
A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Related Works
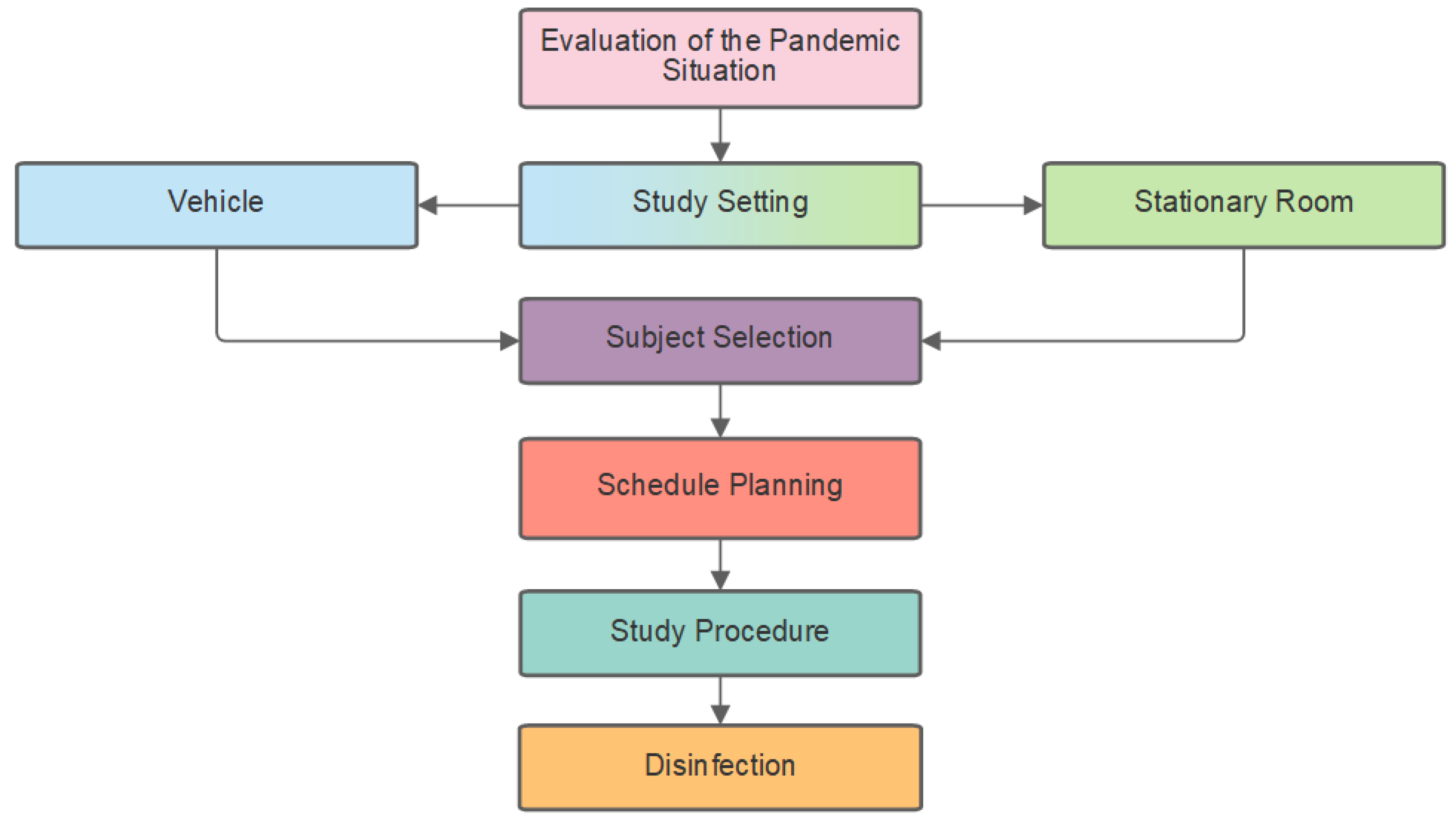
3. Results
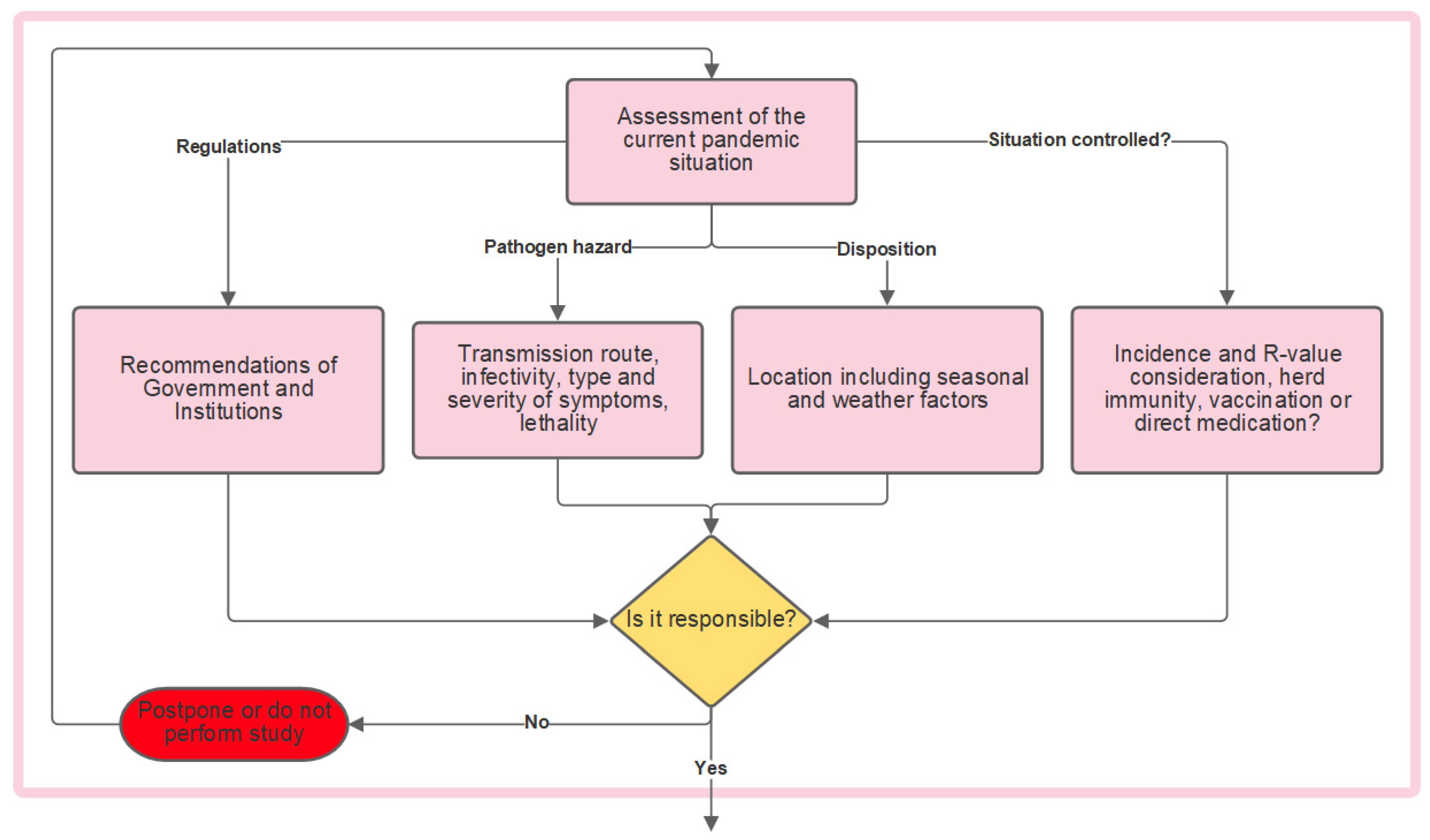
3.1. Evaluation of the Pandemic Situation
3.1.1. Pathogen Hazard
3.1.2. Disposition
3.1.3. Situation Controlled?
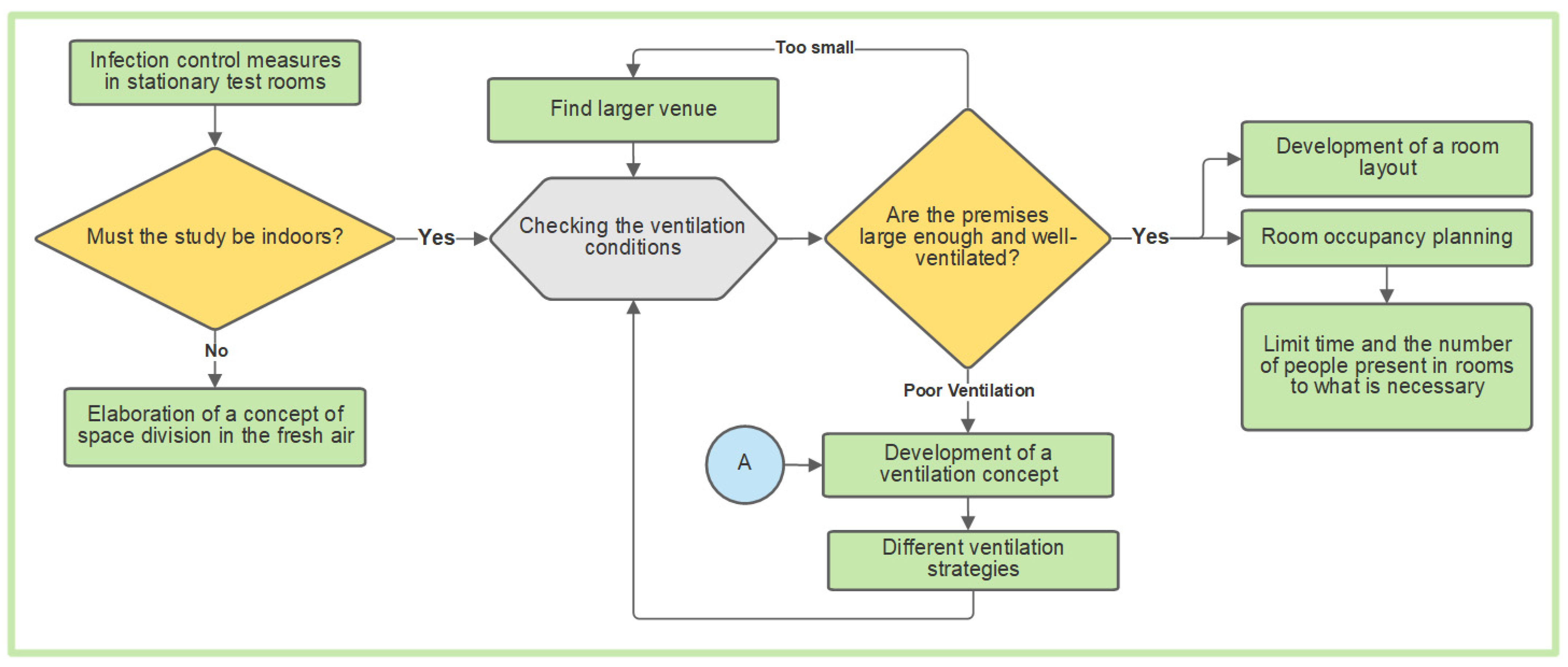
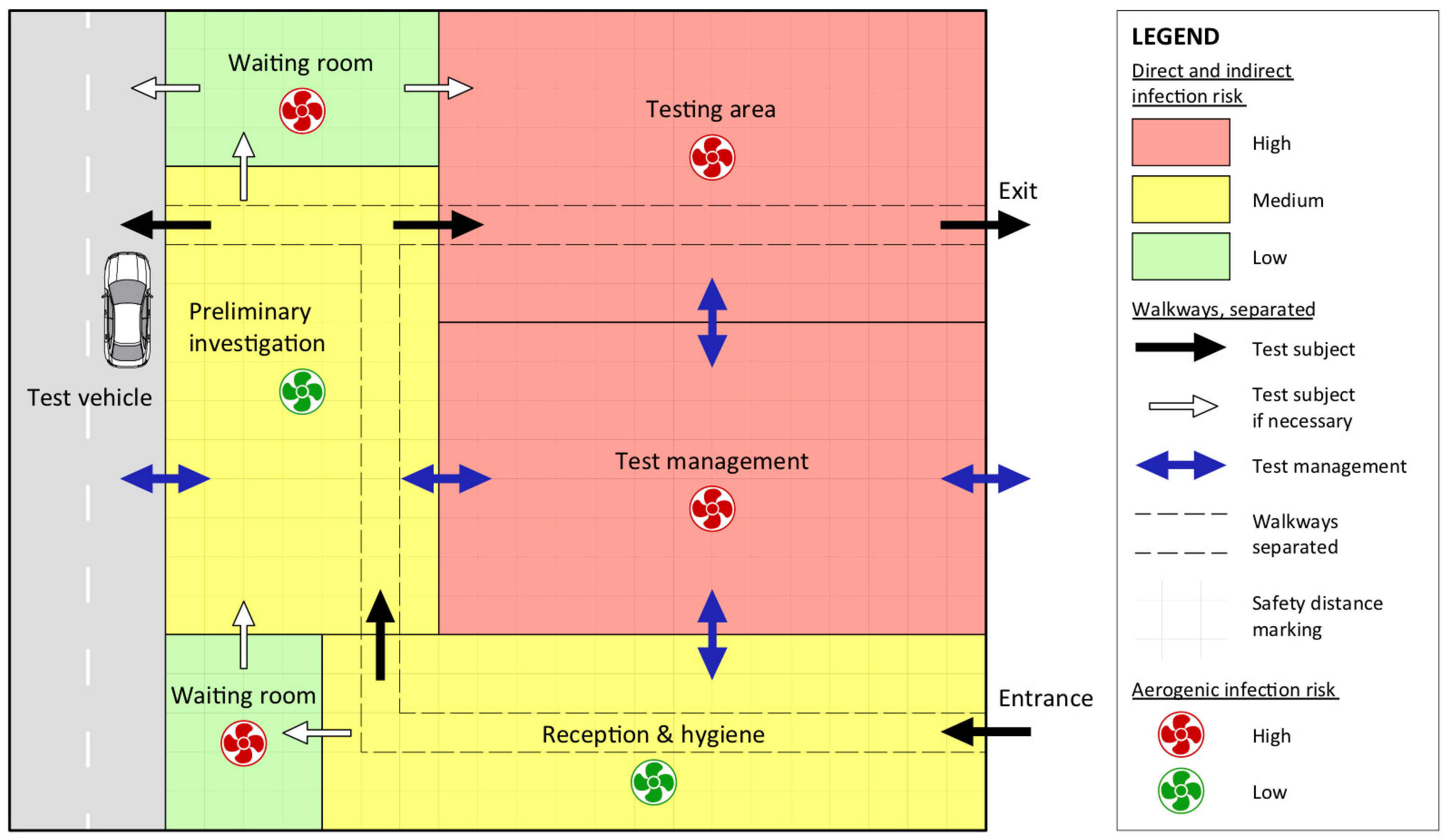
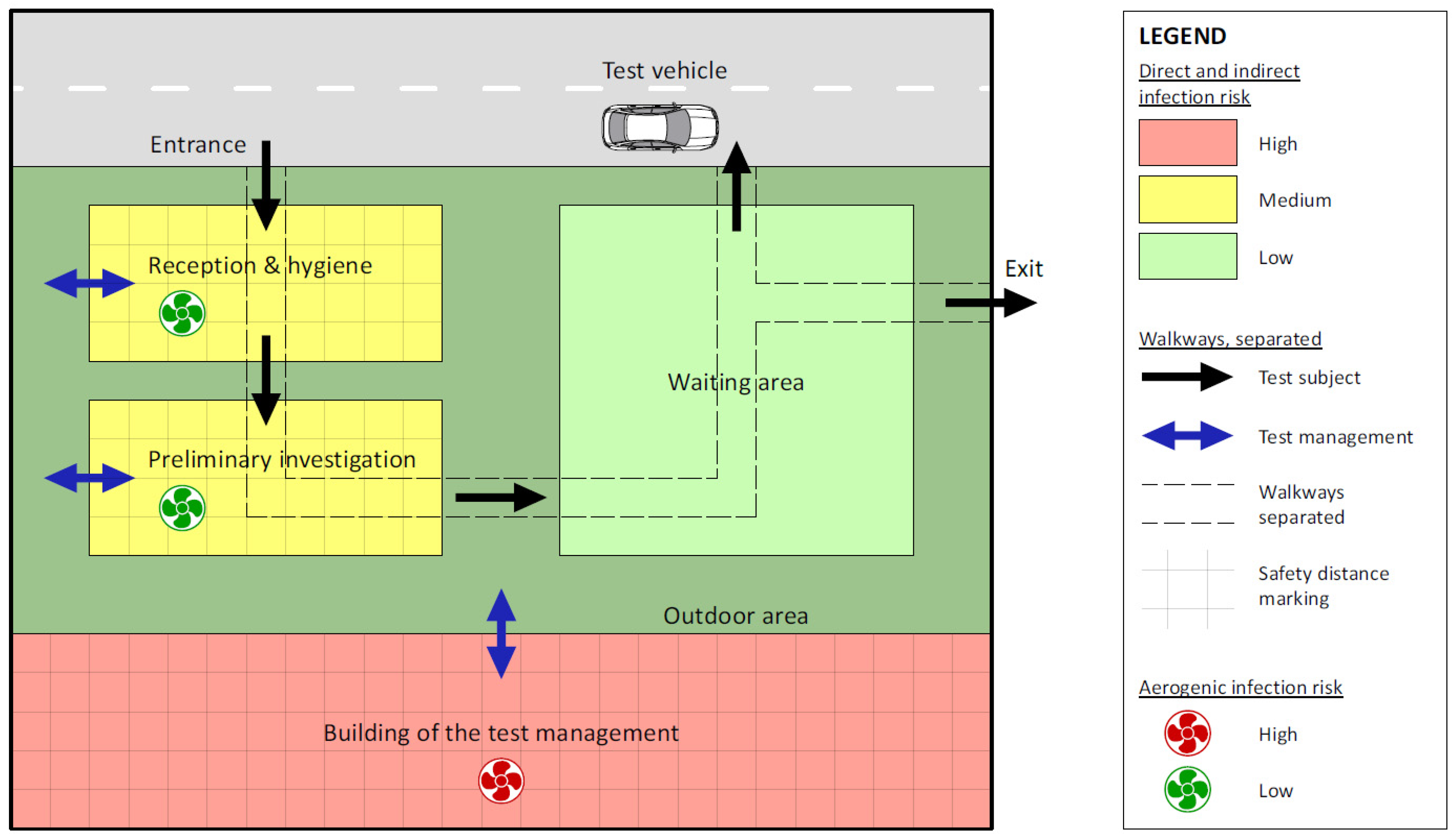
3.2. Infection Protection Measures—Stationary Test Rooms
3.2.1. Stationary Test Rooms—Ventilation Conditions
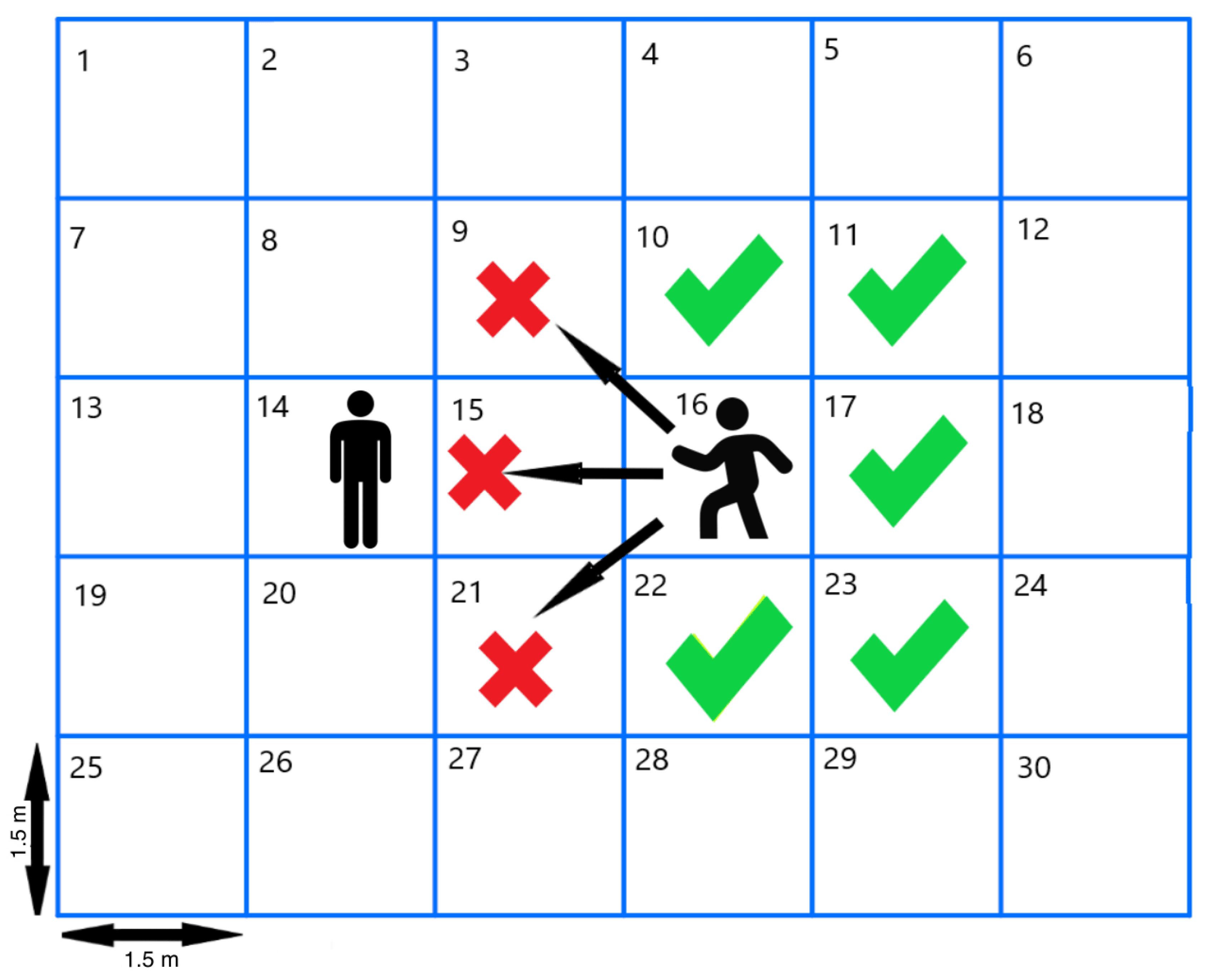
