
Impact of Co-Occurrence of Obesity and SARS-CoV-2 Infection during Pregnancy on Placental Pathologies and Adverse Birth Outcomes: A Systematic Review and Narrative Synthesis

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Reporting Guidelines
2.2. Information Sources and Search Terms
2.3. Inclusion Criteria
2.4. Article Screening and Data Collection
2.5. Defining Outcomes
2.6. Defining Other Variables
2.7. Grouping Studies for Synthesis
2.8. Data Synthesis and Visualisation
2.9. Study Quality Assessment
2.10. Narrative Synthesis
3. Results
3.1. Study Design, Location and Demographics
3.2. Assessment of Study Methodology Quality
3.3. SARS-CoV-2 Infection and Elevated BMI Associate with Placental Pathologies
3.4. SARS-CoV-2 Infection and Elevated BMI Do Not Affect Placental Anthropometry
3.5. SARS-CoV-2 Infection and Elevated BMI Do Not Affect Birth Anthropometry
3.6. SARS-CoV-2 Infection and Elevated BMI Associate with Fetal Demise
4. Discussion
5. Conclusions
- Determine if placental pathologies and fetal growth differ based in placental sex in cases of maternal exposure to SARS-CoV-2 and elevated BMI
- Determine in which trimester the placenta and fetus are most vulnerable to the effects of maternal infection with SARS-CoV-2 and overweight/obesity, and how timing of exposures influence:
- ◦
- occurrence of placental pathologies
- ◦
- vertical transmission
- ◦
- offspring programming
- Determine if SARS-CoV-2 symptomology (mild to severe) and other conditions heightened during pandemics (e.g., maternal stress) differentially affect:
- ◦
- placental pathologies
- ◦
- maternal and fetal inflammation
- ◦
- vertical transmission
- Determine the role of the maternal vaginal and gut microbiomes in pregnancies complicated by maternal SARS-CoV-2 and obesity and whether the microbiomes influence placental growth and development and consequently, fetal development
- Determine if a treatment targeting the gut microbiome is able to reverse or prevent poor placental development and consequently, improve fetal growth via changes at the maternal–fetal interface
- Determine if vaccines prevent adverse placental development and function and protect fetal growth
- Determine if other maternal comorbidities influence:
- ◦
- susceptibility to viral infection
- ◦
- occurrence of placental pathology
- ◦
- altered maternal and gestational tissue proinflammatory milieux
- ◦
- increased vertical transmission
- ◦
- long term offspring developmental programming
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 February 2022).
- Tremmel, M.; Gerdtham, U.G.; Nilsson, P.M.; Saha, S. Economic Burden of Obesity: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2017, 14, 435. [Google Scholar] [CrossRef] [PubMed]
- Fisher, S.C.; Kim, S.Y.; Sharma, A.J.; Rochat, R.; Morrow, B. Is obesity still increasing among pregnant women? Prepregnancy obesity trends in 20 states, 2003–2009. Prev. Med. 2013, 56, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Deputy, N.P.; Dub, B.; Sharma, A.J. Prevalence and Trends in Prepregnancy Normal Weight—48 States, New York City, and District of Columbia, 2011–2015. MMWR Morb. Mortal Wkly. Rep. 2018, 66, 1402–1407. [Google Scholar] [CrossRef] [Green Version]
- MacInnis, N.; Woolcott, C.G.; McDonald, S.; Kuhle, S. Population Attributable Risk Fractions of Maternal Overweight and Obesity for Adverse Perinatal Outcomes. Sci. Rep. 2016, 6, 22895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of Obesity among Adults and Youth: United States, 2011–2014. NCHS Data Brief 2015, 1–8. Available online: https://www.cdc.gov/nchs/products/databriefs/db219.htm#:~:text=Data%20from%20the%20National%20Health%20and%20Nutrition%20Examination%20Survey,than%20in%20men%20(34.3%25) (accessed on 1 February 2022).
