Determining an Appropriate Time to Start Prophylactic Treatment with Intranasal Corticosteroids in Japanese Cedar Pollinosis

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
2.3. Economic Evaluation
2.4. Measurement of Pollen Dispersion
2.5. Statistical Analysis
3. Results
3.1. Patient Population
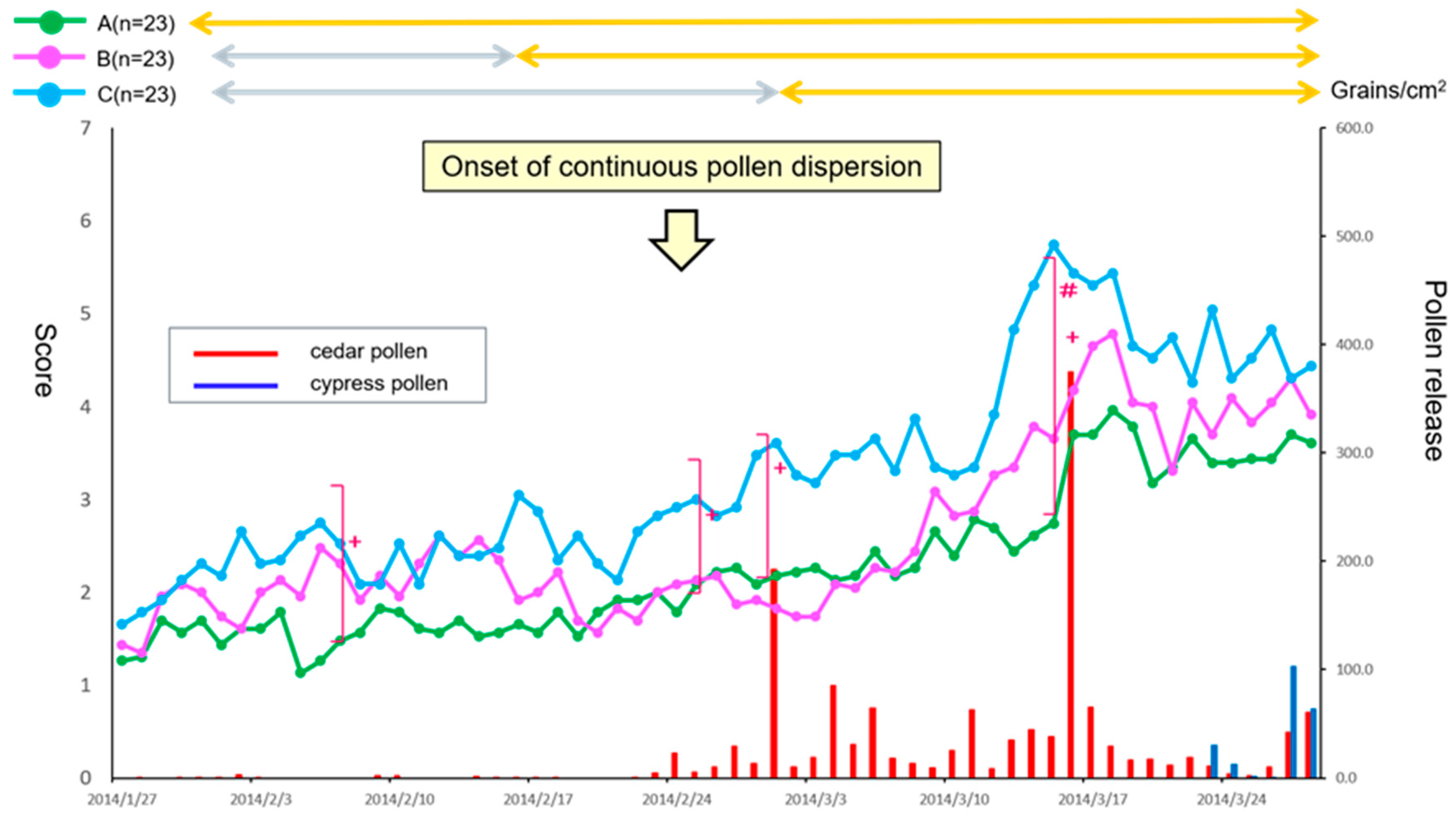
3.2. Fluctuation of Cedar Pollen Dispersion
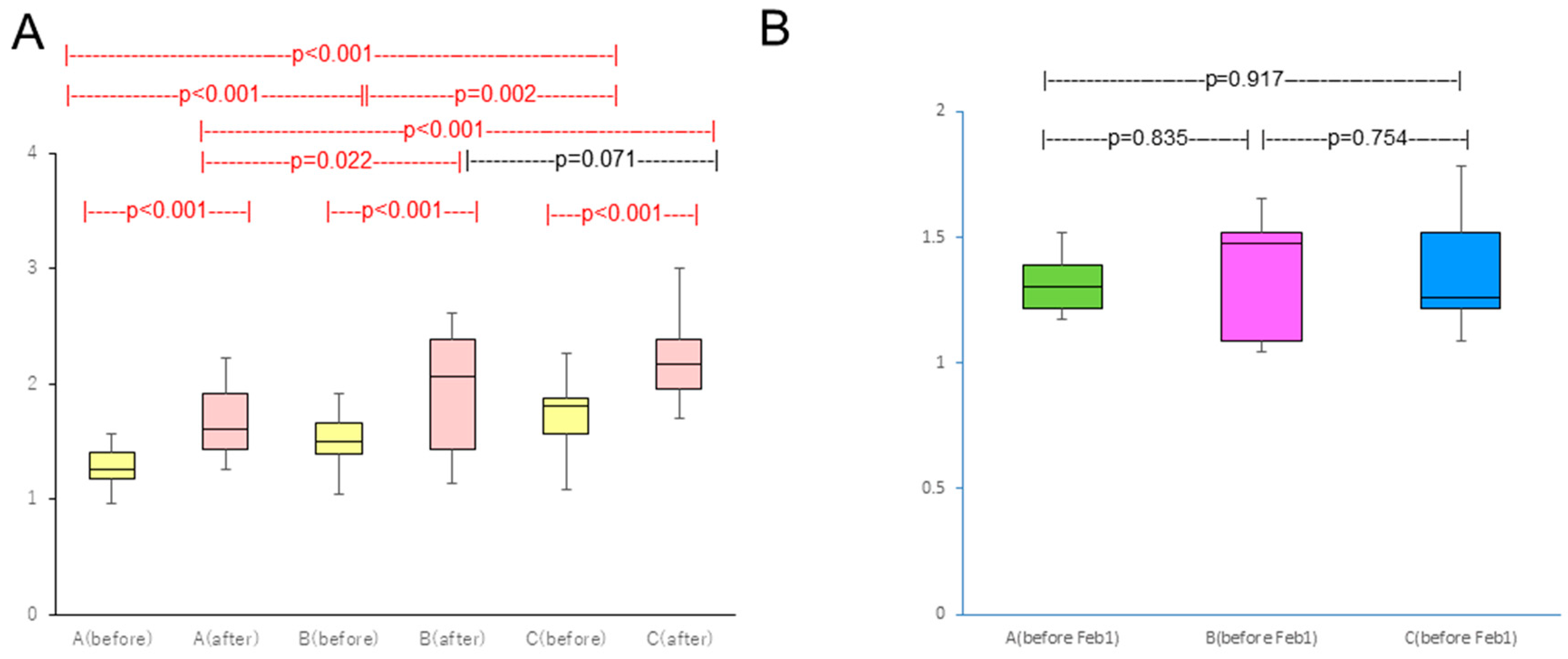
3.3. Primary Endpoint Efficacy
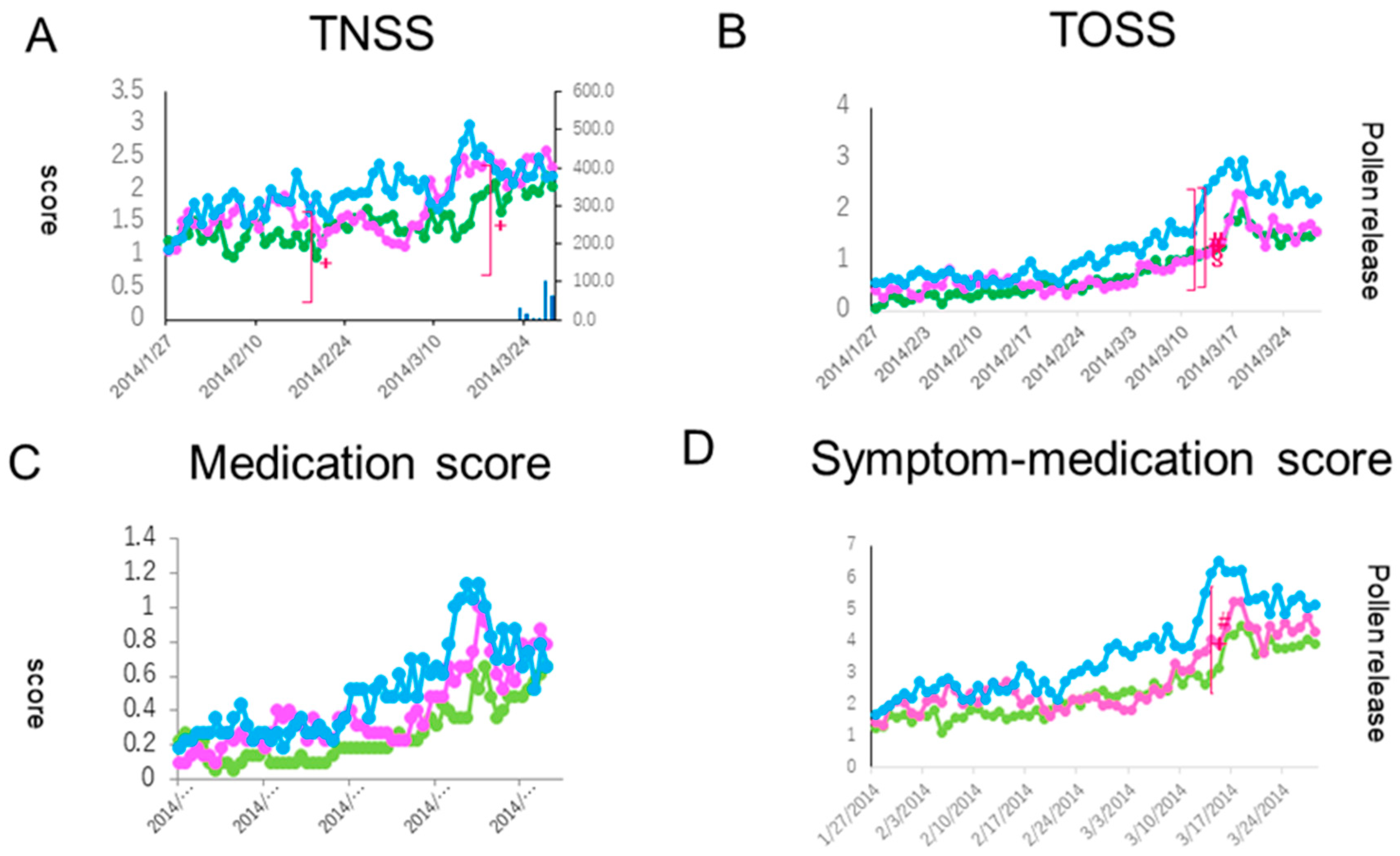
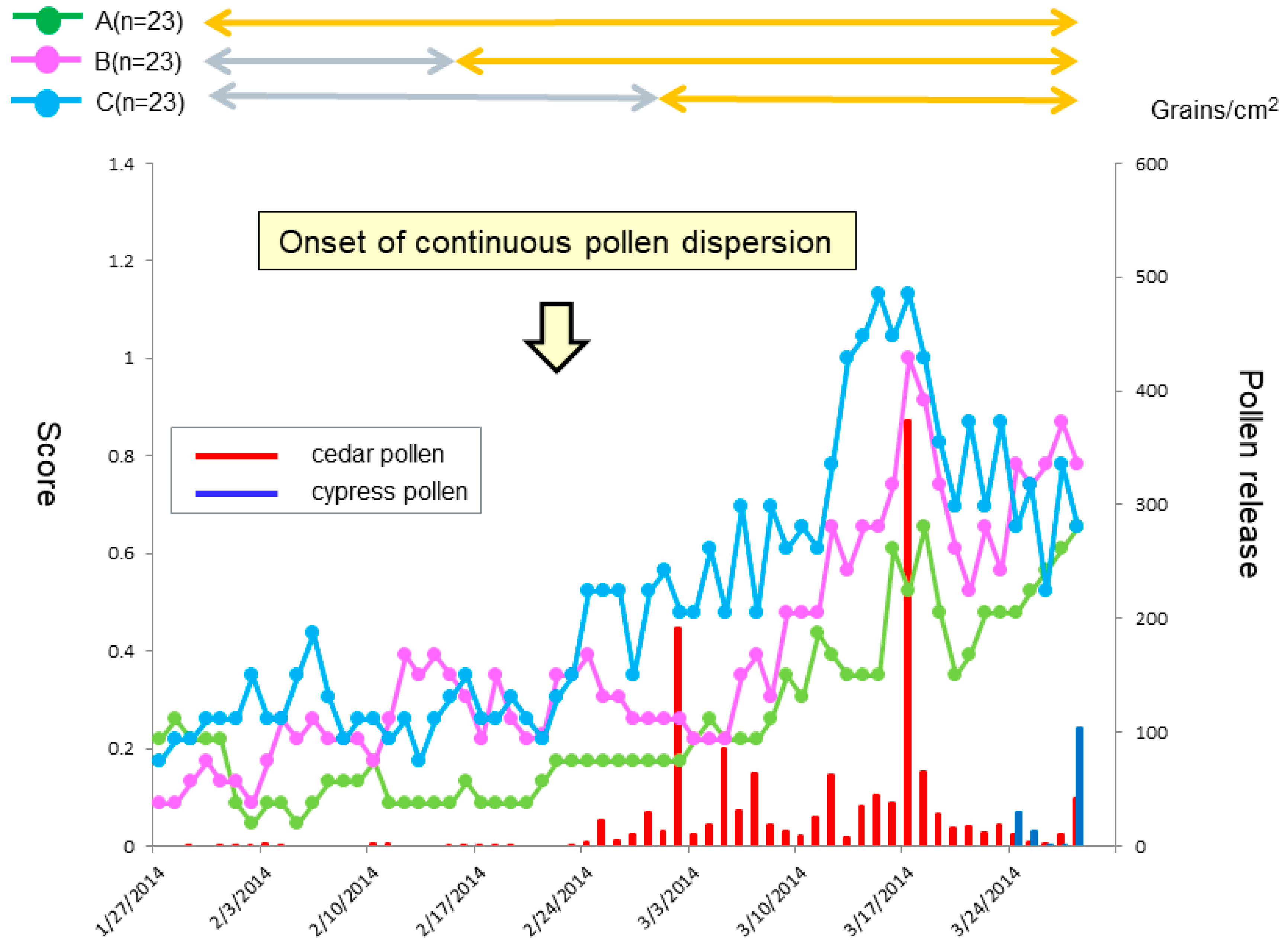
3.4. Secondary Endpoint Efficacy
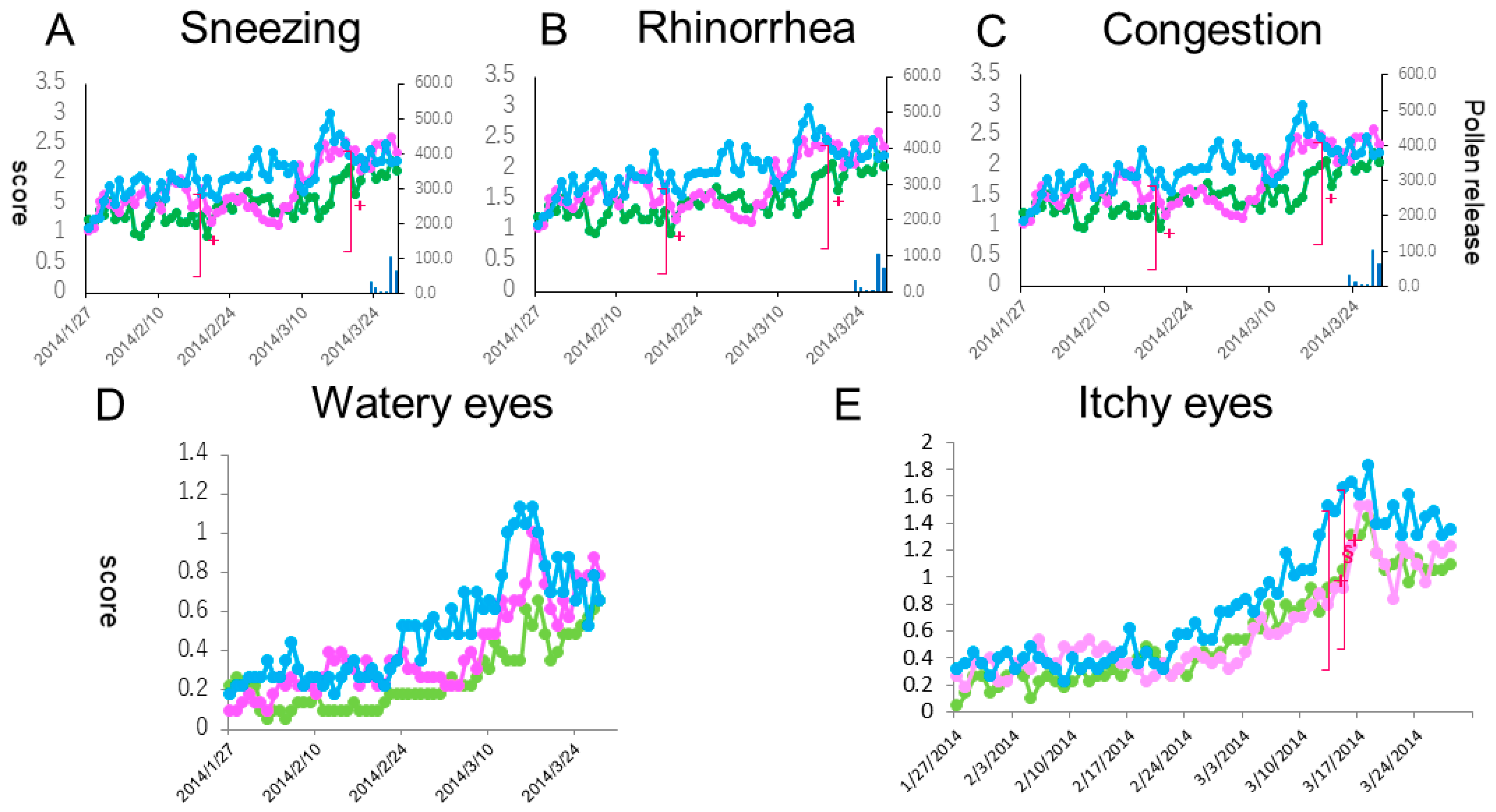
3.5. Courses of Individual Symptoms
3.6. Safety
3.7. Increment Cost Effective Ratio
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Okubo, K.; Kurono, Y.; Ichimura, K.; Enomoto, T.; Okamoto, Y.; Kawauchi, H.; Suzaki, H.; Fujieda, S.; Masuyama, K.; The Japanese Society of Allergology. Japanese Guideline for Allergic Rhinitis 2017. Allergol. Int. 2017, 66, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Saito, H.; Fujieda, S. Present state of Japanese cedar pollinosis: The national affliction. J. Allergy Clin. Immunol. 