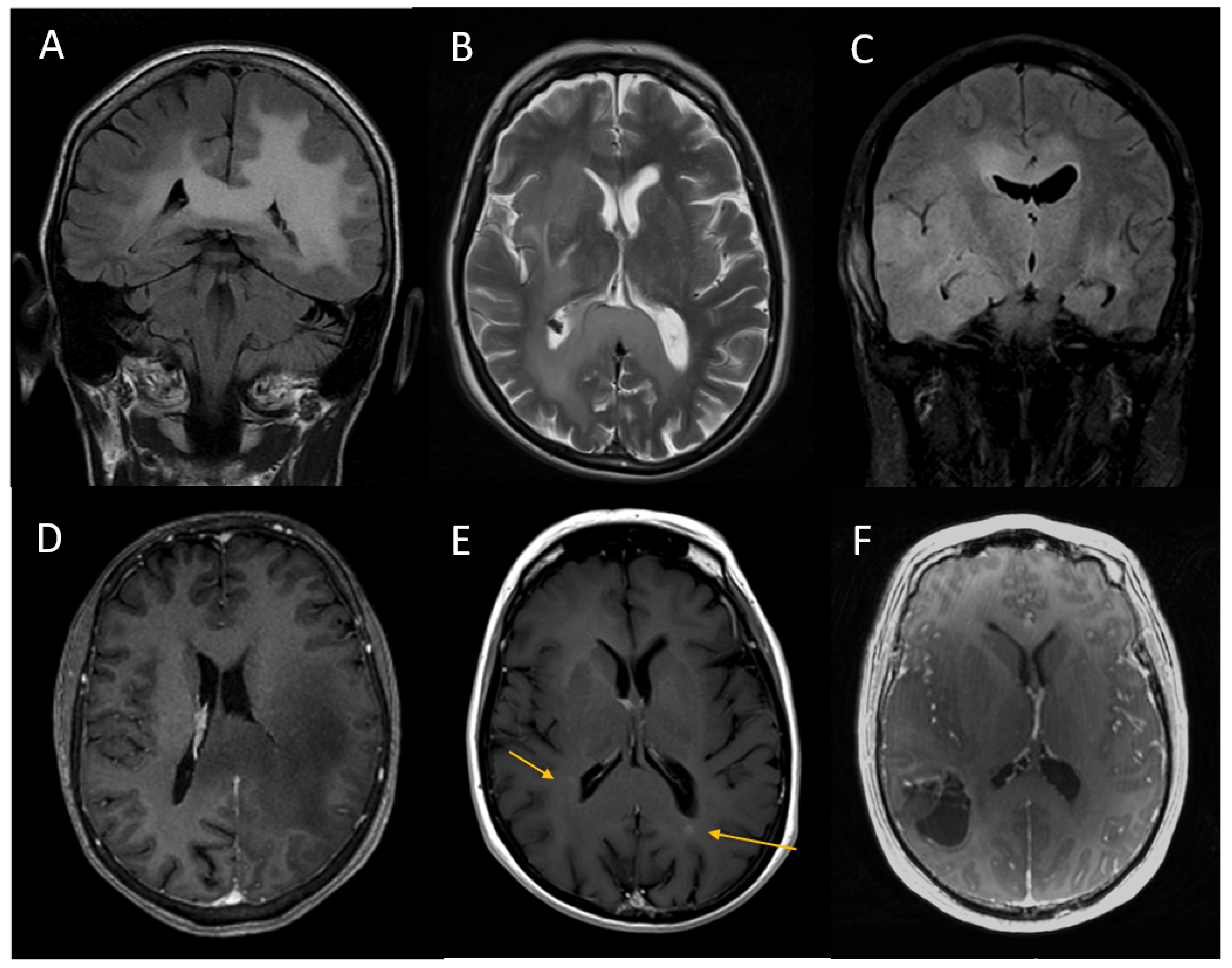
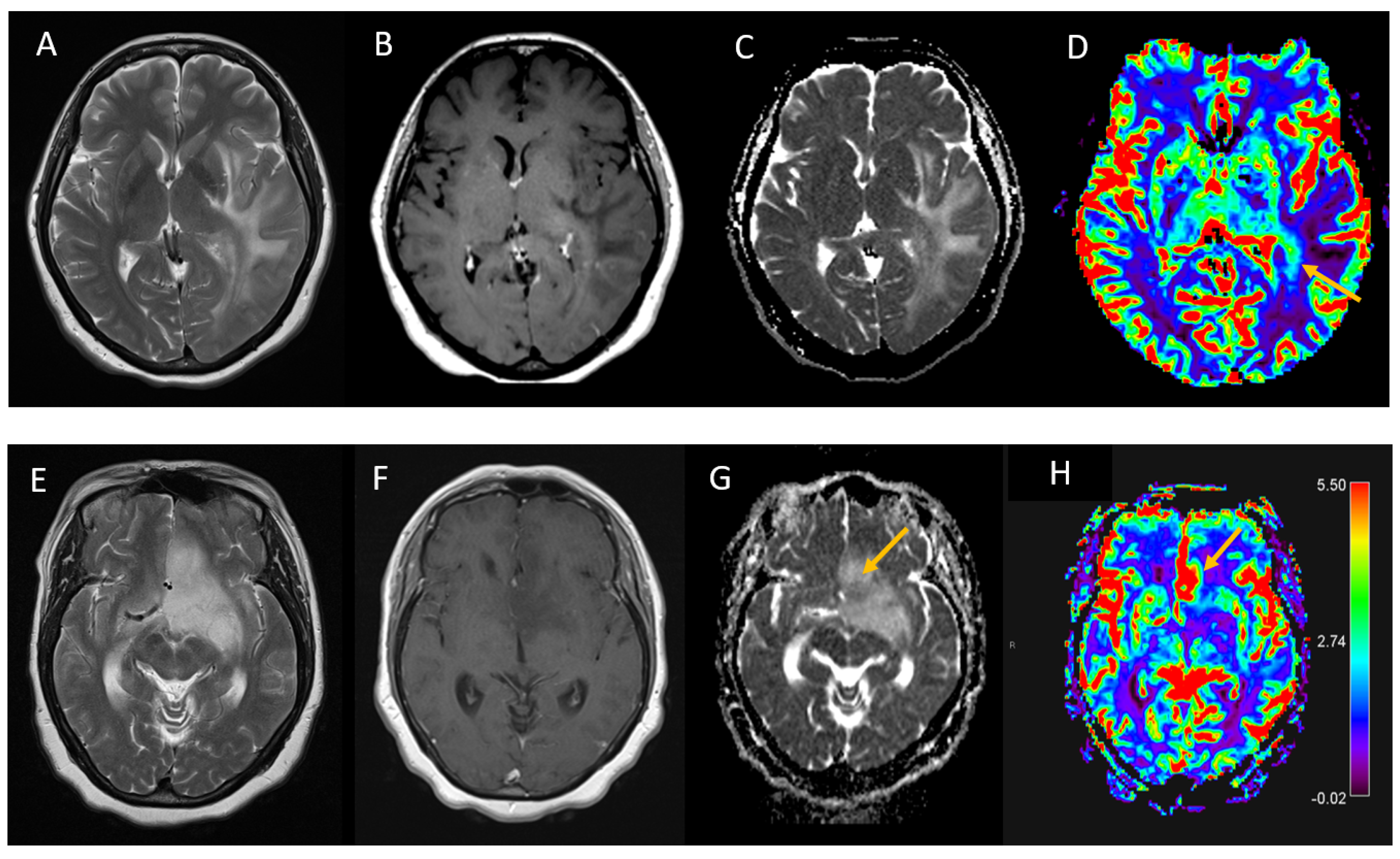
3.2. Imaging Tumour Characteristics
3.3. Histological Grade and Genetic Tumour Characteristics
3.4. Treatment
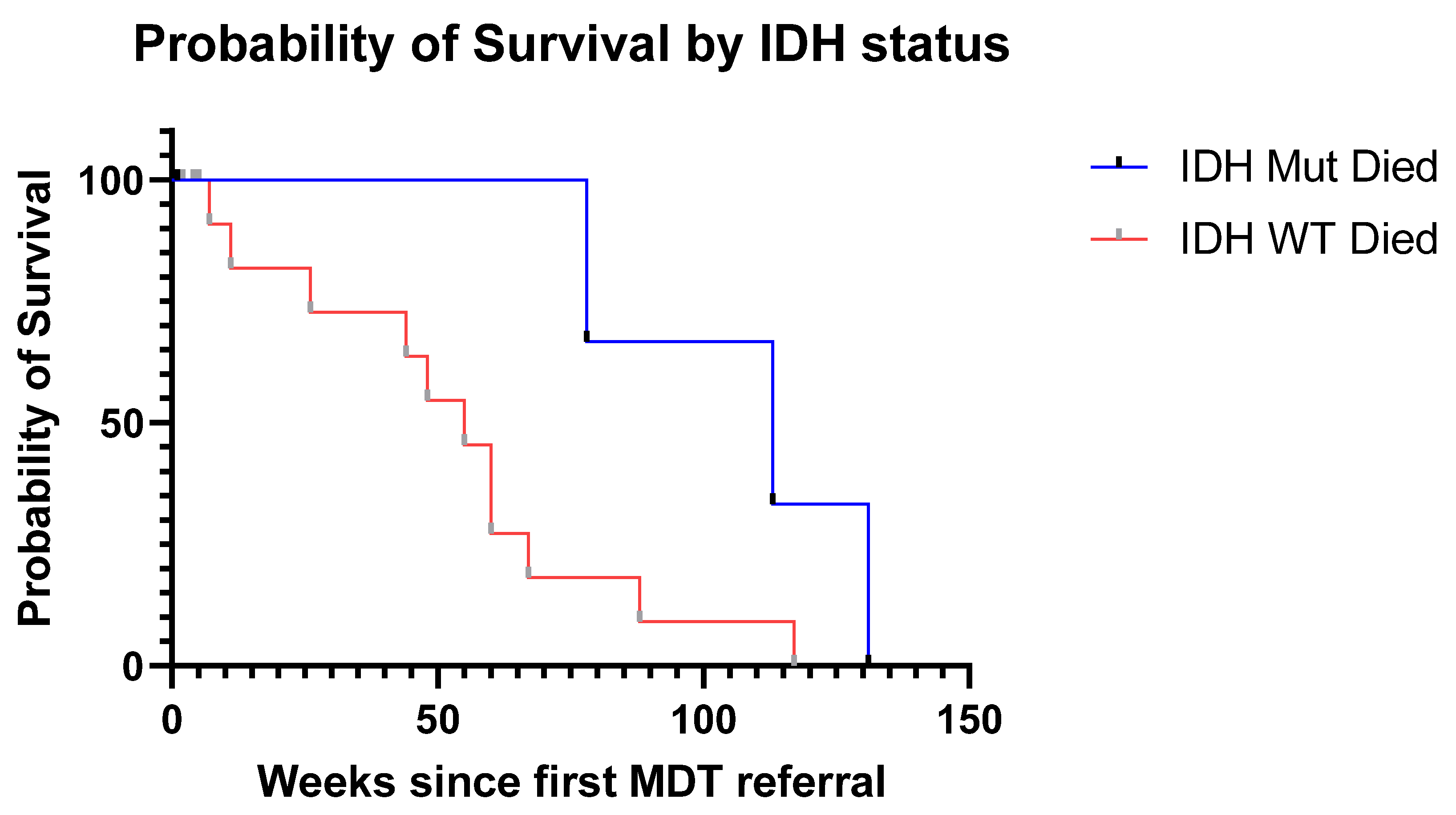
3.5. Survival
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nevin, S. Gliomatosis cerebri. Brain 1938, 61, 170–191. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranjan, S.; Warren, K.E. Gliomatosis cerebri: Current understanding and controversies. Front. Oncol. 2017, 7, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalafallah, A.; Kopparapu, S.; Mukherjee, D. Predictive factors for overall survival in surgical cases of gliomatosis cerebri from the national cancer database. Neuro-Oncology 2020, 22, 88–89. [Google Scholar] [CrossRef]
- Georgakis, M.K.; Spinos, D.; Pourtsidis, A.; Psyrri, A.; Panourias, I.G.; Sgouros, S.; Petridou, E.T. Incidence and survival of gliomatosis cerebri: A population-based cancer registration study. J. Neuro-Oncol. 2018, 138, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.H.; Poisson, L.M.; Brat, D.J.; Zhou, Y.; Cooper, L.; Snuderl, M.; Thomas, C.; Franceschi, A.M.; Griffith, B.; Flanders, A.E. T2–FLAIR mismatch, an imaging biomarker for IDH and 1p/19q status in lower-grade gliomas: A TCGA/TCIA project. Clin. Cancer Res. 2017, 23, 6078–6085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thust, S.; Hassanein, S.; Bisdas, S.; Rees, J.; Hyare, H.; Maynard, J.; Brandner, S.; Tur, C.; Jäger, H.; Yousry, T. Apparent diffusion coefficient for molecular subtyping of non-gadolinium-enhancing WHO grade II/III glioma: Volumetric segmentation versus two-dimensional region of interest analysis. Eur. Radiol. 