
An Effective Convolutional Neural Network Model for the Early Detection of COVID-19 Using Chest X-ray Images

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Related Work
3. Material and Methods
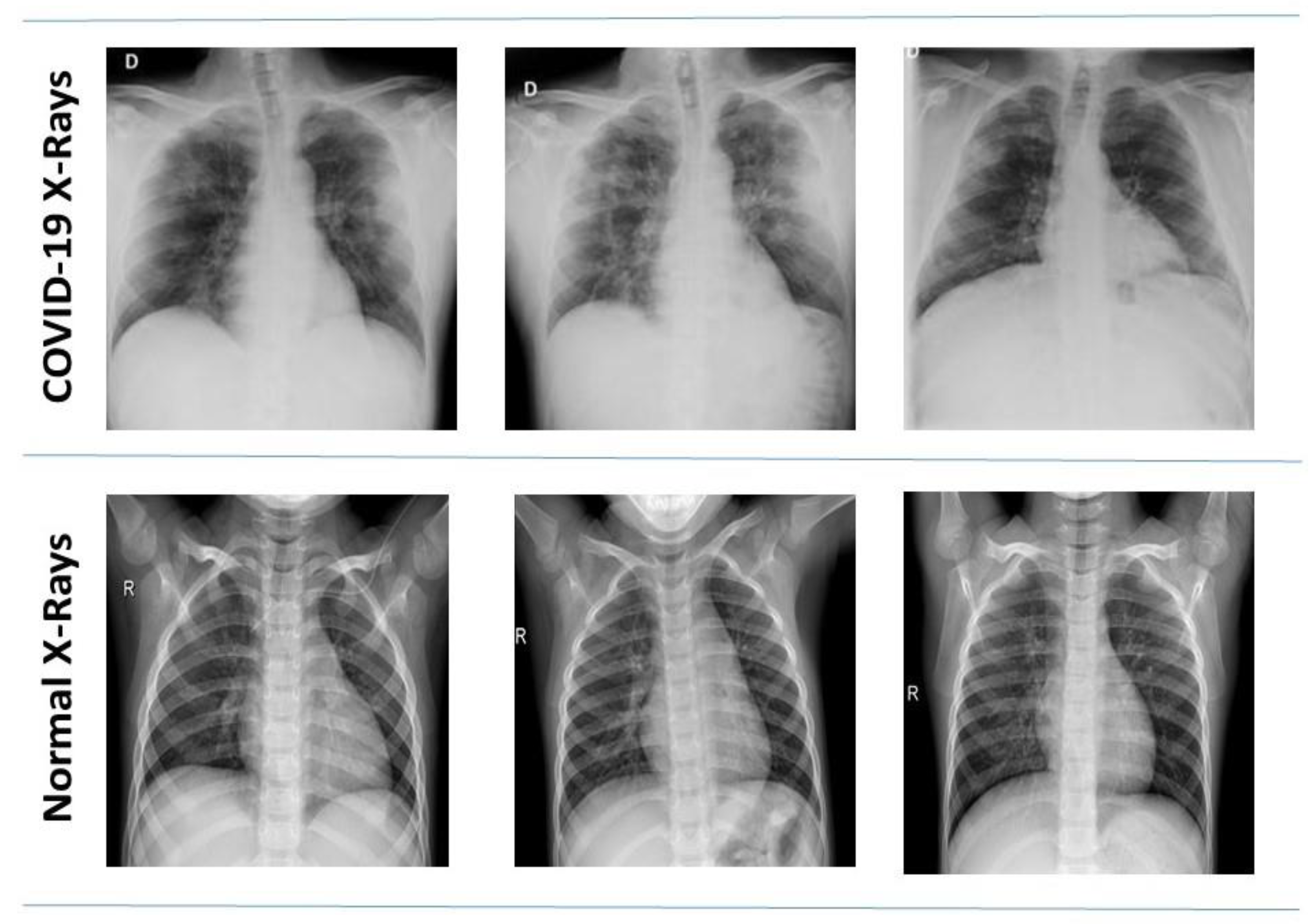
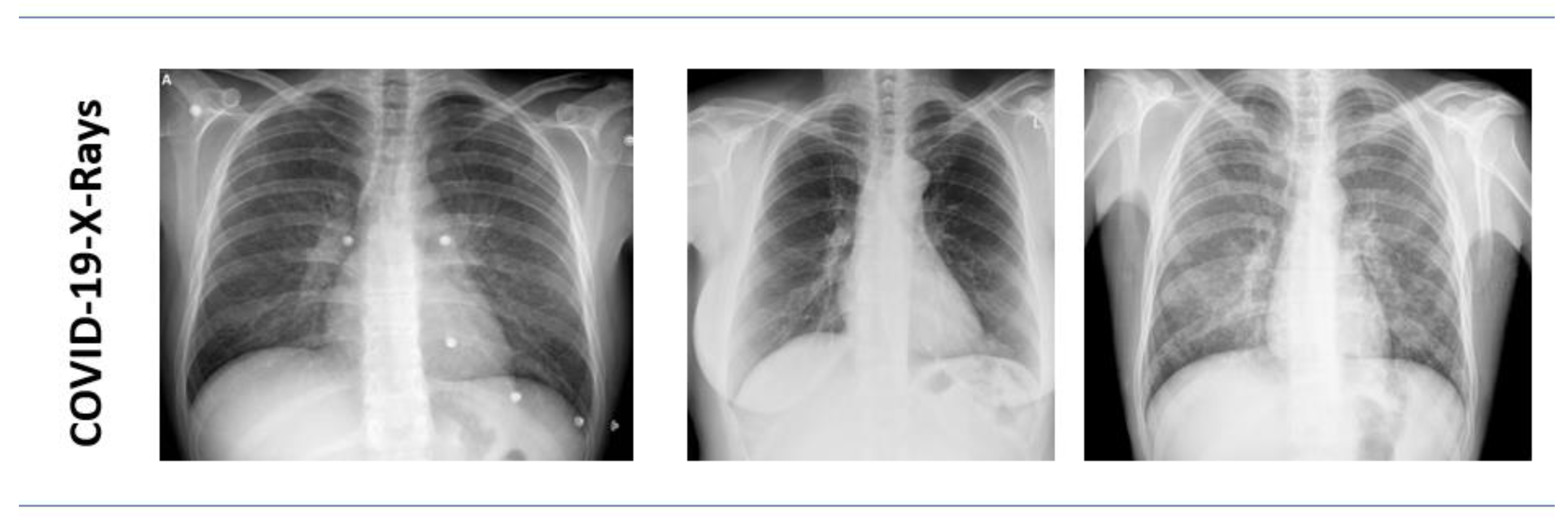
3.1. Dataset
3.1.1. Kaggle COVID-19 Radiography Database
3.1.2. COVID-19 Chest X-ray Dataset by Joseph Paul Cohen
3.1.3. Data Distribution
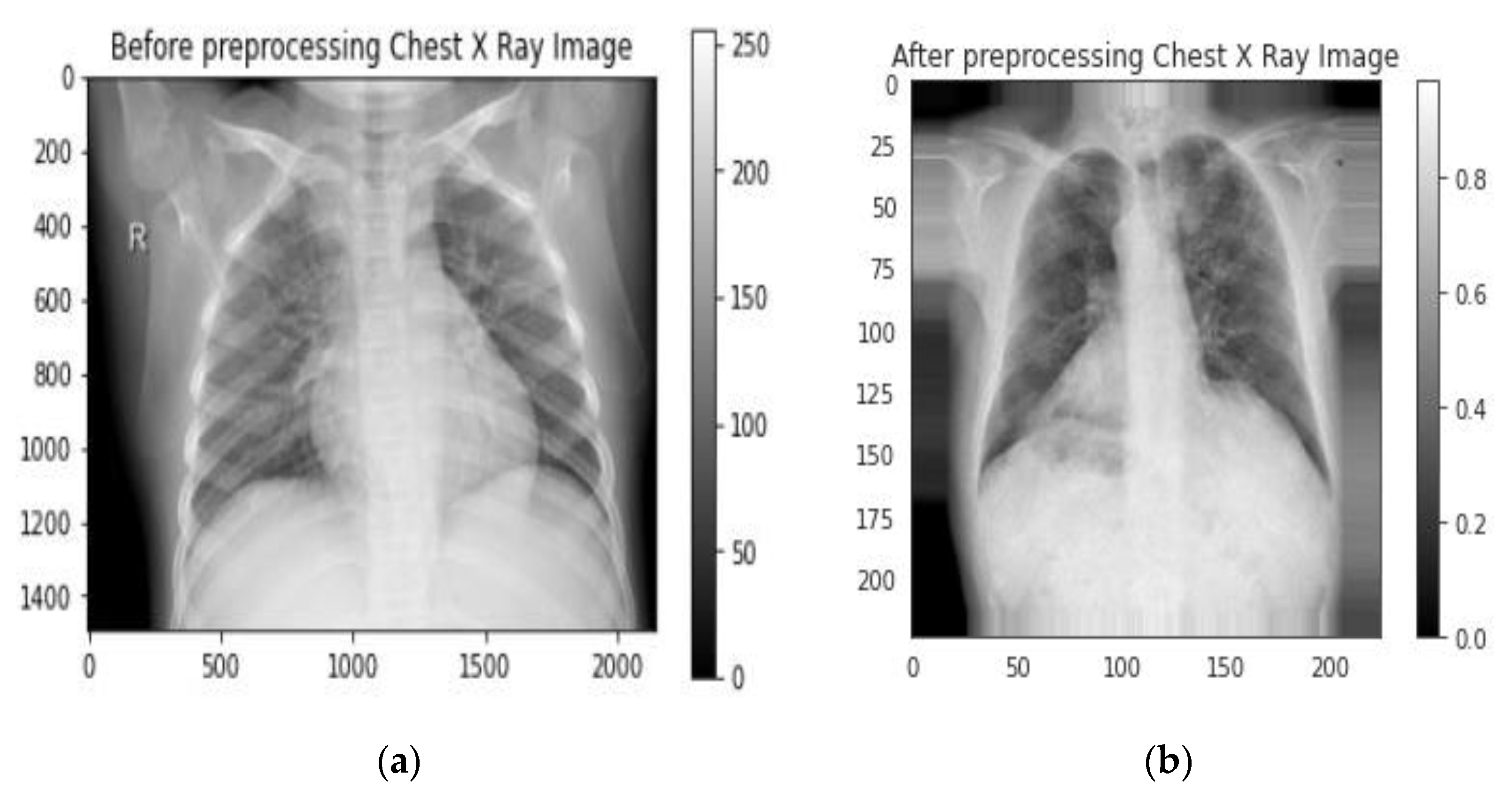
3.2. Preprocessing
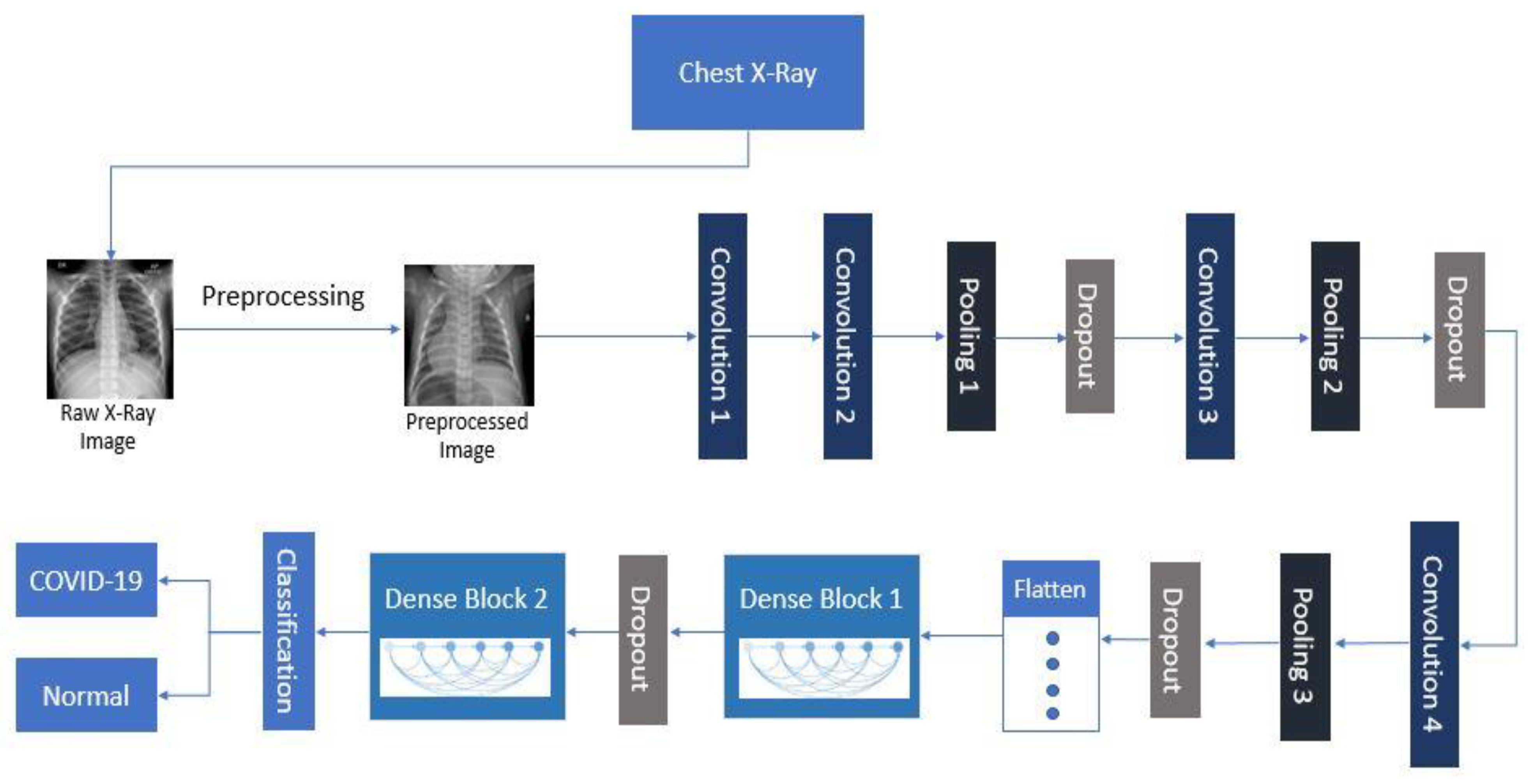
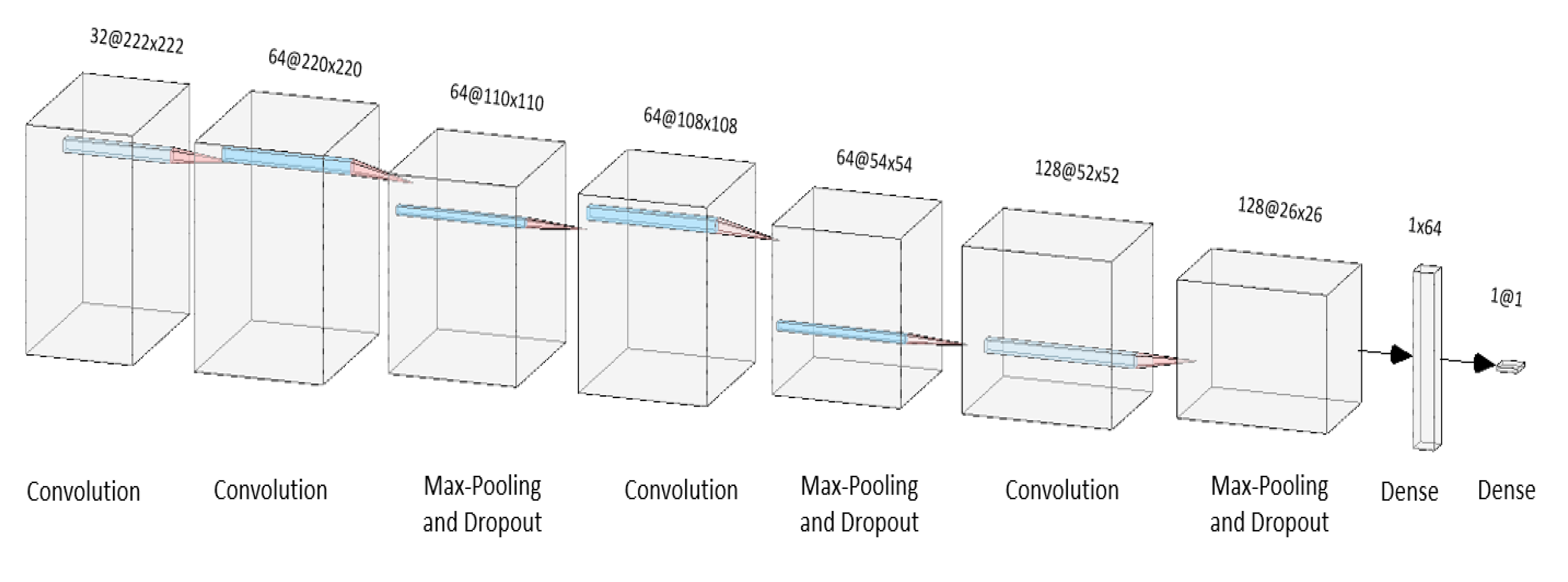
3.3. Layers of the Architecture
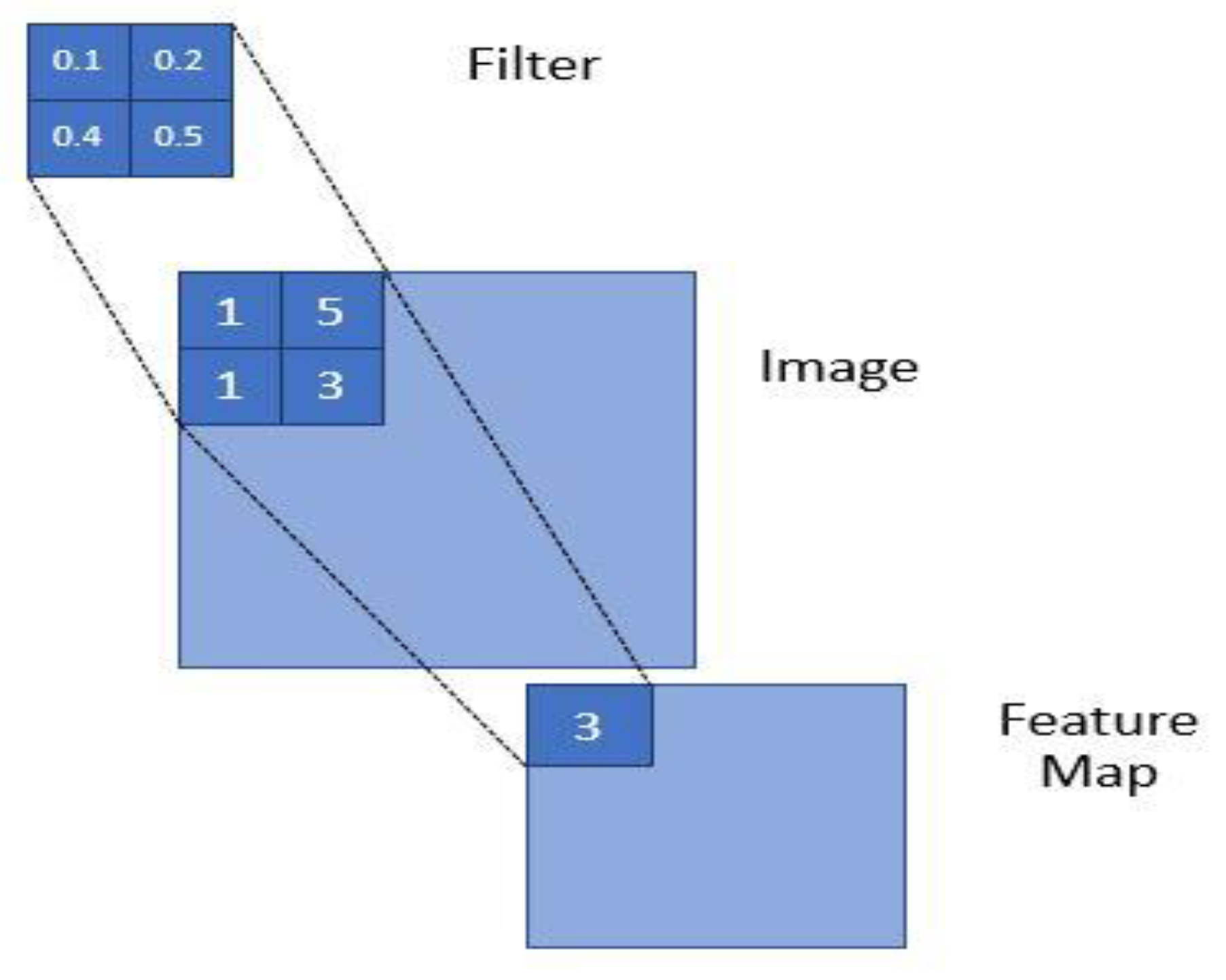
3.3.1. Convolution Layer
| Algorithm 1 Convolution Layer |
|
1. Input: x (X coordinate), y (Y coordinate) 2. Output: sum (sum of product of kernel weight and the value at the corresponding position) 3. x ← 0 4. Ri (Input of feature map), Rj (Output of feature map), Ki × Kj (kernel size) 5. For (i = 0 to i < Rj-Kj) do 6. y ← 0 7. For (j=0 to j < Rj-Kj) do 