1. Introduction
Peri-implantitis is one of the most common problems that can occur during an implant–prosthetic rehabilitation. Mucositis is the initial manifestation of peri-implant disease, with bleeding on gentle probing, erythema, swelling and/or suppuration; peri-implantitis, rather, is a condition that is characterized by inflammation in the peri-implant mucosa, progressive bone loss (radiographic bone loss compared to previous examinations), bleeding on probing and/or suppuration, increased probing depths and/or recession of the mucosal margin [
1].
Schwarz et al. [
2] stated that risk factors for peri-implantitis insurgence are history of chronic periodontitis and poor plaque control with the absence of an appropriate maintenance protocol; other factors with less evidence of involvement in peri-implantitis are smoking, diabetes, persistence of submucosal cement, lack of keratinized mucosa and implant positioning.
Peri-implantitis treatments are mainly directed to removing bacterial biofilm from the contaminated surfaces and to provide more suitable access to implant surfaces in order to facilitate maintenance procedures.
The treatments proposed involve both nonsurgical and surgical therapies; the nonsurgical approach is represented by mechanical decontamination, antibiotics and antiseptics; the surgical approach includes air-powered abrasives, resective surgery and regenerative surgery.
Moreover, an important treatment option that can be added to the abovementioned therapies is represented by surface decontamination with chemical methods (citric acid, EDTA, hydrogen peroxide, saline solution) or lasers [
3].
Laser therapy has been demonstrated to be effective in peri-implantitis management; in the literature, the use of an Er:YAG laser, CO
2 laser and photodynamic therapies (PDTs) [
4], that can be defined as the eradication of target cells by reactive oxygen species using a photosensitizer and light of an appropriate wavelength, has been proposed. It may be an alternative to produce an effect on target bacteria directly in the site of infection, bypassing problems related to antibiotics [
5,
6,
7,
8,
9]. “Photodynamic therapy involves three components: a photosensitizer, light and oxygen. When a photosensitizer is irradiated with a light of a specific wavelength it undergoes a transition from one state to the low energy of a singlet excitation state. Consequently it can decay to its previous state, with fluorescence emission, or may undergo a transition to a triplet state of higher energy. The triplet state can react with the endogenous oxygen to produce singlet oxygen and other radicals, causing a rapid and selective destruction of the target tissue. Photodynamic therapy produces cytotoxic effects on subcellular organelles and molecules, including mitochondria, lysosomes, cell membranes and nuclei of tumor cells” [
10]. If the wavelength used is absorbed in the chromophore used, the laser ray cannot penetrate more deeply, and if the power density is too low (usually, PDT protocols use low-level laser therapy (LLLT) energy, in order to avoid any thermal damage), the decontaminating effects are not enough; as a result, PDT showed an incomplete efficacy in deep bacterial infiltrations [
4,
5].
However, there is evidence that classic PDT has positive effects on periodontal inflammatory indexes [
6].
