
How to Prevent SARS-CoV-2 Transmission in the Agri-Food Industry during the First Pandemic Wave: Effects on Seroprevalence

 ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
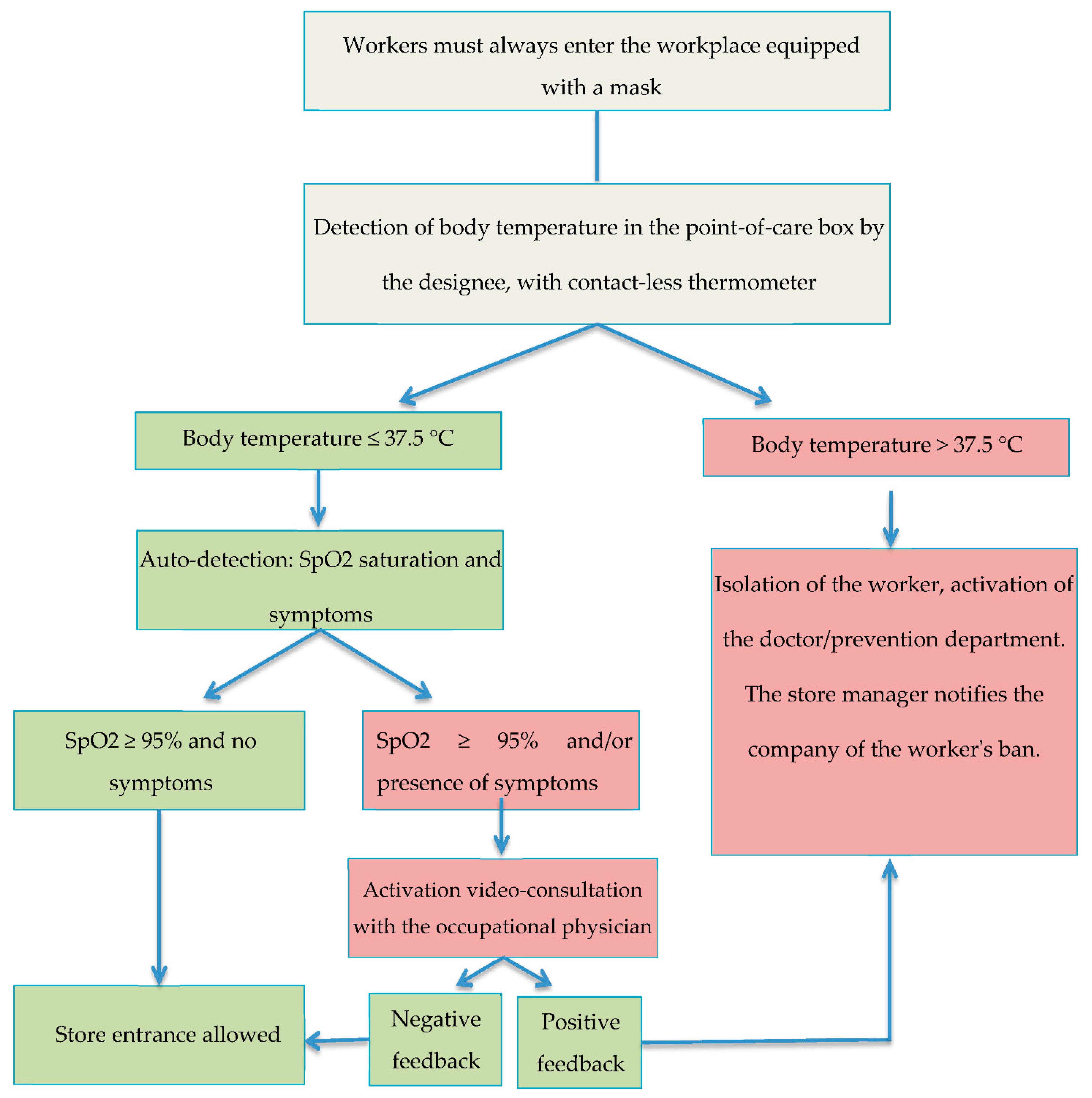
2.2. COVID-19 Risk and Prevention Measures
2.3. Health Parameters Measured
2.4. Statistical Analysis
3. Results
4. Discussion
Outcome Measures on Cost-Utility and Budget Impact
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, A.; Jernigan, D.B. 2019-nCoV CDC Response Team. Initial Public Health Response and Interim Clinical Guidance for the 2019 Novel Coronavirus Outbreak-United States, December 31, 2019-February 4, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 140–146. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Contact Tracing: Public Health Management of Persons, Including Healthcare Workers, Having Had Contact with COVID-19 Cases in the European Union–First Update 31 March 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Public-health-management-persons-contact-novel-coronavirus-cases-2020-03-31.pdf (accessed on 27 October 2020).
- Koh, D. Occupational risks for COVID-19 infection. Occup. Med. 2020, 70, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Assocation (WHO). Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. 14 February 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 (accessed on 11 May 2020).
