


Diagnosis of Canine Tumours and the Value of Combined Detection of VEGF, P53, SF and NLRP3 for the Early Diagnosis of Canine Mammary Carcinoma

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals and Sampling
2.2. Clinical Tumor Examinations
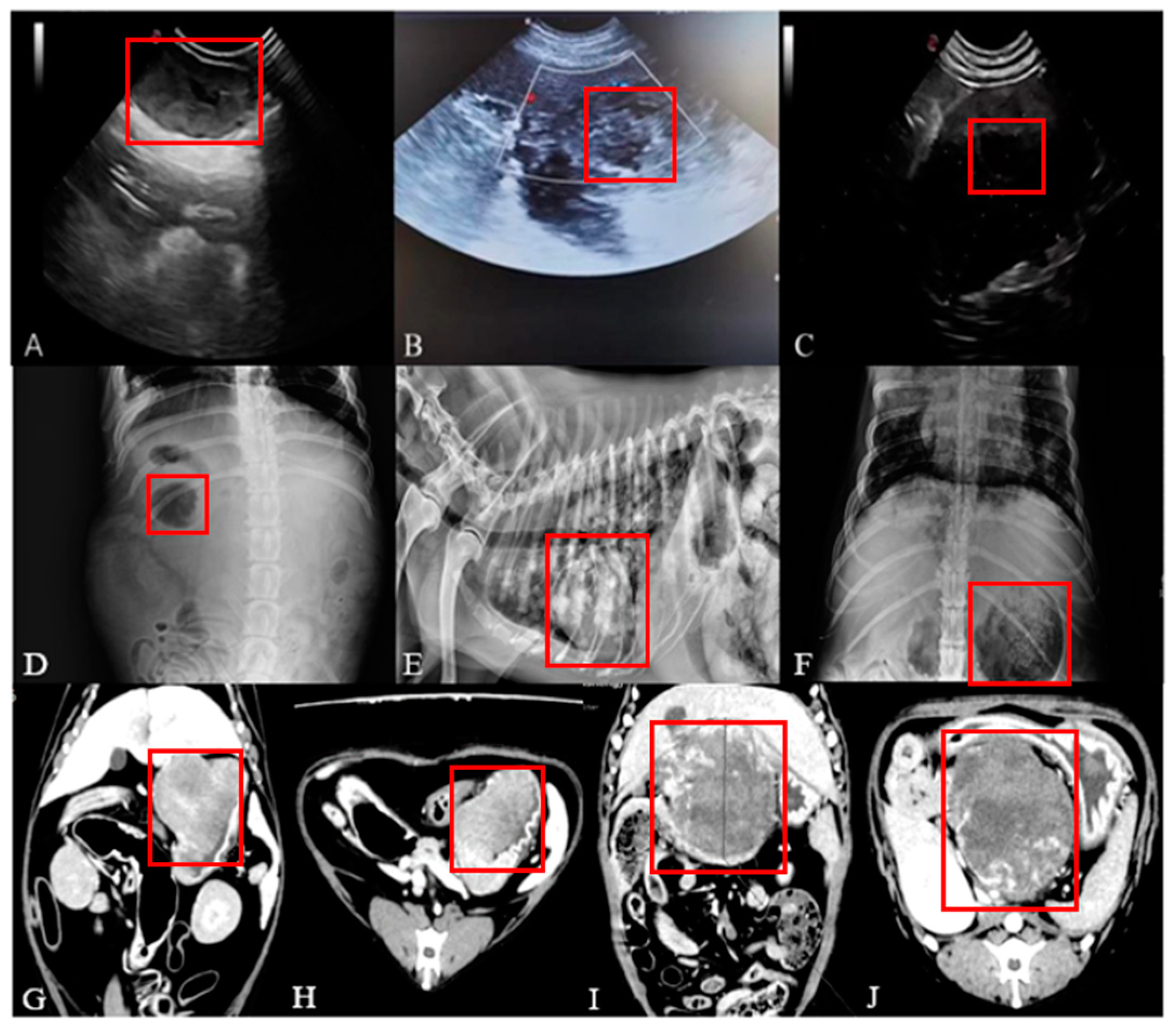
2.3. Imaging Examination
2.4. Haematology Examination
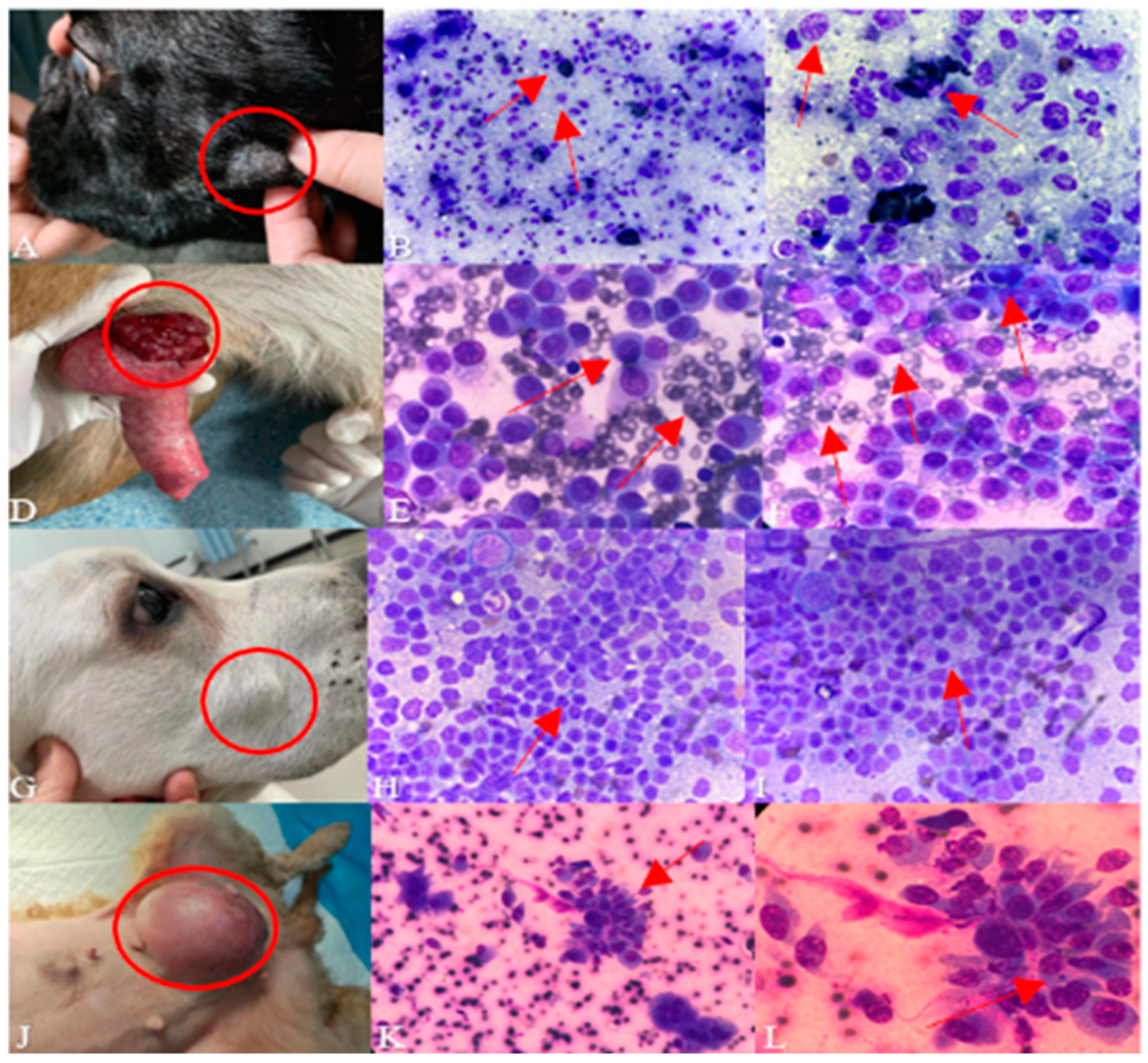
2.5. Cytological Examination
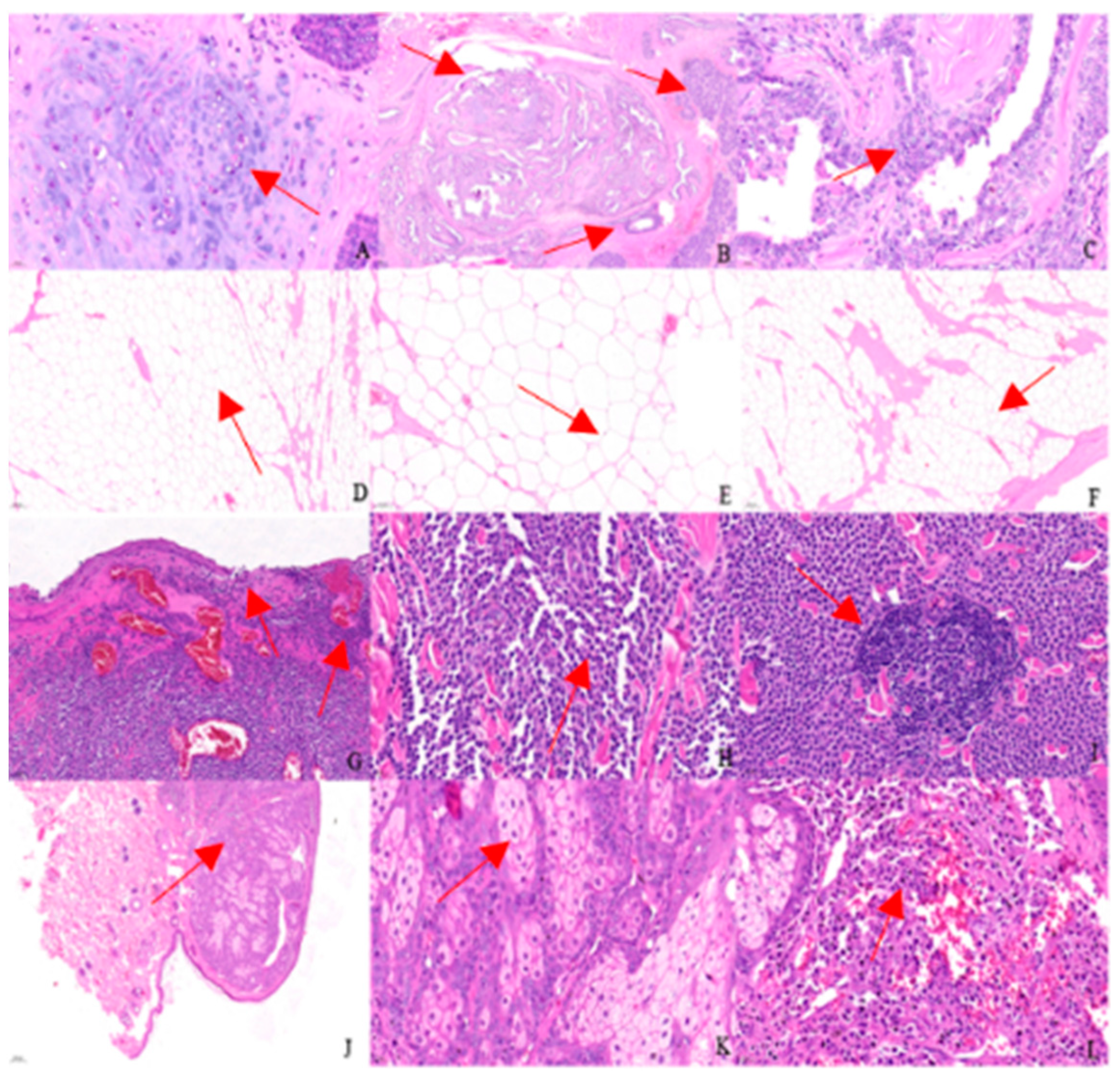
2.6. Pathology Examination
2.7. Molecular Biological Detection
2.7.1. Primer Design
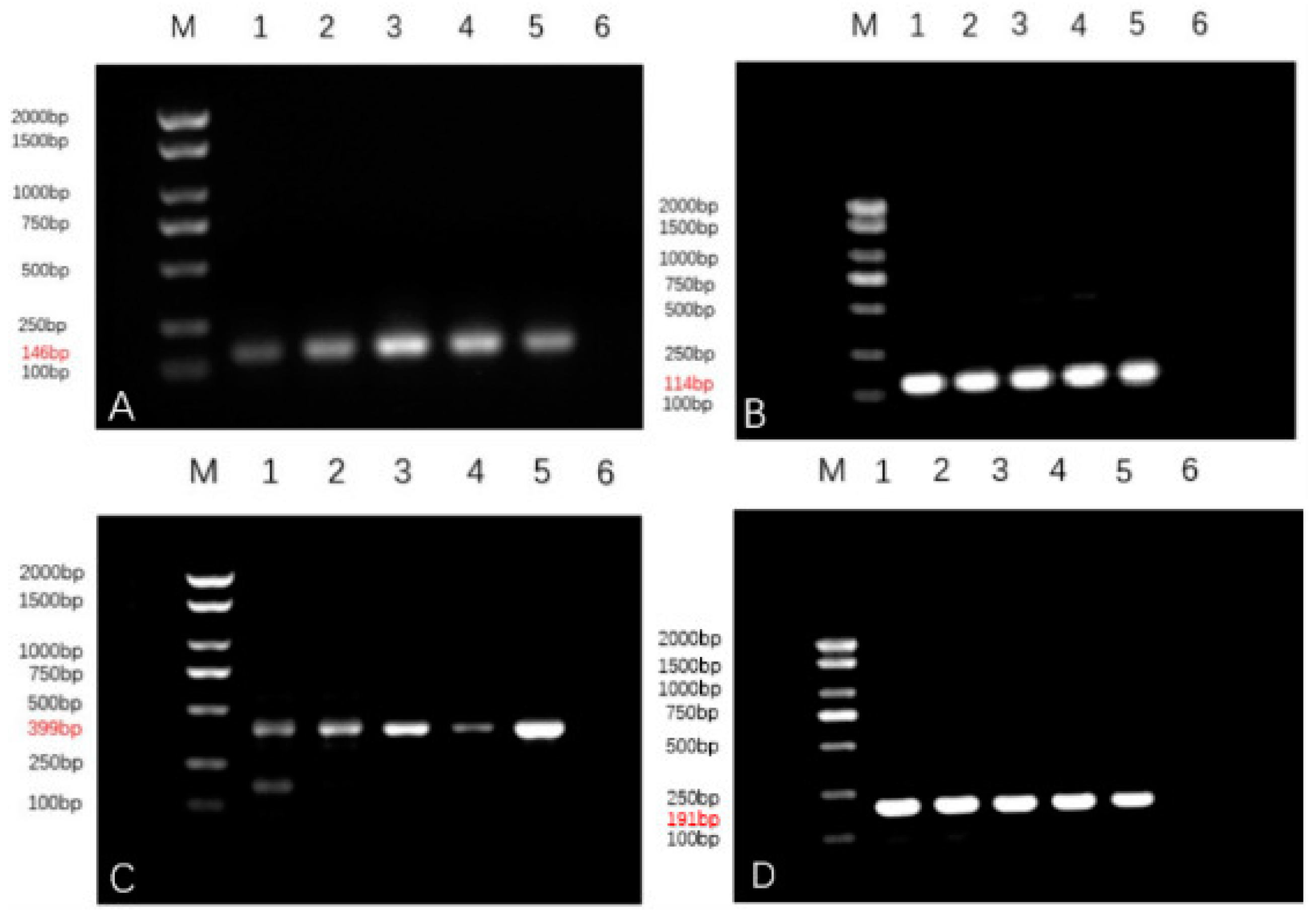
2.7.2. Agarose Gel Electrophoresis
2.7.3. Real-Time PCR
2.7.4. ELISA
3. Results
3.1. Clinical Tumor Examinations
3.2. Imaging Examination
3.3. Haematology Examination
3.4. Cytological Examination
3.5. Pathology Examination
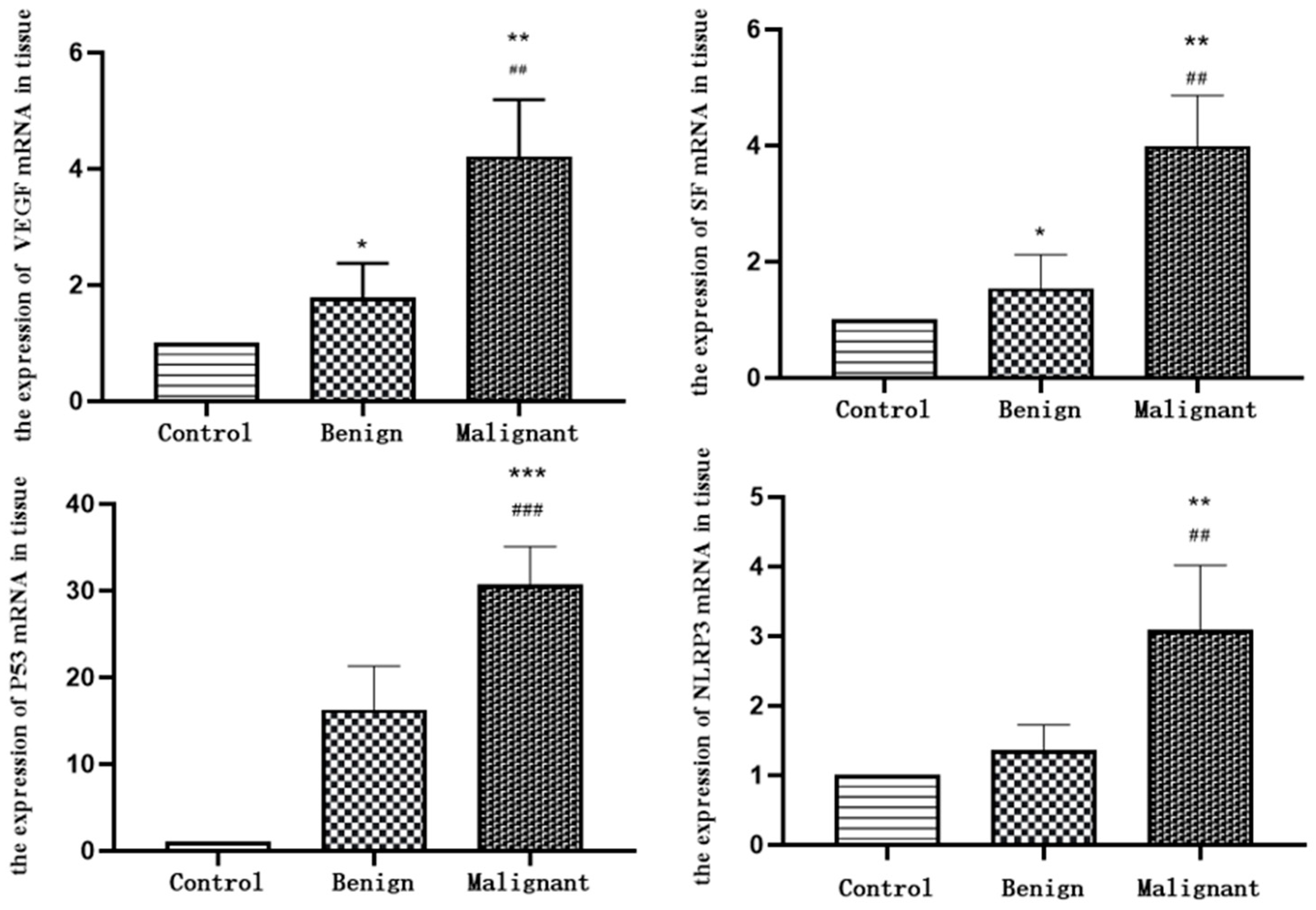
3.6. The Expression of VEGF, SF, P53 and NLRP3 in Tissues
3.6.1. VEGF, SF, P53, NLRP3 Agarose Gel Electropherograms
3.6.2. RT-qPCR Results
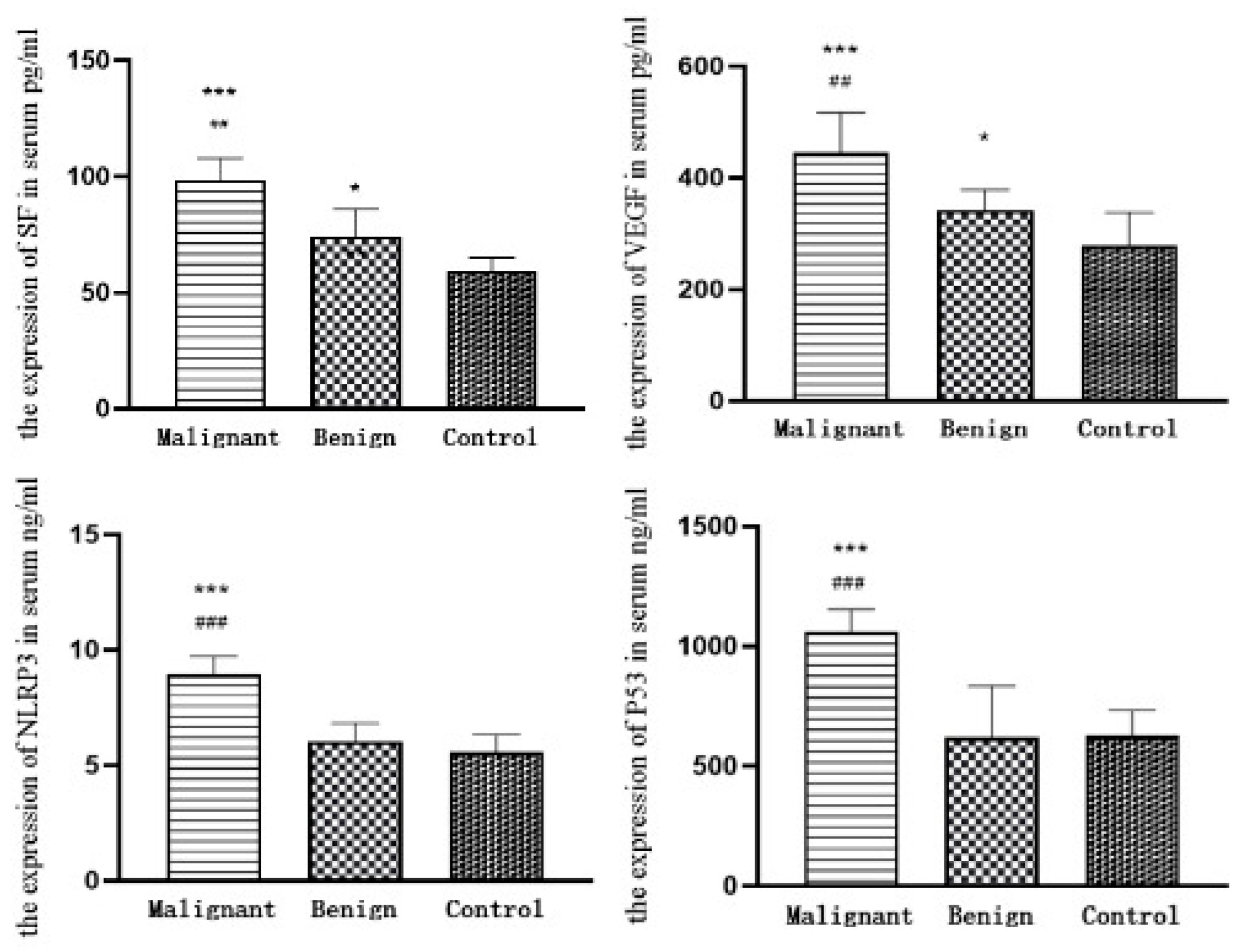
3.7. The Expression of VEGF, SF, P53 and NLRP3 in Sera
3.7.1. ELISA Results
3.7.2. Assessment of the Value of VEGF, SF, P53, and NLRP3 as Individual Tests for Canine Mammary Carcinoma
3.7.3. Comparison of the Value of Combined VEGF, SF, P53 and NLRP3 Assays for the Assessment of Canine Mammary Carcinoma
3.7.4. Area under the Curve for VEGF, SF, P53, and NLRP3 Alone and in Combination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldschmidt, M.; Peña, L.; Rasotto, R.; Zappulli, V. Classification and grading of canine mammary tumors. Vet. Pathol. 2011, 48, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Camus, M.S.; Priest, H.L.; Koehler, J.W.; Driskell, E.A.; Rakich, P.M.; Ilha, M.R.; Krimer, P.M. Cytologic Criteria for Mast Cell Tumor Grading in Dogs With Evaluation of Clinical Outcome. Vet. Pathol. 2016, 53, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Kiupel, M.; Camus, M. Diagnosis and Prognosis of Canine Cutaneous Mast Cell Tumors. Vet. Clin. N. Am. Small Anim. Pract. 2019, 49, 819–836. [Google Scholar] [CrossRef] [PubMed]
