
Mandibular Crowding: Diagnosis and Management—A Scoping Review

 ,
,  ,
,  ,
,  , ,
, ,  ,
,  , ,
, ,  , , ,
, , , 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
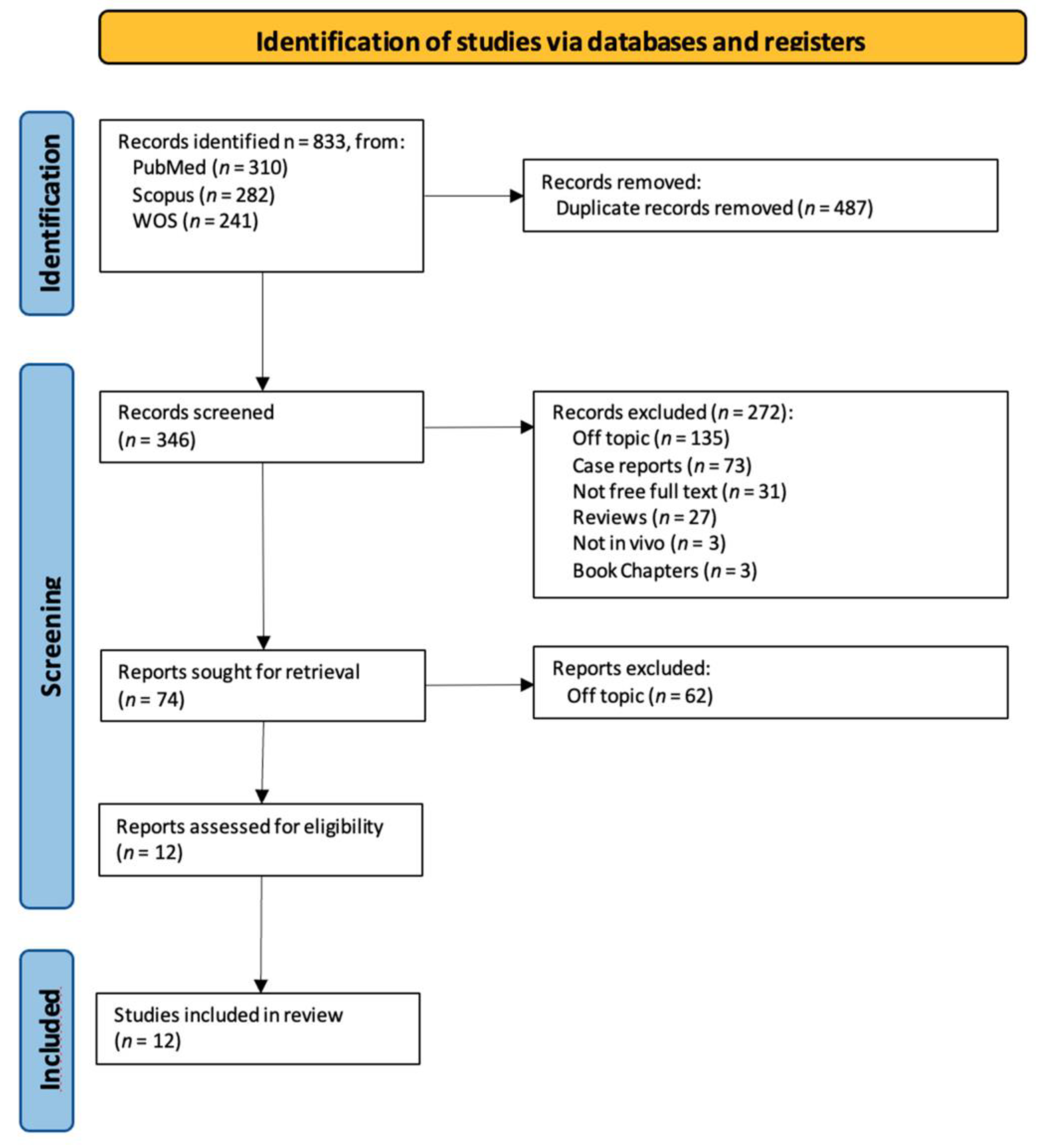
2.2. Search Processing
2.3. Eligibility Criteria
2.4. Data Processing
3. Results
4. Discussion
4.1. Diagnostic Methods
4.2. Prophylaxis
4.3. Treatment
4.4. Treatment Stability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RME | Rapid maxillary expansion |
| LB | Lip bumper |
| ARS | Air-rotor stripping |
| CBCT | Cone beam computed tomography |
References
- Normando, D.; Almeida, M.A.O.; Quintão, C.C.A. Dental Crowding. Angle Orthod. 2013, 83, 10–15. [Google Scholar] [CrossRef]
- Jadhav, V.; Tiwari, M.; Seegavadi, V.; Kamble, R.; Daigavane, P. A Formula for Estimating the Mesiodistal Width of Permanent Mandibular Central Incisors. J. Datta Meghe Inst. Med. Sci. Univ. 2021, 16, 29–32. [Google Scholar] [CrossRef]
- Rizzo, C.; Di Bartolo, I.; Santantonio, M.; Coscia, M.F.; Monno, R.; De Vito, D.; Ruggeri, F.M.; Rizzo, G. Epidemiological and Virological Investigation of a Norovirus Outbreak in a Resort in Puglia, Italy. BMC Infect. Dis. 2007, 7, 135. [Google Scholar] [CrossRef]
- De Vito, D.; Monno, R.; Nuccio, F.; Legretto, M.; Oliva, M.; Coscia, M.F.; Dionisi, A.M.; Calia, C.; Capolongo, C.; Pazzani, C. Diffusion and Persistence of Multidrug Resistant Salmonella Typhimurium Strains Phage Type DT120 in Southern Italy. BioMed Res. Int. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Coscia, M.F.; Monno, R.; Ballini, A.; Mirgaldi, R.; Dipalma, G.; Pettini, F.; Cristallo, V.; Inchingolo, F.; Foti, C.; De Vito, D. Human Papilloma Virus (HPV) Genotypes Prevalence in a Region of South Italy (Apulia). Ann. Dell’istituto Super. Di Sanita 2015, 51, 248–251. [Google Scholar] [CrossRef]
- Paul, S.; Garg, S.; Saraf, B.G.; Sheoran, N.; Chawla, M.; Saji, S.E. Arch Measurements, Bigonial Width, Dental Caries, and Their Effect on Occurrence of Mandibular Incisors Crowding in Early Mixed Dentition Period. Int. J. Clin. Pediatr. Dent. 2021, 14, S57–S62. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef]
- Maspero, C.; Fama, A.; Cavagnetto, D.; Abate, A.; Farronato, M. Treatment of Dental Dilacerations. J. Biol. Regul. Homeost. Agents 2019, 33, 1623–1627. [Google Scholar]
- Grainger, R.M. Orthodontic Treatment Priority Index; Vital Health Stat 2; United States Department of Health, Education, and Welfare: Washington, DC, USA, 1967; pp. 1–49. [Google Scholar]
- Cazzolla, A.P.; Zhurakivska, K.; Ciavarella, D.; Lacaita, M.G.; Favia, G.; Testa, N.F.; Marzo, G.; La Carbonara, V.; Troiano, G.; Lo Muzio, L. Primary Hyperoxaluria: Orthodontic Management in a Pediatric Patient: A Case Report. Spec. Care Dent. 2018, 38, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Lo Russo, L.; Ciavarella, D.; Salamini, A.; Guida, L. Alignment of Intraoral Scans and Registration of Maxillo-Mandibular Relationships for the Edentulous Maxillary Arch. J. Prosthet. Dent. 2019, 121, 737–740. [Google Scholar] [CrossRef]