8. Sum ← 0 9. For (ki=0 to ki < Ki) do 10. For (kj=0 to kj < Kj) 11. sum+ ← image[i+ki][j+kj]*K[ki][kj] 12. Endfor 13. Endfor 14. f1[x][y] TransformToNonLinear(count) 15. Y++ 16. Endfor 17. X++ 18. Endfor |
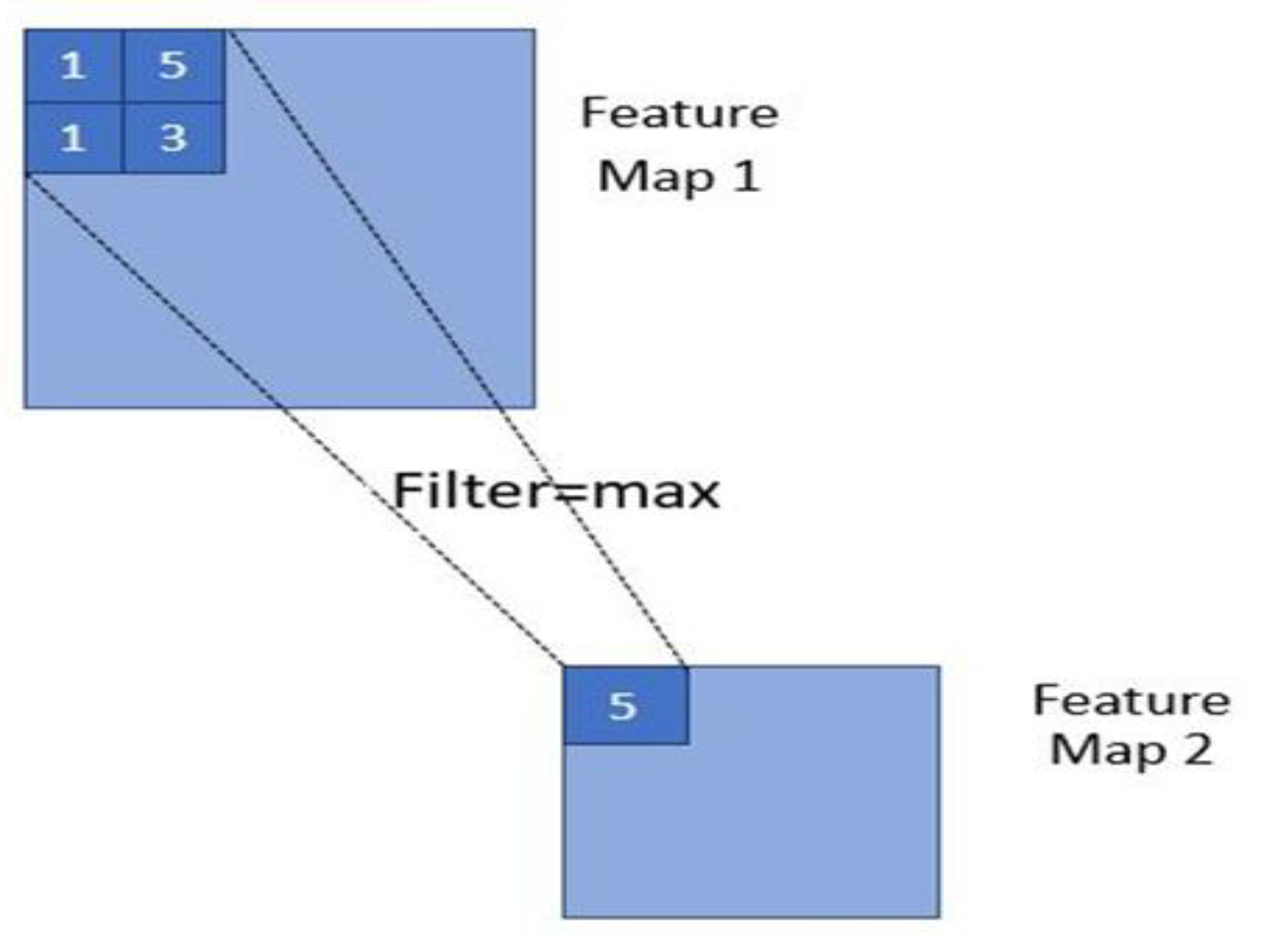
3.3.2. Max-Pooling and Dropout Layer
| Algorithm 2 Pooling Layer |
|
1. Input: x (X coordinate), y (Y coordinate) 2. Output: sum (sum of product of kernel weight and the value at the corresponding position) 3. x ← 0 4. Ri (Input of feature map), Rj (Output of feature map), Ki × Kj (kernel size) 5. For (i = 0 to i < Rj-Kj) do 6. y ← 0 7. For (j=0 to j < Rj-Kj) do 8. Sum ← 0 9. For (ki = 0 to ki < Ki) do 10. For (kj = 0 to kj < Kj) 11. temp ← image[i+ki][j+kj]*Kki][kj] 12. var ← max(var, temp) 13. Endfor 14. Endfor 15. f1[x][y] ← TransformToNonLinear(count) 16. Y++ 17. Endfor 18. X++ 19. Endfor |
3.3.3. Dense Layer
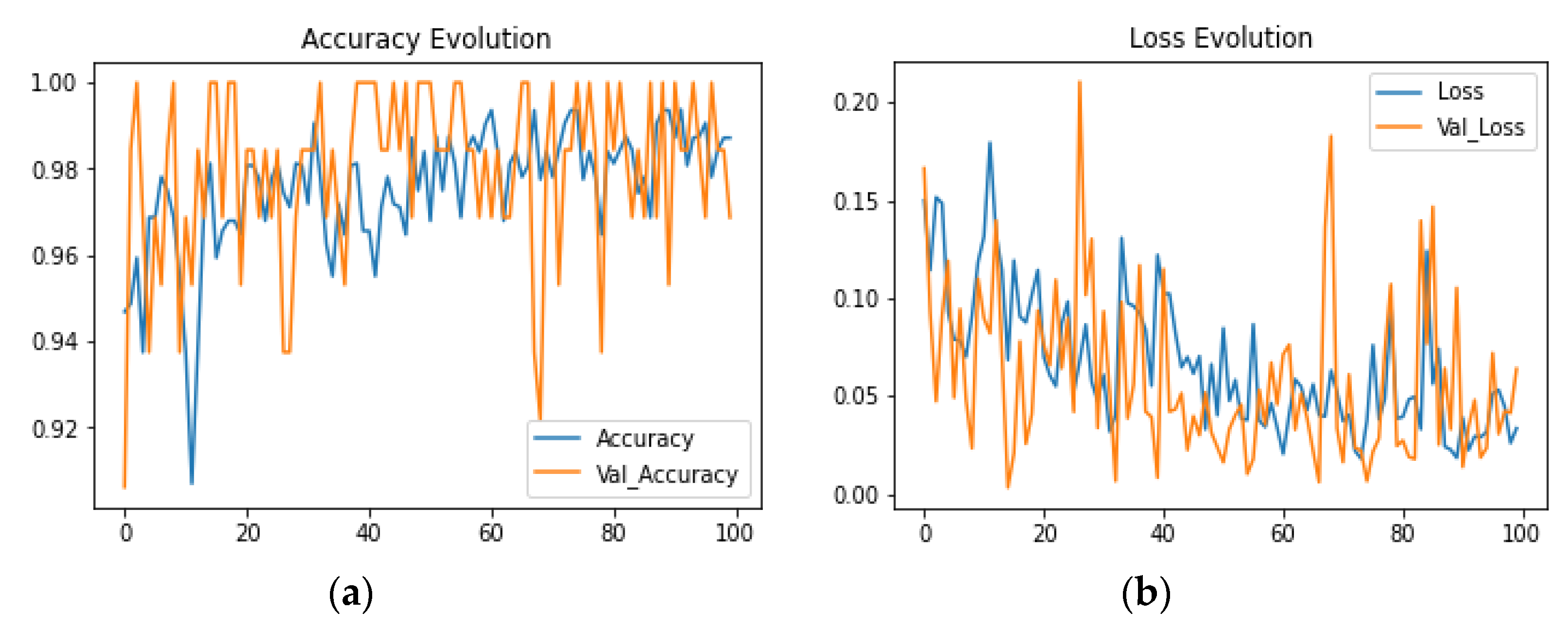
3.4. Training and Validation
4. Experimental Results
4.1. Performance Indicators