- Sauerbrei, W.; Taube, S.E.; McShane, L.M.; Cavenagh, M.M.; Altman, D.G. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): An Abridged Explanation and Elaboration. J. Natl. Cancer Inst. 2018, 110, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Rye, P.D.; Nustad, K.; Stigbrand, T. Tumor marker workshops. Tumour Biol. 2003, 24, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Faria, S.S.; Costantini, S.; de Lima, V.C.C.; de Andrade, V.P.; Rialland, M.; Cedric, R.; Budillon, A.; Magalhães, K.G. NLRP3 inflammasome-mediated cytokine production and pyroptosis cell death in breast cancer. J. Biomed. Sci. 2021, 28, 26. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Mu, K.; Li, T.; Zhang, Y.; Yang, Z.; Jia, X.; Zhao, W.; Huai, W.; Guo, P.; Han, L. Deregulation of the NLRP3 inflammasome in hepatic parenchymal cells during liver cancer progression. Lab. Investig. 2014, 94, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Chen, H.; Wang, S.; Wei, H.; Wang, X.; Shen, R.; Wang, Y.; Lin, R.; Lin, J. NLRP3 Overexpression Associated With Poor Prognosis and Presented as an Effective Therapeutic Target in Osteosarcoma. Front. Pharmacol. 2021, 12, 724923. [Google Scholar] [CrossRef] [PubMed]
- Haga, S.; Nakayama, M.; Tatsumi, K.; Maeda, M.; Imai, S.; Umesako, S.; Yamamoto, H.; Hilgers, J.; Sarkar, N.H. Overexpression of the p53 gene product in canine mammary tumors. Oncol. Rep. 2001, 8, 1215–1219. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.Y.; Zheng, H.H.; Yu, C.; Ye, Y.; Du, C.T.; Xie, G.H. Research progress of good markers for canine mammary carcinoma. Mol. Biol. Rep. 2023, 50, 10617–10625. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, T.F.; Maués, T.; Ramundo, M.S.; Figueiredo, A.M.S.; de Mello, M.F.V.; El-Jaick, K.B.; Ferreira, M.L.G.; Ferreira, A.M.R. TP53 gene expression levels and tumor aggressiveness in canine mammary carcinomas. J. Vet. Diagn. Investig. 