
Detection of Clinical and Subclinical Lumpy Skin Disease Using Ear Notch Testing and Skin Biopsies

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
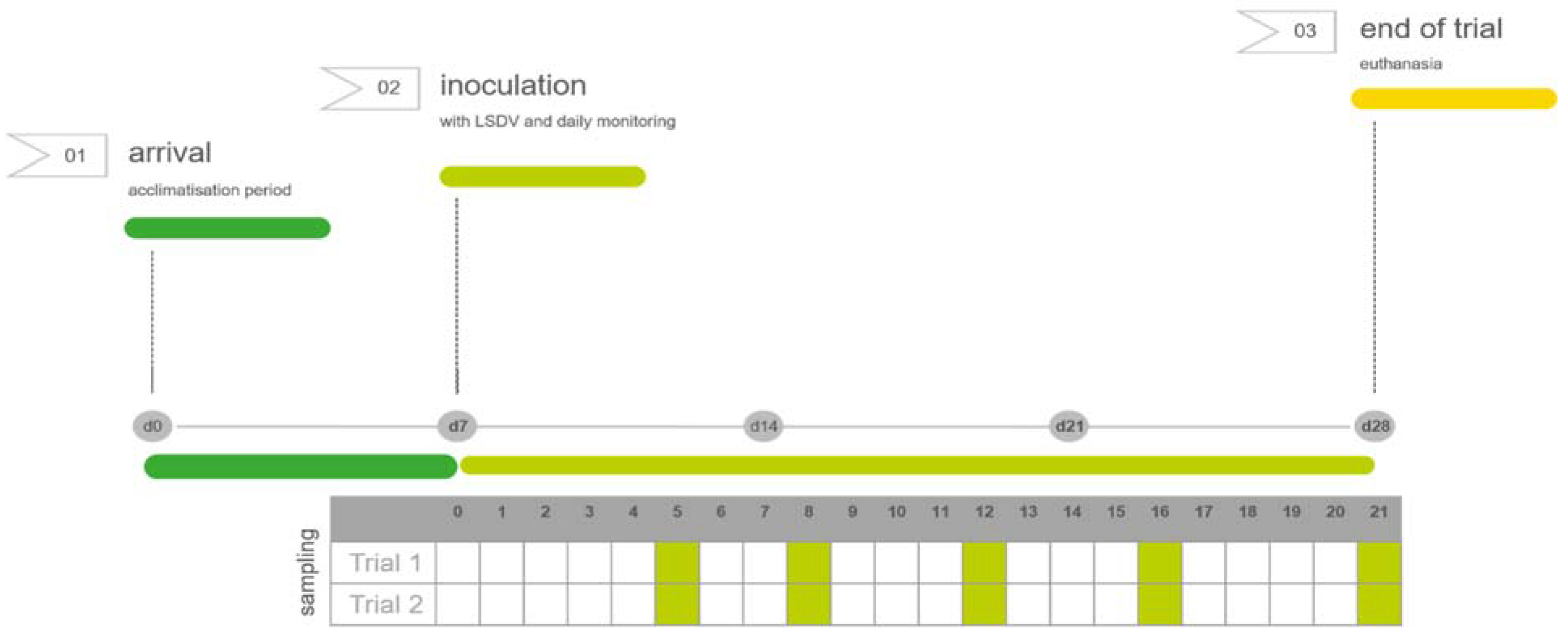
2.1. Animal Inoculation with LSDV
2.2. Clinical Observations, Sample Collection
2.3. Molecular Analysis
2.4. Serological Analysis
2.5. Statistical Analysis
2.6. Ethical and Biosafety Approval Code
3. Results
3.1. Clinical Observations
3.1.1. Animal Survival
3.1.2. Body Temperature
3.1.3. Clinical Scoring
3.1.4. Clinical Versus Subclinical Infection
3.2. Molecular Analysis
3.2.1. EDTA Blood Samples
3.2.2. Skin Biopsies and Ear Notches
3.2.3. Subclinical Versus Clinical Infection
3.3. Serological Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tuppurainen, E.S.M.; Venter, E.H.; Shisler, J.L.; Gari, G.; Mekonnen, G.A.; Juleff, N.; Lyons, N.A.; De Clercq, K.; Upton, C.; Bowden, T.R.; et al. Review: Capripoxvirus Diseases: Current Status and Opportunities for Control. Transbound. Emerg. Dis. 2017, 64, 729–745. [Google Scholar] [CrossRef] [PubMed]
- Abera, Z.; Degefu, H.; Gari, G.; Ayana, Z. Review on Epidemiology and Economic Importance of Lumpy Skin Disease. Int. J. Basic Appl. Virol. 2015, 4, 8–21. [Google Scholar] [CrossRef]
- Casal, J.; Allepuz, A.; Miteva, A.; Pite, L.; Tabakovsky, B.; Terzievski, D.; Alexandrov, T.; Beltrán-Alcrudo, D. Economic Cost of Lumpy Skin Disease Outbreaks in Three Balkan Countries: Albania, Bulgaria and the Former Yugoslav Republic of Macedonia (2016–2017). Transbound. Emerg. Dis. 2018, 65, 1680–1688. [Google Scholar] [CrossRef] [PubMed]
- Limon, G.; Gamawa, A.A.; Ahmed, A.I.; Lyons, N.A.; Beard, P.M. Epidemiological Characteristics and Economic Impact of Lumpy Skin Disease, Sheeppox and Goatpox Among Subsistence Farmers in Northeast Nigeria. Front. Vet. Sci. 2020, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Sohier, C.; Haegeman, A.; Mostin, L.; De Leeuw, I.; Campe, W.V.; De Vleeschauwer, A.; Tuppurainen, E.S.M.; van den Berg, T.; De Regge, N.; De Clercq, K. Experimental Evidence of Mechanical Lumpy Skin Disease Virus Transmission by Stomoxys Calcitrans Biting Flies and Haematopota Spp. Horseflies. Sci. Rep. 2019, 9, 20076. [Google Scholar] [CrossRef]
- Sanz-Bernardo, B.; Haga, I.R.; Wijesiriwardana, N.; Basu, S.; Larner, W.; Diaz, A.V.; Langlands, Z.; Denison, E.; Stoner, J.; White, M.; et al. Quantifying and Modeling the Acquisition and Retention of Lumpy Skin Disease Virus by Hematophagus Insects Reveals Clinically but Not Subclinically Affected Cattle Are Promoters of Viral Transmission and Key Targets for Control of Disease Outbreaks. J. Virol. 2021, 95, e02239-20. [Google Scholar] [CrossRef]
- Nielsen, S.S.; Alvarez, J.; Bicout, D.J.; Calistri, P.; Canali, E.; Drewe, J.A.; Garin-Bastuji, B.; Gonzales Rojas, J.L.; Gortazar Schmidt, C.; et al.; EFSA AHAW Panel (EFSA Panel on Animal Health and Welfare) Scientific Opinion on the assessment of the control measures for category A diseases of Animal Health Law: Lumpy Skin Disease. EFSA J. 2021, 19, 70. [Google Scholar] [CrossRef]