4.2. Comparison with Similar Study
5. Limitations and Future Work
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naming the Coronavirus Disease (COVID-19) and the Virus that Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 31 August 2021).
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 Infection: Origin, Transmission, and Characteristics of Human Coronaviruses. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7113610/ (accessed on 31 August 2021).
- Coronaviruses: Definition, COVID-19, SARS, MERS. Available online: https://www.medicalnewstoday.com/articles/256521 (accessed on 31 August 2021).
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and Multiorgan Response; Elsevier: Amsterdam, The Netherlands, 2021; Available online: https://www.sciencedirect.com/science/article/pii/S0146280620300955 (accessed on 31 August 2021).
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 31 August 2021).
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy: Early Experience and Forecast during an Emergency Response. JAMA 2020, 323, 1545–1546. Available online: https://jamanetwork.com/journals/jama/article-abstract/2763188 (accessed on 31 August 2021). [CrossRef] [PubMed] [Green Version]
- COVID Live Update: 217,920,243 Cases and 4,524,009 Deaths from the Coronavirus—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 31 August 2021).
- Liu, J.; Liao, X.; Qian, S.; Yuan, J.; Wang, F.; Liu, Y.; Wang, Z.; Wang, F.-S.; Liu, L.; Zhang, Z. Community transmission of severe acute respiratory syndrome Coronavirus 2, Shenzhen, China, 2020. Emerg. Infect. Dis. 2020, 26, 1320–1323. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Verardi, R.; et al. Reduced Rate of Hospital Admissions for ACS during Covid-19 Outbreak in Northern Italy. N. Engl. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. Pattern Anal. Appl. 2021, 24, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Karaca-Mandic, P.; Sen, S.; Georgiou, A.; Zhu, Y.; Basu, A. Association of COVID-19-Related Hospital Use and Overall COVID-19 Mortality in the USA. J. Gen. Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Inui, S.; Fujikawa, A.; Jitsu, M.; Kunishima, N.; Watanabe, S.; Suzuki, Y.; Umeda, S.; Uwabe, Y. Chest CT Findings in Cases from the Cruise Ship Diamond Princess with Coronavirus Disease (COVID-19). Radiol. Cardiothorac. Imaging 2020, 2, e200100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apostolopoulos, I.D.; Mpesiana, T.A. Covid-19: Automatic detection from X-ray images utilizing transfer learning with convolutional neural networks. Phys. Eng. Sci. Med. 2020, 43, 635–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- News—HealthITAnalytics. Available online: https://healthitanalytics.com/topic/infrastructure (accessed on 31 August 2021).
- Data Scientists Use Machine Learning to Discover COVID-19 Treatments. Available online: https://healthitanalytics.com/news/data-scientists-use-machine-learning-to-discover-covid-19-treatments (accessed on 31 August 2021).
- Asraf, A.; Islam, M.Z.; Haque, M.R.; Islam, M.M. Deep Learning Applications to Combat Novel Coronavirus (COVID-19) Pandemic. SN Comput. Sci. 2020, 1. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Gupta, P.K.; Srivastava, A. A Review of Modern Technologies for Tackling COVID-19 Pandemic; Elsevier: Amsterdam, The Netherlands, 2020; Available online: https://www.sciencedirect.com/science/article/pii/S1871402120301272 (accessed on 31 August 2021).
- Chouhan, V.; Singh, S.K.; Khamparia, A.; Gupta, D.; Tiwari, P.; Moreira, C.; Damaševičius, R.; De Albuquerque, V.H.C. A novel transfer learning based approach for pneumonia detection in chest X-ray images. Sciences 2020, 10, 559. [Google Scholar] [CrossRef] [Green Version]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-Level Classification of Skin Cancer with Deep Neural Networks. 2017. Available online: https://www.nature.com/articles/nature21056?spm=5176.100239.blogcont100708.20.u9mVh9 (accessed on 31 August 2021).