2017, 29, 865–868. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Walia, V.; Ray, M.; Elble, R.C. p53 in breast cancer: Mutation and countermeasures. Front. Biosci. 2007, 12, 4168–4178. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Kweon, O.K. Mutations of p53 tumor suppressor gene in spontaneous canine mammary tumors. J. Vet. Sci. 2002, 3, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, M.I.; Silva-Carvalho, R.; Pires, I.; Prada, J.; Bianchini, R.; Jensen-Jarolim, E.; Queiroga, F.L. A Comparative Approach of Tumor-Associated Inflammation in Mammary Cancer between Humans and Dogs. Biomed. Res. Int. 2016, 2016, 4917387. [Google Scholar] [CrossRef] [PubMed]
- Millanta, F.; Caneschi, V.; Ressel, L.; Citi, S.; Poli, A. Expression of vascular endothelial growth factor in canine inflammatory and non-inflammatory mammary carcinoma. J. Comp. Pathol. 2010, 142, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.A.; Oliveira, J.T.; Lopes, C.C.; Amorim, I.F.; Vicente, C.M.; Gärtner, F.R.; Matos, A.J. Immunohistochemical expression of vascular endothelial growth factor in canine mammary tumours. J. Comp. Pathol. 2010, 143, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Sleeckx, N.; Van Brantegem, L.; Van den Eynden, G.; Fransen, E.; Casteleyn, C.; Van Cruchten, S.; Veldhuis Kroeze, E.; Van Ginneken, C. Angiogenesis in canine mammary tumours: A morphometric and prognostic study. J. Comp. Pathol. 2014, 150, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Restucci, B.; Papparella, S.; Maiolino, P.; De Vico, G. Expression of vascular endothelial growth factor in canine mammary tumors. Vet. Pathol. 2002, 39, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, P.A.B.; Giuliano, A.; Bęczkowski, P.M.; Horta, R.D.S. Molecular Profile of Canine Hemangiosarcoma and Potential Novel Therapeutic Targets. Vet. Sci. 2023, 10, 387. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Ren, X.; Liu, X.; Shi, D.; Xu, E.; Wang, S.; Liu, Y. Combined detection of CA15-3, CEA, and SF in serum and tissue of canine mammary gland tumor patients. Sci. Rep. 2021, 11, 6651. [Google Scholar] [CrossRef] [PubMed]