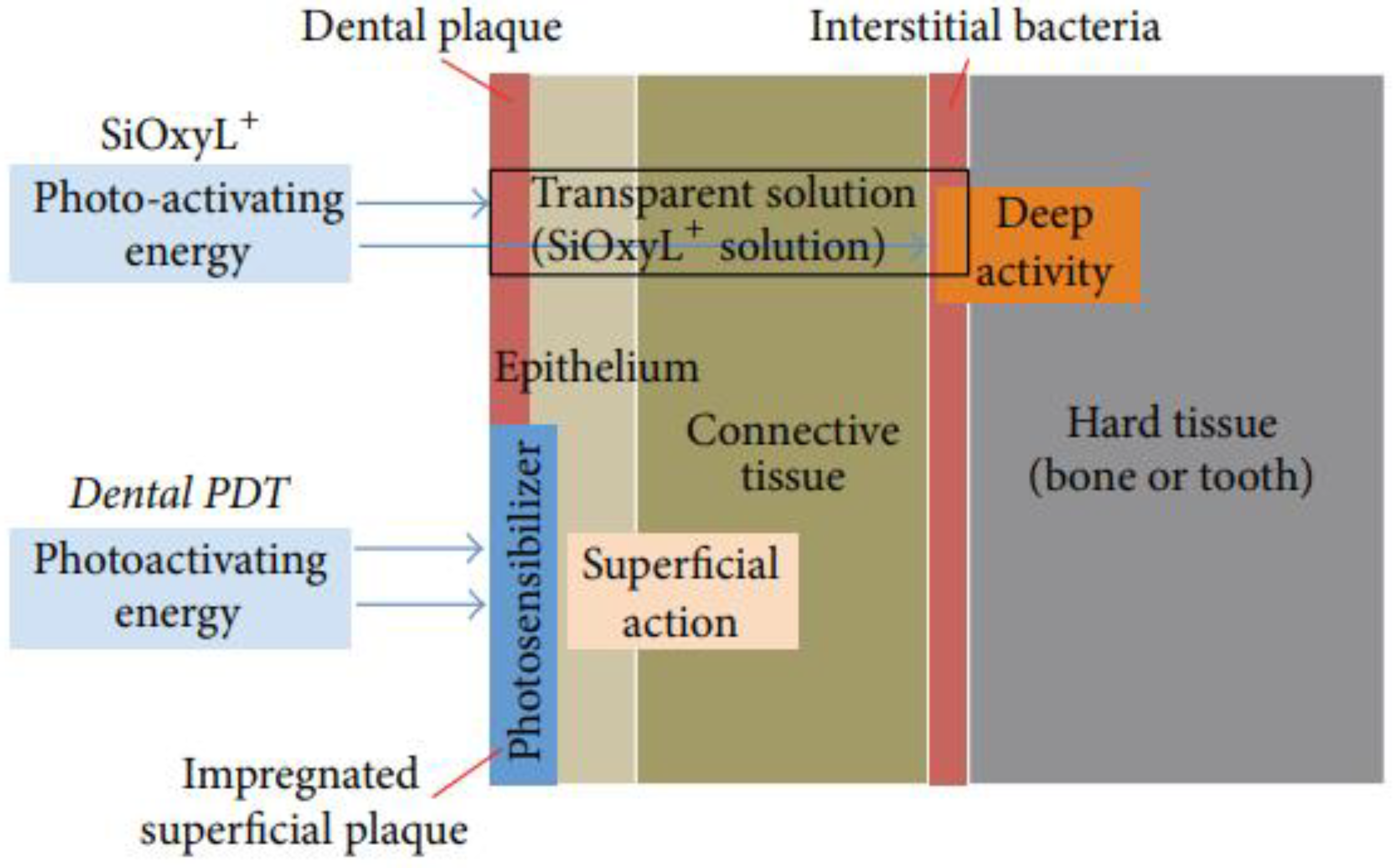
Recently, nonsurgical periodontal therapy combining a 980 nm laser with hydrogen peroxide, as described in the Rey protocol [
8], has been gaining more and more consensus in dentistry. The combination of a high-frequency diode laser (980 nm) and the irrigation of periodontal pockets with hydrogen peroxide, if compared to classic photodynamic therapy (PDT) performed with photoactivating agents, provides important absorption inside the tissues and deep penetration into the biofilm [
7,
8,
9] (
Figure 1).
This treatment modality, named oxygen high-level laser therapy (OHLLT), seems to be able to achieve a deep sanitization of implant surfaces [
5,
10]. In fact, Caccianiga et al. stated that OHLLT appears to be a good adjunct to surgical treatment of peri-implantitis, improving the bacterial and inflammatory condition; the reduced periodontal inflammation, with a decrease in probing depth and bleeding on probing, and the massive reduction in bacteria and particularly in aggressive pathogens often found in affected sites are suggestive of the potential effectiveness of this protocol for the treatment of peri-implant disease [
10].
Together with the treatment option, Caccianiga et al. [
9] reported that Sioxyl+ solution, that is hydrogen peroxide stabilized with glycerol phosphate complexes (HP-GP), provides optimal results in terms of a substantial decrease in the bacterial load combined with a maximal biostimulation induction of soft tissues and osteogenesis.