- Carn, V.M.; Kitching, R.P. An Investigation of Possible Routes of Transmission of Lumpy Skin Disease Virus (Neethling). Epidemiol. Infect. 1995, 114, 219–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuppurainen, E.S.M.; Venter, E.H.; Coetzer, J.A.W. The Detection of Lumpy Skin Disease Virus in Samples of Experimentally Infected Cattle Using Different Diagnostic Techniques. Onderstepoort J. Vet. Res. 2005, 72, 153–164. [Google Scholar] [CrossRef]
- Kononov, A.; Prutnikov, P.; Shumilova, I.; Kononova, S.; Nesterov, A.; Byadovskaya, O.; Pestova, Y.; Diev, V.; Sprygin, A. Determination of Lumpy Skin Disease Virus in Bovine Meat and Offal Products Following Experimental Infection. Transbound. Emerg. Dis. 2019, 66, 1332–1340. [Google Scholar] [CrossRef]
- Wainwright, S.; El Idrissi, A.; Mattioli, R.; Tibbo, M.; Njeumi, F.; Raizman, E. Emergence of Lumpy Skin Disease in the East ErnMediterranean Basin Countries. In Empres Watch; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2013; Volume 29, pp. 1–6. [Google Scholar]
- Tasioudi, K.E.; Antoniou, S.E.; Iliadou, P.; Sachpatzidis, A.; Plevraki, E.; Agianniotaki, E.I.; Fouki, C.; Mangana-Vougiouka, O.; Chondrokouki, E.; Dile, C. Emergence of Lumpy Skin Disease in Greece, 2015. Transbound. Emerg. Dis. 2016, 63, 260–265. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Scientific report on lumpy skin disease: I. Data collection and analysis. EFSA J. 2017, 15, 4773. [Google Scholar] [CrossRef] [Green Version]
- FAO. Sustainable Prevention, Control and Elimination of Lumpy Skin Disease—Eastern Europe and the Balkan. In FAO Animal Production and Health Position Paper; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2017; Volume 2, p. 25. ISBN 978-92-5-109937-7. [Google Scholar]
- Sprygin, A.; Artyuchova, E.; Babin, Y.; Prutnikov, P.; Kostrova, E.; Byadovskaya, O.; Kononov, A. Epidemiological Characterization of Lumpy Skin Disease Outbreaks in Russia in 2016. Transbound. Emerg. Dis. 2018, 65, 1514–1521. [Google Scholar] [CrossRef]
- Roche, X.; Rozstalnyy, A.; TagoPacheco, D.; Kamata, A.; Pittiglio, C.; Alcrudo, D.B.; Bisht, K.; Karki, S.; Kayamori, J.; Larfaoui, F.; et al. Introduction and Spread of Lumpy Skin Disease in South, East and Southeast Asia: Qualitative Risk Assessment and Management. In FAO Animal Production and Health Papers; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2020; Volume 183, p. 62. ISBN 978-92-5-133563-5. [Google Scholar]
- Calistri, P.; De Clercq, K.; Gubbins, S.; Klement, E.; Stegeman, A.; Abrahantes, J.C.; Marojevic, D.; Antoniou, S.-E.; Broglia, A. Lumpy Skin Disease Epidemiological Report IV: Data Collection and Analysis. EFSA J. 2020, 18, e06010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindberg, A.; Brownlie, J.; Gunn, G.J.; Houe, H.; Moennig, V.; Saatkamp, H.W.; Sandvik, T.; Valle, P.S. The Control of Bovine Viral Diarrhoea Virus in Europe: Today and in the Future. Rev. Sci. Tech. Int. Off. Epizoot. 2006, 25, 961–979. [Google Scholar] [CrossRef]
- Albrecht, K.; Linder, M.; Heinrich, A.; Höche, J.; Beer, M.; Gaede, W.; Wernike, K. Re-Introduction of Bovine Viral Diarrhea Virus in a Disease-Free Region: Impact on the Affected Cattle Herd and Diagnostic Implications. Pathogens 2021, 10, 360. [Google Scholar] [CrossRef]