- Balarajan, Y.; Villamor, E. Nationally representative surveys show recent increases in the prevalence of overweight and obesity among women of reproductive age in Bangladesh, Nepal, and India. J. Nutr. 2009, 139, 2139–2144. [Google Scholar] [CrossRef] [Green Version]
- Poston, L.; Harthoorn, L.F.; Van Der Beek, E.M.; Contributors To The ILSI Europe Workshop. Obesity in pregnancy: Implications for the mother and lifelong health of the child. A consensus statement. Pediatr. Res. 2011, 69, 175–180. [Google Scholar] [CrossRef]
- Fitzsimons, K.J.; Modder, J.; Greer, I.A. Obesity in pregnancy: Risks and management. Obstet. Med. 2009, 2, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Howell, K.R.; Powell, T.L. Effects of maternal obesity on placental function and fetal development. Reproduction 2017, 153, R97–R108. [Google Scholar] [CrossRef] [Green Version]
- Sun, C.; Groom, K.M.; Oyston, C.; Chamley, L.W.; Clark, A.R.; James, J.L. The placenta in fetal growth restriction: What is going wrong? Placenta 2020, 96, 10–18. [Google Scholar] [CrossRef]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory mechanisms in obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef] [Green Version]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]
- Mor, G.; Cardenas, I.; Abrahams, V.; Guller, S. Inflammation and pregnancy: The role of the immune system at the implantation site. Ann. N. Y. Acad. Sci. 2011, 1221, 80–87. [Google Scholar] [CrossRef] [Green Version]
- Robson, A.; Harris, L.K.; Innes, B.A.; Lash, G.E.; Aljunaidy, M.M.; Aplin, J.D.; Baker, P.N.; Robson, S.C.; Bulmer, J.N. Uterine natural killer cells initiate spiral artery remodeling in human pregnancy. FASEB J. 2012, 26, 4876–4885. [Google Scholar] [CrossRef]
- Romero, R.; Espinoza, J.; Gonçalves, L.F.; Kusanovic, J.P.; Friel, L.A.; Nien, J.K. Inflammation in preterm and term labour and delivery. Semin. Fetal Neonatal Med. 2006, 11, 317–326. [Google Scholar] [CrossRef]
- Pavan, L.; Tsatsaris, V.; Hermouet, A.; Therond, P.; Evain-Brion, D.; Fournier, T. Oxidized low-density lipoproteins inhibit trophoblastic cell invasion. J. Clin. Endocrinol. Metab. 2004, 89, 1969–1972. [Google Scholar] [CrossRef]
- Islami, D.; Bischof, P.; Chardonnens, D. Modulation of placental vascular endothelial growth factor by leptin and hCG. Mol. Hum. Reprod. 2003, 9, 395–398. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Pérez, A.; Maymó, J.; Gambino, Y.; Dueñas, J.L.; Goberna, R.; Varone, C.; Sánchez-Margalet, V. Leptin stimulates protein synthesis-activating translation machinery in human trophoblastic cells. Biol. Reprod. 2009, 81, 826–832. [Google Scholar] [CrossRef] [Green Version]
- Tessier, D.R.; Ferraro, Z.M.; Gruslin, A. Role of leptin in pregnancy: Consequences of maternal obesity. Placenta 2013, 34, 205–211. [Google Scholar] [CrossRef]
- Bar, J.; Schreiber, L.; Saruhanov, E.; Ben-Haroush, A.; Golan, A.; Kovo, M. Placental histopathological findings in obese and nonobese women with complicated and uncomplicated pregnancies. Arch. Gynecol. Obstet. 2012, 286, 1343–1347. [Google Scholar] [CrossRef]
- Kovo, M.; Zion-Saukhanov, E.; Schreiber, L.; Mevorach, N.; Divon, M.; Ben-Haroush, A.; Bar, J. The Effect of Maternal Obesity on Pregnancy Outcome in Correlation with Placental Pathology. Reprod. Sci. 2015, 22, 1643–1648. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y. Inflammatory lesions in placental pathology. J. Obstet. Gynaecol. Res. 2022, 48, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Silasi, M.; Cardenas, I.; Kwon, J.Y.; Racicot, K.; Aldo, P.; Mor, G. Viral infections during pregnancy. Am. J. Reprod. Immunol. 2015, 73, 199–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, E.Y.; Patterson, P.H. Activation of the maternal immune system induces endocrine changes in the placenta via IL-6. Brain Behav. Immun. 2011, 25, 604–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Racicot, K.; Mor, G. Risks associated with viral infections during pregnancy. J. Clin. Investig. 2017, 127, 1591–1599. [Google Scholar] [CrossRef] [Green Version]
- Horn, L.C.; Röse, I. Placental and fetal pathology in intrauterine viral infections. Intervirology 1998, 41, 219–225. [Google Scholar] [CrossRef]
- Zaga-Clavellina, V.; Diaz, L.; Olmos-Ortiz, A.; Godínez-Rubí, M.; Rojas-Mayorquín, A.E.; Ortuño-Sahagún, D. Central role of the placenta during viral infection: Immuno-competences and miRNA defensive responses. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166182. [Google Scholar] [CrossRef]
