


Development of Real-Time Kinematic Magnetic Resonance Imaging (kMRI) Techniques for Studying the Kinematics of the Spine and Joints in Dogs—Preliminary Study on Cadavers
 , , , , , ,
, , , , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Instrumentation and Protocol
2.3. Image Analysis
3. Results
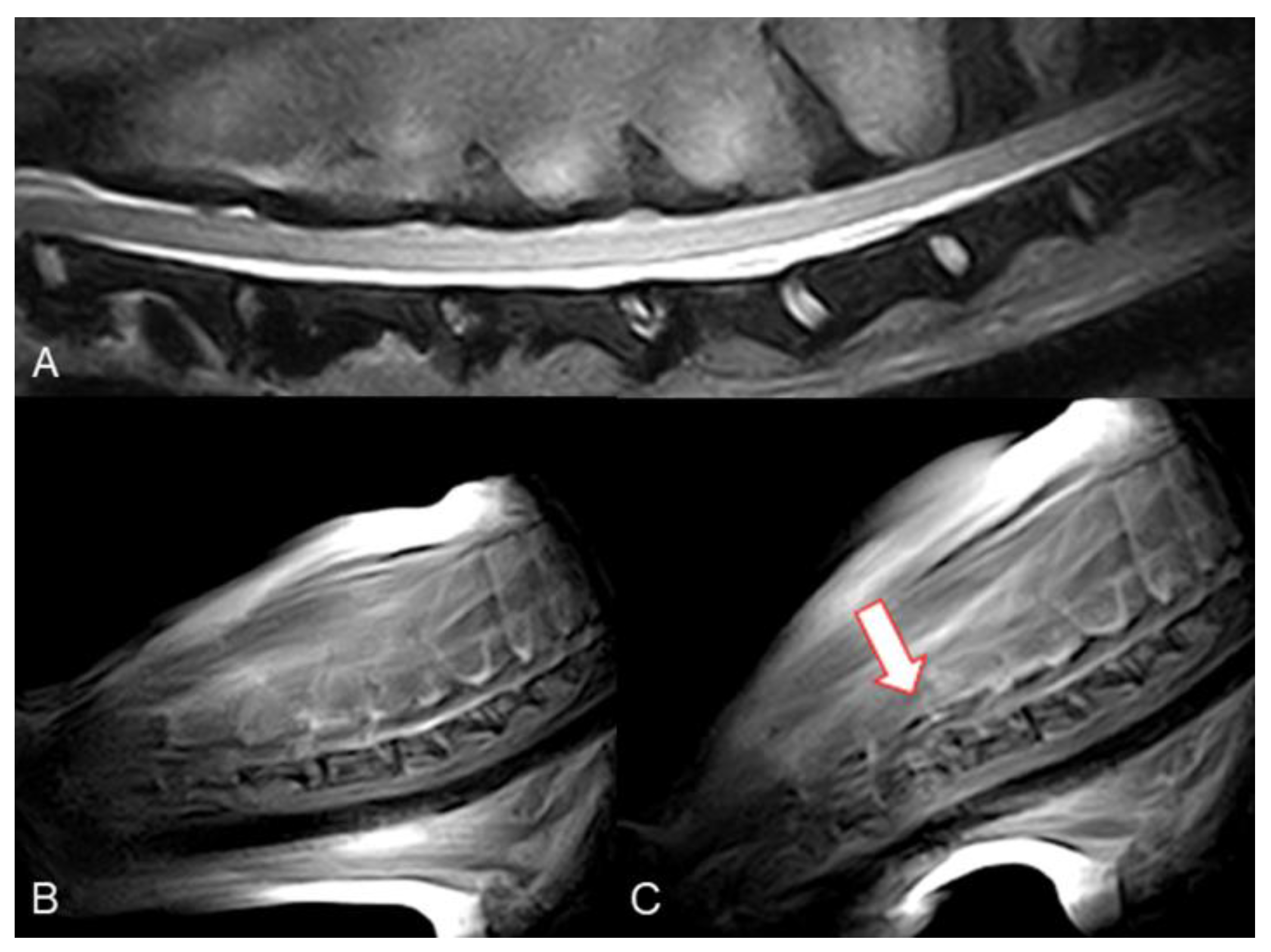
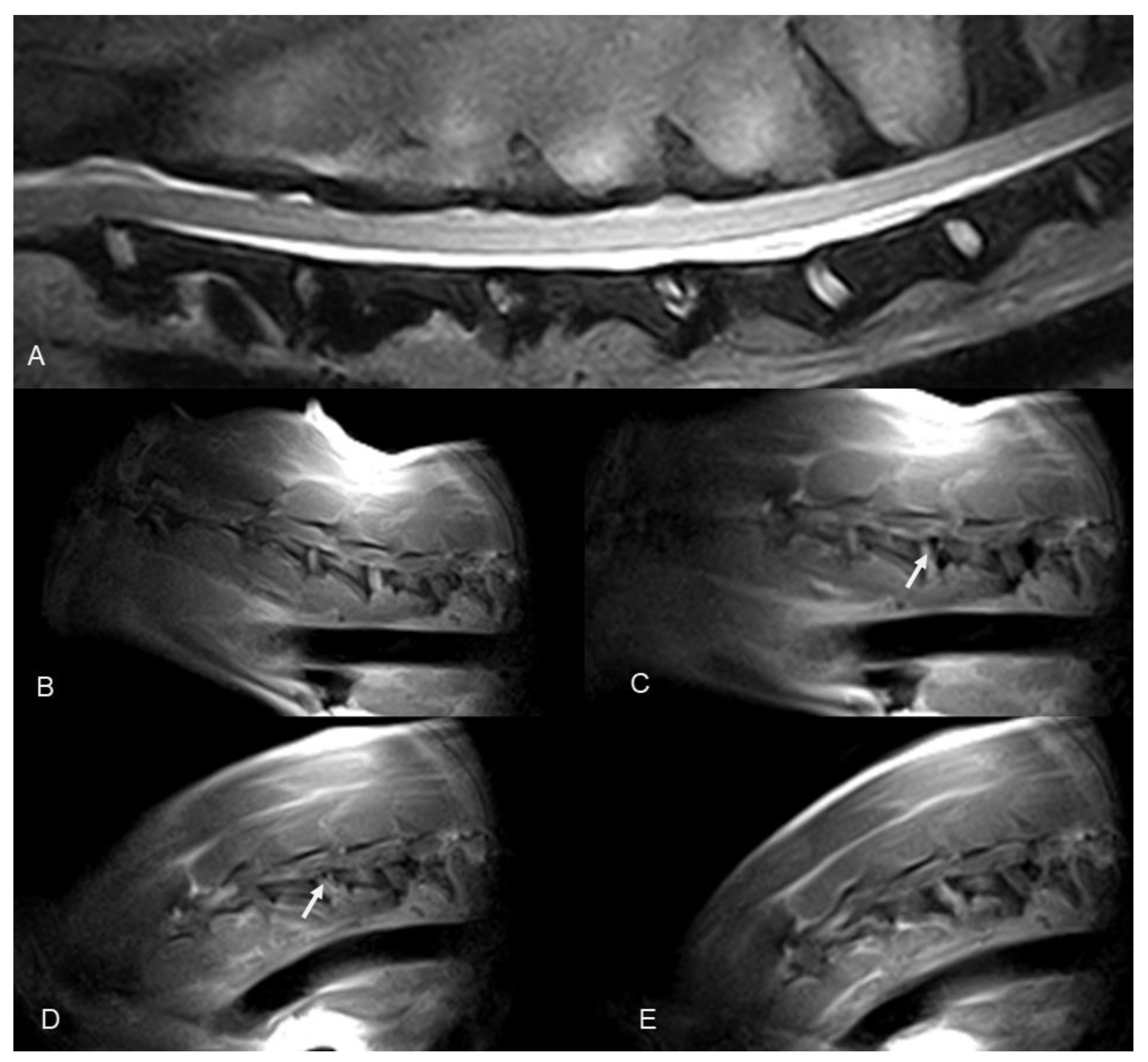
3.1. Cervical Spine kMRI
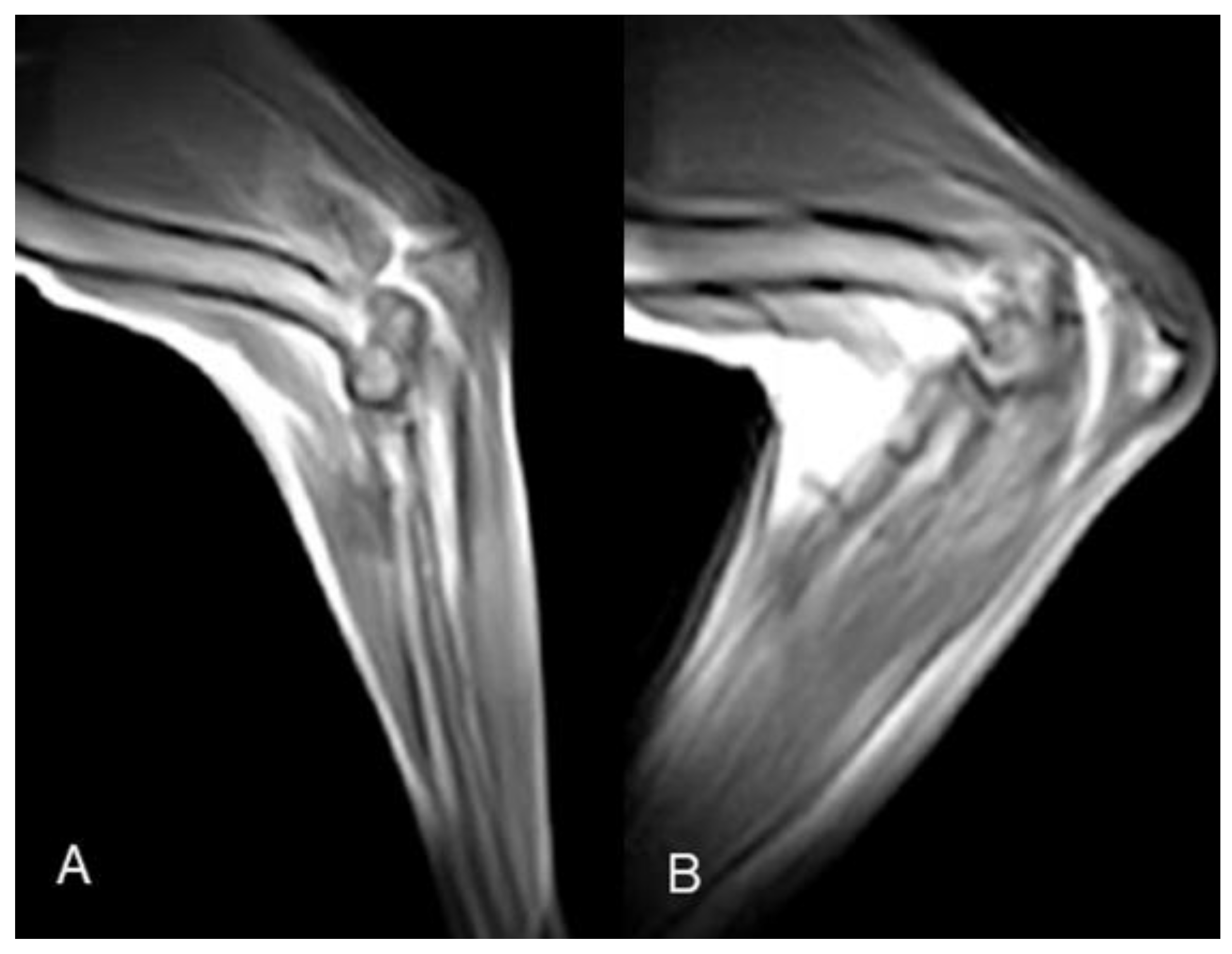
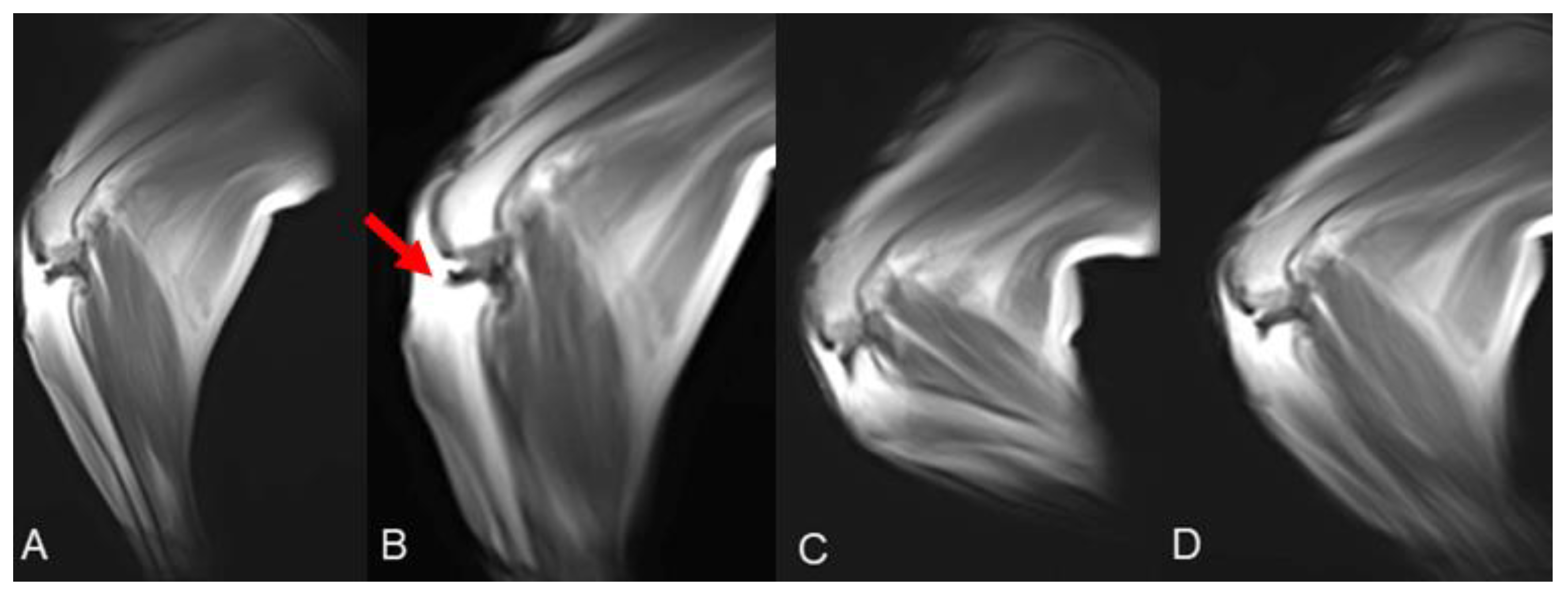
3.2. Elbow kMRI
3.3. Stifle kMRI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Decamp, C.E. Kinetic and kinematic gait analysis and the assessment of lameness in the dog. Vet. Clin. N. Am. Small Anim. Pract. 1997, 27, 825–840. [Google Scholar] [CrossRef]
- Millis, D.; Janas, K. Forelimb Examination, Lameness Assessment, and Kinetic and Kinematic Gait Analysis. Vet. Clin. N. Am. Small Anim. Pract. 2021, 51, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Gavin, P.R.; Holmes, S.P. Orthopedic. In Practical Small Animal MRI; Gavin, P.R., Bagley, R.S., Eds.; Wiley-Blackwell: Ames, IA, USA, 2009; pp. 233–272. [Google Scholar]
- Adamiak, Z.; Jaskólska, M.; Matyjasik, H.; Pomianowski, A.; Kwiatkowska, M. Magnetic resonance imaging of selected limb joints in dogs. Pol. J. Vet. Sci. 2011, 14, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Sage, J.E.; Gavin, P. Musculoskeletal MRI. Vet. Clin. N. Am. Small Anim. Pract. 2016, 46, 421–451. [Google Scholar] [CrossRef]
- Dennis, R. Optimal magnetic resonance imaging of the spine. Vet. Radiol. Ultrasound 2011, 52 (Suppl. S1), S72–S80. [Google Scholar] [CrossRef] [PubMed]