2018, 28, 3779–3788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, M.; Young, R.J.; Babb, J.S.; Peccerelli, N.; Chheang, S.; Gruber, M.L.; Miller, D.C.; Golfinos, J.G.; Zagzag, D.; Johnson, G. Gliomas: Predicting time to progression or survival with cerebral blood volume measurements at dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging. Radiology 2008, 247, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Rajz, G.G.; Nass, D.; Talianski, E.; Pfeffer, R.; Spiegelmann, R.; Cohen, Z.R. Presentation patterns and outcome of gliomatosis cerebri. Oncol. Lett. 2012, 3, 209–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kernick, D.P.; Ahmed, F.; Bhara, A.; Dowson, A.; Elrington, G.; Fontebasso, M.; Giffin, N.J.; Lipscombe, S.; McGregor, A.; Peatfield, R.; et al. Imaging patients with suspected brain tumour; guidance for primary care. Br. J. Gen. Pract. 2010, 58, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Filley, C.M.; Kleinschmidt-DeMasters, B.K.; Lillehei, K.O.; Damek, D.M.; Josette, H. Gliomatosis cerebri: Neurobehavioural and neuropathological observations. Cogn. Behav. Neurol. 2003, 16, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Desclée, P.; Rommel, D.; Hernalsteen, D.; Godfraind, C.; de Coene, B.; Cosnard, G. Gliomatosis cerebri, imaging findings of 12 cases. J. Neuroradiol. 2010, 37, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Freund, M.; Hähnel, S.; Sommer, C.; Martmann, M.; Kiessling, M.; Tronnier, V.; Sartor, K. CT and MRI findings in gliomatosis cerebri: A neuroradiologic and neuropathologic review of diffuse infiltrating brain neoplasms. Eur. Radiol. 2001, 11, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Viton, P.; Brunel, H.; Chinot, O.; Daniel, C.; Barrié, M.; Bouvier, C.; Figarella-Branger, D.; Fuentes, S.; Dufour, H.; Grisoli, F. Histological and MR correlations in Gliomatosis cerebri. J. Neuro-Oncol. 