2014, 133, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Morelli, M.C.; Bordonaro, S.; Hedbys, L.; Romagnani, S.; The Italian Study Group. Effect of pre-seasonal and seasonal treatment with budesonide topical nasal powder in patients with seasonal allergic rhinitis. Allergol. Int. 1996, 45, 151–157. [Google Scholar] [CrossRef]
- Canonica, G.W.; Compalati, E. Minimal persistent inflammation in allergic rhinitis: Implications for current treatment strategies. Clin. Exp. Immunol. 2009, 158, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Noyama, Y.; Okano, M.; Fujiwara, T.; Kariya, S.; Makihara, S.; Haruna, T.; Kanai, K.; Higaki, T.; Nishizaki, K. Effect of intranasal corticosteroid on pre-onset activation of eosinophils and mast cells in experimental Japanese cedar pollinosis. Allergol. Int. 2016, 65, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graft, D.; Aaronson, D.; Chervinsky, P.; Kaiser, H.; Melamed, J.; Pedinoff, A.; Rosen, J.P.; Schenkel, E.J.; Vandewalker, M.L.; Keim, A. A placebo- and active-controlled randomized trial of prophylactic treatment of seasonal allergic rhinitis with mometasone furoate aqueous nasal spray. J. Allergy Clin. Immunol. 1996, 98, 724–731. [Google Scholar] [CrossRef]