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- State Council, China Guidelines for the Selection and Use of Different Types of Masks for Preventing New Coronavirus Infection in Different Populations 2020. 5 February 2020. Available online: http://www.gov.cn/xinwen/2020-02/05/content_5474774.htm (accessed on 25 April 2020). (In Chinese)
- Io Resto a Casa (Stay at Home) Decree Was Approved. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4186 (accessed on 26 April 2020).
- Italian National Institute for Insurance against Industrial Injuries INAIL 2020. Available online: https://www.inail.it/cs/internet/comunicazione/news-ed-eventi/news/news-denunce-contagi-covid-30-giugno-2020.html (accessed on 5 July 2020).
- Belingheri, M.; Paladino, M.E.; Riva, M.A. COVID-19: Health prevention and control in non-healthcare settings. Occup. Med. 2020, 70, 82–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, R.; George, A. Prevention of COVID-19 in the workplace. S. Afr. Med. J. 2020, 110, 269–270. [Google Scholar] [CrossRef] [PubMed]
- Occupational Safety and Health Administration (OSHA). COVID-19: Back to the Workplace. Adapting Workplaces and Protecting Workers. Available online: https://osha.europa.eu/it/publications/covid-19-back-workplace-adapting-workplaces-and-protecting-workers/view (accessed on 29 April 2020).
- Tollånes, M.C.; Bakken Kran, A.M.; Abildsnes, E.; Jenum, P.A.; Breivik, A.C.; Sandberg, S. Evaluation of eleven rapid tests for detection of antibodies against SARS-CoV-2. Clin. Chem. Lab. Med. 2020, 58, 1595–1600. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, T.; Nissen, K.; Krambrich, J.; Rönnberg, B.; Akaberi, D.; Esmaeilzadeh, M.; Salaneck, E.; Lindahl, J.; Lundkvist, Å. Evaluation of a COVID-19 IgM and IgG rapid test; an efficient tool for assessment of past exposure to SARS-CoV-2. Infect Ecol. Epidemiol. 2020, 10, 1754538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italian National Institute for Insurance against Industrial Injuries (INAIL). Coronavirus, Containment and Prevention in the Workplace. Available online: https://www.inail.it/cs/internet/comunicazione/news-ed-eventi/news/news-coronavirus-fase-2-documento-tecnico-lavoro-2020.html (accessed on 28 April 2020).
- International Labour Organization (ILO). Agriculture; Plantations; Other Rural Sectors. Available online: https://www.ilo.org/global/industries-and-sectors/agriculture-plantations-other-rural-sectors/lang--en/index.htm (accessed on 6 May 2020).
- Kaźmierczak-Siedlecka, K.; Vitale, E.; Makarewicz, W. COVID-19-gastrointestinal and gut microbiota-related aspects. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 10853–10859. [Google Scholar]
- Italian National Institut of Statistic (ISTAT). Capitale Umano E Stratificazione Sociale Nell’italia Agricola Secondo il 6° Censimento Generale Dell’agricoltura. Available online: https://www.istat.it/it/files//2013/07/Italia_agricola.pdf (accessed on 19 December 2020).
- Italian National Institute for Insurance against Industrial Injuries (INAIL). Trend of Injuries at Work and Professional Diseases. Available online: https://www.inail.it/cs/internet/docs/alg-dati-inail-2020-marzo.pdf (accessed on 2 January 2021).
- Maugeri, A.; Barchitta, M.; Battiato, S.; Agodi, A. Modeling the Novel Coronavirus (SARS-CoV-2) Outbreak in Sicily, Italy. Int. J. Environ. Res. Public Health 2020, 17, 4964. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Gao, M.; Yang, L.; Chen, X.; Deng, Y.; Yang, S.; Xu, H.; Chen, Z.; Gao, X. A study on infectivity of asymptomatic SARS-CoV-2 carriers. Respir. Med. 2020, 169, 106026. [Google Scholar] [CrossRef]
- Nicastri, E.; D’Abramo, A.; Faggioni, G.; De Santis, R.; Mariano, A.; Lepore, L.; Molinari, F.; Petralito, G.; Fillo, S.; Munzi, D.; et al. Coronavirus disease (COVID-19) in a pauci-symptomatic patient: Epidemiological and clinical challenge in settings with limited community transmission. Euro Surveill. 2020, 25, 2000230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramaci, T.; Pellerone, M.; Ledda, C.; Rapisarda, V. Health promotion, psychological distress, and disease prevention in the workplace: A cross-sectional study of Italian adults. Risk Manag. Healthc. Policy 2017, 10, 167–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapisarda, V.; Ledda, C.; Migliore, M.; Salemi, R.; Musumeci, A.; Bracci, M.; Marconi, A.; Loreto, C.; Libra, M. FBLN-3 as a biomarker of pleural plaques in workers occupationally exposed to carcinogenic fibers: A pilot study. Future Oncol. 2015, 11 (Suppl. 24), 35–37. [Google Scholar] [CrossRef]


