
Public Trust in Health Information Sharing: Implications for Biobanking and Electronic Health Record Systems

Abstract
:1. Introduction
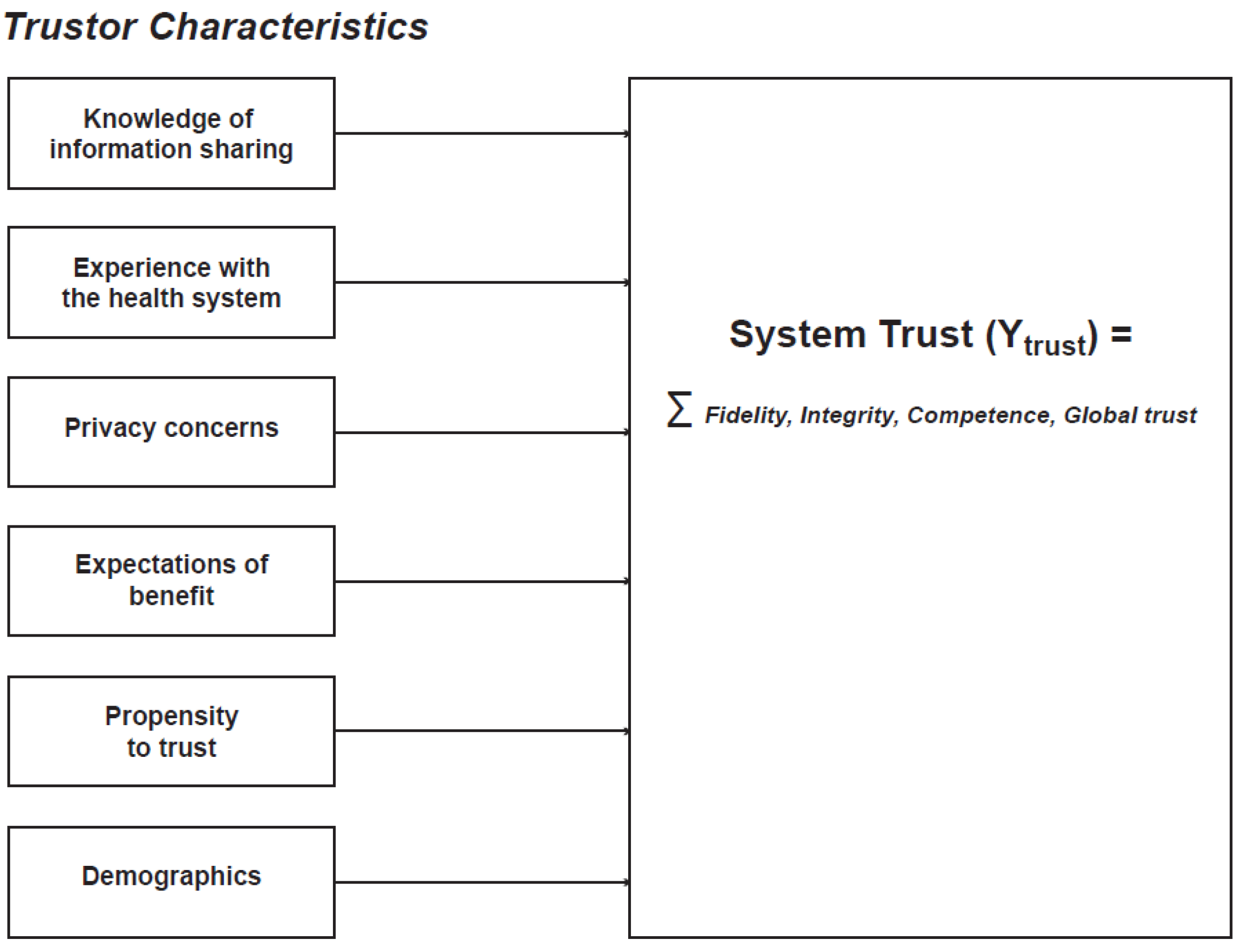
1.1. Conceptual Model
1.2. System Trust and Its Dimensions

1.3. Knowledge of Health Information Sharing
1.4. Experience with the Health System
1.5. Trustor Expectations
1.6. Trustor Privacy Concerns
2. Experimental Section
2.1. Questionnaire Development
2.2. Sample
2.3. Statistical Analysis

{kind=link}
| Trust Dimension | All Variables | Reduced Set of Variables | ||
|---|---|---|---|---|
| No. of Items | Chronbach’s α | No. of Items | Chronbach’s α | |
| Fidelity | 8 | 0.792 | 6 | 0.665 |
| Competency | 9 | 0.816 | 6 | 0.699 |
| Integrity | 5 | 0.818 | 4 | 0.753 |
| Global trust | 4 | 0.915 | 4 | 0.915 |
| Privacy | 6 | 0.8278 | 5 | 0.7658 |
| Self-esteem | 6 | 0.9009 | 4 | 0.8452 |
| Altruism | 4 | 0.6915 | 4 (no change) | 0.6915 (no change) |
| Self-efficacy | 6 | 0.8966 | 4 | 0.8233 |
| Demographic Factor | Sample (%) | US Population a (%) | β' (Univariate) |
|---|---|---|---|
| Sex | |||
| Male | 51.5% | 49.0% | Ref |
| Female | 48.5% | 51.0% | −0.16 |
| Age | |||
| 18–25 | 21.3% | 20.0% | Ref |
| 26–34 | 40.0% | 20.0% | −0.28 |
| 35–54 | 27.9% | 30.0% | −0.27 |
| 55–64 | 8.05% | 10.0% | −0.20 |
| 65+ | 2.68% | 10.0% | 0.30 |
| Race/ Ethnicity | |||
| White Non-Hispanic | 76.1% | 63.2% | Ref |
| Black Non-Hispanic | 7.16% | 12.9% | 0.37 |
| Asian Non-Hispanic | 8.05% | 5.2% | −0.06 |
| Hispanic | 4.70% | 17.0% | −0.12 |
| Other | 3.13% | 27.2% | 0.17 |
| Education | |||
| High School diploma or less | 12.5% | 43.2% | Ref |
| Some college or 2-year college | 42.1% | 28.6% | −0.48 |
| 4-year college | 36.9% | 18.4% | −0.16 |
| Masters or above | 8.50% | 9.8% | −0.21 |
| Home ownership | |||
| Owns home | 37.6% | Ref | |
| Does not own home | 62.4% | −0.28 | |
| Self-rated health | −0.29** | ||
| Excellent | 17.6% | ||
| Very good | 40.7% | ||
| Good | 28.6% | ||
| Fair | 11.4% | ||
| Poor | 1.57% |
3. Results
3.1. Demographics
| Table 3a. Knowledge Questions | Correct Response | Mean (% Answered Correctly) | β' | R2 |
| State and local health departments collect information from physicians and clinics to monitor the health of communities | True | 91.5% | ||
| Permission is NOT required for research using your health information if your identity (name, address) has been removed | True | 76.3% | ||
| Your health information may be used in multiple studies without your permission or knowledge | True | 72.0% | ||
| Institutions may charge money to researchers to access health information | True | 70.2% | ||
| You own your health information | False | 65.5% | ||
| Your physician determines all uses of information in your medical record | False | 64.2% | ||
| A person’s permission is required for all health research | False | 63.1% | ||
| Researchers always need to obtain permission from you to access your medical record | False | 48.5% | ||
| Health insurance companies are prohibited from using your health information to deny your coverage | True | 35.3% | ||