- Pitsios, C.; Papadopoulos, D.; Kompoti, E.; Manoussakis, E.; Garris, V.; Petalas, K.; Tassios, I.; Baibas, N.; Kontou-Fili, K.; Saxoni-Papageorgiou, P.; et al. Efficacy and safety of mometasone furoate vs nedocromil sodium as prophylactic treatment for moderate/severe seasonal allergic rhinitis. Ann. Allergy Asthma Immunol. 2006, 96, 673–678. [Google Scholar] [CrossRef]
- Takahashi, G.; Matsuzaki, Z.; Okamoto, A.; Ito, E.; Matsuoka, T.; Nakayama, T.; Masuyama, K. A randomized control trial of stepwise treatment with fluticasone propionate nasal spray and fexofenadine hydrochloride tablet for seasonal allergic rhinitis. Allergol. Int. 2012, 61, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Makihara, S.; Okano, M.; Fujiwara, T.; Kimura, M.; Higaki, T.; Haruna, T.; Noda, Y.; Kanai, K.; Kariya, S.; Nishizaki, K. Early interventional treatment with intranasal mometasone furoate in Japanese cedar/cypress pollinosis: A randomized placebo-controlled trial. Allergol. Int. 2012, 61, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Yonekura, S.; Sakurai, D.; Katada, K.; Inamine, A.; Hanazawa, T.; Horiguchi, S.; Okamoto, Y. Comparison of nasal steroid