- Robertson, I. Optimal magnetic resonance imaging of the brain. Vet. Radiol. Ultrasound 2011, 52 (Suppl. S1), S15–S22. [Google Scholar] [CrossRef] [PubMed]
- Przeworski, A.; Adamiak, Z.; Głodek, J. Comparison of High-field and Low-field Magnetic Resonance Imaging of Stifle Joint Disorders in Dogs. Pol. J. Vet. Sci. 2016, 19, 663–670. [Google Scholar] [CrossRef] [Green Version]
- Michelini, G.; Corridore, A.; Torlone, S.; Bruno, F.; Marsecano, C.; Capasso, R.; Caranci, F.; Barile, A.; Masciocchi, C.; Splendiani, A. Dynamic MRI in the evaluation of the spine: State of the art. Acta Biomed. 2018, 89 (Suppl. S1), 89–101. [Google Scholar] [PubMed]
- Garetier, M.; Borotikar, B.; Makki, K.; Brochard, S.; Rousseau, F.; Ben Salem, D. Dynamic MRI for articulating joint evaluation on 1.5 T and 3.0 T scanners: Setup, protocols, and real-time sequences. Insights Imaging 2020, 11, 66. [Google Scholar] [CrossRef]
- Tremolada, G.; Winter, M.D.; Kim, S.E.; Spreng, D.; Pozzi, A. Validation of stress magnetic resonance imaging of the canine stifle joint with and without an intact cranial cruciate ligament. Am. J. Vet. Res. 2014, 75, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Provencher, M.; Habing, A.; Moore, S.A.; Cook, L.; Phillips, G.; da Costa, R.C. Kinematic Magnetic Resonance Imaging for Evaluation of Disc-Associated Cervical Spondylomyelopathy in Doberman Pinschers. J Vet. Intern. Med. 2016, 30, 1121–1128. [Google Scholar] [CrossRef]