- Cassano, M.; Russo, G.; Granieri, C.; Ciavarella, D. Modification of Growth, Immunologic and Feeding Parameters in Children with OSAS after Adenotonsillectomy. Acta Otorhinolaryngol. Ital. 2018, 38, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Abate, A.; Inchingolo, F.; Dolci, C.; Cagetti, M.G.; Tartaglia, G.M. Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report. Children 2022, 9, 421. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Maspero, C.; Abate, A.; Grippaudo, C.; Connelly, S.T.; Tartaglia, G.M. 3D Cephalometry on Reduced FOV CBCT: Skeletal Class Assessment through AF-BF on Frankfurt Plane-Validity and Reliability through Comparison with 2D Measurements. Eur. Radiol. 2020, 30, 6295–6302. [Google Scholar] [CrossRef]
- Ergoren, M.C.; Paolacci, S.; Manara, E.; Dautaj, A.; Dhuli, K.; Anpilogov, K.; Camilleri, G.; Suer, H.K.; Sayan, M.; Tuncel, G.; et al. A Pilot Study on the Preventative Potential of Alpha-Cyclodextrin and Hydroxytyrosol against SARS-CoV-2 Transmission. Acta Bio Med. Atenei Parm. 2020, 91, e2020022. [Google Scholar] [CrossRef]
- Maspero, C. Operculectomy and Spontaneous Eruption of Impacted Second Molars: A Retrospective Study. J. Biol. Regul. Homeost. Agents 2019, 33, 1909–1912. [Google Scholar] [CrossRef]
- Maspero, C.; Cappella, A.; Dolci, C.; Cagetti, M.G.; Inchingolo, F.; Sforza, C. Is Orthodontic Treatment with Microperforations Worth It? A Scoping Review. Children 2022, 9, 208. [Google Scholar] [CrossRef]
- Das, P.J.; Dkhar, W.; Pradhan, A. An Evaluation of Dental Crowding in Relation to the Mesiodistal Crown Widths and Arch Dimensions in Southern Indian Population. J. Clin. Diagn. Res. 2017, 11, TC10–TC13. [Google Scholar] [CrossRef] [PubMed]
- Ciavarella, D.; Monsurrò, A.; Padricelli, G.; Battista, G.; Laino, L.; Perillo, L. Unilateral Posterior Crossbite in Adolescents: Surface Electromyographic Evaluation. Eur. J. Paediatr. Dent. 2012, 13, 25–28. [Google Scholar]
- Inchingolo, A.M.; Fatone, M.C.; Malcangi, G.; Avantario, P.; Piras, F.; Patano, A.; Di Pede, C.; Netti, A.; Ciocia, A.M.; De Ruvo, E.; et al. Modifiable Risk Factors of Non-Syndromic Orofacial Clefts: A Systematic Review. Children 2022, 9, 1846. [Google Scholar] [CrossRef] [PubMed]
- Brunelle, J.A.; Bhat, M.; Lipton, J.A. Prevalence and Distribution of Selected Occlusal Characteristics in the US Population, 1988–1991. J. Dent. Res. 1996, 75, 706–713. [Google Scholar] [CrossRef]
- Jain, R. Prevalence of Mandibular Anterior Teeth Crowding in Mixed Dentition Subjects Reporting to a University Hospital in Chennai City. Int. J. Dent. Oral Sci. 2019, S3, 6–11. [Google Scholar] [CrossRef]
- Grippaudo, M.M.; Quinzi, V.; Manai, A.; Paolantonio, E.G.; Valente, F.; La Torre, G.; Marzo, G. Orthodontic Treatment Need and Timing: Assessment of Evolutive Malocclusion Conditions and Associated Risk Factors. Eur. J. Pediatr. Dent. 2020, 21, 203–208. [Google Scholar] [CrossRef]
- Farronato, M.; Boccalari, E.; Del Rosso, E.; Lanteri, V.; Mulder, R.; Maspero, C. A Scoping Review of Respirator Literature and a Survey among Dental Professionals. Int. J. Environ. Res. Public Health 2020, 17, 5968. [Google Scholar] [CrossRef]
- Leighton, B.C. The Early Signs of Malocclusion. Eur. J. Orthod. 2007, 29, i89–i95. [Google Scholar] [CrossRef]