| All forms of discrimination based on genetic information are prohibited by law | False | 30.4% | ||
| Average total score (out of 10) | 6.17 | −0.30 *** | 0.11 | |
| Table 3b. Experience | Frequency | % | β' | R2 |
| Experience with primary care physician | 0.060 | |||
| Does not have a primary care physician | 141 | 31.5 | Ref | |
| Has primary care physician but has not seen at least once in the past year | 52 | 11.6 | 0.18 | |
| Has primary care physician and has seen at least once in past year | 254 | 56.8 | 1.0*** | |
| Experience with insurance | 0.036 | |||
| Does not have health insurance | 151 | 33.8 | Ref | |
| Has health insurance, and has not had a gap in coverage in the past year | 260 | 58.2 | 0.78*** | |
| Has health insurance, and has had a gap in coverage in the past year | 35 | 7.83 | 0.23 | |
| Table 3c: Beliefs about privacy | Mean (Range:1–4) | β' | R2 | |
| Keeping my electronic personal health information private is very important to me | 3.14 | −0.18 | 0.006 | |
| I worry that private information about my health could be used against me | 2.28 | −1.0 *** | 0.208 | |
| There are some things I would not tell my healthcare providers because I can’t trust them with the information | 2.43 | −0.82 *** | 0.160 | |
| Doctors could share embarrassing information about me with people who have no business knowing | 2.09 | −0.93 *** | 0.186 | |
| I believe the privacy of my electronic personal health information is seriously threatened | 2.44 | −0.85 *** | 0.157 | |
| Privacy Index | 2.48 | −1.5 *** | 0.246 | |
| Table 3d: Expectations of health information sharing | Mean (Range:1–4) | β' | R2 | |
| Given what you know about information sharing among organizations in the health system, do you generally have a favorable or unfavorable opinion? | 2.75 | 1.85 *** | 0.614 | |
| What effect do you think that health information sharing is likely to have on the quality of health care that you receive? | 2.82 | 1.33 *** | 0.305 | |
| How likely do you think it is that health information sharing will improve the health of people living in the United States? | 2.51 | 1.17 *** | 0.301 | |
| Table 3e: Psychosocial factors | Mean (Range:1–4) | β' | R2 | |
| Self-esteem | ||||
| I take a positive attitude toward myself | 3.13 | 0.44 *** | 0.036 | |
| I wish I could have more respect for myself | 3.00 | 0.24 ** | 0.014 | |
| I feel that I have a number of good qualities | 3.39 | 0.38 *** | 0.019 | |
| All in all, I am inclined to feel that I am a failure | 3.54 | 0.25 ** | 0.009 | |
| Self-esteem index | 3.26 | 0.48 *** | 0.027 | |
| Altruism | ||||
| I always find ways to help others less fortunate than me | 2.75 | 0.56 *** | 0.052 | |
| The dignity and well-being of all should be the most important concern in any society | 3.14 | 0.40 *** | 0.024 | |
| One of the problems of today’s society is that people are often not kind enough to others | 3.07 | −0.05 | 0.0009 | |
| All people who are unable to provide for their own needs should be helped by others | 2.85 | 0.32 ** | 0.019 | |
| Altruism Index | 2.95 | 0.56 *** | 0.029 | |
| Self-efficacy | ||||
| I can manage to solve difficult problems if I try hard enough | 3.23 | 0.56 *** | 0.036 | |