The role of Er:YAG lasers in peri-implantitis treatment is controversial in the literature; a recent study by AlMoharib et al. [
11] reports an effective bacterial removal activity of Er:YAG lasers from titanium discs; nevertheless, the authors reported no significant differences between Er:YAG lasera and titanium brushes or carbon fiber curettes. Hakki et al. [
12], instead, reported better results with Er:YAG lasers with respect to curettes, titanium brushes, ultrasonic scalers and air abrasives. Positive results were reported also by Takasaki et al. The authors, in an animal model, histologically showed an efficient implant surface debridement, leading to an improvement in bone-to-implant contact [
13]. However, there are studies that reported no advantages with the use of this kind of laser [
14,
15,
16].
The aim of this retrospective controlled study is to compare OHLLT with OHLLT with erbium laser treatment, in order to identify if there is an advantage with this combined treatment modality, especially in bone regeneration.
2. Materials and Methods
The present retrospective controlled study was approved by the Ethics Committee of the School of Medicine and Surgery at Milano Bicocca University (protocol n. 11/17), derived from the approval of the Italian National Institute of Health (ISS), prot. 30/07/2007-0040488, and it was conducted in observance of the Declaration of Helsinki.
We selected a total amount of 210 implants, affected by peri-implantitis, subdivided into 126 in the upper arch and 84 in the mandible, molar and premolar region.
Our cluster of implants consisted of different types of implant surfaces: 50 machined implants, 120 nano-roughness implants, 35 hydroxyapatite-coated implants and 5 zirconia implants.
All implants were finalized with screwed fixed dental prostheses.
Inclusion criteria were: both male and female participants, peri-implantitis without previous surgical treatment in the last year, bleeding on probing, peri-implant pockets > 4 mm, no smoking history, absence of allergies, absence of uncontrolled systemic disease, absence of pregnancy or lactation, absence of abuse of alcohol or drugs, acceptance of the surgical intervention by signing an informed consent.
Exclusion criteria were: peri-implantitis with previous surgical treatment in the last year, absence of bleeding on probing, peri-implant pockets < 4 mm, smoking history, presence of allergies, presence of uncontrolled systemic disease, presence of pregnancy or lactation, abuse of alcohol or drugs, lack of acceptance of the surgical intervention by signing an informed consent. Implants were assessed for bleeding on probing (BOP) and the presence of suppuration: at T0, in fact, all the implants analyzed showed bleeding on probing and the presence of suppuration. All implants were analyzed through periapical radiographs using the long cone paralleling technique. We adopted the distance from the implant shoulder to the alveolar bone crest (DIB) as a reliable radiographic parameter for long-term monitoring in clinical practice. Bone level measurements were taken from implant neck to bone crest, both on the mesial and distal side of implants; for each implant, the lowest measurement between the mesial and distal aspect was considered. Measurements were taken by the same operator.
The software used to take the measurements was Soredex Digora®.
Each implant was evaluated before and after treatment, at T0 (time of diagnosis of peri-implantitis) and at T1 (most recent follow-up of implant treated for peri-implantitis). We set 5 years as the minimum follow-up period for T1.
Bone level measurements were organized in Excel to examine bone levels around implants at the two different time periods.
All patients agreed with the following oral hygiene maintenance protocol at home:
Sonic brush with vertical movement (Broxo), interdental brushes and oral irrigators (Broxo) at least two times every day. We selected 2 groups: the control group was the OHLLT group, where patients with peri-implantitis were treated with a surgical OHLLT protocol; the test group was the OHLLT + Er:Yag group, where the use of an erbium:Yag laser was carried out with OHLLT surgical procedures.
The collected data were analyzed with the Statistical Package for Social Sciences (SPSS) version 11.5.
Surgical Procedures
OHLLT Group (88 implants: 54 in the maxilla, 34 in the mandible)
The OHLLT surgical procedure consists of (
Figure 2 and
Figure 3): local anesthesia; intrasulcular incision for a full thickness periodontal flap; mechanical instrumentation and removal of necrotic tissues with Gracey curettes; ultrasonic instrumentation for supra- and subgingival scaling combined with water–Betadine irrigation (5:1 ratio); air flow device with sodium bicarbonate powder (highly abrasive powder).
