
Self-Ratings of Olfactory Function and Their Relation to Olfactory Test Scores. A Data Science-Based Analysis in Patients with Nasal Polyposis

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Variables and Measurements
2.4.1. Self-Ratings of Olfactory Function
2.4.2. Olfactory Testing
2.4.3. Assessment of the Quality of Life
2.4.4. Bias
2.4.5. Study Size
2.4.6. Quantitative Variables
2.5. Data Analysis
2.5.1. Statistical Comparison of Diagnostic Group Differences in Self-Rated Olfactory Function
2.5.2. Covariance and Correlation Analyses
2.5.3. Assessment of the Utility of Self-Ratings for Olfactory Diagnosis Establishment
3. Results
3.1. Participants and Descriptive Data
3.2. Main Results

{kind=link}
{kind=link}
{kind=link}
| qEffect (rm-ANOVA Factor) | Degrees of Freedom | F-Value | p-Value | p < 0.05 |
|---|---|---|---|---|
| Gender | 1150 | 1.925 | 1.67E-01 | |
| Olfactory diagnosis | 2150 | 40.657 | 7.79E-15 | * |
| Self-assessment score | 1150 | 4.562 | 3.40E-02 | * |
| Gender: olfactory diagnosis | 2150 | 0.171 | 8.43E-01 | |
| Gender: self-assessment score | 1150 | 0.097 | 7.56E-01 | |
| Olfactory diagnosis: self-assessment score | 2150 | 1.586 | 2.08E-01 | |
| Gender: olfactory diagnosis: self-assessment score | 2150 | 0.984 | 3.76E-01 |
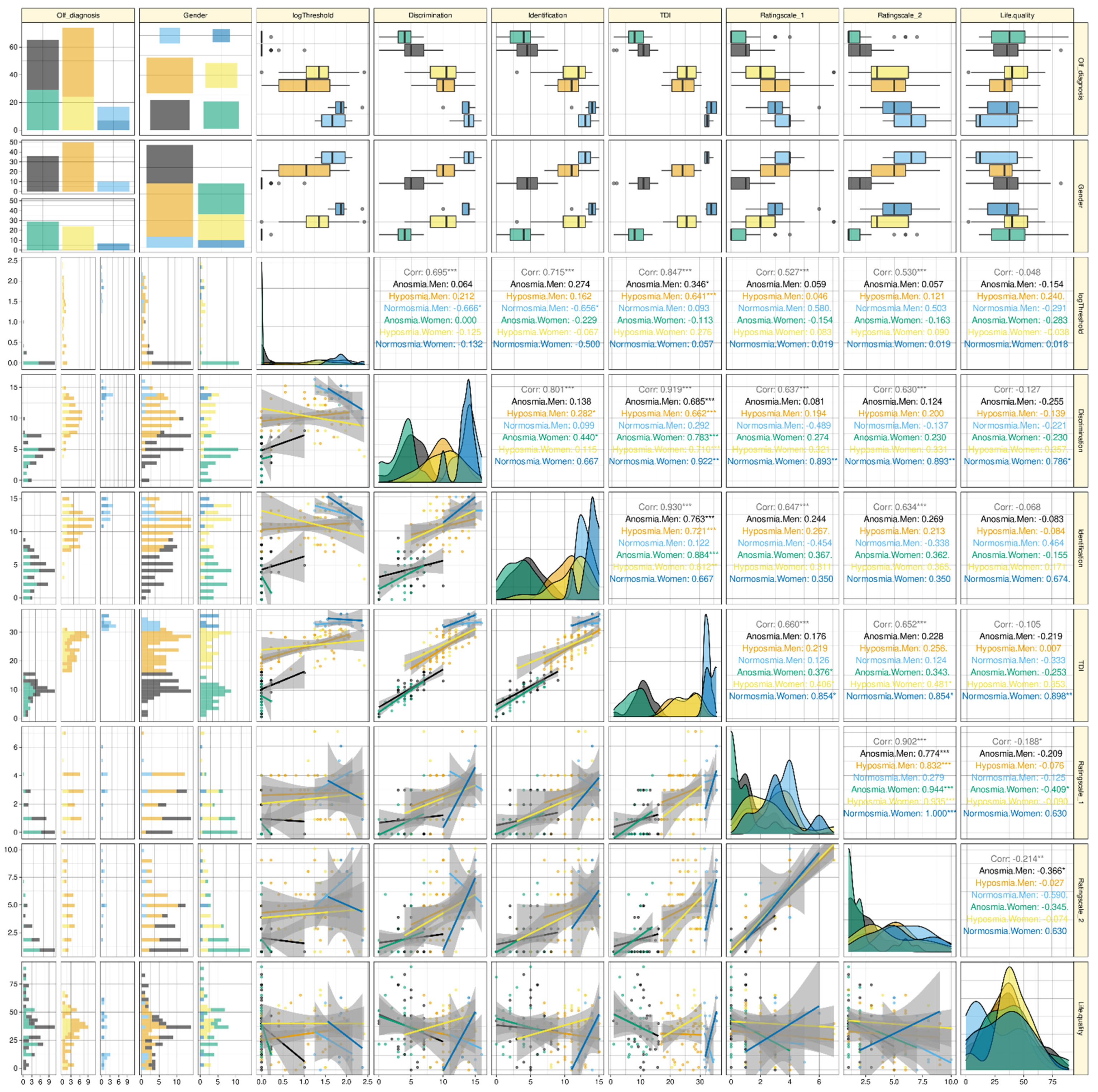
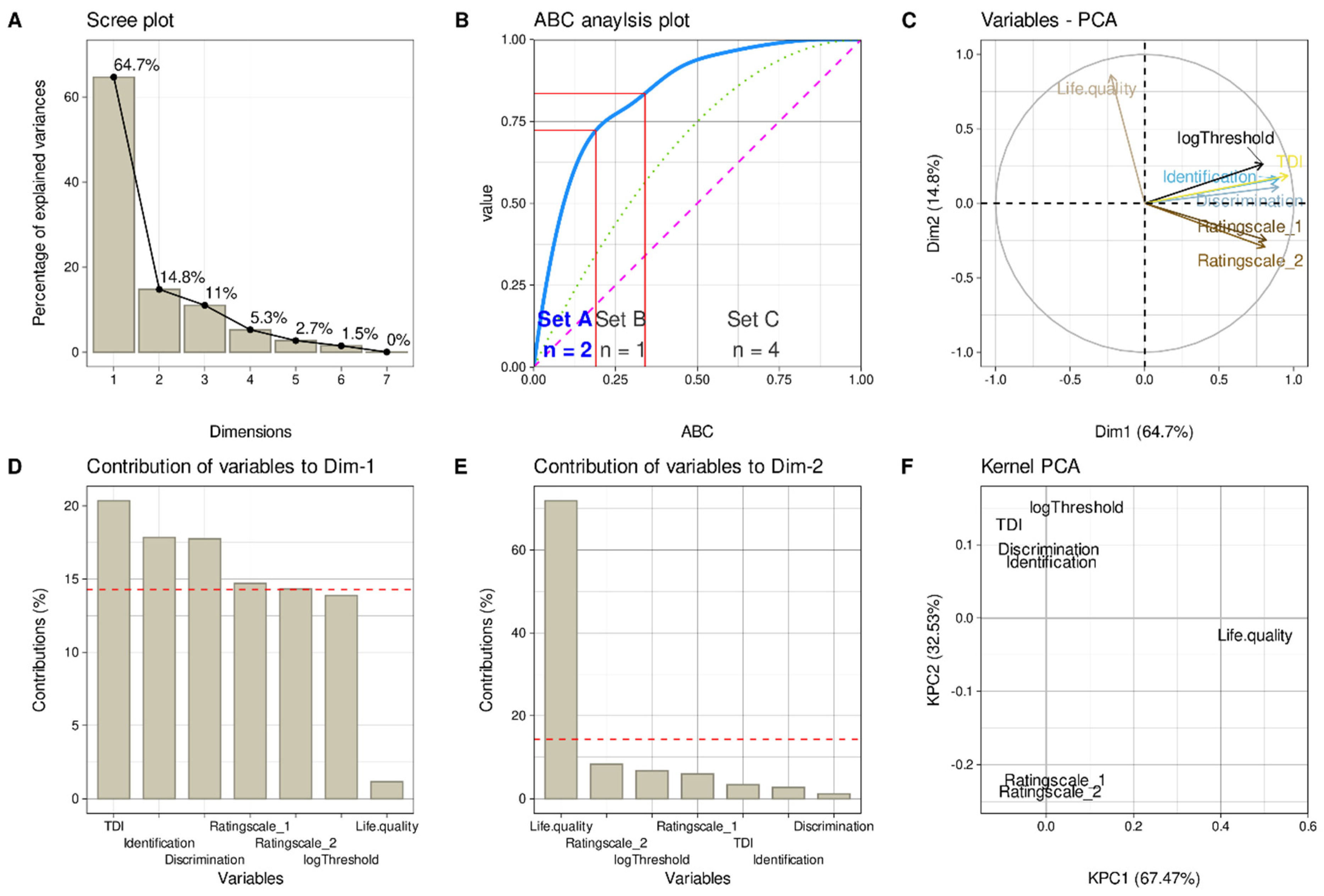
3.3. Pattern of Olfactory Tests and Self-Ratings
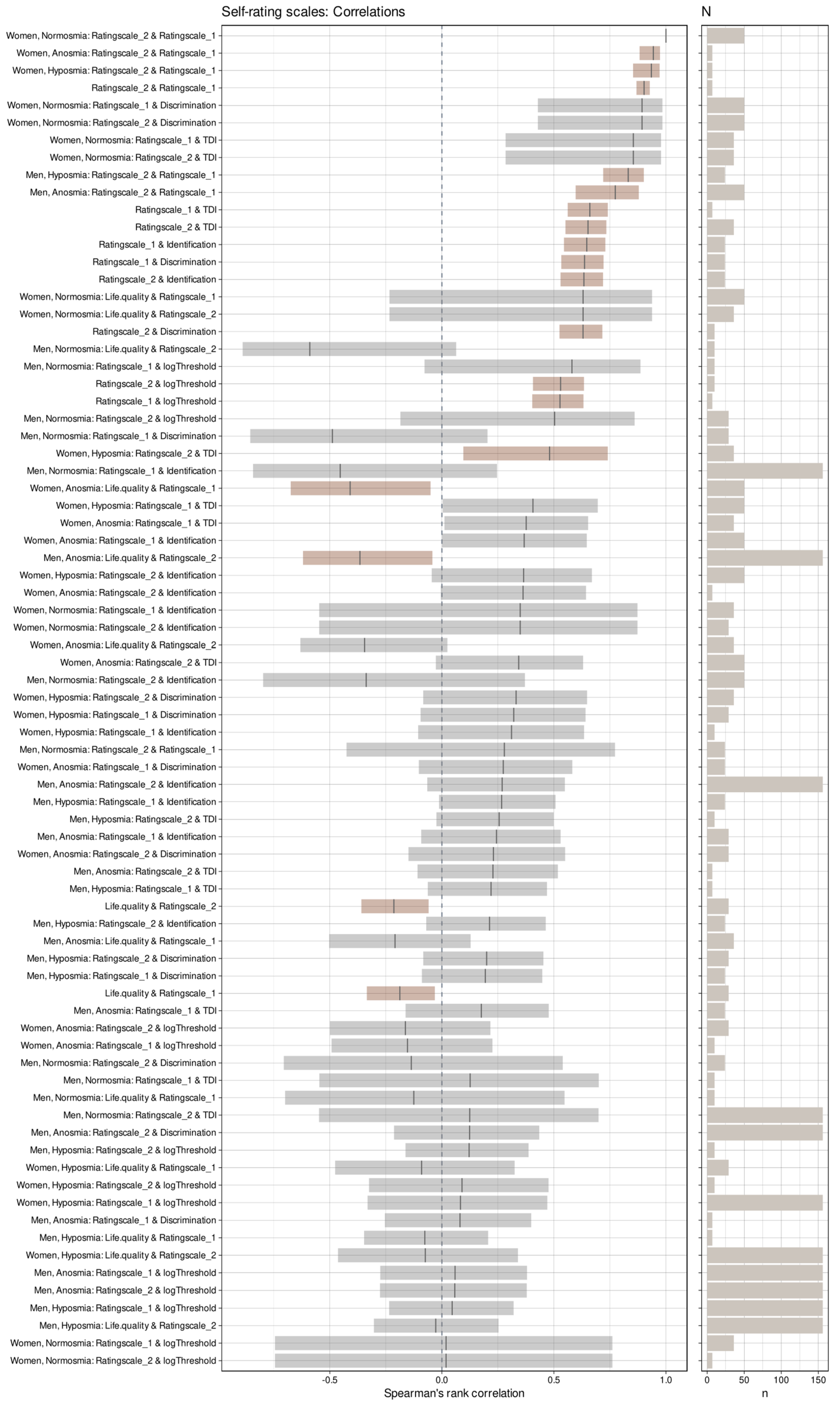
3.4. Correlations of Olfactory Tests and Self-Ratings
3.5. Utility of Self-Ratings for Olfactory Diagnosis Establishment
4. Discussion
4.1. Key Results
4.2. Strengths and Limitations
4.3. Interpretation
4.4. Generalizability
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nguyen, D.T.; Nguyen-Thi, P.L.; Jankowski, R. How Does Measured Olfactory Function Correlate with Self-Ratings of the Sense of Smell in Patients with Nasal Polyposis? Laryngoscope 2012, 122, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, F.S.; Hilgers, F.J.; Emsbroek, G.; Touw, F.I.; van As, C.J.; de Jong, N. Deterioration of Olfaction and Gustation As a Consequence of Total Laryngectomy. Laryngoscope 1999, 109, 1150–1155. [Google Scholar] [CrossRef]