| If someone opposes me, I can find the means and ways to get what I want | 2.60 | 0.20 | 0.006 | |
| I am confident that I could deal efficiently with unexpected events | 3.10 | 0.62 *** | 0.051 | |
| I can solve most problems if I invest the necessary effort | 3.27 | 0.48 *** | 0.027 | |
| Self-efficacy Index | 3.05 | 0.71 *** | 0.041 | |
| Optimism | ||||
| I think the quality of life for the average person is getting worse, not better | 2.72 | 0.58 *** | 0.082 | |
| Generalized trust | ||||
| Generally speaking, most people can be trusted | 2.45 | 0.90*** | 0.143 |
| Trustor Characteristics | β' | p-value |
|---|---|---|
| Knowledge Questions | ||
| Average total score (out of 10). | −0.11 | <0.001 |
| Experience | ||
| Has seen primary care physician and has seen at least once in past year. | 0.34 | 0.002 |
| Beliefs about privacy | ||
| Privacy Index | −0.45 | <0.001 |
| Expectations of health information sharing | ||
| Given what you know about information sharing among organizations in the health system, do you generally have a favorable or unfavorable opinion of it? | 1.36 | <0.001 |
| Psychosocial factors | ||
| Altruism | ||
| Generalized trust |
3.2. Knowledge of Health Information Sharing
3.3. Experience with the Health System
3.4. Privacy Concerns
3.5. Expectations of Benefit
3.7. Multivariable Analysis
4. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kohane, I.S. Using electronic health records to drive discovery in disease genomics. Nat. Rev. Genet. 2011, 12, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Roden, D.; Pulley, J.; Basford, M.; Bernard, G.; Clayton, E.; Balser, J.; Masys, D. Development of a large-scale de-identified DNA biobank to enable personalized medicine. Clin. Pharmacol. Ther. 2008, 84, 362–369. [Google Scholar] [CrossRef] [PubMed]
- McCarty, C.A.; Chisholm, R.L.; Chute, C.G.; Kullo, I.J.; Jarvik, G.P.; Larson, E.B.; Li, R.; Masys, D.R.; Ritchie, M.D.; Roden, D.M.; Struewing, J.P.; et al. The eMERGE Network: A consortium of biorepositories linked to electronic medical records data for conducting genomic studies. BMC Med. Genomics 2011, 4. [Google Scholar] [CrossRef]
- Bowton, E.; Field, J.R.; Wang, S.; Schildcrout, J.S.; van Driest, S.L.; Delaney, J.T.; Cowan, J.; Weeke, P.; Mosley, J.D.; Wells, Q.S.; et al. Biobanks and electronic medical records: Enabling cost-effective research. Sci. Transl. Med. 2014, 6. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Weaving a strong trust fabric. In Digital Infrastructure for the Learning Health System: The Foundation for Continuous Improvement in Health and Health Care: Workshop Series Summary; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Malin, B.A.; Emam, K.E.; O’Keefe, C.M. Biomedical data privacy: Problems, perspectives, and recent advances. J. Am. Med. Inform. Assoc. 2013, 20, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Malin, B.; Loukides, G.; Benitez, K.; Clayton, E.W. Identifiability in biobanks: Models, measures, and mitigation strategies. Hum. Genet. 2011, 130, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Johnson, C. Securing electronic health records without impeding the flow of information. Int. J. Med. Inform. 