
Integrating Neuromonitoring in Pediatric Emergency Medicine: Exploring Two Options for Point-of-Care Electroencephalogram (pocEEG) via Patient Monitors—A Technical Note

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
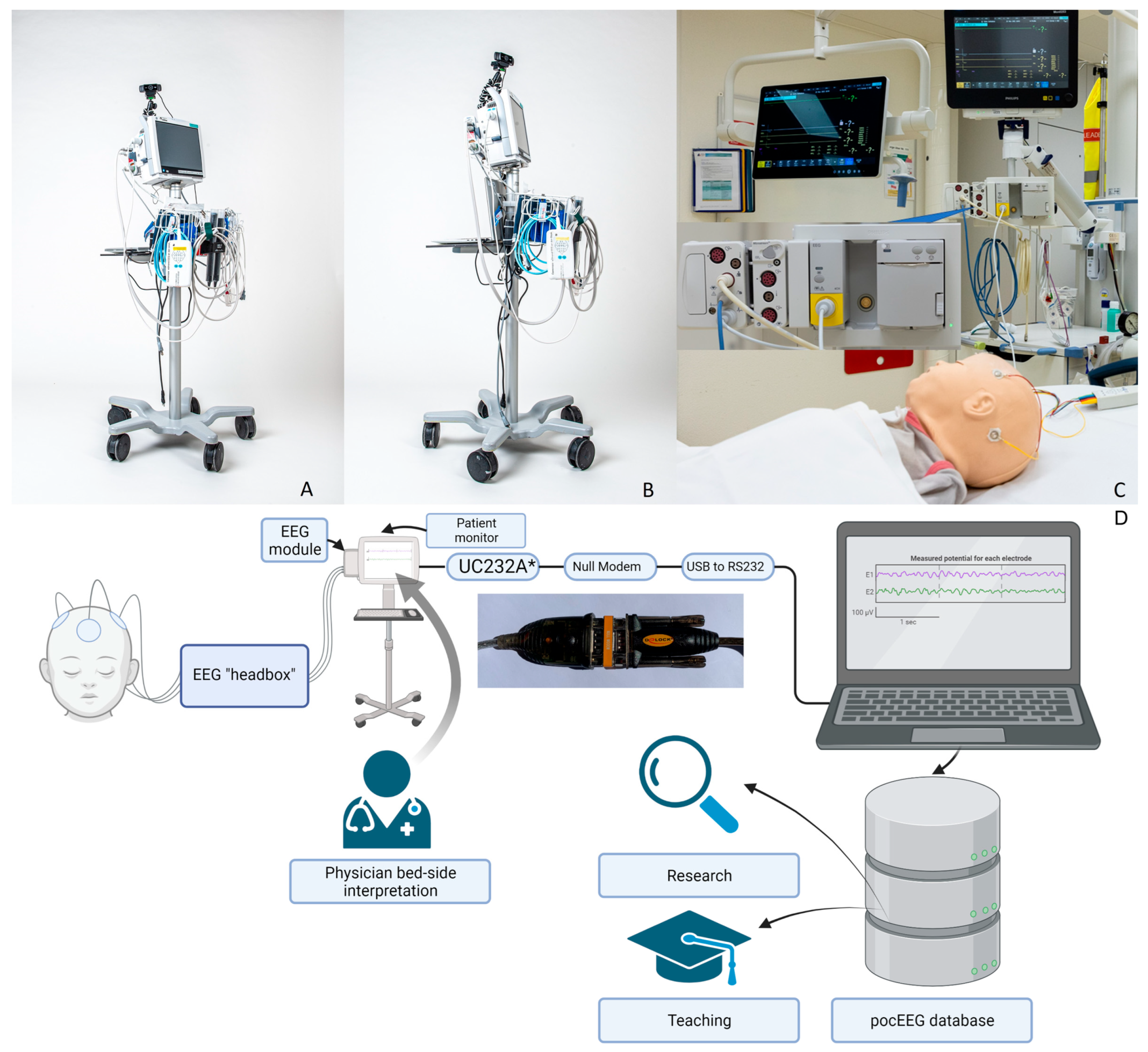
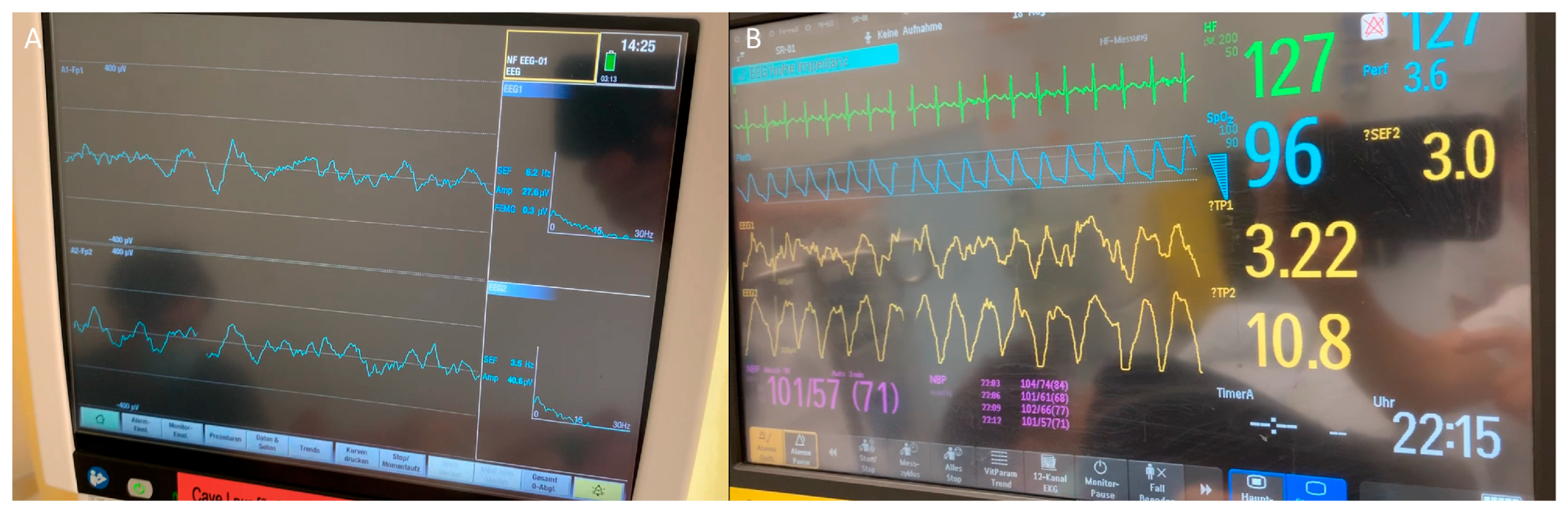
2.1. Solution 1: GE Carescape
2.1.1. EEG Module
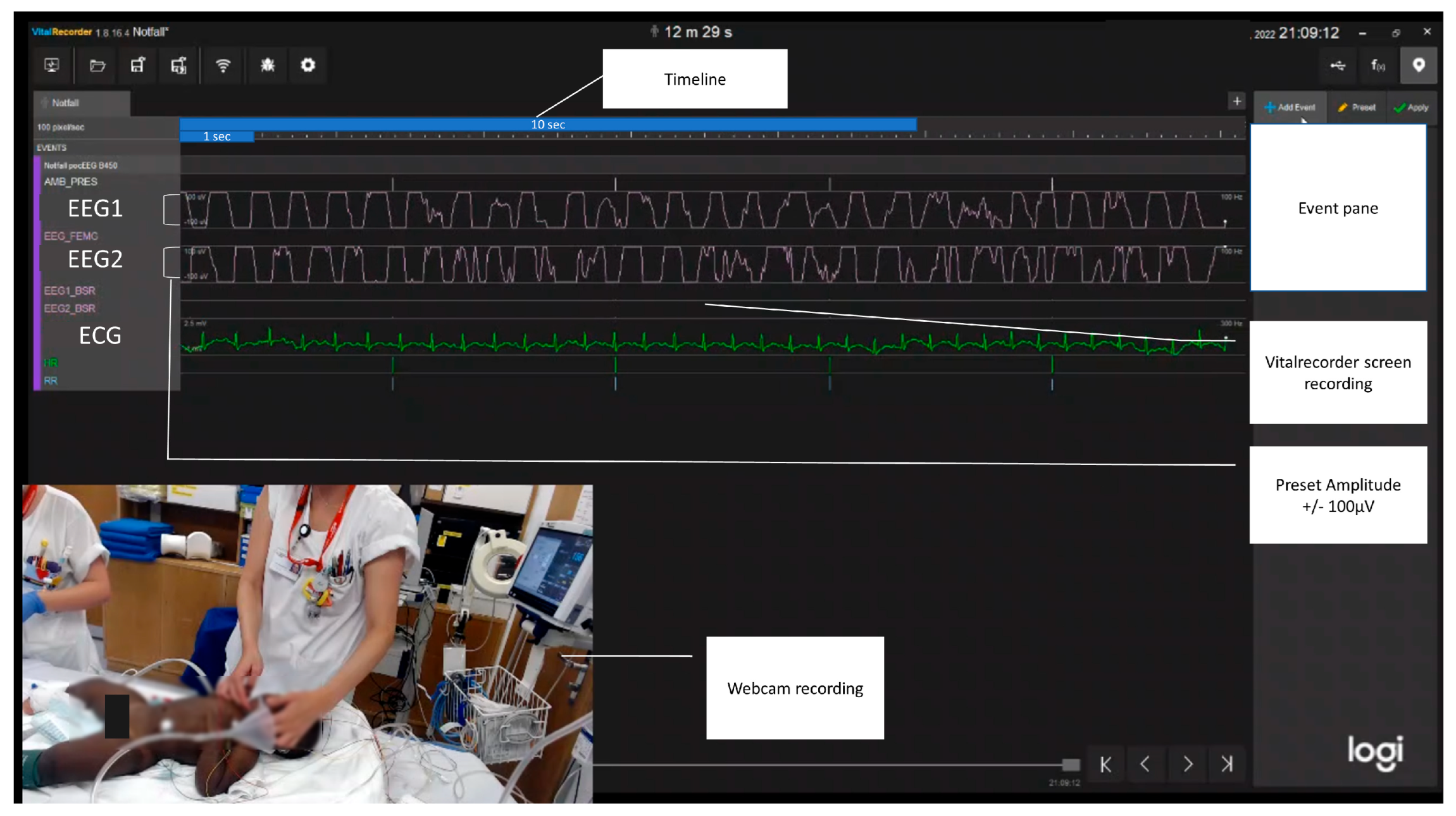
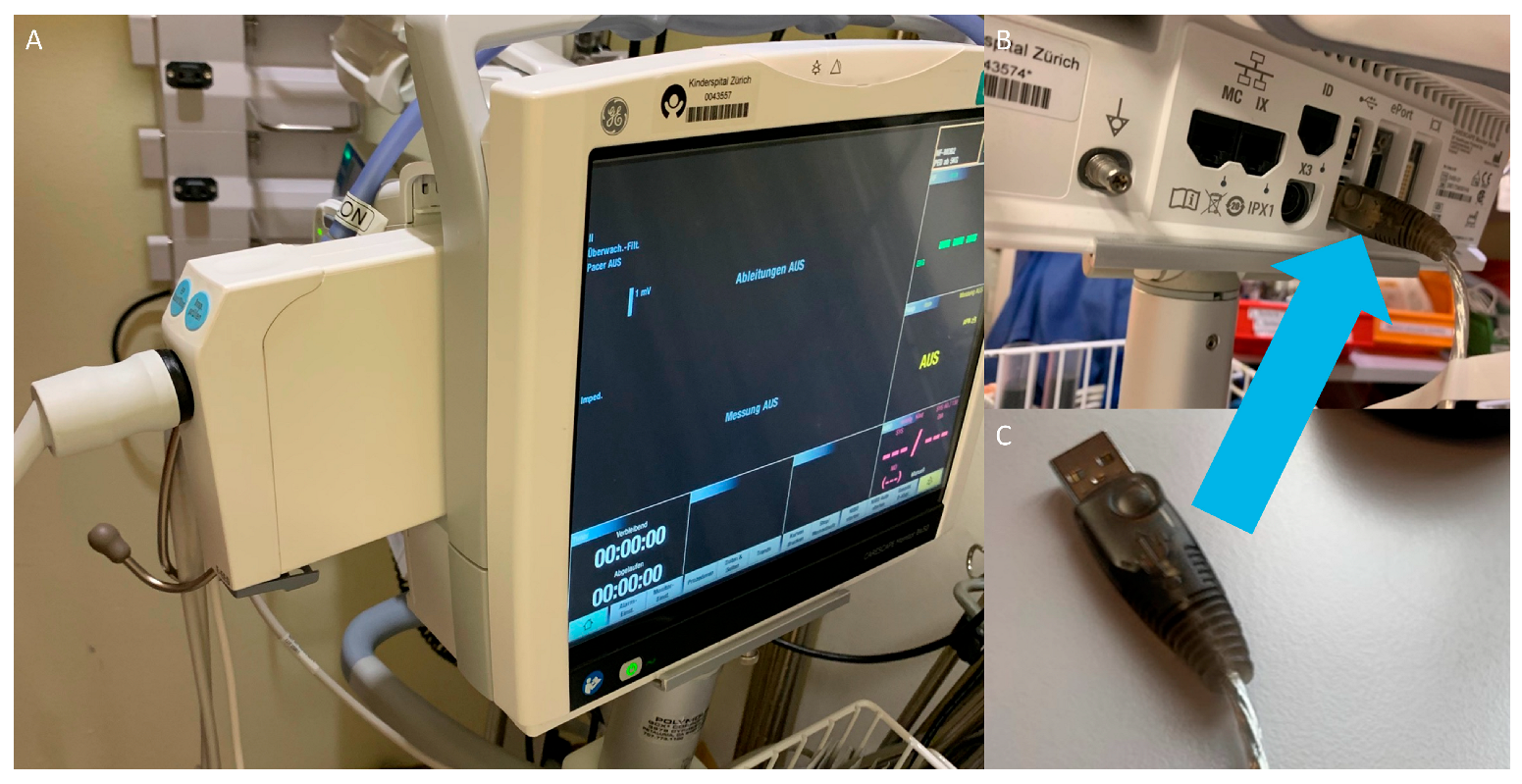
2.1.2. Data Capture
2.1.3. Video pocEEG
2.2. Solution 2: Philips IntelliVue
2.2.1. EEG Module
2.2.2. Data Capture
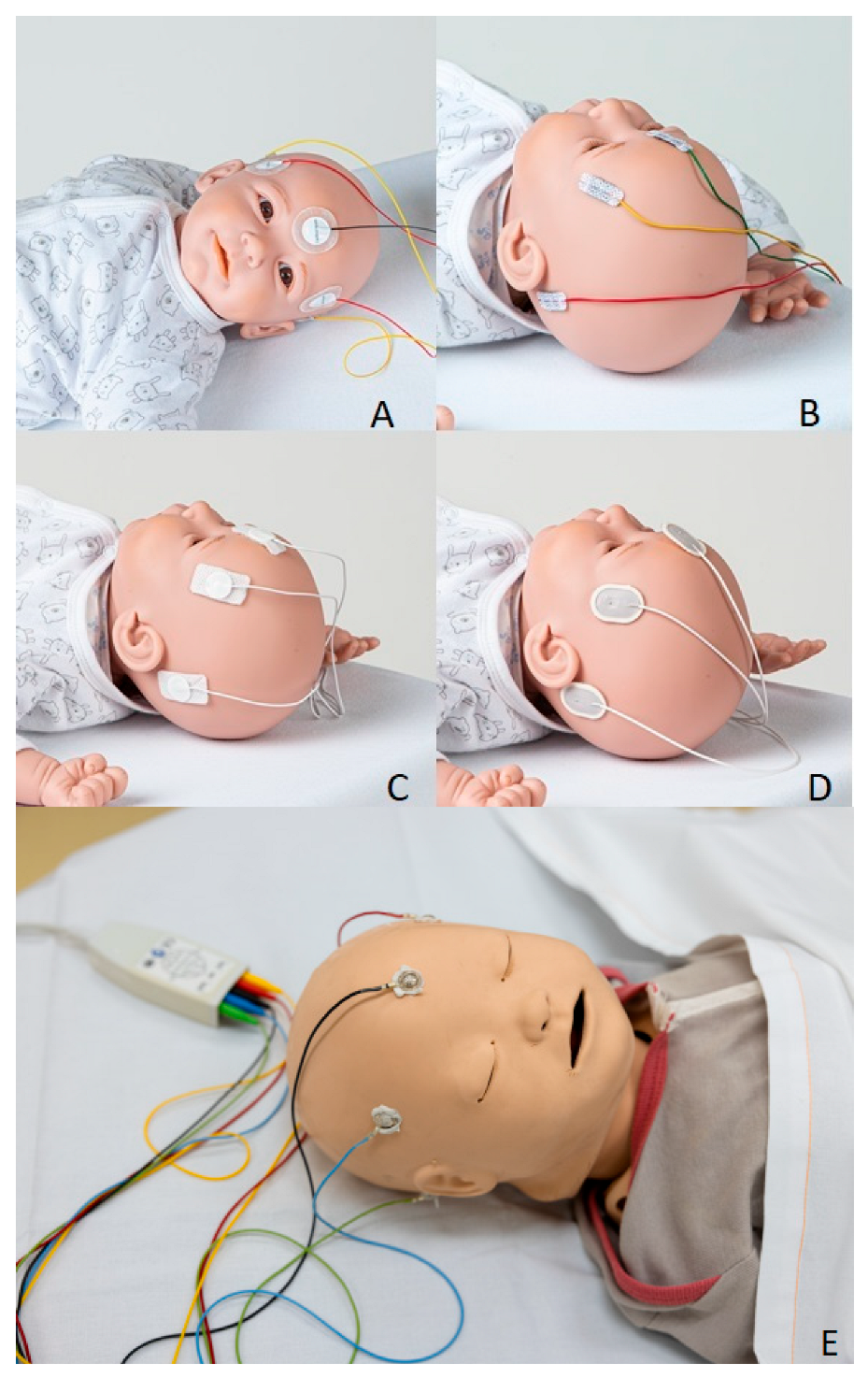
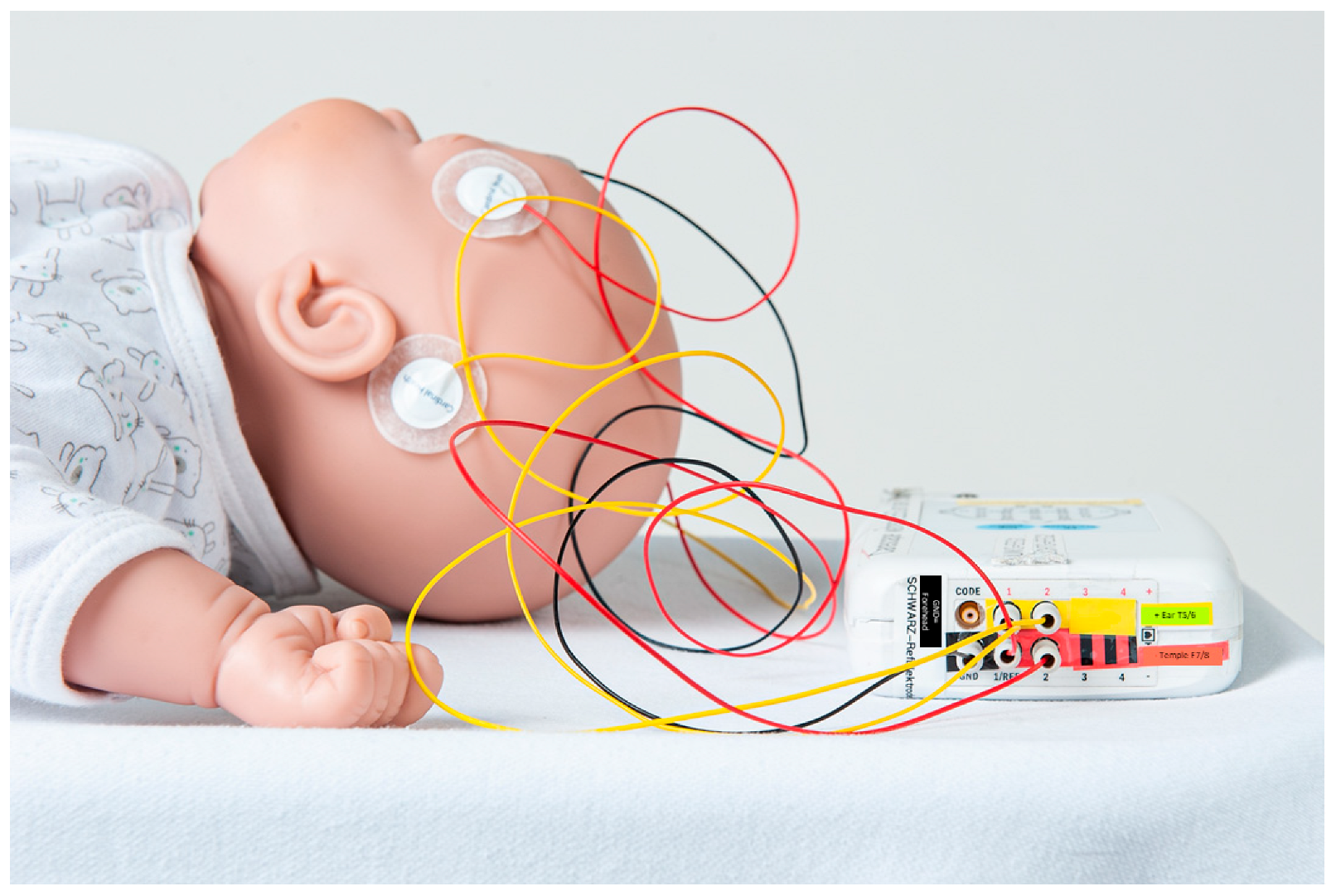
2.3. Electrodes
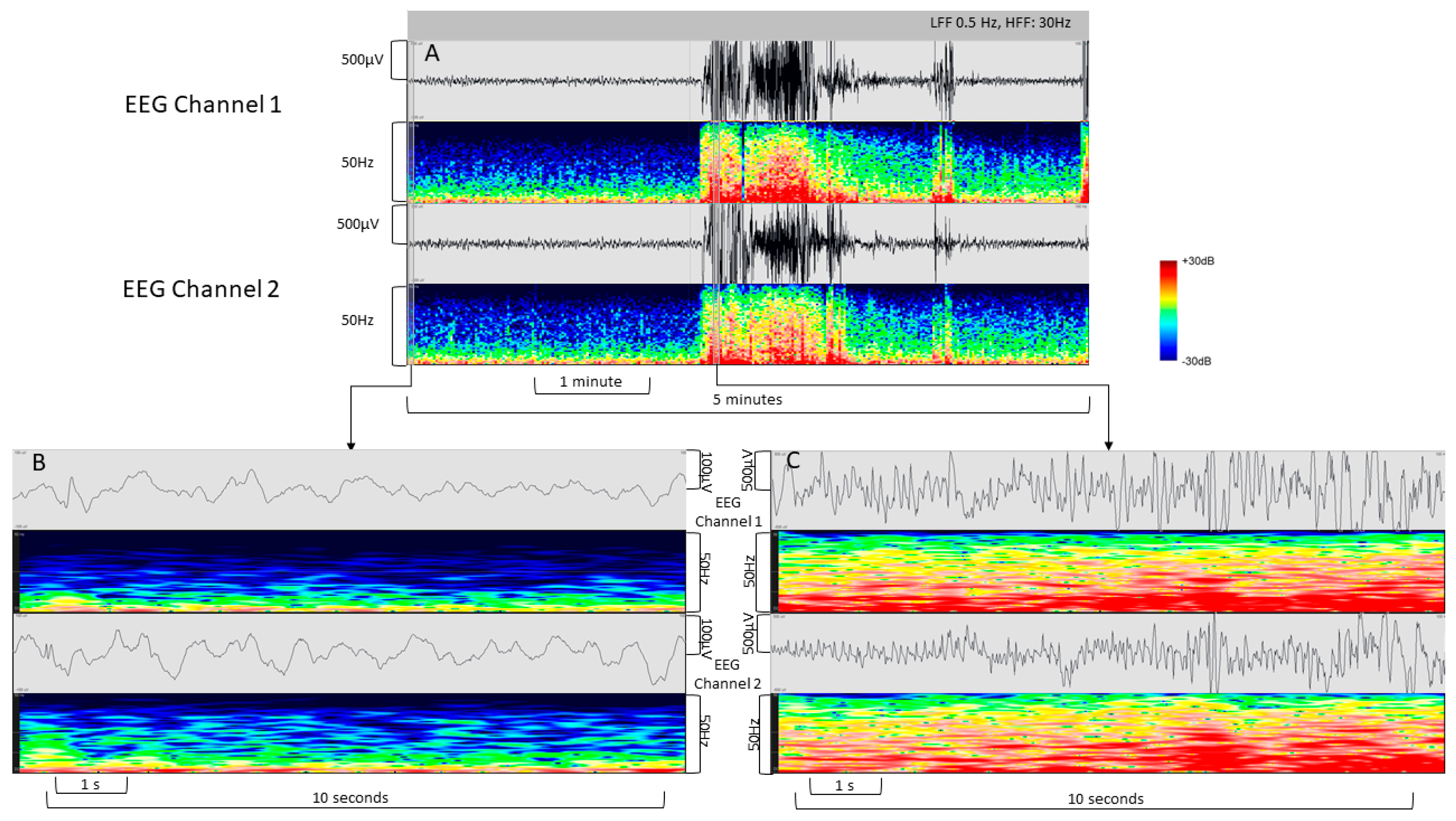
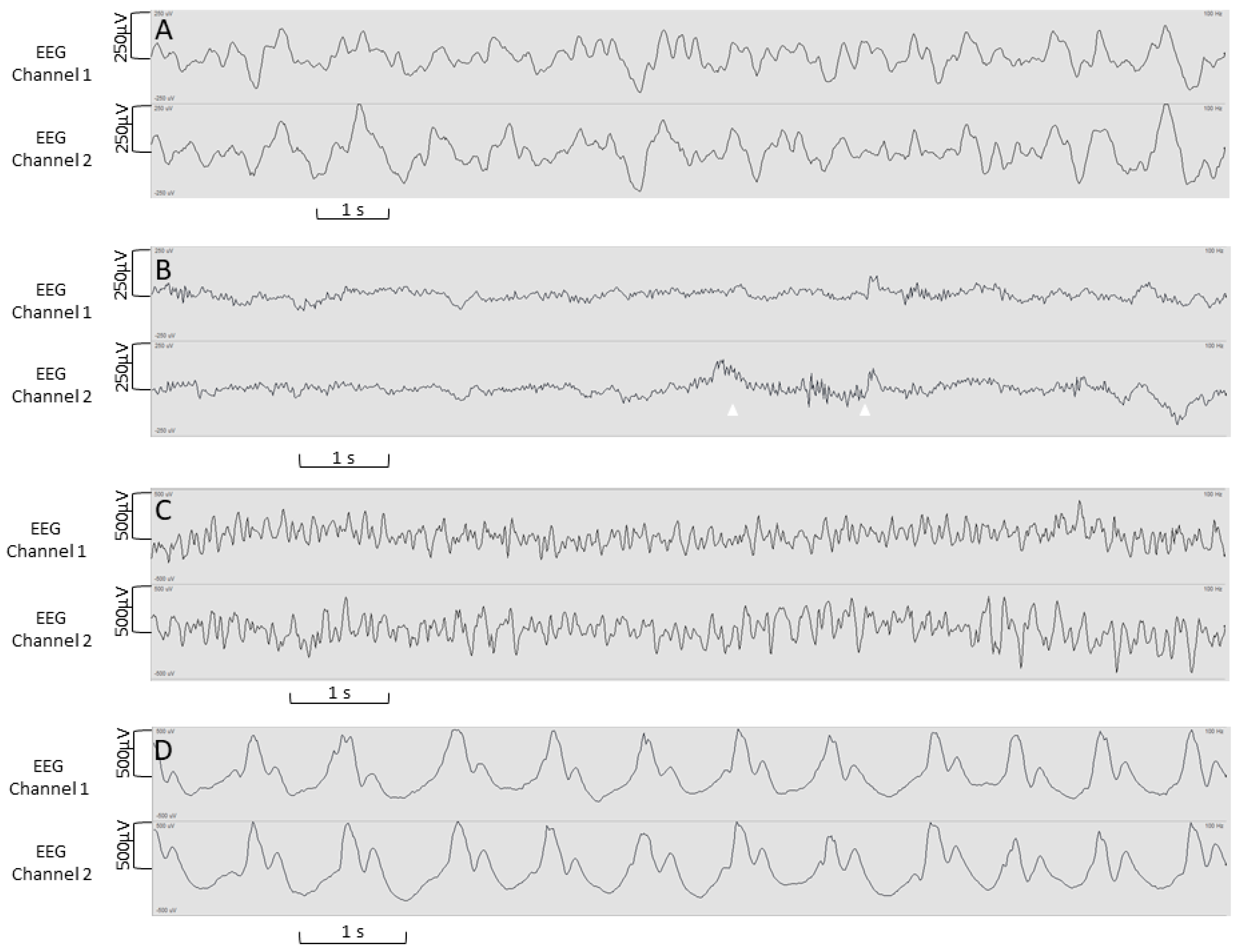
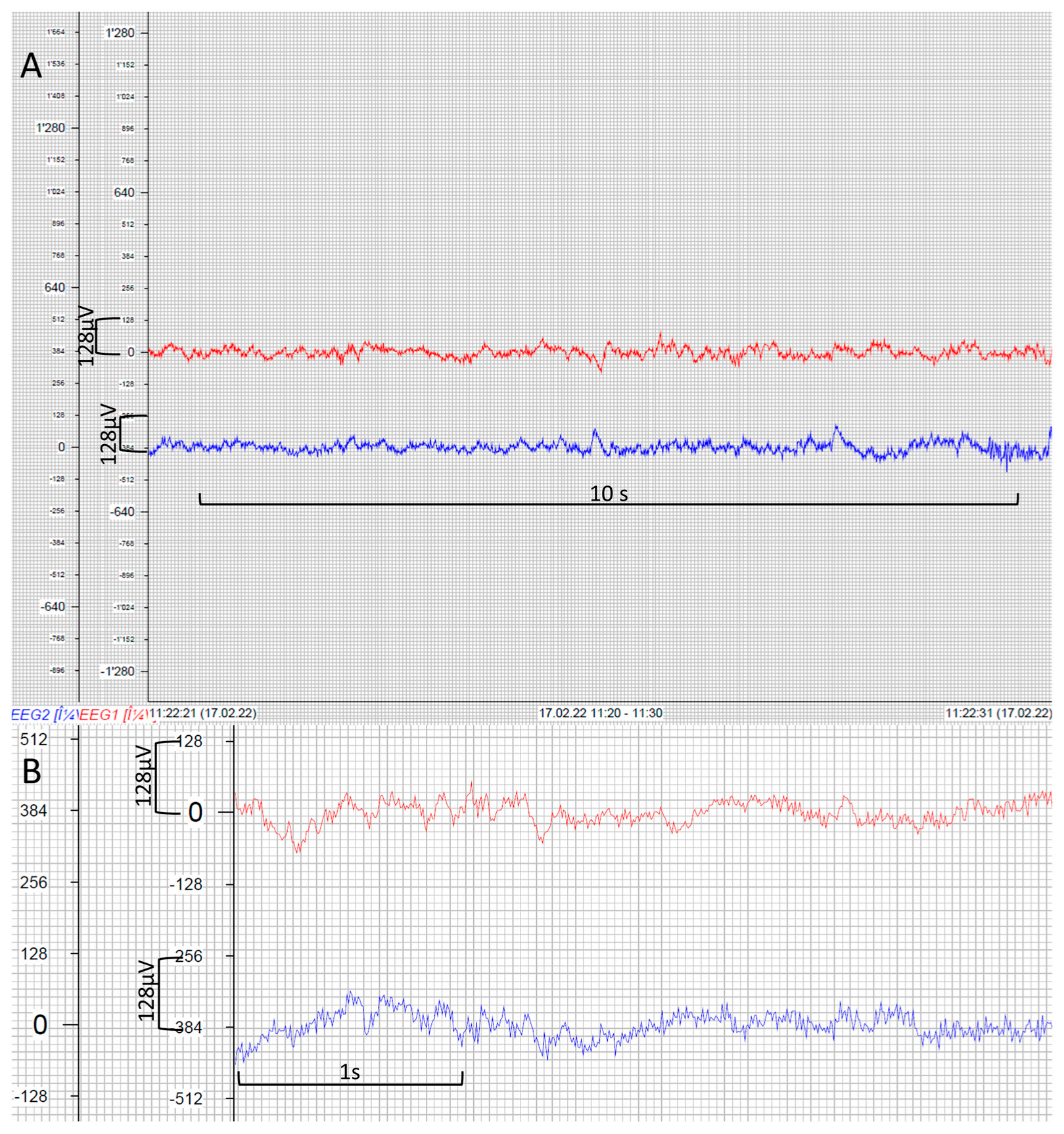
3. Results
4. Discussion
4.1. Limitations
4.2. Remote EEG Interpretation
4.3. Outlook
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GE Carescape EEG Module | Philips IntelliVue EEG Module | |
|---|---|---|
| Sampling rate | 100 Hz per channel | 125 Hz per channel |
| Range | ±400 µV | ±1000 µV |
| Input filter | 0.5 to 30 Hz | 0.5 to 30 Hz |
| Input impedance | >8 MΩ at 10 Hz | >15 MΩ at 10 Hz |
| Impedance limit | 5 (10) kΩ | 5 kΩ (up to 30 kΩ) |
References