2002, 59, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Georgakis, M.K.; Tsivgoulis, G.; Spinos, D.; Dimitriou, N.G.; Kyritsis, A.P.; Herrlinger, U.; Petridou, E.T. Clinical, neuroimaging and histopathological features of gliomatosis cerebri: A systematic review based on synthesis of published individual patient data. J. Neuro-Oncol. 2018, 140, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Förster, A.; Brehmer, S.; Seiz-Rosenhagen, M.; Mildenberger, I.; Giordano, F.A.; Wenz, H.; Reuss, D.; Hänggi, D.; Groden, C. Heterogeneity of glioblastoma with gliomatosis cerebri growth pattern on diffusion and perfusion MRI. J. Neuro-Oncol. 2019, 142, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Thust, S.; Heiland, S.; Falini, A.; Jäger, H.; Waldman, A.; Sundgren, P.; Godi, C.; Katsaros, V.; Ramos, A.; Bargallo, N. Glioma imaging in Europe: A survey of 220 centres and recommendations for best clinical practice. Eur. Radiol. 2018, 28, 3306–3317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, G.T.; Phillips, P.C.; Rorke-Adams, L.B.; Judkins, A.R.; Localio, A.R.; Fisher, M.J. Gliomatosis cerebri: 20 years of experience at the Children’s Hospital of Philadelphia. Cancer 2006, 107, 1597–1606. [Google Scholar] [CrossRef] [PubMed]
- Bellu, L.; Caccese, M.; Cerretti, G.; Berti, F.; Busato, F.; Parisi, A.; Padovan, M.; Zagonel, V.; Lombardi, G. Gliomatosis cerebri: A monocentric real-life experience. J. Cancer Metastasis Treat. 2021, 7, 29. [Google Scholar] [CrossRef]
- Herrlinger, U.; Jones, D.T.; Glas, M.; Hattingen, E.; Gramatzki, D.; Stuplich, M.; Felsberg, J.; Bähr, O.; Gielen, G.H.; Simon, M. Gliomatosis cerebri: No evidence for a separate brain tumor entity. Acta Neuropathol. 2016, 131, 309–319. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristic | |
|---|---|
| Female sex (n, %) | 9 (31%) |