Then, the OHLLT protocol was performed (Wiser diode laser, Sioxyl Solution, Doctor Smile, Vicenza, Italy) (
Figure 4): irrigation of peri-implant pockets with Sioxyl Solution; aspiration of Sioxyl Solution emerging from the gingival sulcus and leaving the remaining solution inside the pocket for 2 min; introduction of the HF Diode Laser Fiber 400 microns within the pocket and reaching the bottom, radiation of subgingival tissues with a back and forth movement using the dedicated program, 60 s per side (2.5 W peak power, high frequency, 10 KHz, power average 0.5 W, fluency 25,000 J/cm
2, 416.66 J/cm
2 per second). After the decontamination with OHLLT, the site was grafted with a mix of Bio-Oss granules 25, autologous bone chips, platelet-rich fibrin (PRF) and collagen membranes (45% Bio-Oss 25, 45% PRF, 10% autologous bone chips). At the end, we carried out flap repositioning and suturing.
OHLLT + Er:Yag Laser Group (112 implants: 72 in the maxilla, 50 in the mandible)
The OHLLT + Erbium:Yag surgical procedure consists of: local anesthesia; intrasulcular incision for a full thickness periodontal flap; Er:YAG laser (Pluser, Doctor Smile, Vicenza, Italy) first applied in order to remove granulation tissue (power: 1.8 W, frequency: 35 Hz, energy: 50 mJ, water: 20%, air: 60%); ultrasonic instrumentation for supra- and subgingival scaling combined with water–Betadine irrigation (5:1 ratio); air flow device with sodium bicarbonate powder (highly abrasive powder); subsequently, the OHLLT protocol was performed (Wiser diode laser, Sioxyl Solution, Doctor Smile, Vicenza, Italy): irrigation of peri-implant pockets with Sioxyl Solution; aspiration of Sioxyl Solution emerging from the gingival sulcus and leaving the remaining solution inside the pocket for 2 min; introduction of the HF Diode Laser Fiber 400 microns within the pocket and reaching the bottom, radiation of subgingival tissues with a back and forth movement using the dedicated program, 60 s per side (2.5 W peak power, high frequency, 10 KHz, power average 0.5 W, fluency 25,000 J/cm
2, 416.66 J/cm
2 per second). After the decontamination with OHLLT, the Er:YAG laser (Pluser, Doctor Smile) was used to treat implant surfaces (power: 0.8 W, frequency: 10 Hz, energy: 80 mJ, water: 60%, air: 60%) and then to create mechanical biostimulating effects on bone tissues (
Figure 5) (power: 3.2–3.8–4.4 W, frequency: 20 Hz, energy: 160–190–220 mJ, depending on bone density, from lower to higher, water: 70%, air: 80%). Finally, a graft mix consisting of Bio-Oss granules, autologous bone chips, platelet-rich fibrin (PRF) and collagen membranes (45% Bio-Oss, 45% PRF, 10% autologous bone chips) was applied, finalizing with flap repositioning and suturing.
3. Results
We carried out a retrospective controlled study establishing, as a control group, the implants treated with only OHLLT, a choice that is supported by extensive literature reporting successful treatments with this modality; the test group was represented by OHLLT + Er:YAG laser treatment.
All peri-implant pockets were treated successfully with clinical signs of soft and hard tissue healing. In fact, at T1, all implants showed the absence of suppuration and contemporary resolution of bleeding on probing (BOP).
The percentage of bone loss was analyzed for each implant.
Mean bone loss due to peri-implantitis at T0 (before laser treatments) was 5.8 mm in the upper arch and 5.2 mm in the mandible, as detected from the preoperative periapical radiographs.
The total amount of bone loss, considering both the upper and lower arch, was 5.6 mm (
Table 1).
In the group of implants that received only OHLLT (Wiser, Doctor Smile), we noticed at T1 a mean bone loss after treatment of 2.1 mm in the upper arch and 2.4 mm in the mandible, resulting in a total mean bone loss of 2.3 mm (
Table 2).