- Pallin, D.J.; Goldstein, J.N.; Moussally, J.S.; Pelletier, A.J.; Green, A.R.; Camargo, C.A., Jr. Seizure visits in US emergency departments: Epidemiology and potential disparities in care. Int. J. Emerg. Med. 2008, 1, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Lutz, N.; Vandermensbrugghe, N.G.; Dolci, M.; Amiet, V.; Racine, L.; Carron, P.N. Pediatric emergencies admitted in the resuscitation room of a Swiss university hospital. Pediatr. Emerg. Care 2014, 30, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Simma, L.; Stocker, M.; Lehner, M.; Wehrli, L.; Righini-Grunder, F. Critically Ill Children in a Swiss Pediatric Emergency Department with an Interdisciplinary Approach: A Prospective Cohort Study. Front. Pediatr. 2021, 9, 721646. [Google Scholar] [CrossRef] [PubMed]
- Jafarpour, S.; Loddenkemper, T. Outcomes in pediatric patients with nonconvulsive status epilepticus. Epilepsy Behav. EB 2015, 49, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Greiner, H.M.; Holland, K.; Leach, J.L.; Horn, P.S.; Hershey, A.D.; Rose, D.F. Nonconvulsive Status Epilepticus: The Encephalopathic Pediatric Patient. Pediatrics 2012, 129, e748–e755. [Google Scholar] [CrossRef] [PubMed]