with antihistamine in prophylactic treatment against pollinosis using an environmental challenge chamber. Allergy Asthma Proc. 2012, 33, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Higaki, T.; Okano, M.; Makihara, S.; Fujiwara, T.; Haruna, T.; Noda, Y.; Kariya, S.; Nishizaki, K. Early interventional treatment with intranasal corticosteroids compared with postonset treatment in pollinonsis. Ann. Allergy Asthma Immunol. 2012, 109, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.J.; Jhaveri, M.; Saverno, K.; Meyer, K.; Nightengale, B. Cost-effectiveness of second-generation antihistamins and motelukast in relieving allergic rhinitis nasal symptoms. Am. Health Drug Benefits 2008, 1, 26–34. [Google Scholar] [PubMed]
- Higaki, T.; Okano, M.; Kariya, S.; Fujiwara, T.; Haruna, T.; Hirai, H.; Murai, A.; Gotoh, M.; Okubo, K.; Yonekura, S.; et al. Determining minimal clinically important differences in Japanese cedar/cypress pollinosis. Allergol. Int. 2013, 62, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Baroody, F.M.; Shenaq, D.; DeTineo, M.; Wang, J.; Naclerio, R.M. Fluticasone furoate nasal spray reduces the nasal-ocular reflex: A mechanism for the efficacy of topical steroids in controlling allergic eye symptoms. J. Allergy Clin. Immunol. 