Implants that received OHLLT (Wiser, Doctor Smile) + Er:YAG laser (Pluser, Doctor Smile), at T1, showed a mean bone loss of 2.0 mm in the upper arch and 2.5 mm in the mandible, with a total mean bone loss of 2.3 mm (
Table 3).
The results showed no statistically significant differences between the two groups at p < 0.01 (p = 0.596).
Statistical analysis revealed no significant difference in postoperative bone loss between the two groups. According to the Kolmogorov–Smirnov test, overall, the data followed a normal distribution (value of the K-S test statistic = 0.0912;
p = 0.36112). Statistical analyses are presented in
Table 4 and
Table 5.
4. Discussion
Peri-implantitis treatment still represents a challenge in dentistry.
Our study has been developed with a meticulous protocol consisting of the usual periodontal instrumentation with the addition of laser treatments; this approach finds support from numerous studies in the scientific literature.
Stein et al. observed a significant improvement of peri-implantitis with a combination of ultrasonic debridement, soft tissue curettage, glycine air powder polishing and Povidone-iodine, as a non-surgical approach [
17].
Peterskilla et al. [
18], with an experimental study in an animal model, stated that low-abrasion air polishing induced the smallest amount of tissue damage compared with hand instrumentation and ultrasonic scalers; this is surely important in the optical of minimally invasive dentistry that represents an unavoidable topic in modern dentistry.
Sahrmann et al. [
19], with an in vitro study, demonstrated that hand instrumentation (Gracey curettes), ultrasonic devices and air powder abrasive devices were not effective in the achievement of an optimal debridement of implant surfaces.
Therefore, laser-assisted treatments have been proposed to overcome the abovementioned important limits of traditional therapies.
PDT has been proposed with the use of low-level laser therapy (LLLT), although with clear limits, particularly due to absence of efficient bactericidal activity because of low power; low release of singlet oxygen with a frequency that does not exceed 1000 Hz because of long pulse time; and low penetration capacity. LLLT, however, has the important characteristic of biostimulation, that means stimulation of cells activity to achieve tissue regeneration [
20,
21].
An implementation of this treatment modality has been developed with the use of HLLT with the addition of Sioxyl Solution (OHLLT), combining high peak power (>2 W in order to eliminate pathogens in the oral cavity) with low mean power (<0.8 W in order to cause biostimulation); in this way, the temperature does not exceed 45 °C (range of tissue vasodilatation) [
9].
OHLLT, with a frequency higher than 7000 Hz (as determined by the pulse length in microseconds), causes a continuous emission of singlet oxygen, causing destruction of pathogenic bacteria (this is in accordance with G. Rey protocols) [
9].
OHLLT has been shown to be effective in reducing the amount of total bacteria on contaminated implant surfaces [
9], in particular in association with hydrogen peroxide [
22,
23].
Many protocols were proposed in the literature for implant surfaces’ decontamination, such as the use of Er:YAG lasers that seem to enhance bacterial decontamination [
24,
25].
Wang et al., in a recent randomized controlled clinical trial, found that Er:YAG lasers may advance bacterial decontamination because they noticed a statistically significant reduction in pocket depth measurements, although there were no improvements in clinical attachment level (CAL), gingival index (GI) or radiographic bone level. The authors concluded that “larger sample size and longer follow-up is needed to confirm if Er:YAG laser irradiation provides additional clinical benefits for peri-implantitis regenerative therapy” [
26].
Swider et al. [
27], in a recent meta-analysis, evaluated 49 articles, but only seven met the strict inclusion criteria during the quality assessment. The studies included were: Birang et al. [
28], Caccianiga et al. [
5], Persson et al. [
29], Arisan et al. [
30], Yoshino et al. [
31], Bassetti et al. [
32] and Dörtbudak et al. [
33]. They concluded that “a high-power diode laser may have some effect on peri-implant pathogens causing peri-implantitis, whereas Er:YAG laser application shows no significant effect on oral bacteria in the long term. aPDT (antimicrobial photodynamic therapy) has the ability to reduce the total count of the different bacterial strains associated with peri-implantitis, e.g.,
A. actinomycetemcomitans,
P. gingivalis,
P. intermedia,
T. denticola,
T. forsythia,
F. nucleatum, and
C. rectus.”
These conclusions of the authors were exactly the same as those published in 2016 by our team [
5].