- Tay, S.K.; Hirsch, L.J.; Leary, L.; Jette, N.; Wittman, J.; Akman, C.I. Nonconvulsive status epilepticus in children: Clinical and EEG characteristics. Epilepsia 2006, 47, 1504–1509. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.A. Continuous electroencephalogram detection of non-convulsive seizures in the pediatric intensive care unit: Review of the utility and impact on management and outcomes. Transl. Pediatr. 2015, 4, 283–289. [Google Scholar] [CrossRef]
- Chen, J.; Xie, L.; Hu, Y.; Lan, X.; Jiang, L. Nonconvulsive status epilepticus after cessation of convulsive status epilepticus in pediatric intensive care unit patients. Epilepsy Behav. EB 2018, 82, 68–73. [Google Scholar] [CrossRef]
- Chin, R.F.; Neville, B.G.; Peckham, C.; Bedford, H.; Wade, A.; Scott, R.C. Incidence, cause, and short-term outcome of convulsive status epilepticus in childhood: Prospective population-based study. Lancet 2006, 368, 222–229. [Google Scholar] [CrossRef]
- Kothare, S.V.; Khurana, D.S.; Valencia, I.; Melvin, J.J.; Legido, A. Use and Value of Ordering Emergency Electroencephalograms and Videoelectroencephalographic Monitoring after Business Hours in a Children’s Hospital: 1-Year Experience. J. Child. Neurol. 2005, 20, 416–419. [Google Scholar] [CrossRef]
- Fernandez, I.S.; Loddenkemper, T.; Datta, A.; Kothare, S.; Riviello, J.J., Jr.; Rotenberg, A. Electroencephalography in the pediatric emergency department: When is it most useful? J. Child. Neurol. 2014, 29, 475–482. [Google Scholar] [CrossRef]