2007, 76, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Kass, N.E.; Natowicz, M.R.; Hull, S.C.; Faden, R.R.; Plantinga, L.; Gostin, L.O.; Slutsman, J. The use of medical records in research: What do patients want? J. Law Med. Ethics 2003, 31, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Faden, R.R.; Kass, N.E.; Goodman, S.N.; Pronovost, P.; Tunis, S.; Beauchamp, T.L. An ethics framework for a learning health care system: A departure from traditional research ethics and clinical ethics. Hastings Cent. Rep. 2013, 43, S16–S27. [Google Scholar] [CrossRef]
- Taitsman, J.K.; Grimm, C.M.; Agrawal, S. Protecting patient privacy and data security. N. Engl. J. Med. 2013, 368, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Wynia, M.; Coughlin, S.; Alpert, S.; Cummins, D.; Emanuel, L. Shared expectations for protection of identifiable health care information: Report of a national consensus process. J. Gen. Intern. Med. 2011, 16, 100–111. [Google Scholar] [CrossRef]
- Thiel, D.; Platt, J.; Platt, T.; King, S.; FIsher, N.; Kardia, S. Testing an online, dynamic consent portal for large population biobank research. Publ. Health Genomics 2014, 18. [Google Scholar] [CrossRef]
- Kaye, J.; Whitley, E.A.; Lund, D.; Morrison, M.; Teare, H.; Melham, K. Dynamic consent: A patient interface for twenty-first century research networks. Eur. J. Hum. Genet. 2014. [Google Scholar] [CrossRef] [Green Version]
- Giddens, A. The Consequences of Modernity; Stanford University Press: Stanford, CA, USA, 1991. [Google Scholar]
- Wynia, M.K. Public health, public trust and lobbying. Am. J. Bioeth. 2007, 7, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Goold, S.D.; Fessler, D.; Moyer, C.A. A measure of trust in insurers. Health Serv. Res. 2006, 41, 58–78. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.A.; Dugan, E.; Zheng, B.; Mishra, A.K. Trust in physicians and medical institutions: What is it, can it be measured, and does it matter? Milbank Q. 2011, 79, 613–639. [Google Scholar] [CrossRef]
- Farrell, H. Institutions and mid-level explanations of trus. In Whom can we trust? How Groups, Networks, and Institutions Make Trust Possible; Russell Sage Foundation: New York, NY, USA, 2009; pp. 127–148. [Google Scholar]
- Cook, K.S.; Hardin, R.; Levi, M. Cooperation without Trust? Russell Sage Foundation: New York, NY, USA, 2005. [Google Scholar]
- Nannestad, P. What have we learned about generalized trust, if anything? Annu. Rev. Polit. Sci. 2008, 11, 413–436. [Google Scholar] [CrossRef]
- Hardin, R. Distrust; Russell Sage Foundation: New York, NY, USA, 2004. [Google Scholar]
- Rousseau, D.M.; Sitkin, S.B.; Burt, R.S.; Camerer, C. Not so different after all: A cross-discipline view of trust. Acad. Manage. Rev. 1998, 23, 393–404. [Google Scholar] [CrossRef]