- Luján-García, J.E.; Moreno-Ibarra, M.A.; Villuendas-Rey, Y.; Yáñez-Márquez, C. Fast COVID-19 and pneumonia classification using chest X-ray images. Mathematics 2020, 8, 1423. [Google Scholar] [CrossRef]
- Sakib, S.; Tazrin, T.; Fouda, M.M.; Fadlullah, Z.M.; Guizani, M. DL-CRC: Deep Learning-Based Chest Radiograph Classification for COVID-19 Detection: A Novel Approach. 2020. Available online: https://ieeexplore.ieee.org/abstract/document/9199819/ (accessed on 31 August 2021).
- Irfan, M.; Iftikhar, M.; Yasin, S.; Draz, U.; Ali, T.; Hussain, S.; Bukhari, S.; Alwadie, A.; Rahman, S.; Glowacz, A.; et al. Role of Hybrid Deep Neural Networks (HDNNs), Computed Tomography, and Chest X-rays for the Detection of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 3056. [Google Scholar] [CrossRef] [PubMed]
- Musleh, A.A.; Maghari, A.Y. COVID-19 Detection in X-ray Images Using CNN Algorithm. 2020. Available online: https://covid19.elsevierpure.com/en/publications/covid-19-detection-in-x-ray-images-using-cnn-algorithm (accessed on 31 August 2021).
- El-Rashidy, N.; El-Sappagh, S.; Islam, S.M.; El-Bakry, H.M.; Abdelrazek, S. End-to-end deep learning framework for coronavirus (COVID-19) detection and monitoring. Electronics 2020, 9, 1439. [Google Scholar] [CrossRef]
- Loddo, A.; Pili, F.; Di Ruberto, C. Deep Learning for COVID-19 Diagnosis from CT Images. Appl. Sci. 2021, 11, 8227. [Google Scholar] [CrossRef]
- Horry, M.J.; Chakraborty, S.; Paul, M.; Ulhaq, A.; Pradhan, B.; Saha, M.; Shukla, N. COVID-19 detection through transfer learning using multimodal imaging data. IEEE Access 2020, 8, 149808–149824. [Google Scholar] [CrossRef]
- Signoroni, A.; Savardi, M.; Benini, S.; Adami, N.; Leonardi, R.; Gibellini, P.; Vaccher, F.; Ravanelli, M.; Borghesi, A.; Maroldi, R. BS-Net: Learning COVID-19 pneumonia severity on a large chest X-ray dataset. Med. Imag. Anal. 2021, 71, 102046. [Google Scholar] [CrossRef] [PubMed]
- Giri, B.; Pandey, S.; Shrestha, R.; Pokharel, K.; Ligler, F.S.; Neupane, B.B. Review of analytical performance of COVID-19 detection methods. Anal. Bioanal. Chem. 2021, 413, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Haque, K.F.; Haque, F.F.; Gandy, L.; Abdelgawad, A. Automatic detection of COVID-19 from chest X-ray images with convolutional neural networks. In Proceedings of the 2020 International Conference on Computing, Electronics & Communications Engineering (iCCECE), Southend, UK, 17–18 August 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 125–130. [Google Scholar]
- Chowdhury, M.E.; Rahman, T.; Khandakar, A.; Mazhar, R.; Kadir, M.A.; Mahbub, Z.B.; Islam, K.R.; Khan, M.S.; Iqbal, A.; Emadi, N.A. Can AI help in screening viral and COVID-19 pneumonia? IEEE Access 2020, 8, 132665–132676. [Google Scholar] [CrossRef]
- COVID-19 Radiography Database. Available online: https://www.kaggle.com/tawsifurrahman/covid19-radiography-database (accessed on 10 February 2021).
- RSM Italian Society of Radiology. Available online: https://www.sirm.org/category/senzacategoria/covid-19/ (accessed on 22 October 2021).