- Landis, B.N.; Hummel, T.; Hugentobler, M.; Giger, R.; Lacroix, J.S. Ratings of Overall Olfactory Function. Chem. Senses 2003, 28, 691–694. [Google Scholar] [CrossRef] [Green Version]
- Cameron, E.L. Measures of Human Olfactory Perception During Pregnancy. Chem. Senses 2007, 32, 775–782. [Google Scholar] [CrossRef] [Green Version]
- Leon, E.A.; Catalanotto, F.A.; Werning, J.W. Retronasal and Orthonasal Olfactory Ability After Laryngectomy. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 32–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knaapila, A.; Tuorila, H.; Kyvik, K.O.; Wright, M.J.; Keskitalo, K.; Hansen, J.; Kaprio, J.; Perola, M.; Silventoinen, K. Self-Ratings of Olfactory Function Reflect Odor Annoyance Rather Than Olfactory Acuity. Laryngoscope 2008, 118, 2212–2217. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.H.; Chu, S.T.; Yuan, B.C.; Shu, C.H. Survey of the Frequency of Olfactory Dysfunction in Taiwan. J. Chin. Med. Assoc. 2009, 72, 68–71. [Google Scholar] [CrossRef] [Green Version]
- Shu, C.H.; Hummel, T.; Lee, P.L.; Chiu, C.H.; Lin, S.H.; Yuan, B.C. The Proportion of Self-Rated Olfactory Dysfunction Does Not Change Across the Life Span. Am. J. Rhinol. Allergy 2009, 23, 413–416. [Google Scholar] [CrossRef]
- Seo, H.S.; Guarneros, M.; Hudson, R.; Distel, H.; Min, B.C.; Kang, J.K.; Croy, I.; Vodicka, J.; Hummel, T. Attitudes Toward Olfaction: A Cross-Regional Study. Chem. Senses 2011, 36, 177–187. [Google Scholar] [CrossRef]
- Trellakis, S.; Tagay, S.; Fischer, C.; Rydleuskaya, A.; Scherag, A.; Bruderek, K.; Schlegl, S.; Greve, J.; Canbay, A.E.; Lang, S.; et al. Ghrelin, Leptin and Adiponectin As Possible Predictors of the Hedonic Value of Odors. Regul. Pept. 2011, 167, 112–117. [Google Scholar] [CrossRef]
- Lötsch, J.; Kraetsch, H.G.; Wendler, J.; Hummel, T. Self-Ratings of Higher Olfactory Acuity Contrast with Reduced Olfactory Test Results of Fibromyalgia Patients. Int. J. Psychophysiol. 2012, 86, 182–186. [Google Scholar] [CrossRef]
- Cameron, E.L. Pregnancy Does Not Affect Human Olfactory Detection Thresholds. Chem. Senses 2014, 39, 143–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollndorfer, K.; Kowalczyk, K.; Nell, S.; Krajnik, J.; Mueller, C.A.; Schöpf, V. The Inability to Self-Evaluate Smell Performance. How the Vividness of Mental Images Outweighs Awareness of Olfactory Performance. Front. Psychol. 2015, 6, 627. [Google Scholar] [CrossRef] [Green Version]