- Ozawa, P.S.; Sripad, P. How do you measure trust in the health system? A systematic review of the literature. Soc. Sci. Med. 2013, 91, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; Zheng, B.; Dugan, E.; Camacho, F.; Kidd, E.; Mishra, A.; Balkrishnan, R. Measuring patients’ trust in their primary care providers. Med. Care Res. Rev. 2002, 59, 293–318. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.A.; Camacho, F.; Dugan, E.; Balkrishnan, R. Trust in the medical profession: Conceptual and measurement issues. Health Serv. Res. 2002, 37, 1419–1439. [Google Scholar] [CrossRef] [PubMed]
- Zheng, B.; Hall, M.A.; Dugan, E.; Kidd, K.E.; Levine, D. Development of a scale to measure patients’ trust in health insurers. Health Serv. Res. 2002, 37, 187–202. [Google Scholar] [PubMed]
- LaVeist, T.A.; Isaac, L.A.; Williams, K.P. Mistrust of health care organizations is associated with underutilization of health services. Health Serv. Res. 2009, 44, 2093–2105. [Google Scholar] [CrossRef]
- McKnight, D.H.; Choudhury, V.; Kacmar, C. Developing and validating trust measures for e-commerce: An integrative typology. Inf. Syst. Res. 2002, 13, 334–359. [Google Scholar] [CrossRef]
- Siegrist, M. The influence of trust and perceptions of risks and benefits on the acceptance of gene technology. Risk Anal. 2000, 20, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Mayer, R.C.; Davis, J.H.; Schoorman, F.D. An integrative model of organizational trust. Acad. Manage. Rev. 1995, 20, 709–734. [Google Scholar]
- Evans, G.; Durant, J. The relationship between knowledge and attitudes in the public understanding of science in Britain. Publ. Underst. Sci. 1995, 4, 57–74. [Google Scholar] [CrossRef]
- Wynne, B. Misunderstood misunderstanding: Social identities and public uptake of science. Publ. Underst. Sci. 1992, 1, 281–304. [Google Scholar] [CrossRef]
- Allum, P.S.; Sturgis, P.; Tabourazi, D.; Brunton-Smith, I. Science knowledge and attitudes across cultures: A meta-analysis. Publ. Underst. Sci. 2008, 17, 35–54. [Google Scholar] [CrossRef]
- Roberts, M.R.; Reid, G.; Schroeder, M.; Norris, S.P. Causal or spurious? The relationship of knowledge and attitudes to trust in science and technology. Publ. Underst. Sci. 2013, 22, 624–641. [Google Scholar] [CrossRef]
- Petersen, A. Biobanks engagements: Engendering trust or engineering consent? Genomics Soc. Policy 2007, 3, 31–43. [Google Scholar] [CrossRef]
- Hurwitz, J.B. User choice, privacy sensitivity, and acceptance of personal information collection. In European Data Protection: Coming of Age; Springer Netherlands: Berlin, Germany, 2013; pp. 295–312. [Google Scholar]
- Gefen, D.; Karahanna, E.; Straub, D.W. Inexperience and experience with online stores: The importance of TAM and trust. Eng. Manag. IEEE Trans. 2003, 50, 307–321. [Google Scholar] [CrossRef]
- Lewis, D.; Weigert, J. The social dynamics of trust: Theoretical and empirical research, 1985–2012. Soc. Forces 2012, 91, 25–31. [Google Scholar] [CrossRef]
- Luhmann, N. Familiarity, confidence, trust: Problems and alternatives. In Trust: Making and Breaking Cooperative Relations; Basil Blackwell: Oxford, UK, 1988; pp. 94–107. [Google Scholar]
- Committee on the Learning Health Care System in America. In Best Care at Lower Cost: The Path to Continuously Learning Health Care in America; The National Academies Press: Washington, DC, USA, 2012.