- Quinzi, V.; Caruso, S.; Mummolo, S.; Nota, A.; Angelone, A.M.; Mattei, A.; Gatto, R.; Marzo, G. Evaluation of Lower Dental Arch Crowding and Dimension after Treatment with Lip Bumper versus Schwarz Appliance. A Prospective Pilot Study. Dent. J. 2020, 8, 34. [Google Scholar] [CrossRef]
- Jain, R. Association Of Mandibular Arch Crowding And Vertical Growth Pattern—A Retrospective Study. Int. J. Dent. Oral Sci. 2021, 8, 4096–4100. [Google Scholar] [CrossRef]
- Satra, P.; Vichare, G.; Bhosale, V. Relationship of Maxillary and Mandibular Effective Base Length, Arch Length and Dental Crowding in Different Vertical Growth Pattern. APOS 2022, 12, 108–114. [Google Scholar] [CrossRef]
- Antoszewska-Smith, J.; Bohater, M.; Kawala, M.; Sarul, M.; Rzepecka-Skupień, M. Treatment of Adults with Anterior Mandibular Teeth Crowding: Reliability of Little’s Irregularity Index. Int. J. Dent. 2017, 2017, 5057941. [Google Scholar] [CrossRef]
- Di Ventura, A.; Lanteri, V.; Farronato, G.; Gaffuri, F.; Beretta, M.; Lanteri, C.; Cossellu, G. Three-Dimensional Evaluation of Rapid Maxillary Expansion Anchored to Primary Molars: Direct Effects on Maxillary Arch and Spontaneous Mandibular Response. Eur. J. Pediatr. Dent. 2019, 20, 38–42. [Google Scholar] [CrossRef]
- Griswold, O.; Li, C.; Orr, J.; Boucher, N.; Shah, S.; Chung, C.-H. Lip Bumper Therapy Does Not Influence the Sagittal Mandibular Incisor Position in a Retrospective CBCT Study. J. Clin. Med. 2022, 11, 6032. [Google Scholar] [CrossRef] [PubMed]
- Nakhjavani, Y.B.; Nakhjavani, F.B.; Jafari, A. Mesial Stripping of Mandibular Deciduous Canines for Correction of Permanent Lateral Incisors. Int. J. Clin. Pediatr. Dent. 2017, 10, 229–233. [Google Scholar] [CrossRef]
- Verma Comparative Evaluation of Stability of Mandibular Anterior Crowding Correction Done with Two Different Treatment Protocols: A Retrospective Study. Available online: https://www.jioh.org/article.asp?issn=0976-7428;year=2022;volume=14;issue=2;spage=189;epage=194;aulast=Verma (accessed on 24 January 2023).
- Persson, M.; Al-Taai, N.; Pihlgren, K.; Westerlund, A. Early Extractions of Premolars Reduce Age-Related Crowding of Lower Incisors: 50 Years of Follow-Up. Clin. Oral Investig. 2022, 26, 4525–4535. [Google Scholar] [CrossRef]
- Berbert, M.; Cotrin, P.; de Oliveira, R.G.; de Oliveira, R.G.; Valarelli, F.P.; de Freitas, M.R.; Freitas, K.M.S. The Influence of 3x3 Bonded Retainer on Anterior Crowding Relapse in Mandibular Incisor Extraction Cases. Dent. Press J. Orthod. 2021, 26, e212081. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Goizueta, O.E.F.M.; Garib, D.G.; Janson, M. Relationship between Maxillary and Mandibular Base Lengths and Dental Crowding in Patients with Complete Class II Malocclusions. Angle Orthod. 2011, 81, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Shivaprakash, G. To Evaluate the Correlation Between Skeletal and Dental Parameters to the Amount of Crowding in Class II Div. 1 Malocclusions. J. Clin. Diagn. Res. 2017, 11, ZC22–ZC27. [Google Scholar] [CrossRef]