- De Decker, S.; Watts, V.; Neilson, D.M. Dynamic Lumbosacral Magnetic Resonance Imaging in a Dog with Tethered Cord Syndrome with a Tight Filum Terminale. Front. Vet. Sci. 2017, 4, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Provencher, M.; Habing, A.; Moore, S.A.; Cook, L.; Phillips, G.; da Costa, R.C. Evaluation of osseous-associated cervical spondylomyelopathy in dogs using kinematic magnetic resonance imaging. Vet. Radiol. Ultrasound 2017, 58, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Zindl, C.; Tucker, R.L.; Jovanovik, J.; Gomez Alvarez, C.; Price, D.; Fitzpatrick, N. Effects Of Image Plane, Patient Positioning, And Foraminal Zone On Magnetic Resonance Imaging Measurements Of Canine Lumbosacral Intervertebral Foramina. Vet. Radiol. Ultrasound 2017, 58, 206–215. [Google Scholar] [CrossRef]
- Lampe, R.; Foss, K.D.; Hague, D.W.; Oliveira, C.R.; Smith, R. Dynamic MRI is reliable for evaluation of the lumbosacral spine in healthy dogs. Vet. Radiol. Ultrasound 2020, 61, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.; Kang, K.; Kim, K.; Choi, J.; Choi, M.; Yoon, J. Translocation of the conus medullaris during dynamic lumbosacral magnetic resonance imaging in dogs. Am. J. Vet. Res. 2021, 82, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Quick, H.H.; Ladd, M.E.; Hoevel, M.; Bosk, S.; Debatin, J.F.; Laub, G.; Schroeder, T. Real-time MRI of joint movement with trueFISP. J. Magn. Reson. Imaging 2002, 15, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Walter, W.R.; Burke, C.J. Editorial Commentary: Real-Time Dynamic Magnetic Resonance Imaging of the Patellofemoral Joint: Ready for Prime Time? Arthroscopy 2022, 38, 1581–1583. [Google Scholar] [CrossRef] [PubMed]