- Herman, S.T.; Abend, N.S.; Bleck, T.P.; Chapman, K.E.; Drislane, F.W.; Emerson, R.G.; Gerard, E.E.; Hahn, C.D.; Husain, A.M.; Kaplan, P.W.; et al. Consensus statement on continuous EEG in critically ill adults and children, part I: Indications. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2015, 32, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Herman, S.T.; Abend, N.S.; Bleck, T.P.; Chapman, K.E.; Drislane, F.W.; Emerson, R.G.; Gerard, E.E.; Hahn, C.D.; Husain, A.M.; Kaplan, P.W.; et al. Consensus statement on continuous EEG in critically ill adults and children, part II: Personnel, technical specifications, and clinical practice. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2015, 32, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Davey, Z.; Gupta, P.B.; Li, D.R.; Nayak, R.U.; Govindarajan, P. Rapid Response EEG: Current State and Future Directions. Curr. Neurol. Neurosci. Rep. 2022, 22, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, H.; Nagase, H.; Nishiyama, M.; Tokumoto, S.; Ishida, Y.; Tomioka, K.; Tanaka, T.; Fujita, K.; Toyoshima, D.; Nishimura, N.; et al. Nonconvulsive Seizure Detection by Reduced-Lead Electroencephalography in Children with Altered Mental Status in the Emergency Department. J. Pediatr. 2019, 207, 213–219.e213. [Google Scholar] [CrossRef] [PubMed]