- Sorokowska, A.; Schriever, V.A.; Gudziol, V.; Hummel, C.; Hähner, A.; Iannilli, E.; Sinding, C.; Aziz, M.; Seo, H.S.; Negoias, S.; et al. Changes of Olfactory Abilities in Relation to Age: Odor Identification in More Than 1400 People Aged 4 to 80 Years. Eur. Arch. Otorhinolaryngol. 2015, 272, 1937–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasunla, A.J.; Daniel, A.; Nwankwo, U.; Kuti, K.M.; Nwaorgu, O.G.; Akinyinka, O.O. Evaluation of Olfactory and Gustatory Function of HIV Infected Women. AIDS Res. Treat. 2016, 2016, 2045383. [Google Scholar] [CrossRef] [PubMed]
- Galletti, B.; Santoro, R.; Mannella, V.K.; Caminiti, F.; Bonanno, L.; De Salvo, S.; Cammaroto, G.; Galletti, F. Olfactory Event-Related Potentials: A New Approach for the Evaluation of Olfaction in Nasopharyngeal Carcinoma Patients Treated with Chemo-Radiotherapy. J. Laryngol. Otol. 2016, 130, 453–461. [Google Scholar] [CrossRef]
- Knaapila, A.; Raittola, A.; Sandell, M.; Yang, B. Self-Ratings of Olfactory Performance and Odor Annoyance Are Associated with the Affective Impact of Odor, but Not with Smell Test Results. Perception 2017, 46, 352–365. [Google Scholar] [CrossRef]
- Seok, J.; Shim, Y.J.; Rhee, C.S.; Kim, J.W. Correlation Between Olfactory Severity Ratings Based on Olfactory Function Test Scores and Self-Reported Severity Rating of Ol-Factory Loss. Acta Otolaryngol. 2017, 137, 750–754. [Google Scholar] [CrossRef]
- Chen, G.; Pan, H.; Li, L.; Wang, J.; Zhang, D.; Wu, Z. Olfactory Assessment in the Chinese Pediatric Population. Medicine 2018, 97, e0464. [Google Scholar] [CrossRef] [PubMed]
- Lötsch, J.; Hummel, T. Clinical Usefulness of Self-Rated Olfactory Performance-A Data Science-Based Assessment of 6000 Patients. Chem. Senses 2019. [Google Scholar] [CrossRef]
- Bogdanov, V.; Walliczek-Dworschak, U.; Whitcroft, K.L.; Landis, B.N.; Hummel, T. Response to Glucocorticosteroids Predicts Olfactory Outcome After ESS in Chronic Rhinosinusitis. Laryngoscope 2020, 130, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.T.; Besser, G.; Prem, B.; Sharma, G.; Koenighofer, M.; Renner, B.; Mueller, C.A. Association Between Orthonasal Olfaction and Chemosensory Perception in Patients with Smell Loss. Laryngoscope 2020, 130, 2213–2219. [Google Scholar] [CrossRef]