- Greene, E.; Rendahl, A.; Goldschmidt, S. The anatomical relationship between the mandibular first molar roots and the mandibular canal based on breed size and skull type. Front. Vet. Sci. 2022, 9, 956976. [Google Scholar] [CrossRef] [PubMed]
- Sharp, N.J.; Wheeler, S.J. Cervical disc disease. In Small Animal Spinal Disorders: Diagnosis and Surgery, 2nd ed.; Sharp, N.J., Wheeler, S.J., Eds.; Elsevier Mosby: Philadelphia, PA, USA, 2005; pp. 93–120. [Google Scholar]
- Fitzpatrick, N.; Smith, T.J.; Evans, R.B.; O’Riordan, J.; Yeadon, R. Subtotal Coronoid Ostectomy for Treatment of Medial Coronoid Disease in 263 Dogs. Vet. Surg. 2009, 38, 233–245. [Google Scholar] [CrossRef]
- Piermattei, D.L.; Johnson, K.A. Approach to the stifle joint through medial incision. In An Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat; Piermattei, D.L., Johnson, K.A., Eds.; Saunders: Philadelphia, PA, USA, 2004; pp. 346–349. [Google Scholar]
- Shapiro, L.M.; Gold, G.E. MRI of weight bearing and movement. Osteoarthr. Cartil. 2012, 20, 69–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, W.R.; Alizai, H.; Bruno, M.; Portugal, S.; Burke, C.J. Real-time dynamic 3-T MRI assessment of spine kinematics: A feasibility study utilizing three different fast pulse sequences. Acta Radiol. 