- Nozawa, M.; Terashima, H.; Tsuji, S.; Kubota, M. A Simplified Electroencephalogram Monitoring System in the Emergency Room. Pediatr. Emerg. Care 2019, 35, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Simma, L.; Bauder, F.; Schmitt-Mechelke, T. Feasibility and usefulness of rapid 2-channel-EEG-monitoring (point-of-care EEG) for acute CNS disorders in the paediatric emergency department: An observational study. Emerg. Med. J. 2021, 38, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-C.; Jung, C.-W. Vital Recorder—A free research tool for automatic recording of high-resolution time-synchronised physiological data from multiple anaesthesia devices. Sci. Rep. 2018, 8, 1527. [Google Scholar] [CrossRef]
- Tanner, A.E.; Särkelä, M.O.; Virtanen, J.; Viertiö-Oja, H.E.; Sharpe, M.D.; Norton, L.; Davies-Schinkel, C.; Young, G.B. Application of subhairline EEG montage in intensive care unit: Comparison with full montage. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2014, 31, 181–186. [Google Scholar] [CrossRef]
- Piantino, J.A.; Lin, A.; Luther, M.; Centeno, L.D.; Williams, C.N.; Newgard, C.D. Simultaneous Heart Rate Variability and Electroencephalographic Monitoring in Children in the Emergency Department. J. Child. Adolesc. Trauma 2021, 14, 165–175. [Google Scholar] [CrossRef]