| Age at date of referral (median, IQR) | 64 years (48 to 69) |
| External referral (n, %) | 18 (62%) |
| Initial symptoms (n, %) | |
| - Neuropsychiatric | 9 (31%) |
| - Seizure | 7 (24%) |
| - Headache | 6 (21%) |
| - Focal weakness | 5 (17%) |
| - Language disorder | 3 (10%) |
| - Nausea and vomiting | 2 (7%) |
| - Visual disturbance | 2 (7%) |
| Imaging Feature | ||
|---|---|---|
| Number of supratentorial lobes involved on MRI (mean, range) | 5 | (3 to 8) |
| Number of brain regions involved on MRI (mean, range) | 7 | (5 to 9) |
| Median lowest ADCmean within the tumour (×10−3 mm2/s, IQR) | 0.81 | 0.64 to 0.90 |
| Median ADCmean within the tumour (×10−3 mm2/s, SD) | 0.97 | 0.87 to 1.01 |
| Median ADCmean in normal white matter (×10−3 mm2/s, SD) | 0.75 | 0.73 to 0.82 |
| T2/FLAIR Mismatch (n, %) | 0 | (0%) |
| Advanced imaging performed (DSC perfusion or MRS) (n, %) | 8 | (28%) |
| Patient Number | Age at Referral | WHO Grade (Where Available) | Histological Diagnosis | IDH Mutation Status (Where Available) (1 = Mutant, 0 = Wild Type) | Number of Supratentorial Lobes Involved on Imaging |
|---|---|---|---|---|---|
| 1 | 49 | 2 | Diffuse Astrocytoma | 1 | 8 |
| 2 | 67 | Non-diagnostic biopsy | 3 | ||
| 3 | 68 | 4 | Glioblastoma | 0 | 8 |
| 4 | 56 | 6 | |||
| 5 | 67 | 4 | Glioblastoma | 0 | 8 |
| 6 | 65 | 3 | “Gliomatosis Cerebri” | 8 | |
| 7 | 51 | 2 | Diffuse Astrocytoma | 0 | 4 |
| 8 | 43 | 3 | |||
| 9 | 69 | 2 | Diffuse Astrocytoma | 0 | 8 |
| 10 | 27 | 2 | Diffuse Astrocytoma | 0 | 3 |
| 11 | 64 | 2 | Diffuse Astrocytoma | 1 | 6 |
| 12 | 33 | 2 | Diffuse Astrocytoma | 0 | 6 |
| 13 | 74 | “Low Grade Glioma” | 2 | ||
| 14 | 51 | 4 | Glioblastoma | 0 | 4 |
| 15 | 27 | 3 | Anaplastic Astrocytoma | 0 | 4 |
| 16 | 48 | 2 | Diffuse Astrocytoma | 1 | 5 |
| 17 | 80 | 4 | |||