2009, 123, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, G.J.; Neffen, H. Efficacy of fluticasone furoate nasal spray vs. placebo for the treatment of ocular and nasal symptoms of allergic rhinitis: A systematic review. Clin. Exp. Allergy 2011, 41, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Rudmik, L.; Drummond, M. Health economic evaluation: Important principles and methodology. Laryngoscope 2013, 123, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Verhaggen, B.G.; Westerhout, K.Y.; Schreder, C.H.; Augustin, M. Health economic comparison of SLIT allergen and SCIT allergoid immunotherapy in patients with seasonal grass-allergic rhinoconjunctivitis in Germany. Clin. Trans. Allergy 2015, 5, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gander, P.; Scott, G.; Mihaere, K.; Scott, H. Societal costs of obstructive sleep apnoea syndrome. N. Z. Med. J. 2010, 123, 13–23. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | Group C | ||
|---|---|---|---|---|
| Number | 24 * | 23 | 23 | |
| Age | Mean ± SD | 36.3 ± 8.9 | 38.2 ± 8.6 | 43.1 ± 9.7 |
| Range | 21–48 | 19–50 | 28–69 | |
| Sex (male/female) | 7/17 * | 5/18 | 5/18 | |
| Sum of Naso-Ocular Symptom Scores from February to March | Drug Cost | Sum of Drug Cost | |||
|---|---|---|---|---|---|
| FFNS (2040 yen/bottle) | Levocetirizine (105 yen/tablet) | Olopatadine Eye Drop (198 yen/bottle) | |||
| Group A | 130 | 4 bottles (8160 yen) | 2.8 tablets (315 yen) | 1.00 bottle (198 yen) | 8673 yen |
| Group B | 150 | 3 bottles (6120 yen) | 2.4 tablets (315 yen) | 0.96 bottle (198 yen) | 6633 yen |
| Group C | 191 | 2 bottles (4080 yen) | 4.5 tablets (525 yen) | 1.43 bottles (396 yen) | 5001 yen |
| Group A | Group B | Group C | |||
|---|---|---|---|---|---|
| Placebo | FFNS | Placebo | FFNS | ||
| Cold | 7 | 3 | 3 | 3 | 1 |
| Urticaria | 1 | ||||
| Headache | 1 | 1 | 1 | ||
| Cough | 1 | 3 | |||
| Pharyngeal discomfort | 1 | 3 | |||
| Itch of face | 1 | ||||
| Fever | 1 | ||||
| Nasal bleeding | 1 | ||||
| Ear pain | 2 | ||||
| Aphthous ulcer | 1 | ||||
| Sore throat | 1 | ||||
| Oral discomfort | 1 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haruna, T.; Kariya, S.; Higaki, T.; Makihara, S.