- Dash, D.; Dash, C.; Primrose, S.; Hernandez-Ronquillo, L.; Moien-Afshari, F.; Ladino, L.D.; Appendino, J.P.; Mazepa, L.; Elliott, C.; Mirsattari, S.M.; et al. Update on Minimal Standards for Electroencephalography in Canada: A Review by the Canadian Society of Clinical Neurophysiologists. Can. J. Neurol. Sci. 2017, 44, 631–642. [Google Scholar] [CrossRef]
- Peltola, M.E.; Leitinger, M.; Halford, J.J.; Vinayan, K.P.; Kobayashi, K.; Pressler, R.M.; Mindruta, I.; Mayor, L.C.; Lauronen, L.; Beniczky, S. Routine and sleep EEG: Minimum recording standards of the International Federation of Clinical Neurophysiology and the International League Against Epilepsy. Clin. Neurophysiol. 2023, 147, 108–120. [Google Scholar] [CrossRef]
- Taran, S.; Ahmed, W.; Pinto, R.; Bui, E.; Prisco, L.; Hahn, C.D.; Englesakis, M.; McCredie, V.A. Educational initiatives for electroencephalography in the critical care setting: A systematic review and meta-analysis. Can. J. Anaesth. 2021, 68, 1214–1230. [Google Scholar] [CrossRef]






| Product | Shape/Cables | Size | Price Per Pack | Electrode Impedance (kΩ) |
|---|---|---|---|---|
| Self-adhesive electrodes—“small footprint” | ||||