- Oleszkiewicz, A.; Hummel, T. Whose Nose Does Not Know? Demographical Characterization of People Unaware of Anosmia. Eur. Arch. Otorhinolaryngol. 2019, 276, 1849–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oleszkiewicz, A.; Kunkel, F.; Larsson, M.; Hummel, T. Consequences of Undetected Olfactory Loss for Human Chemosensory Communication and Well-Being. Philos. Trans. R. Soc. B 2020, 375, 20190265. [Google Scholar] [CrossRef] [PubMed]
- Kobal, G.; Hummel, T.; Sekinger, B.; Barz, S.; Roscher, S.; Wolf, S.R. “Sniffin’ Sticks”: Screening of Olfactory Performance. Rhinology 1996, 34, 222–226. [Google Scholar]
- Hummel, T.; Sekinger, B.; Wolf, S.R.; Pauli, E.; Kobal, G. ‘Sniffin’ Sticks’: Olfactory Performance Assessed by the Combined Testing of Odor Identification, Odor Discrimination and Olfactory Threshold. Chem. Senses 1997, 22, 39–52. [Google Scholar] [CrossRef]
- Oleszkiewicz, A.; Schriever, V.A.; Croy, I.; Hahner, A.; Hummel, T. Updated Sniffin’ Sticks Normative Data Based on an Extended Sample of 9139 Subjects. Eur. Arch. Otorhinolaryngol. 2019, 276, 719–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccirillo, J.F.; Merritt, M.G., Jr.; Richards, M.L. Psychometric and Clinimetric Validity of the 20-Item Sino-Nasal Outcome Test (SNOT-20). Otolaryngol. Head Neck Surg. 2002, 126, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Lötsch, J.; Geisslinger, G.; Hummel, T. Sniffing Out Pharmacology: Interactions of Drugs With Human Olfaction. Trends Pharmacol. Sci. 2012, 33, 193–199. [Google Scholar] [CrossRef]
- Lötsch, J.; Daiker, H.; Hähner, A.; Ultsch, A.; Hummel, T. Drug-Target Based Cross-Sectional Analysis of Olfactory Drug Effects. Eur. J. Clin. Pharmacol. 2015, 71, 461–471. [Google Scholar] [CrossRef]
- Ihaka, R.; Gentleman, R. R: A Language for Data Analysis and Graphics. J. Comput. Graph. Stat. 1996, 5, 299–314. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 20 May 2021).