2021, 62, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Frings, J.; Dust, T.; Krause, M.; Frosch, K.H.; Adam, G.; Warncke, M.; Welsch, G.; Henes, F.O.; Maas, K.J. Dynamic Mediolateral Patellar Translation Is a Sex- and Size-Independent Parameter of Adult Proximal Patellar Tracking Using Dynamic 3 Tesla Magnetic Resonance Imaging. Arthroscopy 2022, 38, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- d’Entremont, A.G.; Nordmeyer-Massner, J.A.; Bos, C.; Wilson, D.R.; Pruessmann, K.P. Do dynamic-based MR knee kinematics methods produce the same results as static methods? Magn. Reson. Med. 2013, 69, 1634–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerigk, L.; Bostel, T.; Hegewald, A.; Thomé, C.; Scharf, J.; Groden, C.; Neumaier-Probst, E. Dynamic magnetic resonance imaging of the cervical spine with high-resolution 3-dimensional T2-imaging. Clin. Neuroradiol. 2012, 22, 93–99. [Google Scholar] [CrossRef]
- Franklin, S.P.; Burke, E.E.; Holmes, S.P. Utility of MRI for Characterizing Articular Cartilage Pathology in Dogs with Medial Coronoid Process Disease. Front. Vet. Sci. 2017, 4, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, P.; Pfeil, A.; Ludewig, E.; Böttcher, P.; Oechtering, G. Magnetic resonance imaging diagnosis: Incomplete ossification of the humeral condyle in a German shepherd dog. J. Small Anim. Pract. 2009, 50, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Piola, V.; Posch, B.; Radke, H.; Telintelo, G.; Herrtage, M.E. Magnetic resonance imaging features of canine incomplete humeral condyle ossification. Vet. Radiol. Ultrasound 2012, 53, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Reichle, J.K.; Snaps, F. The elbow. Clin. Tech. Small. Anim. Pract. 1999, 14, 177–186. [Google Scholar] [CrossRef]