- Zemrani, B.; Gehri, M.; Masserey, E.; Knob, C.; Pellaton, R. A hidden side of the COVID-19 pandemic in children: The double burden of undernutrition and overnutrition. Int. J. Equity Health 2021, 20, 44. [Google Scholar] [CrossRef]
- Karlsson, E.A.; Marcelin, G.; Webby, R.J.; Schultz-Cherry, S. Review on the impact of pregnancy and obesity on influenza virus infection. Influenza Other Respir. Viruses 2012, 6, 449–460. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US) and National Research Council (US). Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; The National Academies Press: Washington, DC, USA, 2009; ISBN ISBN-13: 978-0-309-13113-1. [Google Scholar] [CrossRef]
- Benton, S.J.; Lafreniere, A.J.; Grynspan, D.; Bainbridge, S.A. A synoptic framework and future directions for placental pathology reporting. Placenta 2019, 77, 46–57. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.; Boyd, T.K.; Brundler, M.A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef] [Green Version]
- Macdonald, E.M.; Koval, J.J.; Natale, R.; Regnault, T.; Campbell, M.K. Population-based placental weight ratio distributions. Int. J. Pediatr. 2014, 2014, 291846. [Google Scholar] [CrossRef] [Green Version]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]
- Rubin, R. Rubin’s Pathology: Clinicopathologic Foundations of Medicine; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2008; ISBN 0-7817-9516-8 / 978-07817-9516-6. [Google Scholar]
- Derricott, H.; Jones, R.L.; Heazell, A.E. Investigating the association of villitis of unknown etiology with stillbirth and fetal growth restriction—A systematic review. Placenta 2013, 34, 856–862. [Google Scholar] [CrossRef]
- Nijman, T.A.; van Vliet, E.O.; Benders, M.J.; Mol, B.W.; Franx, A.; Nikkels, P.G.; Oudijk, M.A. Placental histology in spontaneous and indicated preterm birth: A case control study. Placenta 2016, 48, 56–62. [Google Scholar] [CrossRef]
- Dudley, D.J.; Goldenberg, R.; Conway, D.; Silver, R.M.; Saade, G.R.; Varner, M.W.; Pinar, H.; Coustan, D.; Bukowski, R.; Stoll, B.; et al. A new system for determining the causes of stillbirth. Obstet. Gynecol. 2010, 116, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Redline, R.W.; Ravishankar, S. Fetal vascular malperfusion, an update. APMIS 2018, 126, 561–569. [Google Scholar] [CrossRef] [Green Version]
- Saleemuddin, A.; Tantbirojn, P.; Sirois, K.; Crum, C.P.; Boyd, T.K.; Tworoger, S.; Parast, M.M. Obstetric and perinatal complications in placentas with fetal thrombotic vasculopathy. Pediatr. Dev. Pathol. 2010, 13, 459–464. [Google Scholar] [CrossRef]
- Lepais, L.; Gaillot-Durand, L.; Boutitie, F.; Lebreton, F.; Buffin, R.; Huissoud, C.; Massardier, J.; Guibaud, L.; Devouassoux-Shisheboran, M.; Allias, F. Fetal thrombotic vasculopathy is associated with thromboembolic events and adverse perinatal outcome but not with neurologic complications: A retrospective cohort study of 54 cases with a 3-year follow-up of children. Placenta 2014, 35, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Vik, T.; Redline, R.; Nelson, K.B.; Bjellmo, S.; Vogt, C.; Ng, P.; Strand, K.M.; Nu, T.N.T.; Oskoui, M. The Placenta in Neonatal Encephalopathy: A Case-Control Study. J. Pediatr. 2018, 202, 77. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, P.; Huppertz, B.; Frank, H.G. The fibrinoids of the human placenta: Origin, composition and functional relevance. Ann. Anat. 1996, 178, 485–501. [Google Scholar] [CrossRef] [PubMed]
- Devisme, L.; Chauvière, C.; Franquet-Ansart, H.; Chudzinski, A.; Stichelbout, M.; Houfflin-Debarge, V.; Subtil, D. Perinatal outcome of placental massive perivillous fibrin deposition: A case-control study. Prenat. Diagn. 2017, 37, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Mutter, G.L.; Mooney, E.E. Pathology of the Female Reproductive Tract; Implantation and Placenta—Perivillous Fibrin Deposition and Maternal Floor ‘Infarction’; Churchill Livingstone: London, UK, 2014; ISBN 978-0-443-07477-6. [Google Scholar]
- He, M.; Migliori, A.; Maari, N.S.; Mehta, N.D. Follow-up and management of recurrent pregnancy losses due to massive perivillous fibrinoid deposition. Obstet. Med. 2018, 11, 17–22. [Google Scholar] [CrossRef]
- Ortega, M.A.; Saez, M.; Asúnsolo, Á.; Romero, B.; Bravo, C.; Coca, S.; Sainz, F.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Upregulation of VEGF and PEDF in Placentas of Women with Lower Extremity Venous Insufficiency during Pregnancy and Its Implication in Villous Calcification. BioMed Res. Int. 2019, 2019, 5320902. [Google Scholar] [CrossRef]