- Kukulj, S.; Jaganjac, M.; Boranic, M.; Krizanac, S.; Santic, Z.; Poljak-Blazi, M. Altered iron metabolism, inflammation, transferrin receptors, and ferritin expression in non-small-cell lung cancer. Med. Oncol. 2010, 27, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Zheng, H.; Liu, X.; Xie, G. The Analysis of E-Cadherin, N-Cadherin, Vimentin, HER-2, CEA, CA15-3 and SF Expression in the Diagnosis of Canine Mammary Tumors. Animals 2022, 12, 3050. [Google Scholar] [CrossRef] [PubMed]
- Fredenberg, E.; Willsher, P.; Moa, E.; Dance, D.R.; Young, K.C.; Wallis, M.G. Measurement of breast-tissue x-ray attenuation by spectral imaging: Fresh and fixed normal and malignant tissue. Phys. Med. Biol. 2018, 63, 235003. [Google Scholar] [CrossRef] [PubMed]
- Filippou, A.; Damianou, C. Ultrasonic attenuation of canine mammary tumours. Ultrasonics 2022, 125, 106798. [Google Scholar] [CrossRef] [PubMed]
- von Stade, L.; Randall, E.K.; Rao, S.; Marolf, A.J. CT imaging features of canine thymomas. Vet. Radiol. Ultrasound 2019, 60, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Illei, P.B.; Shyu, S. Fine needle aspiration of thymic epithelial neoplasms and non-neoplastic lesions. Semin. Diagn. Pathol. 2020, 37, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.H.; Du, C.T.; Yu, C.; Zhang, Y.Z.; Huang, R.L.; Tang, X.Y.; Xie, G.H. Epidemiological Investigation of Canine Mammary Tumors in Mainland China Between 2017 and 2021. Front. Vet. Sci. 2022, 9, 843390. [Google Scholar] [CrossRef]
- McShane, L.M.; Hayes, D.F. Publication of tumor marker research results: The necessity for complete and transparent reporting. J. Clin. Oncol. 2012, 30, 4223–4232. [Google Scholar] [CrossRef] [PubMed]