| Micro Neolead® ECG Electrodes (Neotech Products, Valencia, CA, USA) | Rectangular, colored cable | 9 mm × 14 mm w/adhesive 9 × 25 mm | 8.55 USD (Pack of 3) (17.10 USD per patient) | 12–16 kΩ |
| Self-adhesive electrodes—“medium footprint” | ||||
| Neonatal Kendall® ECG electrodes (CardinalHealth, Dublin, Ireland) | Round, colored cable | Diameter 17 mm, w/adhesive border 30 mm | 1.25 USD (Pack of 3) (2.50 USD per patient) | 4–6 kΩ |
| OBM Neonatal Hydrogel Sensors® (Natus Medical Inc., Middleton, WI, USA) | Rectangular, white cable | Diameter 10 mm w/adhesive 30 mm × 18 mm | 4.10 USD (Pack of 5) (4.10 USD per patient) | N/A |
| Ambu® White Sensor 40556 (Ambu A/S, Ballerup, Denmark) | Square, colored cable | Diameter 17 mm, w/adhesive border 22 mm × 22 mm | 2.75 USD (Pack of 3) (5.5 USD per patient) | 7–8.5 kΩ |
| Self-adhesive electrodes—“large footprint” | ||||
| Ambu Neuroline 720® (Ambu A/S, Ballerup, Denmark) | Rectangular (rounded), white cable | 30 mm × 21 mm | 22 USD (Pack of 12) (22 USD per patient) | 5–6 kΩ |
| Reusable electrodes | ||||
| Philips M1931A Reusable EEG Adult Cup Electrode (Philips Medical Systems, Boeblingen, Germany) | Round, colored cable | Diameter 10 mm, silver | 110 USD (Pack of 6) | <5 kΩ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simma, L.; Romano, F.; Schmidt, S.; Ramantani, G.; Bölsterli, B.K. Integrating