According to our results [
5] and Swider et al. [
27], in the current research, we decided to test the efficacy of OHLLT alone [
5] or associated with an Er:Yag laser, combining these two lasers every time we needed to improve bone regeneration. Er:Yag lasers, due to the significant absorption in water and hydroxyapatite, cannot penetrate more than 2 µm inside soft and hard tissues. OHLLT, rather, showed the ability to remove periodontal pathogenic bacteria from periodontal and peri-implant pockets and to improve soft and hard tissue healing [
5,
10], because the proposed diode lasers, with high peak power (2.5 Watt) and low mean power (0.5 Watt), a frequency of 10 KHz, t-on of 20 microns and t-off of 80 microns, can penetrate deeply into oxygenated tissues.
Our study investigated this argument, analyzing a wider sample of implants with peri-implantitis; the results confirm that the Er:YAG laser seems to be ineffective in enhancing bone level gain with respect to OHLLT alone, because there were no statistically significant differences in postoperative bone levels between implants that received only OHLLT and implants with OHLLT + Er:YAG laser. In effect, OHLLT seems to have the crucial effect of greatly enhancing bacterial removal from the implant surfaces and in hard and soft tissue all around the implant’s defects, in particular in addition to hydrogen peroxide [
5,
10]; the laser increases the H
2O
2 bactericidal activity thanks to its photodynamic action, the transfer of energy from the laser to the H2O2 molecule results in its homolytic scission to OH− (hydroxyl radical) or its decomposition to H
2O and
1O
2 (singlet oxygen) [
9]. Instead, the potential advantageous role of Er:YAG has been downgraded with the analysis of our study.
5. Conclusions
OHLLT protocols for peri-implantitis treatment seem to be effective in obtaining successful marginal bone gain. OHLLT plays a central role in enhancing clinical results, leading to a bacterial decontamination not achievable with other treatment modalities, such as only hand instrumentation, antibiotic therapy or LLLT. Peri-implantitis protocols with Er:Yag laser irradiation combined with OHLLT seem to be unable to modify bone regeneration compared to OHLLT alone; thus, it is clearly not able, alone, to resolve peri-implantitis. Further studies could be necessary to assess the enhancements of other parameters, such as periodontal probing depth and clinical attachment levels.
Author Contributions
Conceptualization, G.C., G.R. and M.B.; Data curation, G.C., G.R., P.C., A.L. and A.B.; Formal analysis, A.L. and A.B.; Funding acquisition, M.B. and S.C.; Investigation, G.C., G.R., P.C., A.L. and S.C.; Methodology, G.C., G.R., P.C., A.L., M.B. and A.B.; Project administration, G.C. and M.B.; Resources, M.B. and S.C.; Software, P.C. and A.B.; Supervision, G.C., M.B. and S.C.; Validation, G.C., G.R. and M.B.; Visualization, P.C., A.L., A.B. and S.C.; Writing–original draft, G.C.; Writing–review & editing, G.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Ethics Committee of the School of Medicine and Surgery at Milano Bicocca University (protocol n. 11/17), and received the approval of the Italian National Institute of Health (ISS), protocol 30 July 2007-0040488.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S313–S318. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89 (Suppl. S1), S267–S290. [Google Scholar] [CrossRef]