- Babiuk, S.; Parkyn, G.; Copps, J.; Larence, J.E.; Sabara, M.I.; Bowden, T.R.; Boyle, D.B.; Kitching, R.P. Evaluation of an Ovine Testis Cell Line (OA3.Ts) for Propagation of Capripoxvirus Isolates and Development of an Immunostaining Technique for Viral Plaque Visualization. J. Vet. Diagn. Investig. 2007, 19, 486–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haegeman, A.; De Leeuw, I.; Mostin, L.; Van Campe, W.; Aerts, L.; Venter, E.; Tuppurainen, E.; Saegerman, C.; De Clercq, K. Comparative evaluation of lumpy skin disease virus-based live attenuated vaccines. Vaccines 2021, 9, 473. [Google Scholar] [CrossRef]
- Sameea Yousefi, P.; Mardani, K.; Dalir-Naghadeh, B.; Jalilzadeh-Amin, G. Epidemiological study of lumpy skin disease outbreaks in North-western Iran. Transbound. Emerg. Dis. 2017, 64, 1782–1789. [Google Scholar] [CrossRef]
- Haegeman, A.; Zro, K.; Vandenbussche, F.; Demeestere, L.; Van Campe, W.; Ennaji, M.M.; De Clercq, K. Development and Validation of Three Capripoxvirus Real-Time PCRs for Parallel Testing. J. Virol. Methods 2013, 193, 446–451. [Google Scholar] [CrossRef]
- Haegeman, A.; De Leeuw, I.; Mostin, L.; Van Campe, W.; Aerts, L.; Vastag, M.; De Clercq, K. An Immunoperoxidase Monolayer Assay (IPMA) for the detection of Lumpy skin disease antibodies. J. Virol. Methods 2020, 277, 113800. [Google Scholar] [CrossRef] [PubMed]
- Midway, S.; Robertson, M.; Flinn, S.; Kaller, M. Comparing multiple comparisons: Practical guidance for choosing the best multiple comparisons test. PeerJ 2020, 8, e10387. [Google Scholar] [CrossRef] [PubMed]
- Tuppurainen, E.S.M.; Lubinga, J.C.; Stoltsz, W.H.; Troskie, M.; Carpenter, S.T.; Coetzer, J.A.W.; Venter, E.H.; Oura, C.A.L. Mechanical Transmission of Lumpy Skin Disease Virus by Rhipicephalus Appendiculatus Male Ticks. Epidemiol. Infect. 2013, 141, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Issimov, A.; Kutumbetov, L.; Orynbayev, M.B.; Khairullin, B.; Myrzakhmetova, B.; Sultankulova, K.; White, P.J. Mechanical transmission of lumpy skin disease virus by Stomoxys spp. (Stomoxys calsitrans, Stomoxys sitiens, Stomoxys indica), Diptera: Muscidae. Animals 2020, 10, 477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chihota, C.M.; Rennie, L.F.; Kitching, R.P.; Mellor, P.S. Mechanical transmission of lumpy skin disease virus by Aedes aegypti (Diptera: Culicidae). Epidemiol. Infect. 2001, 126, 317–321. [Google Scholar] [CrossRef] [Green Version]
- Tuppurainen, E.; Alexandrov, T.; Beltrán-Alcrudo, D. Lumpy skin disease field manual—A manual for veterinarians. In FAO Animal Production and Health Manual; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2017; Volume 20, p. 60. ISBN 978-92-5-109776-2. [Google Scholar]
- World Organization for Animal Health (OIE). Terrestrial Animal Health Code, Chapter 11.9: Infection with Lumpy Skin Disease. 2021. Available online: https://www.oie.int/fileadmin/Home/eng/Health_standards/tahc/current/chapitre_lsd.pdf (accessed on 17 October 2021).