- Cook, C.R.; Cook, J.L. Diagnostic imaging of canine elbow dysplasia: A review. Vet. Surg. 2009, 38, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Zalcman, A.R.; Cook, C.; Mai, W. General Features and Optimized Technique for the Musculoskeletal System. In Diagnostic MRI in Dogs and Cats; Mai, W., Ed.; CRC Press: Boca Raton, FL, USA, 2018; pp. 130–152. [Google Scholar]
- Tempelaere, C.; Pierrart, J.; Lefèvre-Colau, M.M.; Vuillemin, V.; Cuénod, C.A.; Hansen, U.; Mir, O.; Skalli, W.; Gregory, T. Dynamic Three-Dimensional Shoulder Mri during Active Motion for Investigation of Rotator Cuff Diseases. PLoS ONE 2016, 11, e0158563. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Breed | Sex 1 | Age 2 | Breed Size |
|---|---|---|---|---|
| Case 1 | Weimaraner | ME | 9 | Large |
| Case 2 | Mongrel | ME | 12 | Extra small |
| Case 3 | French Bulldog | FE | 11 | Small |
| Case 4 | Mongrel | ME | 7 | Large |
| Case 5 | Rottweiler | FE | 6 | Giant |
| Case 6 | Pitbull | ME | 8 | Medium |
| Case 7 | Dobermann Pinscher | ME | 8 | Large |
| Case | Cervical Spine | Elbow 1 | Stifle 2 |
|---|---|---|---|
| Case 1 | fair | N.A. | N.A. |
| Case 2 | fair | N.A. | N.A. |
| Case 3 | fair | N.A. | N.A. |
| Case 4 | fair | N.A. | N.A. |
| Case 5 | good | unacceptable (RE) unacceptable (LE) | N.A. |
| Case 6 | good | good (RE) | excellent (RS) excellent (LS) |