- Rokaya, D.; Srimaneepong, V.; Wisitrasameewon, W.; Humagain, M.; Thunyakitpisal, P. Peri-implantitis Update: Risk Indicators, Diagnosis, and Treatment. Eur. J. Dent. 2020, 14, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Lshehri, F.A. The role of lasers in the treatment of peri-implant diseases: A review. Saudi. Dent. J. 2016, 28, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Paiusco, A. Clinical, Radiographic and Microbiological Evaluation of High Level Laser Therapy, a New Photodynamic Therapy Protocol, in Peri-Implantitis Treatment; a Pilot Experience. BioMed Res. Int. 2016, 2016, 6321906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bombeccari, G.P.; Guzzi, G.; Gualini, F.; Gualini, S.; Santoro, F.; Spadari, F. Photodynamic therapy to treat periimplantitis. Implant Dent. 2013, 22, 631–638. [Google Scholar] [CrossRef]
- Caccianiga, G.; Cambini, A.; Rey, G.; Paiusco, A.; Fumagalli, T.; Giacomello, M.S. The use of Laser diodes superpulses in Implantology. Eur. J. Inflamm. 2012, 10, 97–100. [Google Scholar] [CrossRef] [Green Version]
- Rey, G. L’apport du laser dans le traitement des poches paradontales. Implantodontie 2000, 38, 27–34. [Google Scholar]
- Caccianiga, G.; Baldoni, M.; Ghisalberti, C.A.; Paiusco, A. A Preliminary In Vitro Study on the Efficacy of High-Power Photodynamic Therapy (HLLT): Comparison between Pulsed Diode Lasers and Superpulsed Diode Lasers and Impact of Hydrogen Peroxide with Controlled Stabilization. BioMed Res. Int. 2016, 2016, 1386158. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Paiusco, A.; Lauritano, D.; Cura, F.; Ormianer, Z.; Carinci, F. Oxygen high level laser therapy is efficient in treatment of chronic periodontitis: A clinical and microbiological study using PCR analysis. J. Biol. Regul. Homeost. Agents 2016, 30 (Suppl. S1), 87–97. [Google Scholar] [PubMed]
- AlMoharib, H.S.; Steffensen, B.; Zoukhri, D.; Finkelman, M.; Gyurko, R. Efficacy of an Er:YAG laser in the decontamination of dental implant surfaces: An in vitro study. J. Periodontol. 2021, 1–9. [Google Scholar] [CrossRef]
- Hakki, S.S.; Tatar, G.; Dundar, N.; Demiralp, B. The effect of different cleaning methods on the surface and temperature of failed titanium implants: An in vitro study. Lasers Med. Sci. 2017, 32, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Takasaki, A.A.; Aoki, A.; Mizutani, K.; Kikuchi, S.; Oda, S.; Ishikawa, I. Er:YAG laser therapy for peri-implant infection: A histological study. Lasers Med Sci. 2007, 22, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Saffarpour, A.; Fekrazad, R.; Heibati, M.N.; Bahador, A.; Saffarpour, A.; Rokn, A.R.; Iranparvar, A.; KharaziFard, M.J. Bactericidal Effect of Erbium-Doped Yttrium Aluminum Garnet Laser and Photodynamic Therapy on Aggregatibacter Actinomycetemcomitans Biofilm on Implant Surface. Int. J. Oral Maxillofac. Implant. 2016, 31, e71–e78. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Hegewald, A.; John, G.; Sahm, N.; Becker, J. Four-year follow-up of combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination. J. Clin. Periodontol. 2013, 40, 962–967. [Google Scholar] [CrossRef]
- Schmage, P.; Thielemann, J.; Nergiz, I.; Scorziello, T.M.; Pfeiffer, P. Effects of 10 cleaning instruments on four different implant surfaces. Int. J. Oral Maxillofac. Implant. 2012, 27, 308–317. [Google Scholar]
- Stein, J.M.; Hammächer, C.; Michael, S.S. Combination of ultrasonic decontamination, soft tissue curettage, and submucosal air polishing with povidone-iodine application for non-surgical therapy of peri-implantitis: 12 Month clinical outcomes. J. Periodontol. 2017. [Google Scholar] [CrossRef]
- Petersilka, G.; Heckel, R.; Koch, R.; Ehmke, B.; Arweiler, N. Evaluation of an ex vivo porcine model to investigate the effect of low abrasive airpolishing. Clin. Oral Investig. 2018, 22, 2669–2673. [Google Scholar] [CrossRef] [Green Version]