- Moller, J.; Moritz, T.; Schlottau, K.; Krstevski, K.; Hoffmann, D.; Beer, M.; Hoffmann, B. Experimental lumpy skin disease virus infection of cattle: Comparison of a field strain and a vaccine strain. Arch. Virol. 2019, 164, 2931–2941. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Health Status | Food Intake | Nasal Discharge | Number of Noduli | Dissemination of Noduli | |||||
|---|---|---|---|---|---|---|---|---|---|
| Normal | 0 | Normal | 0 | Normal | 0 | No noduli | 0 | No Noduli | 0 |
| Mild Illness | 1 | Slightly Decreased | 0.5 | Mild | 1 | <10 | 1 | Localized | 1 |
| Severe Illness | 2 | Decreased | 1 | Marked Mucous | 2 | >10 | 2 | Generalized | 2 |
| Does Not Eat | 1.5 | Purulent | 3 | ||||||
| Sample | Blood | Skin Biopsies of Normal Skin (No Lesions or Nodules). | Ear Notch | |||||
|---|---|---|---|---|---|---|---|---|
| Area | Vena jugularis | Neck Area | Back Area | Ear | ||||
| Experiment (Exp) | Exp1 | Exp2 | Exp1 | Exp2 | Exp1 | Exp2 | Exp1 | Exp2 |
| Clinical LSD, Cpmax at dpi (or Range) | (15–16) dpi | 12 dpi | 21 dpi | 21 dpi | (12–21) dpi | 21 dpi | (12–21) dpi | (12–21) dpi |
| Clinical LSD, Median Cpmax | 27.96 | 27.88 | 33.50 | 30.62 | 33.82 | 32.24 | 27.06 | 29.41 |
| Clinical LSD, Range Cpmax | (26.50–30.13) | (25.72–30.19) | (25.66–36.42) | (29.58–32.25) | (28.64–39.67) | (31.60–32.74) | (17.62–38.17) | (29.12–29.91) |
| Subclinical LSD, Cpmax at dpi | 8 dpi | 8 dpi | 21 dpi | 21 dpi | 16 dpi | 16 dpi | 21 dpi | 21 dpi |
| Subclinical LSD, Cpmax | R04: 37.53 | R07: 36.28 | R04: 36.61 | R07: 33.47 | R04: 39.77 | R07: 35.60 | R04: 28.61 | R07: 37.54 |
| R08: 39.23 | R08: 32.25 | R08: 33.98 | R08: 37.49 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aerts, L.; Haegeman, A.; De Leeuw, I.; Philips, W.; Van Campe, W.; Behaeghel, I.; Mostin, L.; De Clercq, K. Detection of Clinical and Subclinical Lumpy Skin Disease Using Ear Notch Testing and Skin Biopsies. Microorganisms 2021, 9, 2171. https://doi.org/10.3390/microorganisms9102171
Aerts L, Haegeman A, De Leeuw I, Philips W, Van Campe W, Behaeghel I, Mostin L, De Clercq K. Detection of Clinical and Subclinical Lumpy Skin Disease Using Ear Notch Testing and Skin Biopsies. Microorganisms. 2021; 9(10):2171. https://doi.org/10.3390/microorganisms9102171
Chicago/Turabian StyleAerts, Laetitia, Andy Haegeman, Ilse De Leeuw, Wannes Philips, Willem Van Campe, Isabelle Behaeghel, Laurent Mostin, and Kris De Clercq. 2021. "Detection of Clinical and Subclinical Lumpy Skin Disease Using Ear Notch Testing and Skin Biopsies" Microorganisms 9, no. 10: 2171. https://doi.org/10.3390/microorganisms9102171
APA StyleAerts, L., Haegeman, A., De Leeuw, I., Philips, W., Van Campe, W., Behaeghel, I., Mostin, L., & De Clercq, K. (2021). Detection of Clinical and Subclinical Lumpy Skin Disease Using Ear Notch Testing and Skin Biopsies. Microorganisms, 9(10), 2171. https://doi.org/10.3390/microorganisms9102171