| 18 | 70 | 4 | Glioblastoma | 0 | 8 |
| 19 | 68 | Non-diagnostic biopsy | 5 | ||
| 20 | 47 | 3 | Anaplastic Astrocytoma | 1 | 5 |
| 21 | 70 | Gemistocystic Astrocytoma | 0 | 3 | |
| 22 | 43 | 2 | Astrocytoma | 1 | 8 |
| 23 | 18 | 3 | Anaplastic Astrocytoma | 3 | |
| 24 | 79 | 4 | Glioblastoma | 0 | 3 |
| 25 | 57 | 3 | Pleomorphic Xanthastrocytoma | 0 | 3 |
| 26 | 65 | 3 | Anaplastic Astrocytoma | 0 | 4 |
| 27 | 75 | 4 | Glioblastoma | 6 | |
| 28 | 71 | 4 | Glioblastoma | 0 | 8 |
| 29 | 54 | 4 | Glioblastoma | 0 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doig, D.; Thorne, L.; Rees, J.; Fersht, N.; Kosmin, M.; Brandner, S.; Jäger, H.R.; Thust, S. Clinical, Imaging and Neurogenetic Features of Patients with Gliomatosis Cerebri Referred to a Tertiary Neuro-Oncology Centre. J. Pers. Med. 2023, 13, 222. https://doi.org/10.3390/jpm13020222
Doig D, Thorne L, Rees J, Fersht N, Kosmin M, Brandner S, Jäger HR, Thust S. Clinical, Imaging and Neurogenetic Features of Patients with Gliomatosis Cerebri Referred to a Tertiary Neuro-Oncology Centre. Journal of Personalized Medicine. 2023; 13(2):222. https://doi.org/10.3390/jpm13020222
Chicago/Turabian StyleDoig, David, Lewis Thorne, Jeremy Rees, Naomi Fersht, Michael Kosmin, Sebastian Brandner, Hans Rolf Jäger, and Stefanie Thust. 2023. "Clinical, Imaging and Neurogenetic Features of Patients with Gliomatosis Cerebri Referred to a Tertiary Neuro-Oncology Centre" Journal of Personalized Medicine 13, no. 2: 222. https://doi.org/10.3390/jpm13020222
APA StyleDoig, D., Thorne, L., Rees, J., Fersht, N., Kosmin, M., Brandner, S., Jäger, H. R., & Thust, S. (2023). Clinical, Imaging and Neurogenetic Features of Patients with Gliomatosis Cerebri Referred to a Tertiary Neuro-Oncology Centre. Journal of Personalized Medicine, 13(2), 222. https://doi.org/10.3390/jpm13020222