- Moran, M.C.; Mulcahy, C.; Zombori, G.; Ryan, J.; Downey, P.; McAuliffe, F.M. Placental volume, vasculature and calcification in pregnancies complicated by pre-eclampsia and intra-uterine growth restriction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 195, 12–17. [Google Scholar] [CrossRef]
- Zeng, J.; Marcus, A.; Buhtoiarova, T.; Mittal, K. Distribution and potential significance of intravillous and intrafibrinous particulate microcalcification. Placenta 2017, 50, 94–98. [Google Scholar] [CrossRef]
- Schweikhart, G.; Kaufmann, P.; Beck, T. Morphology of placental villi after premature delivery and its clinical relevance. Arch. Gynecol. 1986, 239, 101–114. [Google Scholar] [CrossRef]
- Turowski, G.; Vogel, M. Re-view and view on maturation disorders in the placenta. APMIS 2018, 126, 602–612. [Google Scholar] [CrossRef]
- Redline, R.W. Distal villous immaturity. Diagn. Histopathol. 2012, 18, 189–194. [Google Scholar] [CrossRef]
- Neville, G.; Russell, N.; O’Donoghue, K.; Fitzgerald, B. Rounded intraplacental hematoma—A high risk placental lesion as illustrated by a prospective study of 26 consecutive cases. Placenta 2019, 81, 18–24. [Google Scholar] [CrossRef]
- Stevens, D.U.; de Nobrega Teixeira, J.A.; Spaanderman, M.E.A.; Bulten, J.; van Vugt, J.M.G.; Al-Nasiry, S. Understanding decidual vasculopathy and the link to preeclampsia: A review. Placenta 2020, 97, 95–100. [Google Scholar] [CrossRef]
- Fox, H.; Elston, C.W. Pathology of the placenta. Major Probl. Pathol. 1978, 7, 1–491. [Google Scholar] [CrossRef]
- Basnet, K.M.; Bentley-Lewis, R.; Wexler, D.J.; Kilic, F.; Roberts, D.J. Prevalence of Intervillous Thrombi Is Increased in Placentas from Pregnancies Complicated by Diabetes. Pediatr. Dev. Pathol. 2016, 19, 502–505. [Google Scholar] [CrossRef]
- Crocker, I. Gabor Than Award Lecture 2006: Pre-eclampsia and villous trophoblast turnover: Perspectives and possibilities. Placenta 2007, 28, S4–S13. [Google Scholar] [CrossRef]
- Vedmedovska, N.; Rezeberga, D.; Teibe, U.; Melderis, I.; Donders, G.G. Placental pathology in fetal growth restriction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 155, 36–40. [Google Scholar] [CrossRef]
- Becroft, D.M.; Thompson, J.M.; Mitchell, E.A. Placental infarcts, intervillous fibrin plaques, and intervillous thrombi: Incidences, cooccurrences, and epidemiological associations. Pediatr. Dev. Pathol. 2004, 7, 26–34. [Google Scholar] [CrossRef]
- Shen-Schwarz, S.; Ruchelli, E.; Brown, D. Villous oedema of the placenta: A clinicopathological study. Placenta 1989, 10, 297–307. [Google Scholar] [CrossRef]
- Ruffolo, P.R. The pathogenesis of necrosis. I. Correlated light and electron microscopic observations of the myocardial necrosis induced by the intravenous injection of papain. Am. J. Pathol. 1964, 45, 741–756. [Google Scholar]
- Watkins, J.C.; Torous, V.F.; Roberts, D.J. Defining Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Placentitis. Arch. Pathol. Lab. Med. 2021, 145, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, J.S.; Nijland, M.J.; Knoblich, P. Placental ischemia and cardiovascular dysfunction in preeclampsia and beyond: Making the connections. Expert Rev. Cardiovasc. Ther. 2008, 6, 1367–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, J.M. Pathophysiology of ischemic placental disease. Semin. Perinatol. 2014, 38, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Handel, B.J.; Prashad, S.; Huang, A.; Hamalainen, E.; Chen, A.; Mikkola, H.K. The First Trimester Human Placenta Is a Site of Primitive Red Blood Cell Maturation. Blood 2007, 110, 2224. [Google Scholar] [CrossRef]
- Van Handel, B.; Prashad, S.L.; Hassanzadeh-Kiabi, N.; Huang, A.; Magnusson, M.; Atanassova, B.; Chen, A.; Hamalainen, E.I.; Mikkola, H.K. The first trimester human placenta is a site for terminal maturation of primitive erythroid cells. Blood 2010, 116, 3321–3330. [Google Scholar] [CrossRef] [Green Version]
- da Cunha Castro, E.C.; Popek, E. Abnormalities of placenta implantation. APMIS 2018, 126, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.A.; Ernst, L.M.; Miller, E.S. Basal Plate Myometrial Fibers and Hypertensive Disorders of Pregnancy: A Case-Control Study. Pediatr. Dev. Pathol. 2018, 21, 296–299. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Moga, C.; Guo, B.; Schopflocher, D.; Harstall, C. Development of a Quality Appraisal Tool for Case Series Studies Using a Modified Delphi Technique; The Institute of Health Economics: Edmonton, AB, Canada, 2012; Available online: https://www.ihe.ca/research-programs/rmd/cssqac/cssqac-about (accessed on 1 February 2022).