3.2.2. Stationary Test Rooms—Room Occupancy Planning
3.3. Infection Protection Measures—Vehicle
3.3.1. Vehicle Occupancy
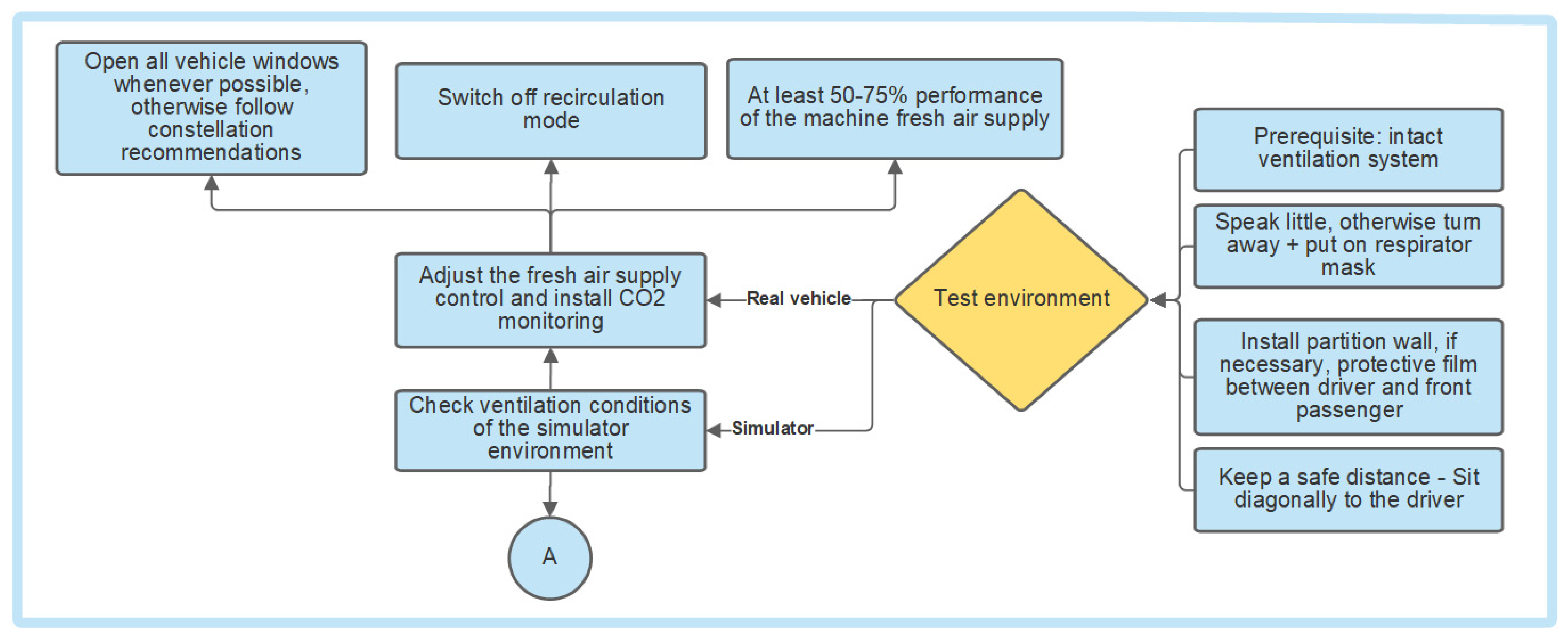
3.3.2. Ventilation in a Vehicle
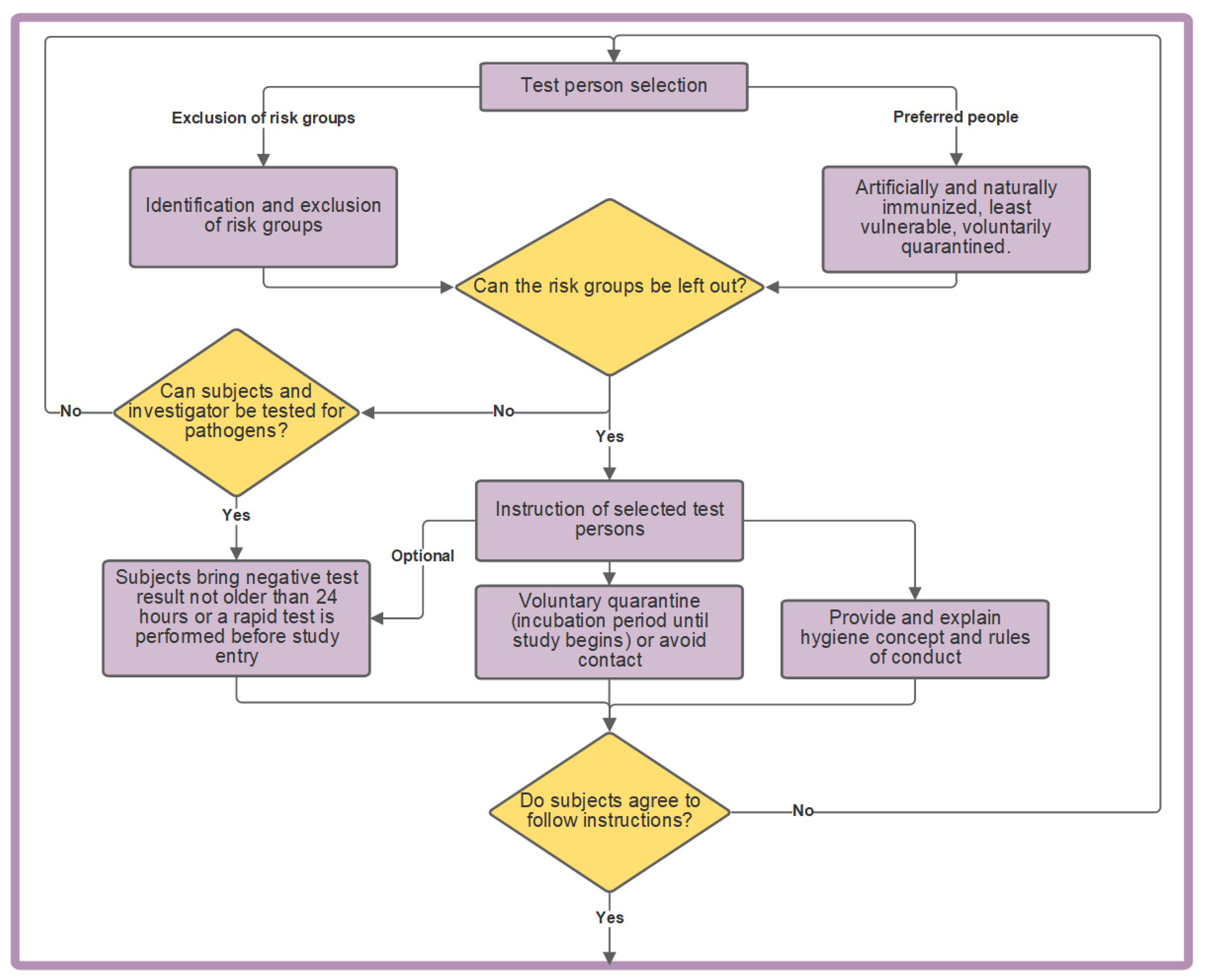
3.4. Subject Selection
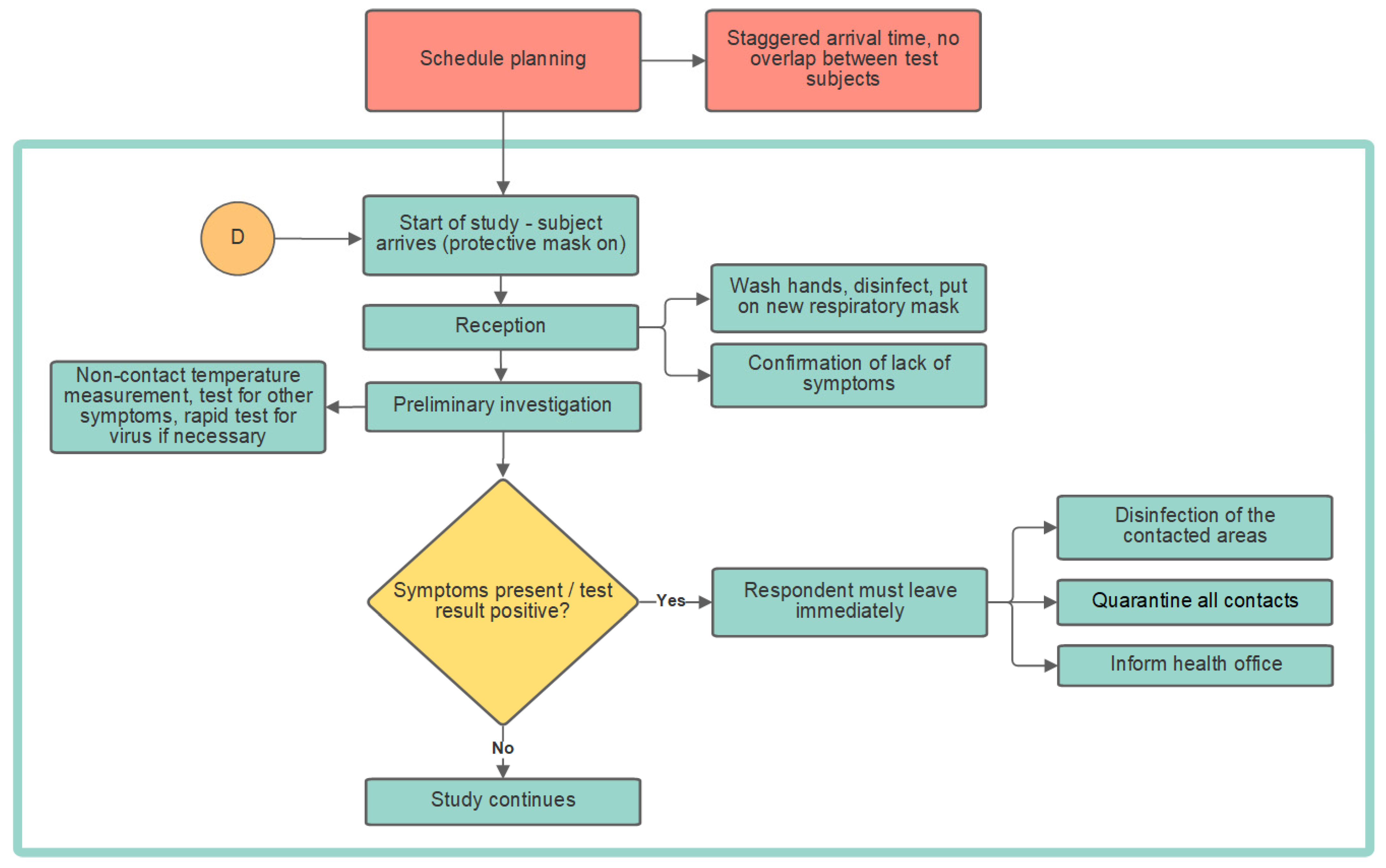
3.5. Conducting the Study
3.5.1. Planning of Test Times
3.5.2. Reception
3.5.3. Preliminary Investigation
3.5.4. During the Experiment
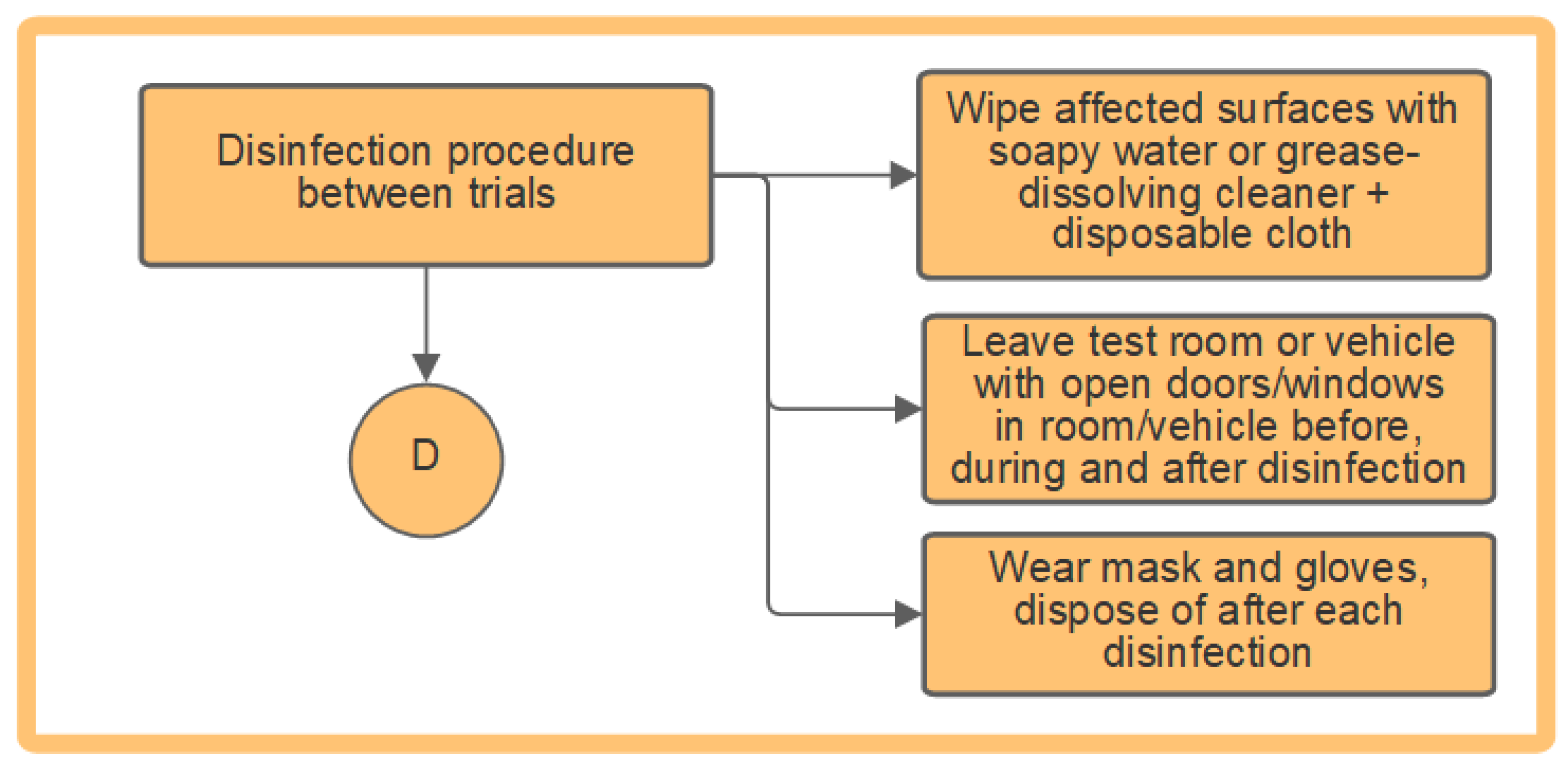
3.6. Disinfection
4. Discussion
5. Conclusions and Future Works