- Anadol, E.; Yar Saglam, A.S.; Gultiken, N.; Karakas, K.; Alcigir, E.; Alkan, H.; Kanca, H. Expression of iNOS, COX-2 and VEGF in canine mammary tumours and non-neoplastic mammary glands: Association with clinicopathological features and tumour grade. Acta Vet. Hung. 2017, 65, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Al-Dissi, A.N.; Haines, D.M.; Singh, B.; Kidney, B.A. Immunohistochemical expression of vascular endothelial growth factor and vascular endothelial growth factor receptor-2 in canine simple mammary gland adenocarcinomas. Can. Vet. J. 2010, 51, 1109–1114. [Google Scholar]
- Shao, B.Z.; Xu, Z.Q.; Han, B.Z.; Su, D.F.; Liu, C. NLRP3 inflammasome and its inhibitors: A review. Front. Pharmacol. 2015, 6, 262. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Knovich, M.A.; Coffman, L.G.; Torti, F.M.; Torti, S.V. Serum ferritin: Past, present and future. Biochim. Biophys. Acta 2010, 1800, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Demir, H.; Beypinar, I.; Urvay, S.; Davarcı, S.E.; Baykara, M. Prognostic role of pre-operative serum ferritin level in stage 2 colon cancer. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6473–6479. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Liu, J.; Xu, D.; Zhang, T.; Hu, W.; Feng, Z. Gain-of-function mutant p53 in cancer progression and therapy. J. Mol. Cell Biol. 2020, 12, 674–687. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, F.; Collavin, L.; Del Sal, G. Mutant p53 as a guardian of the cancer cell. Cell Death Differ. 2019, 26, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.; Gama, A.; Seixas, F.; Faustino-Rocha, A.I.; Lopes, C.; Gaspar, V.M.; Mano, J.F.; Medeiros, R.; Oliveira, P.A. Mammary Glands of Women, Female Dogs and Female Rats: Similarities and Differences to Be Considered in Breast Cancer Research. Vet. Sci. 2023, 10, 379. [Google Scholar] [CrossRef] [PubMed]
- Amirkhani Namagerdi, A.; d’Angelo, D.; Ciani, F.; Iannuzzi, C.A.; Napolitano, F.; Avallone, L.; De Laurentiis, M.; Giordano, A. Triple-Negative Breast Cancer Comparison With Canine Mammary Tumors From Light Microscopy to Molecular Pathology. Front. Oncol. 2020, 10, 563779. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of Primer | Expected Product/Bp | Sequence (5′–3′) | |