- Indraccolo, U.; Graziani, C.; Di Iorio, R.; Corona, G.; Bonito, M.; Indraccolo, S.R. External cephalic version for singleton breech presentation: Proposal of a practical check-list for obstetricians. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2340–2353. [Google Scholar]
- Schwartz, D.A.; Baldewijns, M.; Benachi, A.; Bugatti, M.; Collins, R.R.J.; De Luca, D.; Facchetti, F.; Linn, R.L.; Marcelis, L.; Morotti, D.; et al. Chronic Histiocytic Intervillositis with Trophoblast Necrosis Is a Risk Factor Associated with Placental Infection from Coronavirus Disease 2019 (COVID-19) and Intrauterine Maternal-Fetal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Transmission in Live-Born and Stillborn Infants. Arch. Pathol. Lab. Med. 2021, 145, 517–528. [Google Scholar] [CrossRef]
- Richtmann, R.; Torloni, M.R.; Otani, A.R.; Levi, J.E.; Tobara, M.C.; de Almeida Silva, C.; Dias, L.; Miglioli-Galvão, L.; Silva, P.M.; Kondo, M.M. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: A case series. Case Rep. Womens Health 2020, 27, e00243. [Google Scholar] [CrossRef]
- Menter, T.; Mertz, K.D.; Jiang, S.; Chen, H.; Monod, C.; Tzankov, A.; Waldvogel, S.; Schulzke, S.M.; Hösli, I.; Bruder, E. Placental Pathology Findings during and after SARS-CoV-2 Infection: Features of Villitis and Malperfusion. Pathobiology 2021, 88, 69–77. [Google Scholar] [CrossRef]
- Jang, W.K.; Lee, S.Y.; Park, S.; Ryoo, N.H.; Hwang, I.; Park, J.M.; Bae, J.G. Pregnancy outcome, antibodies, and placental pathology in SARS-CoV-2 infection during early pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 5709. [Google Scholar] [CrossRef]
- Fan, C.; Guo, Y.; Qu, P.; Wang, S.; Wang, M.; Yuan, J.; Li, C.; Gao, L.; Pang, Y.; Li, Z.; et al. No obviously adverse pregnancy complications and outcomes of the recovered pregnant women from COVID-19. Reprod. Toxicol. 2021, 100, 163–166. [Google Scholar] [CrossRef]
- Hanna, N.; Lin, X.; Thomas, K.; Vintzileos, A.; Chavez, M.; Palaia, T.; Ragolia, L.; Verma, S.; Khullar, P.; Hanna, I. Underestimation of SARS-CoV-2 infection in placental samples. Am. J. Obstet. Gynecol. 2021, 225, 572–575.e1. [Google Scholar] [CrossRef]
- Adhikari, E.H.; Moreno, W.; Zofkie, A.C.; MacDonald, L.; McIntire, D.D.; Collins, R.R.; Spong, C.Y. Pregnancy outcomes among women with and without severe acute respiratory syndrome Coronavirus 2 infection. JAMA Netw. Open 2020, 3, e2029256. [Google Scholar] [CrossRef]
- Patberg, E.T.; Adams, T.; Rekawek, P.; Vahanian, S.A.; Akerman, M.; Hernandez, A.; Rapkiewicz, A.V.; Ragolia, L.; Sicuranza, G.; Chavez, M.R.; et al. Coronavirus disease 2019 infection and placental histopathology in women delivering at term. Am. J. Obstet. Gynecol. 2021, 224, 382.e1–382.e18. [Google Scholar] [CrossRef]