-i.; Kanai, K.; Komatsubara, Y.; Oka, A.; Nishizaki, K.; Okano, M. Determining an Appropriate Time to Start Prophylactic Treatment with Intranasal Corticosteroids in Japanese Cedar Pollinosis. Med. Sci. 2019, 7, 11. https://doi.org/10.3390/medsci7010011
Haruna T, Kariya S, Higaki T, Makihara S-i, Kanai K, Komatsubara Y, Oka A, Nishizaki K, Okano M. Determining an Appropriate Time to Start Prophylactic Treatment with Intranasal Corticosteroids in Japanese Cedar Pollinosis. Medical Sciences. 2019; 7(1):11. https://doi.org/10.3390/medsci7010011
Chicago/Turabian StyleHaruna, Takenori, Shin Kariya, Takaya Higaki, Sei-ichiro Makihara, Kengo Kanai, Yasutoshi Komatsubara, Aiko Oka, Kazunori Nishizaki, and Mitsuhiro Okano. 2019. "Determining an Appropriate Time to Start Prophylactic Treatment with Intranasal Corticosteroids in Japanese Cedar Pollinosis" Medical Sciences 7, no. 1: 11. https://doi.org/10.3390/medsci7010011
APA StyleHaruna, T., Kariya, S., Higaki, T., Makihara, S. -i., Kanai, K., Komatsubara, Y., Oka, A., Nishizaki, K., & Okano, M. (2019). Determining an Appropriate Time to Start Prophylactic Treatment with Intranasal Corticosteroids in Japanese Cedar Pollinosis. Medical Sciences, 7(1), 11. https://doi.org/10.3390/medsci7010011