- Kassambara, A. rstatix: Pipe-Friendly Framework for Basic Statistical Tests. 2021. Available online: https://CRAN.R-project.org/package=rstatix (accessed on 20 May 2021).
- Wickham, H.; Seidel, D. scales: Scale Functions for Visualization. 2020. Available online: https://CRAN.R-project.org/package=scales (accessed on 20 May 2021).
- Hotelling, H. Analysis of a Complex of Statistical Variables Into Principal Components. J. Educ. Psychol. 1933, 24, 498–520. [Google Scholar] [CrossRef]
- Pearson, K. LIII. On Lines and Planes of Closest Fit to Systems of Points in Space. Lond. Edinb. Dublin Philos. Mag. J. Sci. 1901, 2, 559–572. [Google Scholar] [CrossRef] [Green Version]
- Le, S.; Josse, J.; Husson, F. FactoMineR: A Package for Multivariate Analysis. J. Stat. Softw. 2008, 25, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Ultsch, A.; Lötsch, J. Computed ABC Analysis for Rational Selection of Most Informative Variables in Multivariate Data. PLoS ONE 2015, 10, e0129767. [Google Scholar] [CrossRef] [Green Version]
- Juran, J.M. The Non-Pareto Principle; Mea Culpa. Qual. Prog. 1975, 8, 8–9. [Google Scholar]
- Kaiser, H.F. The Varimax Criterion for Analytic Rotation in Factor Analysis. Psychometrika 1958, 23, 187–200. [Google Scholar] [CrossRef]
- Guttman, L. Some Necessary Conditions for Common Factor Analysis. Psychometrika 1954, 19, 149–161. [Google Scholar] [CrossRef]
- Linting, M.; van der Kooij, A. Nonlinear Principal Components Analysis With CATPCA: A Tutorial. J. Personal. Assess. 2012, 94, 12–25. [Google Scholar] [CrossRef]
- Karatzoglou, A.; Smola, A.; Hornik, K.; Zeileis, A. Kernlab–An S4 Package for Kernel Methods in R. J. Stat. Softw. 2004, 11, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Spearman, C. The Proof and Measurement of Association Between Two Things. Am. J. Psychol. 1904, 15, 72–101. [Google Scholar] [CrossRef]
- Schloerke, B.; Crowley, J.; Cook, D.; Briatte, F.; Marbach, M.; Thoen, E.; Elberg, A.; Larmarange, J. GGally: Extension to ‘ggplot2’. Available online: https://CRAN.R-project.org/package=GGally (accessed on 20 May 2021).
- Rushworth, A. Inspectdf: Inspection, Comparison and Visualisation of Data Frames. R package version. Available online: https://CRAN.R-project.org/package=inspectdf (accessed on 20 May 2021).