- Pasciuti, E.; Coloccia, G.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Bordea, I.R.; Cardarelli, F.; Di Venere, D.; Inchingolo, F.; Dipalma, G. Deep Bite Treatment with Aligners: A New Protocol. Appl. Sci. 2022, 12, 6709. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Carpentiere, V.; Piras, F.; Netti, A.; Ferrara, I.; Campanelli, M.; Latini, G.; Viapiano, F.; Costa, S.; Malcangi, G.; et al. Orthodontic Surgical Treatment of Impacted Mandibular Canines: Systematic Review and Case Report. Appl. Sci. 2022, 12, 8008. [Google Scholar] [CrossRef]
- Tepedino, M.; Iancu-Potrubacz, M.; Ciavarella, D.; Masedu, F.; Marchione, L.; Chimenti, C. Expansion of Permanent First Molars with Rapid Maxillary Expansion Appliance Anchored on Primary Second Molars. J. Clin. Exp. Dent. 2018, 10, e241–e247. [Google Scholar] [CrossRef]
- Ciavarella, D.; Tepedino, M.; Chimenti, C.; Troiano, G.; Mazzotta, M.; Foschino Barbaro, M.P.; Lo Muzio, L.; Cassano, M. Correlation between Body Mass Index and Obstructive Sleep Apnea Severity Indexes—A Retrospective Study. Am. J. Otolaryngol. 2018, 39, 388–391. [Google Scholar] [CrossRef]
- Troiano, G.; Dioguardi, M.; Cocco, A.; Zhurakivska, K.; Ciavarella, D.; Muzio, L.L. Increase the Glyde Path Diameter Improves the Centering Ability of F6 Skytaper. Eur. J. Dent. 2018, 12, 089–093. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Ciavarella, D.; Parziale, V.; Mastrovincenzo, M.; Palazzo, A.; Sabatucci, A.; Suriano, M.M.; Bossù, M.; Cazzolla, A.P.; Lo Muzio, L.; Chimenti, C. Condylar Position Indicator and T-Scan System II in Clinical Evaluation of Temporomandibular Intracapsular Disease. J. Cranio-Maxillofac. Surg. 2012, 40, 449–455. [Google Scholar] [CrossRef]
- Cianci, C.; Pappalettera, G.; Renna, G.; Casavola, C.; Laurenziello, M.; Battista, G.; Pappalettere, C.; Ciavarella, D. Mechanical Behavior of PET-G Tooth Aligners Under Cyclic Loading. Front. Mater. 2020, 7, 104. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Malcangi, G.; Costa, S.; Fatone, M.C.; Avantario, P.; Campanelli, M.; Piras, F.; Patano, A.; Ferrara, I.; Di Pede, C.; et al. Tooth Complications after Orthodontic Miniscrews Insertion. Int. J. Environ. Res. Public Health 2023, 20, 1562. [Google Scholar] [CrossRef] [PubMed]
- De Vito, D.; Zullo, M.J.; Benincasa, C.; Aiello, E.; Giacomello, M.S.; Mortellaro, C.; Greco Lucchina, A. Facial Mask and Plexiglass Box: A Critical Overview on the Current Strategies to Protect Patients from COVID-19 Infection. J. Biol. Regul. Homeost. Agents 2021, 35, 139–145. [Google Scholar] [CrossRef] [PubMed]
- De Vito, D.; Di Ciaula, A.; Palmieri, V.O.; Trerotoli, P.; Larocca, A.M.V.; Montagna, M.T.; Portincasa, P. Reduced COVID-19 Mortality Linked with Early Antibodies against SARS-CoV-2, Irrespective of Age. Eur. J. Intern. Med. 2022, 98, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Raucci, G.; Pachêco-Pereira, C.; Elyasi, M.; d’Apuzzo, F.; Flores-Mir, C.; Perillo, L. Predictors of Postretention Stability of Mandibular Dental Arch Dimensions in Patients Treated with a Lip Bumper during Mixed Dentition Followed by Fixed Appliances. Angle Orthod. 2017, 87, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef]
- Freitas, K.M.S.; Massaro, C.; Miranda, F.; de Freitas, M.R.; Janson, G.; Garib, D. Occlusal Changes in Orthodontically Treated Subjects 40 Years after Treatment and Comparison with Untreated Control Subjects. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 671–685. [Google Scholar] [CrossRef]