- Brien, M.E.; Bouron-Dal Soglio, D.; Dal Soglio, S.; Couture, C.; Boucoiran, I.; Nasr, Y.; Widdows, K.; Sharps, M.C.; El Demellawy, D.; Ep Heazell, A.; et al. Pandemic stress and SARS-CoV-2 infection are associated with pathological changes at the maternal-fetal interface. Placenta 2021, 115, 37–44. [Google Scholar] [CrossRef]
- Lu-Culligan, A.; Chavan, A.R.; Vijayakumar, P.; Irshaid, L.; Courchaine, E.M.; Milano, K.M.; Tang, Z.; Pope, S.D.; Song, E.; Vogels, C.B.F.; et al. SARS-CoV-2 infection in pregnancy is associated with robust inflammatory response at the maternal-fetal interface. medRxiv 2021. [Google Scholar] [CrossRef]
- Joseph, N.T.; Dude, C.M.; Verkerke, H.P.; Irby, L.S.; Dunlop, A.L.; Patel, R.M.; Easley, K.A.; Smith, A.K.; Stowell, S.R.; Jamieson, D.J.; et al. Maternal Antibody Response, Neutralizing Potency, and Placental Antibody Transfer after Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Obstet. Gynecol. 2021, 138, 189–197. [Google Scholar] [CrossRef]
- Rosenbloom, J.I.; Raghuraman, N.; Carter, E.B.; Kelly, J.C. Coronavirus disease 2019 infection and hypertensive disorders of pregnancy. Am. J. Obstet. Gynecol. 2021, 224, 623–624. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.J.; Romero, R.; Chaemsaithong, P.; Kim, J.S. Chronic inflammation of the placenta: Definition, classification, pathogenesis, and clinical significance. Am. J. Obstet. Gynecol. 2015, 213, S53–S69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, M.; Curran, P.; Raker, C.; Martin, S.; Larson, L.; Bourjeily, G. Placental findings associated with maternal obesity at early pregnancy. Pathol. Res. Pract. 2016, 212, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Duffley, E.; Grynspan, D.; Scott, H.; Lafreniere, A.; Vereira de Andrade, C.B.; Bloise, E.; Connor, K.L. Gestational age and infection are greater predictors of placental histopathology than maternal prepregnancy BMI. medRxiv 2021. [Google Scholar] [CrossRef]
- Goldstein, J.A.; Gallagher, K.; Beck, C.; Kumar, R.; Gernand, A.D. Maternal-Fetal Inflammation in the Placenta and the Developmental Origins of Health and Disease. Front. Immunol. 2020, 11, 531543. [Google Scholar] [CrossRef]
- Megli, C.J.; Coyne, C.B. Infections at the maternal-fetal interface: An overview of pathogenesis and defence. Nat. Rev. Microbiol. 2022, 20, 67–82. [Google Scholar] [CrossRef]
- Barke, T.L.; Money, K.M.; Du, L.; Serezani, A.; Gannon, M.; Mirnics, K.; Aronoff, D.M. Sex modifies placental gene expression in response to metabolic and inflammatory stress. Placenta 2019, 78, 1–9. [Google Scholar] [CrossRef]