- Brodersen, K.H.; Ong, C.S.; Stephan, K.E.; Buhmann, J.M. The Balanced Accuracy and Its Posterior Distribution. In Proceedings of the 20th International Conference on Pattern Recognition (ICPR), Istanbul, Turkey, 23–26 August 2010; pp. 3121–3124. [Google Scholar]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; Chapman and Hall: San Francisco, CA, USA, 1995. [Google Scholar]
- Altman, D.G.; Bland, J.M. Diagnostic Tests. 1: Sensitivity and Specificity. BMJ 1994, 308, 1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, D.G.; Bland, J.M. Diagnostic Tests 2: Predictive Values. BMJ 1994, 309, 102. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, T.J. A Method of Establishing Groups of Equal Amplitude in Plant Sociology Based on Similarity of Species Content and Its Application to Analyses of the Vegetation on Danish Commons. Biol. Skar. 1948, 5, 1–34. [Google Scholar]
- Jardine, N.; van Rijsbergen, C.J. The Use of Hierarchic Clustering in Information Retrieval. Inf. Storage Retr. 1971, 7, 217–240. [Google Scholar] [CrossRef]
- Kuhn, M. Caret: Classification and Regression Training. Astrophys. Source Code Libr. 2018, 1505. Available online: https://cran.r-project.org/package=caret (accessed on 20 May 2021).
- Kassambara, A. ggpubr: ‘ggplot2’ Based Publication Ready Plots. 2020. Available online: https://cran.r-project.org/package=ggpubr (accessed on 20 May 2021).
- Arnold, J.B. ggthemes: Extra Themes, Scales and Geoms for ‘ggplot2’. 2019. Available online: https://cran.r-project.org/package=ggthemes (accessed on 20 May 2021).
- Greenhouse, S.W.; Geisser, S. On Methods in the Analysis of Profile Data. Psychometrika 1959, 24, 95–112. [Google Scholar] [CrossRef]
- Thomas, J.D.; Bradley, E. Bootstrap Confidence Intervals. Stat. Sci. 1996, 11, 189–228. [Google Scholar] [CrossRef]
- Watson, D. Bioplotr: Pretty, Simple, Optionally Interactive Plots for Bioinformatics Analysis Pipelines. 2021. Available online: https://github.com/dswatson/bioplotr (accessed on 20 May 2021).
- Katz, M.H. Multivariable Analysis: A Practical Guide for Clinicians, 2nd ed.; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position Paper on Olfactory Dysfunction. Rhinol. Suppl. 2017, 54, 1–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hummel, T.; Nordin, S. Olfactory Disorders and Their Consequences for Quality of Life. Acta Otolaryngol. 2005, 125, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Smeets, M.A.M.; Veldhuizen, M.G.; Galle, S.; Gouweloos, J.; de Haan, A.J.A.; Vernooij, J.; Visscher, F.; Kroeze, J.H.A. Sense of Smell Disorder and Health-Related Quality of Life. Rehabil. Psychol. 2009, 54, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Y.; Karakas, Z.; Uzun, B.; Sen, C.; Comoglu, S.; Orhan, K.S.; Aydogdu, S.; Karagenc, A.O.; Tugcu, D.; Karaman, S.; et al. Olfactory Dysfunction and Quality of Life in Patients with Transfusion-Dependent Thalassemia. Eur. Arch. Otorhinolaryngol. 2017, 274, 3417–3421. [Google Scholar] [CrossRef] [PubMed]
- Croy, I.; Nordin, S.; Hummel, T. Olfactory Disorders and Quality of Life–An Updated Review. Chem. Senses 2014, 39, 185–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, L.Q.; Hummel, T.; Otte, M.S.; Bitter, T.; Besser, G.; Mueller, C.A.; Welge-Lussen, A.; Bulut, O.C.; Goktas, O.; Negoias, S.; et al. Association Between Olfactory Function and Quality of Life in Patients with Olfactory Disorders: A Multicenter Study in Over 760 Participants. Rhinology 2021, 59, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Mattos, J.L.; Schlosser, R.J.; Storck, K.A.; Soler, Z.M. Understanding the Relationship Between Olfactory-Specific Quality of Life, Objective Olfactory Loss, and Patient Factors in Chronic Rhinosinusitis. Int. Forum Allergy Rhinol. 2017, 7, 734–740. [Google Scholar] [CrossRef]
- Hefner, R.; Togerson, W.S. Theory and Methods of Scaling. Behav. Sci. 1959, 4, 245–247. [Google Scholar] [CrossRef]