- Mahmoudzadeh, M.; Mirzaei, H.; Farhadian, M.; Mollabashi, V.; Khosravi, M. Comparison of Anterior Crowding Relapse Tendency in Patients Treated with Incisor Extraction, Premolar Extraction, and Nonextraction Treatment. J. World Fed. Orthod. 2018, 7, 61–65. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Type of Study | Aim of the Study | Materials | Results |
|---|---|---|---|---|
| Partha Jyoti Das et al., 2017 [18] | Cross-sectional study | To assess dental crowding in relation to mesiodistal crown widths and arch lengths | A total of 132 patients were separated into two groups: crowded and non-packed, each of which had 66 subjects (33 males and 33 females), all of whom were between the ages of 15 and 35 and had been sent to the radiology department for a brain computed tomography scan. | The results of this study showed that in South Indian men, both the factors—mesiodistal crown width and arch dimensions—contributed to dental crowding, and the crowded dentition had larger mesiodistal teeth and smaller arch dimensions. However, in women, neither of these factors was found to be the cause of crowding. |
| Vincenzo Quinzi, Silvia Caruso et al., 2020 [27] | Prospective pilot study | This prospective study’s objective was to evaluate dental crowding and arch measurements before and after lip bumper versus Schwarz’s appliance therapy. | The present study investigated the pre- and post-treatment orthodontic records of 20 patients (10 males and 10 females). The following criteria were used for inclusion: first/second molar class malocclusion; mild to moderate (4–6 mm) crowding of the mandibular arch; mixed dentition; and age 9 years at the start of therapy. | Both a Schwarz appliance and a lip bumper are effective in lessening crowding in mixed dentition. The expansion of the dental arch is the reason for this improvement; however the two appliances’ allocation of the resulting space differed slightly. |
| Fathima Bareera Rezvi, Ravindra Kumar Jain et al., 2019 [28] | Retrospective cross-sectional study | To assess the frequency of mandibular anterior tooth crowding in patients with mixed dentition who present to a university hospital in Chennai. | A total of 3652 participants who attended the Saveetha Dental College’s Orthodontics department between June 2019 and March 2020 were included in the research. Data were retrieved from digital records. | Crowding of the mandibular anterior teeth was substantially correlated with age, although there was no correlation with gender. |
| Priyanka Satra, Gauri Vichare et al., 2022 [29] | Retrospective study | To evaluate, quantify and compare the maxillary and mandibular effective base lengths, arch lengths and the degree of dental crowding in individuals with various vertical development patterns. | A sample of 100 study models (aged 16 to 25) and pre-treatment lateral cephalograms was randomly chosen. Based on the measurement of the gonial angle, the sample was separated into two groups: clockwise (50) and anticlockwise (50) rotation. | Dental crowding is caused by the mandible rotating clockwise as well as skeletal and dental variables including shorter effective base lengths and shorter arch lengths, respectively. |