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robert Koch Institut (RKI). Coronavirus SARS-CoV-2: Informationen zur Ausweisung internationaler Risikogebiete Durch das Auswärtige Amt, BMG und BMI. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Risikogebiete_neu.html (accessed on 12 March 2021).
- Technische Universität Dresden. Hygienekonzept für Fahrsimulator-Studie. Available online: https://tu-dresden.de/bu/verkehr/iad/kft/ressourcen/dateien/newsdokumente/202103/EMISA_Hygienekonzept_Coronavirus-Fragebogen.pdf?lang=de (accessed on 23 August 2021).
- Technische Universität Berlin. FAQ zu Aersolen in Bezug auf SARS-CoV-2: Dauerlüften, Luftfilter—Wie Umgehen mit Den Aerosolen in Innenräumen? Available online: https://www.tu.berlin/forschen/themenportal-forschen/2020/august/faq-zu-aersolen-in-bezug-auf-sars-cov-2/ (accessed on 12 March 2021).
- Kriegel, M. Anzahl der mit SARS-CoV-2 beladenen Partikel in der Raumluft und Deren Eingeatmete Menge, sowie die Bewertung des Infektionsrisikos, sich Darüber mit COVID-19 Anzustecken. 2020. Available online: https://depositonce.tu-berlin.de/bitstream/11303/11767.3/9/Virenbeladene_Partikel_im_Raum_v3.pdf (accessed on 12 March 2021).