- Sahrmann, P.; Ronay, V.; Hofer, D.; Attin, T.; Jung, R.E.; Schmidlin, P.R. In vitro cleaning potential of three di(erent implant debridement methods. Clin. Oral Implant. Res. 2015, 26, 314–319. [Google Scholar] [CrossRef]
- Leonida, A.; Paiusco, A.; Rossi, G.; Carini, F.; Baldoni, M.; Caccianiga, G. Effects of low-level laser irradiation on proliferation and osteoblastic differentiation of human mesenchymal stem cells seeded on a three-dimensional biomatrix: In vitro pilot study. Lasers Med. Sci. 2013, 28, 125–132. [Google Scholar] [CrossRef]
- Caccianiga, G.; Cambini, A.; Donzelli, E.; Baldoni, M.; Rey, G.; Paiusco, A. Effects of laser biostimulation on the epithelial tissue for keratinized layer differentiation: An in vitro study. J. Biol. Regul. Homeost. Agents 2016, 30 (Suppl. S1), 99–105. [Google Scholar] [PubMed]
- Caccianiga, G.; Urso, E.; Monguzzi, R.; Gallo, K.; Rey, G. Efecto bactericida del láser de diodo en periodoncia. Av. Periodoncia Implantol. Oral 2007, 19, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Caccianiga, G.; Urso, E.; Monguzzi, R.; Gallo, K.; Rey, G. Efecto bactericida del láser Nd: YAP. Estudio in vitro. Av. Odontoestomatol. 2007, 23, 127–133. [Google Scholar] [CrossRef]
- Badran, Z.; Bories, C.; Struillou, X.; Saffarzadeh, A.; Verner, C.; Soueidan, A. Er:YAG laser in the clinical management of severe peri-implantitis: A case report. J. Oral Implantol. 2011, 37, 212–217. [Google Scholar] [CrossRef]
- Clem, D.; Gunsolley, J.C. Peri-implantitis Treatment Using Er:YAG Laser and Bone Grafting. A Prospective Consecutive Case Series Evaluation: 1 Year Posttherapy. Int. J. Periodontics Restor. Dent. 2019, 39, 479–489. [Google Scholar] [CrossRef]
- Wang, C.W.; Ashnagar, S.; Gianflippo, R.D.; Arnett, M.; Kinney, J.; Wang, H.L. Laser-assisted regenerative surgical therapy for peri-implantitis: A randomized controlled clinical trial. J. Periodontol. 2020, 92, 378–388. [Google Scholar] [CrossRef]
- Swider, K.; Dominiak, M.; Grzech-Lesniak, K.; Matys, J. Effect of Different Laser Wavelengths on Periodontopathogens in Peri- Implantitis: A Review of In Vivo Studies. Microorganisms 2019, 7, 189. [Google Scholar] [CrossRef] [Green Version]
- Birang, E.; Talebi Ardekani, M.R.; Rajabzadeh, M.; Sarmadi, G.; Birang, R.; Gutknecht, N. Evaluation of Effectiveness of Photodynamic Therapy With Low-level Diode Laser in Nonsurgical Treatment of Peri-implantitis. J. Lasers Med. Sci. 2017, 8, 136–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persson, G.R.; Roos-Jansåker, A.M.; Lindahl, C.; Renvert, S. Microbiologic results after non-surgical erbium-doped:yttrium, aluminum, and garnet laser or air-abrasive treatment of peri-implantitis: A randomized clinical trial. J. Periodontol. 2011, 82, 1267–1278. [Google Scholar] [CrossRef]
- Arısan, V.; Karabuda, Z.C.; Arıcı, S.V.; Topçuoğlu, N.; Külekçi, G. A randomized clinical trial of an adjunct diode laser application for the nonsurgical treatment of peri-implantitis. Photomed. Laser Surg. 2015, 33, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Yoshino, T.; Yamamoto, A.; Ono, Y. Innovative regeneration technology to solve peri-implantitis by Er:YAG laser based on the microbiologic diagnosis: A case series. Int. J. Periodontics Restor. Dent. 2015, 35, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, M.; Schär, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin. Oral Implant. Res. 2014, 25, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Dörtbudak, O.; Haas, R.; Bernhart, T.; Mailath-Pokorny, G. Lethal photosensitization for decontamination of implant surfaces in the treatment of peri-implantitis. Clin. Oral Implant. Res. 2001, 12, 104–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}