- Milstein, A. Code red and blue—Safely limiting health care’s GDP footprint. N. Engl. J. Med. 2013, 368, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Coloma, P.M.; Schuemie, M.J.; Trifirò, G.; Gini, R.; Herings, R.; Hippisley-Cox, J.; Mazzaglia, G.; Giaquinto, C.; Corrao, G.; Pedersen, L.; et al. Combining electronic healthcare databases in Europe to allow for large-scale drug safety monitoring: The EU-ADR Project. Pharmacoepidemiol. Drug Saf. 2011, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.J.; Murphy-Bollinger, J.; Scott, J.; Hudsoon, K.L. Public opinion about the importance of privacy in biobank research. Am. J. Hum. Genet. 2009, 85. [Google Scholar] [CrossRef] [PubMed]
- Pullman, D.; Etchegary, H.; Gallagher, K.; Hodgkinson, K.; Keough, M.; Morgan, D.; Street, C. Personal privacy, public benefits, and biobanks: A conjoint analysis of policy priorities and public perceptions. Genet. Med. 2012, 14. [Google Scholar] [CrossRef]
- Das, T.K.; Teng, B.S. The risk-based view of trust: A conceptual framework. J. Bus. Psychol. 2004, 19, 85–116. [Google Scholar] [CrossRef]
- Colquitt, J.A.; Scott, B.A.; LePine, J.A. Trust, trustworthiness, and trust propensity: A meta-analytic test of their unique relationships with risk taking and job performance. J. Appl. Psychol. 2007, 92, 909–927. [Google Scholar] [CrossRef] [PubMed]
- Bishop, L.; Holmes, B.J.; Kelley, C.M. National Consumer Health Privacy Survey 2005; California HealthCare Foundation: Oakland, CA, USA, 2005. [Google Scholar]
- Visschers, V.H.; Keller, C.; Siegrist, M. Climate change benefits and energy supply benefits as determinants of acceptance of nuclear power stations: Investigating an explanatory model. Energ. Polic. 2011, 39, 3621–3629. [Google Scholar] [CrossRef]
- Siegrist, M.; Connor, M.; Keller, C. Trust, confidence, procedural fairness, outcome fairness, moral conviction, and the acceptance of GM field experiments. Risk Anal. 2012, 32, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Boulware, L.E.; Cooper, L.A.; Ratner, L.E.; LaVeist, T.A.; Powe, N.R. Race and trust in the health care system. Publ. Health Rep. 2003, 118, 358–365. [Google Scholar] [CrossRef]
- Anderson, C.L.; Agarwal, R. The digitization of healthcare: Boundary risks, emotion, and consumer willingness to disclose personal health information. Inf. Syst. Res. 2011, 22, 469–490. [Google Scholar] [CrossRef]
- Thiel, D.; Platt, T.; Platt, J.; King, S.; Kardia, S.L. Community perspectives on public health biobanking: An analysis of community meetings on the Michigan Bio-Trust for health. J. Community Genet. 2014, 5, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Platt, T.; Platt, J.; Thiel, D.; Fisher, N.; Kardia, S. “Cool! And creepy”: Engaging with college student stakeholders in Michigan’s biobank (forthcoming). J. Community Genet. 2014, 5, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.W.; Marsden, P.V.; Hout, M.; Jibum, K. General Social Surveys, 1972–2012: Cumulative Codebook; Roper Center for Public Opinion Research, University of Connecticut: Storrs, CT, USA, 2013. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. Generalized self-efficacy scale. In Measures in Health Psychology: A Users Portfolio. Causal and Control Beliefs; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Rosenberg, M.; Schooler, C.; Schoenbach, C.; Rosenberg, F. Global self-esteem and specific self-esteem: Different concepts, different outcomes. Am. Sociol. Rev. 1995, 60, 141–156. [Google Scholar] [CrossRef]
- Trust Survey (Pilot). Available online: https://umich.qualtrics.com/SE/?SID=SV_dnd2Y20M8aWPcxL (accessed on 14 January 2015).