- Schulze-Röbbecke, R.; Reska, M.; Lemmen, S. Welche Schutzmaske schützt vor COVID-19?: Was ist evidenzbasiert? Krankenhaushygiene up2date 2020, 15, 123–132. [Google Scholar]
- Kriegel, M.; Hartmann, A. COVID-19 Ansteckung über Aerosolpartikel: Vergleichende Bewertung von Innenräumen Hinsichtlich des Situationsbedingten R-Wertes. 2021. Available online: https://depositonce.tu-berlin.de/bitstream/11303/12578/5/kriegel_hartmann_2021.pdf (accessed on 25 April 2021).
- Paschotta, R. Luftwechselrate. Available online: https://www.energie-lexikon.info/luftwechselrate.html#:%7E:text=Die%20Luftwechselrate%20eines%20Raums%20oder,%2Fh%20%3D%20h%E2%88%921 (accessed on 12 March 2021).
- Makoto, T. Prediction and Countermeasures for Infection by Virus Contaminated Droplet in Indoor Environment. Available online: https://www.covid19-ai.jp/en-us/presentation/2020_rq1_droplet_infection_simulation/articles/article003/ (accessed on 12 March 2021).
- Makoto, T. Prediction and Countermeasures for Infection by Virus Contaminated Droplet in Indoor Environment. Available online: https://www.covid19-ai.jp/en-us/presentation/2020_rq1_droplet_infection_simulation/articles/article004/ (accessed on 12 March 2021).
- Pischinger, S.; Seiffert, U. Vieweg Handbuch Kraftfahrzeugtechnik; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2016; ISBN 978-3-658-09527-7. [Google Scholar]
- Sinanovic, A. Durchführung von Probandenstudien während der COVID-19 Pandemie. Bachelorarbeit; Technische Universität Berlin: Berlin, Germany, 2021. [Google Scholar]
- BG-Verkehr. Taxi. Available online: https://www.bg-verkehr.de/coronavirus/tipps-fuer-unternehmen-und-ihre-beschaeftigten/taxi (accessed on 11 March 2021).