- Madany Mamlouk, A.; Chee-Ruiter, C.; Hofmann, U.G.; Bower, J.M. Quantifying Olfactory Perception: Mapping Olfactory Perception Space by Using Multidimensional Scaling and Self-Organizing Maps. Neurocomputing 2003, 52, 591–597. [Google Scholar] [CrossRef]
- Seo, H.S.; Lee, S.; Cho, S. Relationships between Personality Traits and Attitudes Toward the Sense of Smell. Front. Psychol. 2013, 4, 901. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, R.J.; Attuquayefio, T. Human Olfactory Consciousness and Cognition: Its Unusual Features May Not Result from Unusual Functions but From Limited Neocortical Processing Resources. Front. Psychol. 2013, 4, 819. [Google Scholar] [CrossRef] [Green Version]
- Smeets, M.A.M.; Schifferstein, H.N.J.; Boelema, S.R.; Lensvelt-Mulders, G. The Odor Awareness Scale: A New Scale for Measuring Positive and Negative Odor Awareness. Chem. Senses 2008, 33, 725–734. [Google Scholar] [CrossRef] [Green Version]



| Reference | Subjects [n] (Total Sample) | Setting | Rating Scale | Olfactory Test | Verdict |
|---|---|---|---|---|---|
| [2] | 63 | Laryngectomy | 7-point NRS | Threshold (PEA), discrimination (8 odors) | High correlation |
| [3] | 60 and 23 | Healthy volunteers | VAS | Threshold, discrimination, identification (Sniffin’ Sticks) | No correlation (n = 60) or present correlation (n = 23) |
| [4] | 100 | Pregnant women | 7-point NRS | Identification (UPSIT) | No correlation |
| [5] | 36 | Healthy volunteers | VAS | Identification (n-butanol), 10-item identification (CCCRC) | Good correlation |
| [6] | 1311 | Twins, general population | 7-point NRS | Identification (6 odors) | No correlation |
| [7] | 211 | General population | 5-point NRS, VAS | Identification (16 odors) | Weak correlation |
| [8] | 1005 | General population | 4-point NRS, VAS | Identification (16 odors) | No correlation |
| [9] | 1082 | General population | 5-point NRS | None | - |
| [10] | 31 | Healthy volunteers | VAS | Threshold, discrimination, identification (Sniffin’ Sticks) | Not tested |
| [11] | 31 | Fibromyalgia | 3-point NRS | Threshold, discrimination, identification (Sniffin’ Sticks) | Poor correlation |
| [1] | 80 | Nasal polyposis | VAS based DyNaChron questionnaire | Threshold (n-butanol), identification (16 odors) | Strong correlation |
| [12] | Pregnant women | 9-point NRS | Threshold (PEA), | Poor agreement | |
| [13] | 75 | Patients with olfactory dysfunction | 9-point NRS | Threshold, discrimination, identification (Sniffin’ Sticks) | No correlation |
| [14] | 1422 | General population and olfactory dysfunction | 5-point NRS | Identification (16 odors) | Low but significant correlation |
| [15] | 162 | HIV infection | 1-point NRS | Threshold, discrimination, identification (Sniffin’ Sticks) | Self-ratings and test results differed |
| [16] | 9 | Nasopharyngeal carcinoma | 10-point NRS, 6-point NRS | Olfactory event-related potentials | Significant correlation |
| [17] | 117 (44 tested) | General population | 7-point NRS | Identification (14 odors) | No correlation |
| [18] | 1555 | Olfactory loss | 5-point NRS | Threshold (n-butanol), Identification (CCSIT) | Significant correlation |
| [19] | 193 | Children | Questionnaire | Discrimination, identification (Sniffin’ Sticks), Threshold (5 odors; T&T) | No correlation |
| [20] | 6049 | General population and olfactory dysfunction | 5-point numerical | 12-item odor identification | Moderate agreement |
| [21] | 52 | Nasal polyposis | 10-point NRS | Threshold, discrimination, identification (Sniffin’ Sticks) | High correlation |
| [22] | 203 | Olfactory dysfunction | 10-point NRS | Threshold, discrimination, identification (Sniffin’ Sticks) | Weak significant correlation |
| Parameter | Three Diagnoses | Anosmia | Hyposmia | Normosmia | Three Diagnoses | Anosmia | Hyposmia | Normosmia |
|---|---|---|---|---|---|---|---|---|
| Men | Women | |||||||
| Rating scale 1 | ||||||||
| Sensitivity, recall | 60 (29.4–87.2) | 75.7 (60.6–87.5) | 42 (28.6–55.1) | 60 (25–90) | 59.3 (41.2–90) | 58.3 (45.3–72.3) | 54.1 (39.5–69.1) | 71.4 (40–100) |
| Specificity | 78.1 (61.9–88.7) | 80 (69.4–90.3) | 72.2 (58.5–84.5) | 80.2 (72–88.8) | 76.8 (60.8–100) | 96.7 (90.7–100) | 69.2 (57.6–81) | 75.3 (66.3–83.9) |