| Case 7 | good | N.A. | excellent (RS) excellent (LS) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canal, S.; Tamburro, R.; Falerno, I.; Signore, F.D.; Simeoni, F.; De Pasquale, F.; De Bonis, A.; Maraone, A.; Paolini, A.; Bianchi, A.; et al. Development of Real-Time Kinematic Magnetic Resonance Imaging (kMRI) Techniques for Studying the Kinematics of the Spine and Joints in Dogs—Preliminary Study on Cadavers. Animals 2022, 12, 2790. https://doi.org/10.3390/ani12202790
Canal S, Tamburro R, Falerno I, Signore FD, Simeoni F, De Pasquale F, De Bonis A, Maraone A, Paolini A, Bianchi A, et al. Development of Real-Time Kinematic Magnetic Resonance Imaging (kMRI) Techniques for Studying the Kinematics of the Spine and Joints in Dogs—Preliminary Study on Cadavers. Animals. 2022; 12(20):2790. https://doi.org/10.3390/ani12202790
Chicago/Turabian StyleCanal, Sara, Roberto Tamburro, Ilaria Falerno, Francesca Del Signore, Francesco Simeoni, Francesco De Pasquale, Andrea De Bonis, Annamaria Maraone, Andrea Paolini, Amanda Bianchi, and et al. 2022. "Development of Real-Time Kinematic Magnetic Resonance Imaging (kMRI) Techniques for Studying the Kinematics of the Spine and Joints in Dogs—Preliminary Study on Cadavers" Animals 12, no. 20: 2790. https://doi.org/10.3390/ani12202790
APA StyleCanal, S., Tamburro, R., Falerno, I., Signore, F. D., Simeoni, F., De Pasquale, F., De Bonis, A., Maraone, A., Paolini, A., Bianchi, A., Rosto, M., & Vignoli, M. (2022). Development of Real-Time Kinematic Magnetic Resonance Imaging (kMRI) Techniques for Studying the Kinematics of the Spine and Joints in Dogs—Preliminary Study on Cadavers. Animals, 12(20), 2790. https://doi.org/10.3390/ani12202790