- Bustamante Helfrich, B.; Chilukuri, N.; He, H.; Cerda, S.R.; Hong, X.; Wang, G.; Pearson, C.; Burd, I.; Wang, X. Maternal vascular malperfusion of the placental bed associated with hypertensive disorders in the Boston Birth Cohort. Placenta 2017, 52, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Chou, D.; Ma, Y.; Zhang, J.; McGrath, C.; Parry, S. Cytomegalovirus infection of trophoblast cells elicits an inflammatory response: A possible mechanism of placental dysfunction. Am. J. Obstet. Gynecol. 2006, 194, 535–541. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Pathophysiology of placental-derived fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S745–S761. [Google Scholar] [CrossRef] [Green Version]
- Ernst, L.M. Maternal vascular malperfusion of the placental bed. APMIS 2018, 126, 551–560. [Google Scholar] [CrossRef] [Green Version]
- Gaillard, R.; Durmuş, B.; Hofman, A.; Mackenbach, J.P.; Steegers, E.A.; Jaddoe, V.W. Risk factors and outcomes of maternal obesity and excessive weight gain during pregnancy. Obesity 2013, 21, 1046–1055. [Google Scholar] [CrossRef]
- Cooper, H.J.; Iwamoto, M.; Lash, M.; Conners, E.E.; Paladini, M.; Slavinski, S.; Fine, A.D.; Kennedy, J.; Heinke, D.; Ciaranello, A.; et al. Maternal Zika Virus Infection: Association with Small-for-Gestational-Age Neonates and Preterm Birth. Obstet. Gynecol. 2019, 134, 1197–1204. [Google Scholar] [CrossRef] [Green Version]




 represents NW women;
represents NW women;  represents women who are either NW or OW;
represents women who are either NW or OW;  represents OW women and
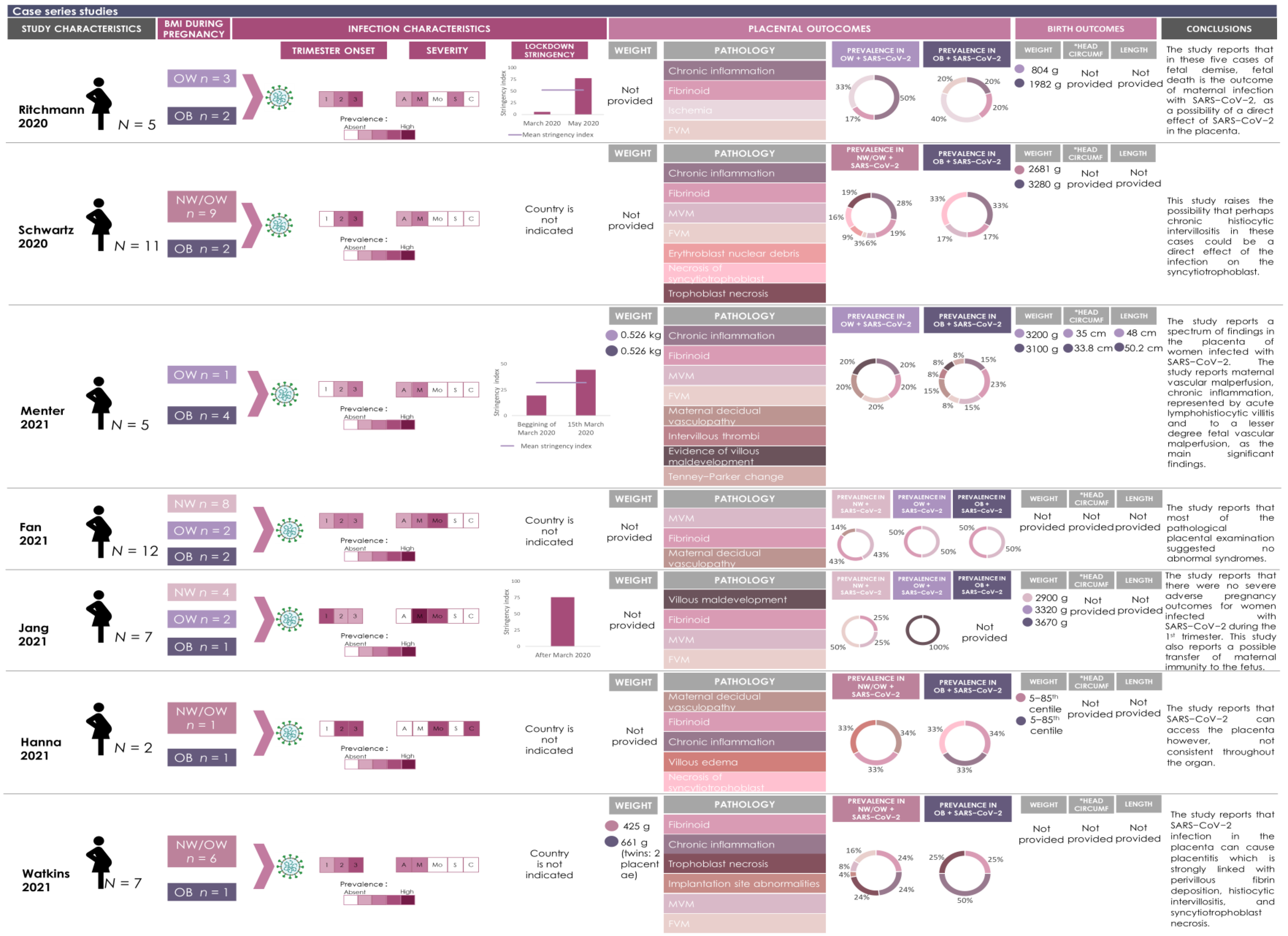
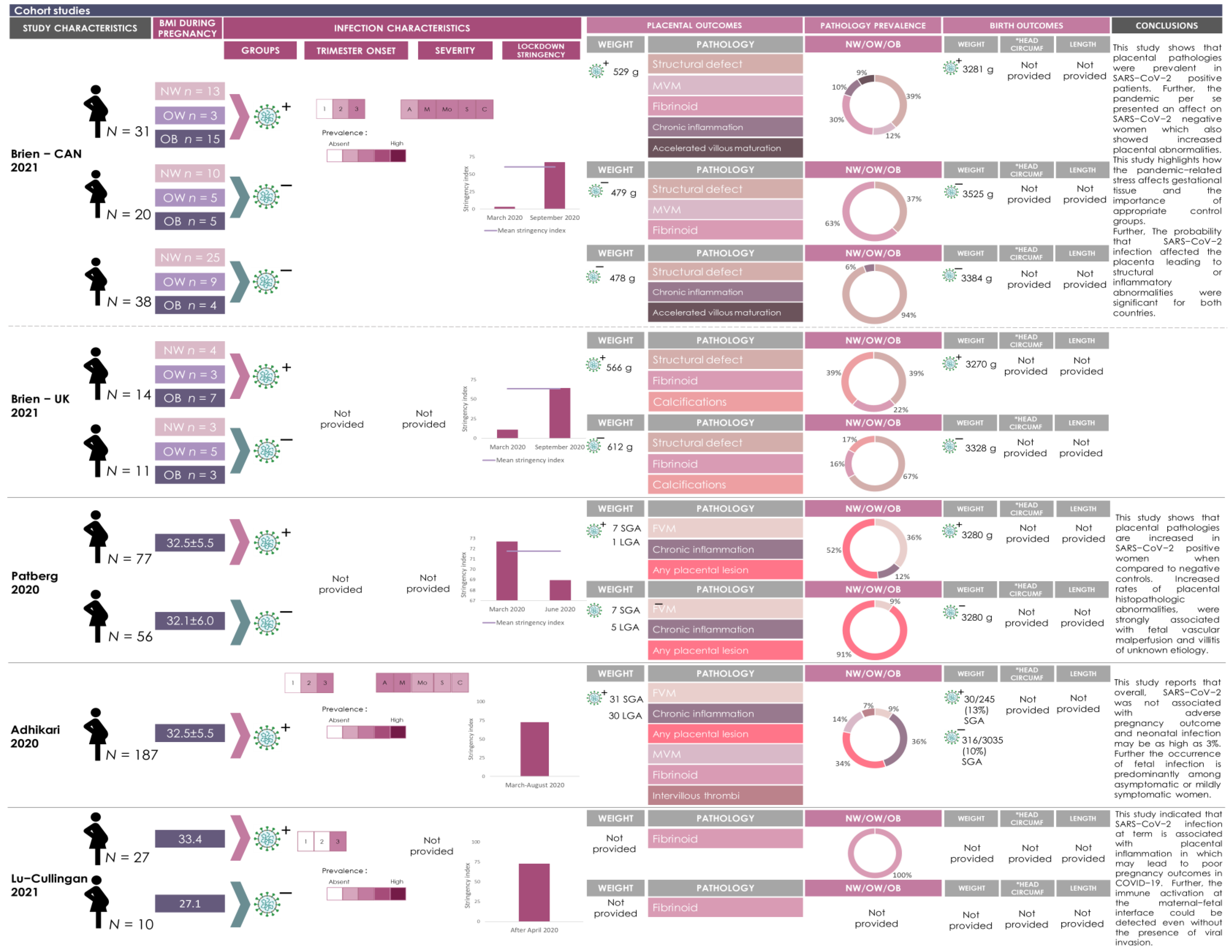
represents OW women and  represents OB women. The prevalence of viral infection during each trimester is represented by different shades of pink (higher the n, darker the color. Blank means absent). The severity of the infection is categorized by asymptomatic (A); mild (M); moderate (Mo), severe (S) and critical (C) and the prevalence is represented by different shades of pink (higher the n, darker the color. Blank means absent). The lockdown stringency in each country during the timeline of the study is represented as a bar chart. The mean lockdown stringency index is indicated for studies that were conducted over one month. Each placental pathology reported in the study was further categorized according to the synoptic framework for placental pathology. The prevalence of placental pathologies is represented in pie charts and categorized by maternal BMI. Rectangles of different colors are representing the placental pathologies and correspond with the colors of the placental pathologies represented in the pie chart. Placental pathologies in cases of SARS-CoV-2 infection are represented by the prevalence (n number) stratified by BMI category. Placental and birth anthropometry values are represented by the mean of each maternal BMI category. *Head Circumf = head circumference.