|---|---|---|---|
| SF | 146 | Sense | GATGCTGCTTCTGGTATGTCCTATCTC |
| Anti-sense | GAATACACTCCACCATCCTCTTGACG | ||
| VEGF | 399 | Sense | CAGGCGTATGCAGGCAAAGA |
| Anti-sense | GAGGTGGCTTGTGCTGGTGT | ||
| P53 | 191 | Sense | GACACAGTGTGGTGGTGCCTTA |
| Anti-sense | GGCACAAACGCGTACCTCAA | ||
| NLRP3 | 114 | Sense | GCAACAGTGTGAGGTGAGGCTAC |
| Anti-sense | TGCAATGCTCTTGGAGACACAGG | ||
| Group | Canine Number | Mean Age | Tumor Size (Mean ± SD) | Sex | Mammary Gland | Mental State |
|---|---|---|---|---|---|---|
| Healthy dogs | 30 | 4.5 | 0 | female | Smooth | Normal |
| Benign tumor dogs | 179 | 6.7 | 1.56 ± 0.48 | female | Protrusion | Normal |
| Malignant tumor dogs | 269 | 8.9 | 1.82 ± 0.24 | female | Redness, swelling, rupture | Bad |
| Parameters | Unit | Min–Max | Value |
|---|---|---|---|
| White blood cells (WBC) | 109/L | 6–17 | 12.51 |
| Neutrophil percentage (NE%) | % | 52.0–81 | 72.3 |
| Lymphocyte percentage (Lym%) | % | 12–33 | 16.4 |
| Monocyte percentage (Mon%) | % | 2.0–13 | 7.8 |
| Eosinophil percentage (Eos%) | % | 1.0–4.0 | 3.4 |
| Basophil percentage (Bas%) | % | 0–1.3 | 0.1 |
| Basophil (Bas#) | 109/L | 20–27 | 21.5 |
| Red blood cells (RBC) | 1012/L | 5.1–8.5 | 6.04 |
| Hemoglobin (HGB) | g/L | 85–153 | 130 |
| Red blood cell specific volume (HCT) | % | 26–47 | 37.5 |
| Mean corpuscular volume (MCV) | fL | 60–76 | 62 |
| Mean corpuscular hemoglobin (MCH) | pg | 20–27 | 21.5 |
| Mean corpuscular hemoglobin concentration (MCHC) | g/L | 300–380 | 347 |
| Platelet count (PLT) | 109/L | 117–490 | 636 |
| Neutrophil (NE#) | 109/L | 3.62–13.3 | 9.05 |
| Lymphocyte (Lym#) | 109/L | 0.83–4.91 | 2.06 |
| Monocyte (Mon#) | 109/L | 0.14–1.97 | 0.97 |
| Eosinophil (Eos#) | 109/L | 0.04–1.62 | 0.42 |
| Parameters | Unit | Min-Max | Value |
|---|---|---|---|
| Alanine transaminase (ALT) | U/L | 5-125 | 55 |
| Glutamic acid (GLU) | mmol/L | 3.89-7.94 | 5.38 |