- COVID-19 Chest X-ray. Available online: https://github.com/ieee8023/covid-chestxray-dataset (accessed on 10 February 2021).
- Radiopaedia | Epoch (Machine Learning). Available online: https://radiopaedia.org/articles/epoch-machine-learning#:~:text=An%20epoch%20is%20a%20term,of%20data%20is%20very%20large (accessed on 6 May 2021).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | COVID-19 Samples | Normal Samples | Type |
|---|---|---|---|
| Kaggle [31] | 300 | 400 | PA |
| GitHub [33] | 100 | 0 | PA |
| Total | 400 | 400 |
| Layer (Type) | Output Shape | Parameters |
|---|---|---|
| Conv2D | (None, 222, 222, 32) | 896 |
| Conv2D | (None, 220, 220, 64) | 18,496 |
| MaxPooling2D | (None, 110, 110, 64) | 0 |
| Dropout | (None, 110, 110, 64) | 0 |
| Conv2D | (None, 108, 108, 64) | 36,928 |
| MaxPooling2D | (None, 54, 54, 64) | 0 |
| Dropout | (None, 54, 54, 64) | 0 |
| Conv2D | (None, 52, 52, 128) | 73,856 |
| MaxPooling2D | (None, 26, 26, 128) | 0 |
| Dropout | (None, 26, 26, 128) | 0 |
| Flatten | (None, 86528) | 0 |
| Dense | (None, 64) | 5,537,856 |
| Dropout | (None, 64) | 0 |
| Dense | (None, 1) | 65 |
| Total: 5,668,097 |
| Class | Training | Validation |
|---|---|---|
| COVID-19 | 300 | 100 |
| Normal | 300 | 100 |
| Total | 600 | 200 |
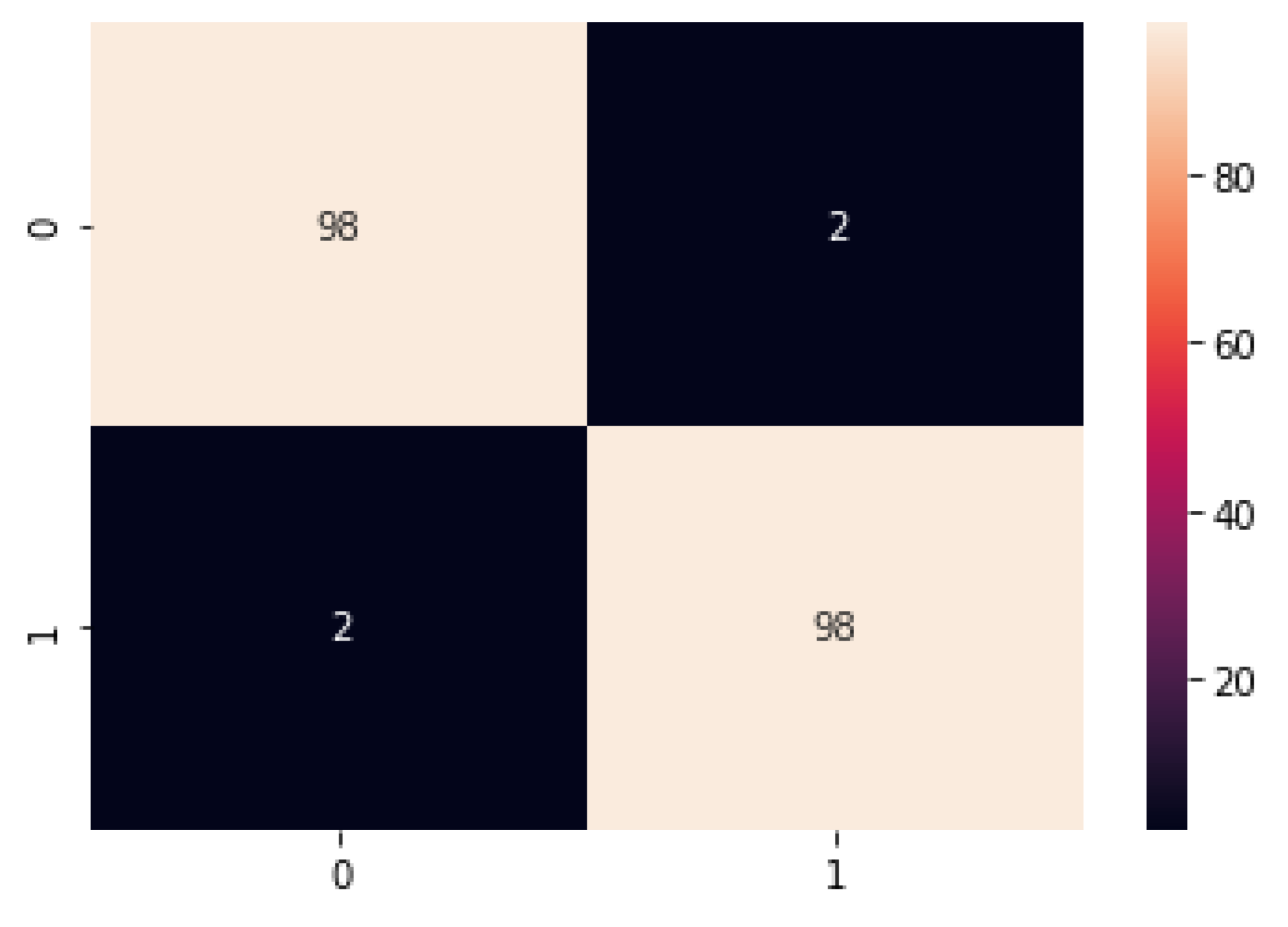
| Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|
| 98.5% | 98% | 98% | 98% |
| Method | COVID-19 Samples | Normal Samples | Class | Accuracy | Preprocessing |
|---|---|---|---|---|---|
| Xception CNN [20] | 287 | 1349 | Multi | 91% | ✔ |
| DL-CRC [21] | 209 | 27,228 | Multi | 93.94% | ✔ |
| CNN [23] | 278 | 278 | Binary | 89.7% | - |
| ConvNet [24] | 250 | 500 | Binary | 97.78% | - |
| Sequential CNN [29] | 206 | 206 | Binary | 97.56% | ✔ |
| CheXNet [30] | 165 | 165 | Multi | 99.7% | ✔ |
| Customized CNN (this work) | 400 | 400 | Binary | 98.5% | ✔ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farooq, M.S.; Rehman, A.U.; Idrees, M.; Raza, M.A.; Ali, J.; Masud, M.; Al-Amri, J.F.; Kazmi, S.H.R. An Effective Convolutional Neural Network Model for the Early Detection of COVID-19 Using Chest X-ray Images. Appl. Sci. 2021, 11, 10301. https://doi.org/10.3390/app112110301
Farooq MS, Rehman AU, Idrees M, Raza MA, Ali J, Masud M, Al-Amri JF, Kazmi SHR. An Effective Convolutional Neural Network Model for the Early Detection of COVID-19 Using Chest X-ray Images. Applied Sciences. 2021; 11(21):10301. https://doi.org/10.3390/app112110301
Chicago/Turabian StyleFarooq, Muhammad Shoaib, Attique Ur Rehman, Muhammad Idrees, Muhammad Ahsan Raza, Jehad Ali, Mehedi Masud, Jehad F. Al-Amri, and Syed Hasnain Raza Kazmi. 2021. "An Effective Convolutional Neural Network Model for the Early Detection of COVID-19 Using Chest X-ray Images" Applied Sciences 11, no. 21: 10301. https://doi.org/10.3390/app112110301
APA StyleFarooq, M. S., Rehman, A. U., Idrees, M., Raza, M. A., Ali, J., Masud, M., Al-Amri, J. F., & Kazmi, S. H. R. (2021). An Effective Convolutional Neural Network Model for the Early Detection of COVID-19 Using Chest X-ray Images. Applied Sciences, 11(21), 10301. https://doi.org/10.3390/app112110301