| J. Antoszewska-Smith, M. Bohater et al., 2017 [30] | Research article | This study attempted to determine the validity of Little’s Irregularity Index (LII) as a measure of the stability of treatment results in individuals with crowded mandibular incisors. | Digital dental casts of 302 individuals were used to create the material. There were 201 women and 101 men, between the ages of 21 and 39, with late crowding of the mandibular front teeth before treatment. All patients were divided into three groups after Little’s Irregularity Index measurement. | Thirty years after its introduction, LII has shown to be a dependable measure that enables the choice in the best treatment options. |
| Di Ventura et al.,2019 [31] | Retrospective study | Evaluated the effect of RME on mandibular arch in mixed dentition. | Patients (n = 54) were divided into two groups: (n = 21) patients treated with RME; (n = 17) patients that did not receive any treatment. | The results of this study show a significant increase in interdental width in the lower arch after 9 months of RME therapy. |
| Olivia Griswold et al., 2022 [32] | Retrospective study | Evaluated the changes in sagittal mandibular incisors’ position in response to lip bumper therapy using CBCT (cone beam computed tomography). | Patients (n = 34) were divided in two groups: rapid maxillary expansion group with no lower treatment (experimental group) and an RME (rapid maxillary expansion) + LB (lip bumper) group (control group). | There was no statistically significant difference in the amount of mandibular incisor protrusion between the two groups. |
| Nakhjavani et al., 2017 [33] | Clinical trial | The purpose of this study was to determine the effectiveness of mesial stripping of mandibular deciduous canines for the correction of rotated and lingually erupted lateral incisors. | A total of 42 patients with <3 mm mandibular crowding were included and followed up for 5 months. | Mesial stripping of mandibular primary canines resulted in full crowding correction; in just a few cases, the amount of crowding did not reach zero. |
| Purva Verma et al., 2022 [34] | Retrospective study | To compare the stability of mandibular anterior crowding after correction with two treatment protocols. | Patients (n = 32) were divided into two groups: (n = 15) patients treated with passive self-ligation non-extraction protocol; (n = 17) patients treated with conventional ligation lower incisor extraction protocol. Changes in intermolar width, intercanine width, Little’s Irregularity Index and mandibular incisor inclination at pretreatment, post-debonding and 1 year post-debonding were evaluated. | Change in intermolar width was similar in both groups. The relapse in intercanine width and inclination of lower incisor was significantly greater in patients treated in non-extraction protocol. |
| Mahmoudzadeh et al., 2022 [27] | Cross-sectional study | To compare the relapse tendency of crowding in patients treated with different protocols. | Patients (n = 120) were treated with fixed appliances and followed up after 3.5 years. Patients were divided into three groups: patients treated without extraction, patients treated with single extraction and patients treated with premolar extraction. | Treatment modality does not influence the post-treatment relapse. |