| Positive predictive value, precision | 59.5 (13–80) | 69.2 (55.3–83.8) | 61.5 (44.4–76.9) | 25 (8.7–44.5) | 53.9 (16.1–100) | 95 (84–100) | 53.8 (38.9–69.2) | 26.9 (12.5–44.4) |
| Negative predictive value | 84.4 (44.6–98.5) | 84.5 (73.9–92.2) | 53 (41.4–65.7) | 94.7 (88.6–98.7) | 74.1 (59.7–98.6) | 71.4 (60.6–81.5) | 69.4 (57.6–79.7) | 95.5 (90–100) |
| F1 | 51.1 (20–80) | 72 (60–82.1) | 50 (36.1–61.2) | 35.9 (14.3–55.8) | 54.5 (25–80.6) | 72.4 (60.6–83) | 53.8 (40.6–66) | 38.9 (19.3–57.1) |
| Balanced Accuracy | 69.5 (49.5–84.6) | 77.5 (68.8–85.5) | 56.8 (47–65.7) | 70.4 (53–86.1) | 72 (54.6–85.1) | 77.7 (70.4–85.2) | 61.7 (52.4–71) | 73.3 (58.4–87.5) |
| Rating scale 2 | ||||||||
| Sensitivity, recall | 59.3 (26.6–94.3) | 86.7 (74.2–97.1) | 54 (38.9–68.3) | 50 (18.2–81.8) | 70.6 (33.3–92.9) | 82.9 (71.4–93.2) | 45.5 (29.7–61.9) | 71.4 (40–100) |
| Specificity | 80.9 (65.6–95.5) | 75 (63.8–85.7) | 78.7 (65.8–88.9) | 90.9 (84–96.6) | 82.6 (69.6–98.4) | 80.5 (69.4–91.1) | 94.8 (87.9–100) | 77.3 (68.5–85.5) |
| Positive predictive value, precision | 65.2 (20–83.3) | 67.3 (54.3–80.5) | 73.5 (57.8–87.1) | 38.5 (12.5–66.7) | 77.3 (16.7–95.7) | 80 (68–90.2) | 85 (66.7–100) | 28.2 (13.8–45.5) |
| Negative predictive value | 89.8 (52.2–97.8) | 90.6 (81.1–98) | 61 (48.5–72.9) | 94.2 (88.5–97.8) | 83.3 (64.8–98.6) | 83.3 (73.1–93.8) | 72.4 (62–81) | 95.7 (90–100) |
| F1 | 62.9 (23.5–82.7) | 75.7 (65.1–84.4) | 62.1 (48.2–73.3) | 42.9 (17.4–66.7) | 59.5 (26.1–87.5) | 81.3 (72.1–89.1) | 59.1 (43.1–73.4) | 40.8 (20.5–58.5) |
| Balanced Accuracy | 72.1 (56.5–86.7) | 80.6 (72.5–87.8) | 66.3 (56.6–75) | 70.3 (54.4–86) | 75.3 (61.5–88.1) | 81.9 (73.9–89.3) | 70 (61.7–78.6) | 74.2 (58.9–88.2) |
| Combined rating scales 1 and 2 | ||||||||
| Sensitivity, recall | 66.7 (26.6–85.3) | 75.7 (60.6–87.5) | 66 (52.2–78.7) | 50 (18.2–81.8) | 70.6 (33.3–92.9) | 82.9 (71.4–93.2) | 45.5 (29.7–61.9) | 71.4 (40–100) |
| Specificity | 84.6 (59.6–95.5) | 84.9 (75–93.2) | 69.8 (56.2–81.8) | 90.9 (84–96.6) | 82.6 (69.6–98.4) | 80.5 (69.4–91.1) | 94.8 (87.9–100) | 77.3 (68.5–85.5) |
| Positive predictive value, precision | 68.1 (20–85) | 75 (60.5–88.6) | 70.2 (56.5–82.1) | 38.5 (12.5–66.7) | 77.3 (16.7–95.7) | 80 (68–90.2) | 85 (66.7–100) | 28.2 (13.8–45.5) |
| Negative predictive value | 85.1 (55.6–97.6) | 85.2 (75.4–92.6) | 65.3 (51.1–78.3) | 94.2 (88.5–97.8) | 83.3 (64.8–98.6) | 83.3 (73.1–93.8) | 72.4 (62–81) | 95.7 (90–100) |
| F1 | 67 (23.5–82.2) | 75 (63.4–84.8) | 68 (56–77.2) | 42.9 (17.4–66.7) | 59.5 (26.1–87.5) | 81.3 (72.1–89.1) | 59.1 (43.1–73.4) | 40.8 (20.5–58.5) |
| Balanced Accuracy | 72.6 (57.3–86.1) | 80 (72.1–87.4) | 67.8 (58.4–76) | 70.3 (54.4–86) | 75.3 (61.5–88.1) | 81.9 (73.9–89.3) | 70 (61.7–78.6) | 74.2 (58.9–88.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lötsch, J.; Hintschich, C.A.; Petridis, P.; Pade, J.; Hummel, T. Self-Ratings of Olfactory Function and Their Relation to Olfactory Test Scores. A Data Science-Based Analysis in Patients with Nasal Polyposis. Appl. Sci. 2021, 11, 7279. https://doi.org/10.3390/app11167279
Lötsch J, Hintschich CA, Petridis P, Pade J, Hummel T. Self-Ratings of Olfactory Function and Their Relation to Olfactory Test Scores. A Data Science-Based Analysis in Patients with Nasal Polyposis. Applied Sciences. 2021; 11(16):7279. https://doi.org/10.3390/app11167279
Chicago/Turabian StyleLötsch, Jörn, Constantin A. Hintschich, Petros Petridis, Jürgen Pade, and Thomas Hummel. 2021. "Self-Ratings of Olfactory Function and Their Relation to Olfactory Test Scores. A Data Science-Based Analysis in Patients with Nasal Polyposis" Applied Sciences 11, no. 16: 7279. https://doi.org/10.3390/app11167279
APA StyleLötsch, J., Hintschich, C. A., Petridis, P., Pade, J., & Hummel, T. (2021). Self-Ratings of Olfactory Function and Their Relation to Olfactory Test Scores. A Data Science-Based Analysis in Patients with Nasal Polyposis. Applied Sciences, 11(16), 7279. https://doi.org/10.3390/app11167279