{kind=link}
| If Your Values Are in This Column YOU CAN ENTER | If Your Values Are in This Column YOU CANNOT ENTER |
|---|---|
| Body Temperature ≤ 37.5 °C | Body Temperature > 37.5 °C |
| Oxygen saturation > 95 | Oxygen saturation ≤ 95 |
| You are not having difficulty in breathing | You are having difficulty in breathing |
| You do not have a cough | You have a cough (excluding allergy) |
| You do not have a fever | You have a fever |
| You did not have a fever yesterday | You had a fever yesterday |
| You do not have diarrhea | You have diarrhea |
| You do not feel nauseous | You feel nauseous |
| You do not have vomiting | You have vomiting |
| You have no alterations in the perception of smells | You have alterations in the perception of smells |
| You do not have altered taste perception | You have altered taste perception |
| You have not widespread muscle pain | You have widespread muscle pain |
| You do not have tearing and redness of the eyes | You have tearing/redness of the eyes (excluding allergy) |
| You have no nasal congestion and/or runny nose | You have nasal congestion and/or runny nose (excluding allergy) |
| Sample Characteristics | Agricultural Workers 180 (100%) | Workers in the Supply Chain 148 (100%) | p-Value | |
|---|---|---|---|---|
| Male | 177 (98%) | 91 (61%) | <0.05 | |
| Age (years) | 43.6 ± 7.2 | 42.2 ± 5.6 | n.s. | |
| Years of employment | 19.5 ± 5.4 | 18.5 ± 4.1 | n.s. | |
| Smokers | 145 (80%) | 111 (75%) | n.s. | |
| Pack/years | <20 >20 | 103 (71%) 42 (29%) | 84 (76%) 27 (24%) | n.s. n.s. |
| Alcohol use | 180 (100%) | 148 (100%) | n.s. | |
| Physical Risks: MMC, Sb, Pi | 180 (100%) | 148 (100%) | n.s. | |
| Climate risk and UV rays | 180 (100%) | 17 (11%) | <0.05 | |
| Body vibration risk | 20 (11.1%) | 17 (11%) | n.s. | |
| Chemical Risk | 21 (11.6%) | 0 (0%) | <0.05 | |
| COVID-19 risk | low medium/high | 180 (100%) 0 (0%) | 0 (0%) 148 (100%) | <0.05 <0.05 |
| Clinical Signs/Symptoms | Supply Chain Workers 32 (100%) | Agricultural Workers 17 (100%) | p-Values |
|---|---|---|---|
| Fever | 20 (61%) | 10 (57%) | n.s. |
| Muscle or joint pain | 6 (19%) | 4 (22%) | n.s. |
| Dry cough | 5 (18%) | 2 (11%) | n.s. |
| Nausea or vomit | 5 (8%) | 1 (4%) | n.s. |
| Loss of taste and smell | 5 (8%) | 1 (4%) | n.s. |
| Oxygen saturation < 95% | 1 (4%) | 1 (4%) | n.s. |
| IgG− | IgG+ | IgM− | IgM+ | NMS | p-Values | |
|---|---|---|---|---|---|---|
| Agricultural workers | 180 (55%) | 0 | 180 (55%) | 0 | 0 | n.s. |
| Supply chain workers | 147 (44%) | 1(1%) | 148 (45%) | 0 | 1 (1%) | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitale, E.; Vella, F.; Filetti, V.; Cirrincione, L.; Indelicato, G.; Cannizzaro, E.; Rapisarda, V. How to Prevent SARS-CoV-2 Transmission in the Agri-Food Industry during the First Pandemic Wave: Effects on Seroprevalence. Appl. Sci. 2021, 11, 10051. https://doi.org/10.3390/app112110051
Vitale E, Vella F, Filetti V, Cirrincione L, Indelicato G, Cannizzaro E, Rapisarda V. How to Prevent SARS-CoV-2 Transmission in the Agri-Food Industry during the First Pandemic Wave: Effects on Seroprevalence. Applied Sciences. 2021; 11(21):10051. https://doi.org/10.3390/app112110051
Chicago/Turabian StyleVitale, Ermanno, Francesca Vella, Veronica Filetti, Luigi Cirrincione, Giuliano Indelicato, Emanuele Cannizzaro, and Venerando Rapisarda. 2021. "How to Prevent SARS-CoV-2 Transmission in the Agri-Food Industry during the First Pandemic Wave: Effects on Seroprevalence" Applied Sciences 11, no. 21: 10051. https://doi.org/10.3390/app112110051
APA StyleVitale, E., Vella, F., Filetti, V., Cirrincione, L., Indelicato, G., Cannizzaro, E., & Rapisarda, V. (2021). How to Prevent SARS-CoV-2 Transmission in the Agri-Food Industry during the First Pandemic Wave: Effects on Seroprevalence. Applied Sciences, 11(21), 10051. https://doi.org/10.3390/app112110051