- Mathai, V.; Das, A.; Bailey, J.A.; Breuer, K. Airflows inside passenger cars and implications for airborne disease transmission. Sci. Adv. 2021, 7, eabe0166. [Google Scholar] [CrossRef] [PubMed]
- Fruin, S.A.; Hudda, N.; Sioutas, C.; Delfino, R.J. Predictive model for vehicle air exchange rates based on a large, representative sample. Environ. Sci. Technol. 2011, 45, 3569–3575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knibbs, L.D.; Morawska, L.; Bell, S.C. The risk of airborne influenza transmission in passenger cars. Epidemiol. Infect. 2012, 140, 474–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert Koch Institut (RKI). Epidemiologischer Steckbrief zu SARS-CoV-2 und COVID-19. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html;jsessionid=A26AFC1E37AB7F14D92A29479166C41F.internet121?nn=2386228 (accessed on 12 March 2021).
- Robert Koch Institut (RKI). Coronavirus SARS-CoV-2: Informationen und Hilfestellungen für Personen mit einem höheren Risiko für einen schweren COVID-19-Krankheitsverlauf. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Risikogruppen.html (accessed on 12 March 2021).
- Robert Koch Institut (RKI). Warum Treten Grippewellen Immer im Winter auf? Available online: https://www.rki.de/SharedDocs/FAQ/Influenza/FAQ02.html (accessed on 27 April 2021).
- Suttorp, N. (Ed.) Infektionskrankheiten: Verstehen, Erkennen, Behandeln; Thieme: Stuttgart, Germany; New York, NY, USA, 2004; ISBN 9783131877116. [Google Scholar]
- Robert Koch Institut (RKI). Navigation: Virus und Epidemiologie. Available online: https://www.rki.de/SharedDocs/FAQ/NCOV2019/FAQ_Liste_Epidemiologie.html (accessed on 12 March 2021).
- Bundeszentrale für Gesundheitliche Aufklärung (BZgA). Im Alltag Maske Tragen. Available online: https://www.infektionsschutz.de/coronavirus/alltag-in-zeiten-von-corona/im-alltag-maske-tragen.html (accessed on 11 March 2021).
- Kähler, C.; Hain, R. Musizieren während der Pandemie -was rät die Wissenschaft?: Über Infektionsrisiken beim Chorsingen und Musizieren mit Blasinstrumenten. Available online: https://www.unibw.de/lrt7/musizieren_waehrend_der_pandemie.pdf (accessed on 12 March 2021).
- Ahlawat, A.; Wiedensohler, A.; Mishra, S.K. An Overview on the Role of Relative Humidity in Airborne Transmission of SARS-CoV-2 in Indoor Environments. Aerosol. Air Qual. Res. 2020, 20, 1856–1861. [Google Scholar] [CrossRef]
- Bundeszentrale für Gesundheitliche Aufklärung (BZgA). Abstand Halten. Available online: https://www.infektionsschutz.de/coronavirus/alltag-in-zeiten-von-corona/abstand-halten.html#:%7E:text=Achten%20Sie%20im%20%C3%B6ffentlichen%20Raum,Sie%20auf%20H%C3%A4ndesch%C3%BCtteln%20oder%20Umarmungen (accessed on 11 March 2021).
- Bundeszentrale für Gesundheitliche Aufklärung (BZgA). Regelmäßig Lüften. Available online: https://www.infektionsschutz.de/coronavirus/alltag-in-zeiten-von-corona/regelmaessig-lueften.html (accessed on 11 March 2021).
- Xie, X.; Li, Y.; Chwang, A.T.Y.; Ho, P.L.; Seto, W.H. How far droplets can move in indoor environments--revisiting the Wells evaporation-falling curve. Indoor Air 2007, 17, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege (BGW). Medizinische Gesichtsmaske—Mund-Nasen-Schutz (MNS). Available online: https://www.bgw-online.de/DE/Arbeitssicherheit-Gesundheitsschutz/Hygiene_und_Infektionsschutz/Masken/Maske-02_Mund-Nasen-Schutz.html (accessed on 11 March 2021).
- Deutschland. Die Timeline zum Coronavirus in Deutschland: Hier findet ihr die Wichtigsten Entwicklungen zu COVID-19 in Deutschland im Überblick. Available online: https://www.deutschland.de/de/die-timeline-coronavirus-germany-deutschland (accessed on 11 March 2021).
- Heinrich, C.; Collin, C. Corona-Nachweis: Die Testverfahren im Überblick. Available online: https://www.apotheken-umschau.de/krankheiten-symptome/infektionskrankheiten/coronavirus/corona-nachweis-die-testverfahren-im-ueberblick-724147.html#PCR-Schnelltest (accessed on 12 March 2021).
- Ott, W.; Klepeis, N.; Switzer, P. Air change rates of motor vehicles and in-vehicle pollutant concentrations from secondhand smoke. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Seifried, J.; Böttcher, S.; von Kleist, M.; Jenny, M.A.; Antão, E.; Oh, D.Y.; Jung-Sendzik, T.; Broich, K.; Denkinger, C.; Bartenschlager, T.; et al. Antigentests als ergänzendes Instrument in der Pandemiebekämpfung. Epidemiol. Bull. 2021, 17, 3–14. [Google Scholar] [CrossRef]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kantusch, T.; Sinanovic, A.; Marker, S. A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic. Appl. Sci. 2021, 11, 8556. https://doi.org/10.3390/app11188556
Kantusch T, Sinanovic A, Marker S. A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic. Applied Sciences. 2021; 11(18):8556. https://doi.org/10.3390/app11188556
Chicago/Turabian StyleKantusch, Timmy, Advan Sinanovic, and Stefanie Marker. 2021. "A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic" Applied Sciences 11, no. 18: 8556. https://doi.org/10.3390/app11188556
APA StyleKantusch, T., Sinanovic, A., & Marker, S. (2021). A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic. Applied Sciences, 11(18), 8556. https://doi.org/10.3390/app11188556