- Buhrmester, M.; Kwang, T.; Gosling, S.D. Amazon’s Mechanical Turk: A new source of inexpensive, yet high-quality, data? Perspect. Psychol. Sci. 2011, 6, 3–5. [Google Scholar] [CrossRef]
- Paolacci, G.; Chandler, J.; Ipeirotis, P. Running experiments on Amazon Mechanical turk. Judgm. Decis. Mak. 2010, 5, 411–419. [Google Scholar]
- Willison, D.J.; Steeves, V.; Charles, C.; Schwartz, L.; Ranford, J.; Agarwal, G.; Cheng, J.; Thabane, L. Consent for use of personal information for health research: Do people with potentially stigmatizing health conditions and the general public differ in their opinions? BMC Med. Ethics 2009, 10. [Google Scholar] [CrossRef]
- Duquette, D.; Langbo, C.; Bach, J.; Kleyn, M. Michigan Bio-Trust for health: Public support for using residual dried blood spot samples for health research. Publ. Health Genomics 2012, 15, 146–155. [Google Scholar] [CrossRef]
- Botkin, J.R.; Rothwell, E.; Anderson, R.; Stark, L.A.; Mitchell, J. Public attitudes regarding the use of electronic health information and residual clinical tissues for research. J. Community Genet. 2014, 5, 205–213. [Google Scholar] [CrossRef] [PubMed]
- McWhirter, R.; Critchley, C.; Nicol, D.; Chalmers, D.; Whitton, T.; Otlowski, M.; Burgess, M.; Dickinson, J. Community engagement for big epidemiology: Deliberative democracy as a tool. J. Pers. Med. 2014, 4, 459–474. [Google Scholar] [CrossRef]
- Olson, J.E.; Ryu, E.; Johnson, K.J.; Koenig, B.A.; Maschke, K.J.; Morrisette, J.A.; Liebow, M.; Takahashi, P.Y.; Fredericksen, Z.S.; Sharma, R.G.; et al. The mayo clinic biobank: A building block for individualized medicine. Mayo Clin. Proc. 2013, 88, 952–962. [Google Scholar] [CrossRef] [PubMed]
- O’Doherty, K.C.; Hawkins, A.K.; Burgess, M.M. Involving citizens in the ethics of biobank research: Informing institutional policy through structured public deliberation. Soc. Sci. Med. 2012, 75, 1604–1611. [Google Scholar] [CrossRef] [PubMed]
- Hartzler, A.; McCarty, C.A.; Rasmussen, L.V.; Williams, M.S.; Brilliant, M.; Bowton, E.A.; Clayton, E.W.; Faucett, W.A.; Ferryman, K.; Field, J.R.; et al. Stakeholder engagement: A key component of integrating genomic information into electronic health records. Genet. Med. 2013, 15, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Kimball, B.C.; Nowakowski, K.E.; Maschke, K.J.; McCormick, J.B. Genomic data in the electronic medical record: Perspectives from a biobank community advisory board. J. Empir. Res. Hum. Res. Ethics 2014, 9, 16–24. [Google Scholar] [CrossRef]
- Dixon, W.G.; Spencer, K.; Williams, H.; Sanders, C.; Lund, D.; Whitley, E.A.; Kaye, J. A dynamic model of patient consent to sharing of medical record data. Br. Med. J. 2014, 348, g1294. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Platt, J.; Kardia, S. Public Trust in Health Information Sharing: Implications for Biobanking and Electronic Health Record Systems. J. Pers. Med. 2015, 5, 3-21. https://doi.org/10.3390/jpm5010003
Platt J, Kardia S. Public Trust in Health Information Sharing: Implications for Biobanking and Electronic Health Record Systems. Journal of Personalized Medicine. 2015; 5(1):3-21. https://doi.org/10.3390/jpm5010003
Chicago/Turabian StylePlatt, Jodyn, and Sharon Kardia. 2015. "Public Trust in Health Information Sharing: Implications for Biobanking and Electronic Health Record Systems" Journal of Personalized Medicine 5, no. 1: 3-21. https://doi.org/10.3390/jpm5010003
APA StylePlatt, J., & Kardia, S. (2015). Public Trust in Health Information Sharing: Implications for Biobanking and Electronic Health Record Systems. Journal of Personalized Medicine, 5(1), 3-21. https://doi.org/10.3390/jpm5010003