| UREA | mmol/L | 2.5-9.6 | 13.64 |
| Creatinine (CREA) | umol/L | 44-159 | 120.3 |
| Total protein (TP) | g/L | 52-82 | 61.7 |
| BUN/CRE | 16-218 | 113.366 | |
| Albumin (ALB) | g/L | 23-40 | 29.9 |
| Globulin (GLO) | g/L | 25-45 | 31.8 |
| A/G | 0.8-2.0 | 0.94 | |
| Alkaline phosphatase (ALP) | U/L | 23-213 | 411 |
| Group | NLRP3 | P53 | SF | VEGF |
|---|---|---|---|---|
| Control | 1 | 1 | 1 | 1 |
| Benign | 1.358 ± 0.3664 | 16.25 ± 5.023 | 1.541 ± 0.5786 * | 1.783 ± 0.5894 * |
| Malignant | 3.086 ± 0.9313 **## | 38.70 ± 17.04 ***### | 3.989 ± 0.8782 **## | 3.932 ± 1.320 **## |
| Group | SF (ng/mL) | P53 (pg/mL) | VEGF (pg/mL) | NLRP3 (ng/mL) |
|---|---|---|---|---|
| Malignant | 105.39 ± 3.81 ***## | 1027.24 ± 54.29 ***### | 460.31 ± 19.58 ***## | 8.26 ± 0.29 ***### |
| Benign | 88.40 ± 10.11 * | 935.45 ± 25.65 * | 396.54 ± 25.65 * | 7.37 ± 0.47 |
| Control | 56.27 ± 5.72 | 606.82 ± 44.51 | 246.85 ± 44.51 | 5.24 ± 0.51 |
| Marker | Sensitivity (%) | Specificity (%) | Accuracy (%) | Youden Index (%) |
|---|---|---|---|---|
| SF | 56.7 (17/30) | 77.8 (21/27) | 66.7 (38/57) | 0.345 |
| VEGF | 53.3 (16/30) | 85.2 (23/27) | 68.4 (39/57) | 0.385 |
| P53 | 63.3 (19/30) | 81.5 (22/27) | 71.9 (41/57) | 0.448 |
| NLRP3 | 50.0 (15/30) | 70.4 (19/27) | 59.7 (34/57) | 0.204 |
| Marker | Sensitivity (%) | Specificity (%) | Accuracy (%) | Youden Index |
|---|---|---|---|---|
| SF+VEGF | 66.7 (20/30) | 74.1 (20/27) | 70.2 (40/57) | 0.408 |
| SF+P53 | 73.3 (22/30) | 71.9 (19/27) | 72.0 (41/57) | 0.452 |
| SF+NLRP3 | 63.3 (19/30) | 71.9 (19/27) | 66.7 (38/57) | 0.352 |
| VEGF+P53 | 70.0 (21/30) | 77.8 (21/27) | 73.7 (42/57) | 0.478 |
| VEGF+NLRP3 | 73.3 (22/30) | 66.7 (18/27) | 70.2 (40/57) | 0.400 |
| P53+NLRP3 | 80.0 (24/30) | 66.7 (18/27) | 73.7 (42/57) | 0.467 |
| SF+VEGF+P53 | 83.3 (25/30) | 63.0 (17/27) | 73.7 (42/57) | 0.463 |
| SF+VEGF+NLRP3 | 76.7 (23/30) | 62.9 (17/27) | 70.2 (40/57) | 0.396 |
| SF+P53+NLRP3 | 83.3 (25/30) | 59.3 (16/27) | 71.9 (41/57) | 0.426 |