| Persson et al., 2022 [35] | Longitudinal, case-control study | To assess the effects of early extraction of four premolars on the crowding of lower incisors after 50 years of follow-up. | Patients (n = 45) were divided into: a group of patients who underwent extraction of all first premolars (n = 24) and a group of untreated patients with a normal occlusion (n = 21). | Lower incisor alignment remains unchanged into late adulthood in patients who have all first premolars removed compared with untreated subjects. |
| Berbert et al., 2020 [36] | Retrospective study | To evaluate if the 3 × 3 bonded mandibular retainer influences the relapse of crowding at 1 year of follow up. | Patients (n = 16) were treated with mandibular incisor extraction and were divided into: patients who did not present the 3x3 bonded retainer (n = 9) and patients with 3 × 3 bonded retainer (n = 7). | Patients with 3x3 bonded retainer showed good stability in mandibular incisor alignment in comparison to patients without retainer. |
| Methods of Treatment of Mandibular Crowding | Goal |
|---|---|
| Schwarz’s appliance Lip bumper appliance | To increment the perimeter of mandibular arch |
| Slicing | It is a simple procedure that recovers the Leeway space in advance, that is, before the exchange of the milk molars and without resorting to any orthodontic appliance |
| Serial extraction | To create space in the mixed dentition for the eruption of permanent teeth into more favorable positions over basal bone to prevent or reduce the complexity of future orthodontic treatment in the permanent dentition |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patano, A.; Malcangi, G.; Inchingolo, A.D.; Garofoli, G.; De Leonardis, N.; Azzollini, D.; Latini, G.; Mancini, A.; Carpentiere, V.; Laudadio, C.; et al. Mandibular Crowding: Diagnosis and Management—A Scoping Review. J. Pers. Med. 2023, 13, 774. https://doi.org/10.3390/jpm13050774
Patano A, Malcangi G, Inchingolo AD, Garofoli G, De Leonardis N, Azzollini D, Latini G, Mancini A, Carpentiere V, Laudadio C, et al. Mandibular Crowding: Diagnosis and Management—A Scoping Review. Journal of Personalized Medicine. 2023; 13(5):774. https://doi.org/10.3390/jpm13050774
Chicago/Turabian StylePatano, Assunta, Giuseppina Malcangi, Alessio Danilo Inchingolo, Grazia Garofoli, Nicole De Leonardis, Daniela Azzollini, Giulia Latini, Antonio Mancini, Vincenzo Carpentiere, Claudia Laudadio, and et al. 2023. "Mandibular Crowding: Diagnosis and Management—A Scoping Review" Journal of Personalized Medicine 13, no. 5: 774. https://doi.org/10.3390/jpm13050774
APA StylePatano, A., Malcangi, G., Inchingolo, A. D., Garofoli, G., De Leonardis, N., Azzollini, D., Latini, G., Mancini, A., Carpentiere, V., Laudadio, C., Inchingolo, F., D’Agostino, S., Di Venere, D., Tartaglia, G. M., Dolci, M., Dipalma, G., & Inchingolo, A. M. (2023). Mandibular Crowding: Diagnosis and Management—A Scoping Review. Journal of Personalized Medicine, 13(5), 774. https://doi.org/10.3390/jpm13050774