represents NW women; represents women who are either NW or OW; represents OW women and represents OB women. The prevalence of viral infection during each trimester is represented by different shades of pink (higher the n, darker the color. Blank means absent). The severity of the infection is categorized by asymptomatic (A); mild (M); moderate (Mo), severe (S) and critical (C) and the prevalence is represented by different shades of pink (higher the n, darker the color. Blank means absent). The lockdown stringency in each country during the timeline of the study is represented as a bar chart. The mean lockdown stringency index is indicated for studies that were conducted over one month. Each placental pathology reported in the study was further categorized according to the synoptic framework for placental pathology. The prevalence of placental pathologies is represented in pie charts and categorized by maternal BMI. Rectangles of different colors are representing the placental pathologies and correspond with the colors of the placental pathologies represented in the pie chart. Placental pathologies in cases of SARS-CoV-2 infection are represented by the prevalence (n number) stratified by BMI category. Placental and birth anthropometry values are represented by the mean of each maternal BMI category. *Head Circumf = head circumference.
represents OB women. The prevalence of viral infection during each trimester is represented by different shades of pink (higher the n, darker the color. Blank means absent). The severity of the infection is categorized by asymptomatic (A); mild (M); moderate (Mo), severe (S) and critical (C) and the prevalence is represented by different shades of pink (higher the n, darker the color. Blank means absent). The lockdown stringency in each country during the timeline of the study is represented as a bar chart. The mean lockdown stringency index is indicated for studies that were conducted over one month. Each placental pathology reported in the study was further categorized according to the synoptic framework for placental pathology. The prevalence of placental pathologies is represented in pie charts and categorized by maternal BMI. Rectangles of different colors are representing the placental pathologies and correspond with the colors of the placental pathologies represented in the pie chart. Placental pathologies in cases of SARS-CoV-2 infection are represented by the prevalence (n number) stratified by BMI category. Placental and birth anthropometry values are represented by the mean of each maternal BMI category. *Head Circumf = head circumference.
represents NW women; represents women who are either NW or OW; represents OW women and represents OB women. The prevalence of viral infection during each trimester is represented by different shades of pink (higher the n, darker the color. Blank means absent). The severity of the infection is categorized by asymptomatic (A); mild (M); moderate (Mo), severe (S) and critical (C) and the prevalence is represented by different shades of pink (higher the n, darker the color. Blank means absent). The lockdown stringency in each country during the timeline of the study is represented as a bar chart. The mean lockdown stringency index is indicated for studies that were conducted over one month. Each placental pathology reported in the study was further categorized according to the synoptic framework for placental pathology. The prevalence of placental pathologies is represented in pie charts and categorized by maternal BMI. Rectangles of different colors are representing the placental pathologies and correspond with the colors of the placental pathologies represented in the pie chart. Placental pathologies in cases of SARS-CoV-2 infection are represented by the prevalence (n number) stratified by BMI category. Placental and birth anthropometry values are represented by the mean of each maternal BMI category. *Head Circumf = head circumference.



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferraz, T.; Benton, S.J.; Zareef, I.; Aribaloye, O.; Bloise, E.; Connor, K.L. Impact of Co-Occurrence of Obesity and SARS-CoV-2 Infection during Pregnancy on Placental Pathologies and Adverse Birth Outcomes: A Systematic Review and Narrative Synthesis. Pathogens 2023, 12, 524. https://doi.org/10.3390/pathogens12040524
Ferraz T, Benton SJ, Zareef I, Aribaloye O, Bloise E, Connor KL. Impact of Co-Occurrence of Obesity and SARS-CoV-2 Infection during Pregnancy on Placental Pathologies and Adverse Birth Outcomes: A Systematic Review and Narrative Synthesis. Pathogens. 2023; 12(4):524. https://doi.org/10.3390/pathogens12040524
Chicago/Turabian StyleFerraz, Thaina, Samantha J. Benton, Israa Zareef, Oluwatomike Aribaloye, Enrrico Bloise, and Kristin L. Connor. 2023. "Impact of Co-Occurrence of Obesity and SARS-CoV-2 Infection during Pregnancy on Placental Pathologies and Adverse Birth Outcomes: A Systematic Review and Narrative Synthesis" Pathogens 12, no. 4: 524. https://doi.org/10.3390/pathogens12040524
APA StyleFerraz, T., Benton, S. J., Zareef, I., Aribaloye, O., Bloise, E., & Connor, K. L. (2023). Impact of Co-Occurrence of Obesity and SARS-CoV-2 Infection during Pregnancy on Placental Pathologies and Adverse Birth Outcomes: A Systematic Review and Narrative Synthesis. Pathogens, 12(4), 524. https://doi.org/10.3390/pathogens12040524