Neuromonitoring in Pediatric Emergency Medicine: Exploring Two Options for Point-of-Care Electroencephalogram (pocEEG) via Patient Monitors—A Technical Note. J. Pers. Med. 2023, 13, 1411. https://doi.org/10.3390/jpm13091411
Simma L, Romano F, Schmidt S, Ramantani G, Bölsterli BK. Integrating Neuromonitoring in Pediatric Emergency Medicine: Exploring Two Options for Point-of-Care Electroencephalogram (pocEEG) via Patient Monitors—A Technical Note. Journal of Personalized Medicine. 2023; 13(9):1411. https://doi.org/10.3390/jpm13091411
Chicago/Turabian StyleSimma, Leopold, Fabrizio Romano, Steffen Schmidt, Georgia Ramantani, and Bigna K. Bölsterli. 2023. "Integrating Neuromonitoring in Pediatric Emergency Medicine: Exploring Two Options for Point-of-Care Electroencephalogram (pocEEG) via Patient Monitors—A Technical Note" Journal of Personalized Medicine 13, no. 9: 1411. https://doi.org/10.3390/jpm13091411
APA StyleSimma, L., Romano, F., Schmidt, S., Ramantani, G., & Bölsterli, B. K. (2023). Integrating Neuromonitoring in Pediatric Emergency Medicine: Exploring Two Options for Point-of-Care Electroencephalogram (pocEEG) via Patient Monitors—A Technical Note. Journal of Personalized Medicine, 13(9), 1411. https://doi.org/10.3390/jpm13091411