| VEGF+P53+NLRP3 | 86.7 (26/30) | 59.3 (16/27) | 73.7 (42/57) | 0.460 |
| SF+VEGF+P53+NLRP3 | 93.3 (28/30) | 55.6 (15/27) | 75.4 (43/57) | 0.489 |
| Marker | AUC | p | 95%CI |
|---|---|---|---|
| SF | 0.683 | 0.018 | 0.540~0.826 |
| VEGF | 0.736 | 0.002 | 0.608~0.863 |
| P53 | 0.749 | 0.001 | 0.615~0.884 |
| NLRP3 | 0.679 | 0.020 | 0.539~0.819 |
| SF+VEGF | 0.804 | <0.001 | 0.686~0.921 |
| SF+P53 | 0.827 | <0.001 | 0.720~0.934 |
| SF+NLRP3 | 0.772 | <0.001 | 0.649~0.894 |
| VEGF+P53 | 0.807 | <0.001 | 0.697~0.918 |
| VEGF+NLRP3 | 0.789 | <0.001 | 0.672~0.906 |
| P53+NLRP3 | 0.796 | <0.001 | 0.682~0.910 |
| SF+VEGF+P53 | 0.852 | <0.001 | 0.756~0.948 |
| SF+VEGF+NLRP3 | 0.833 | <0.001 | 0.724~0.942 |
| SF+P53+NLRP3 | 0.852 | <0.001 | 0.756~0.947 |
| VEGF+P53+NLRP3 | 0.863 | <0.001 | 0.771~0.955 |
| SF+VEGF+P53+NLRP3 | 0.879 | <0.001 | 0.790~0.968 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, N.-Y.; Zheng, H.-H.; Yu, C.; Ye, Y.; Xie, G.-H. Diagnosis of Canine Tumours and the Value of Combined Detection of VEGF, P53, SF and NLRP3 for the Early Diagnosis of Canine Mammary Carcinoma. Animals 2024, 14, 1272. https://doi.org/10.3390/ani14091272
Yang N-Y, Zheng H-H, Yu C, Ye Y, Xie G-H. Diagnosis of Canine Tumours and the Value of Combined Detection of VEGF, P53, SF and NLRP3 for the Early Diagnosis of Canine Mammary Carcinoma. Animals. 2024; 14(9):1272. https://doi.org/10.3390/ani14091272
Chicago/Turabian StyleYang, Ning-Yu, Hui-Hua Zheng, Chao Yu, Yan Ye, and Guang-Hong Xie. 2024. "Diagnosis of Canine Tumours and the Value of Combined Detection of VEGF, P53, SF and NLRP3 for the Early Diagnosis of Canine Mammary Carcinoma" Animals 14, no. 9: 1272. https://doi.org/10.3390/ani14091272
APA StyleYang, N. -Y., Zheng, H. -H., Yu, C., Ye, Y., & Xie, G. -H. (2024). Diagnosis of Canine Tumours and the Value of Combined Detection of VEGF, P53, SF and NLRP3 for the Early Diagnosis of Canine Mammary Carcinoma. Animals, 14(9), 1272. https://doi.org/10.3390/ani14091272