
Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis



Abstract
:1. Introduction
2. Case Presentation
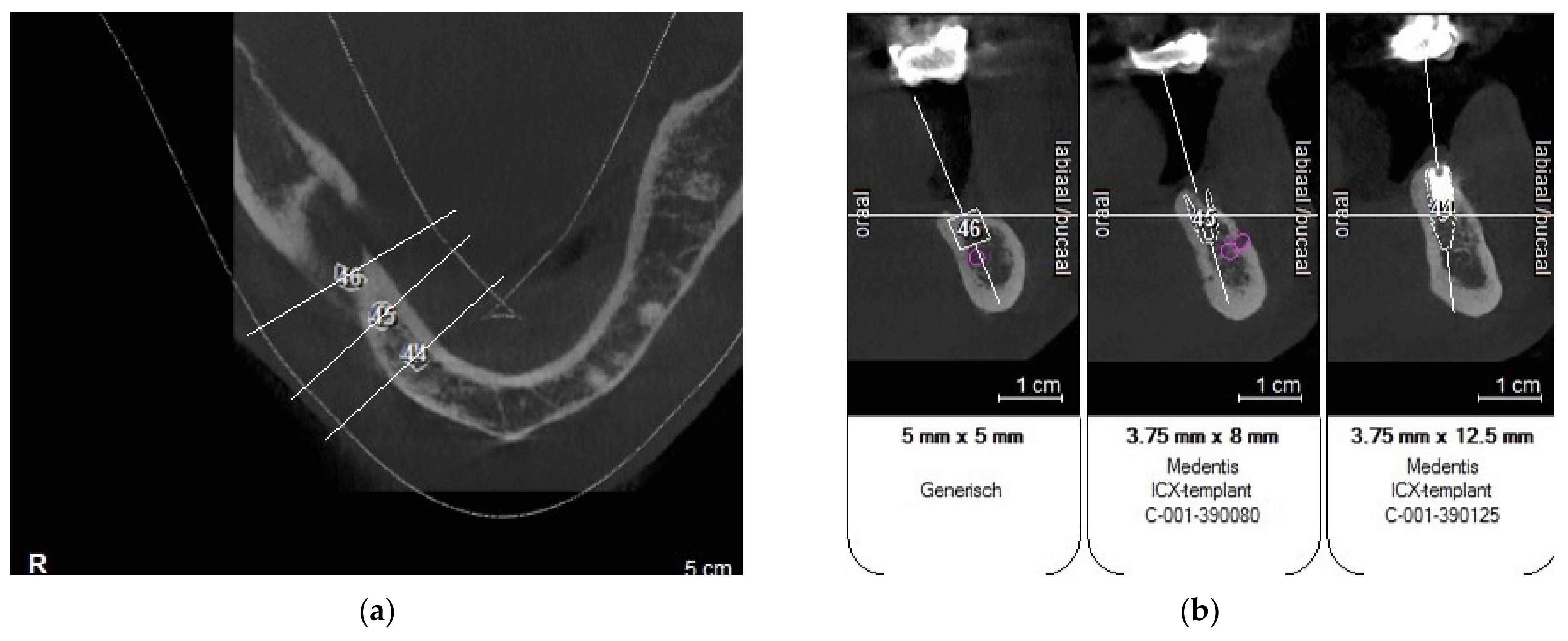
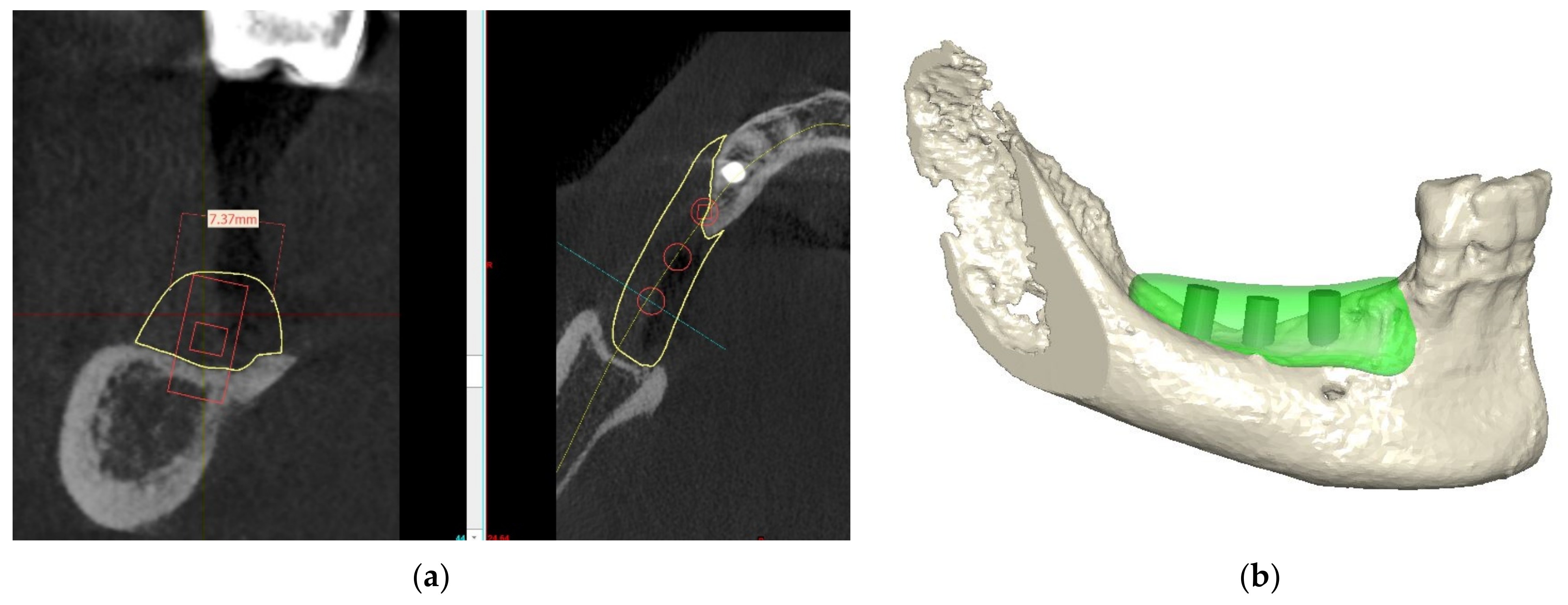
3. Pre-Surgical Planning
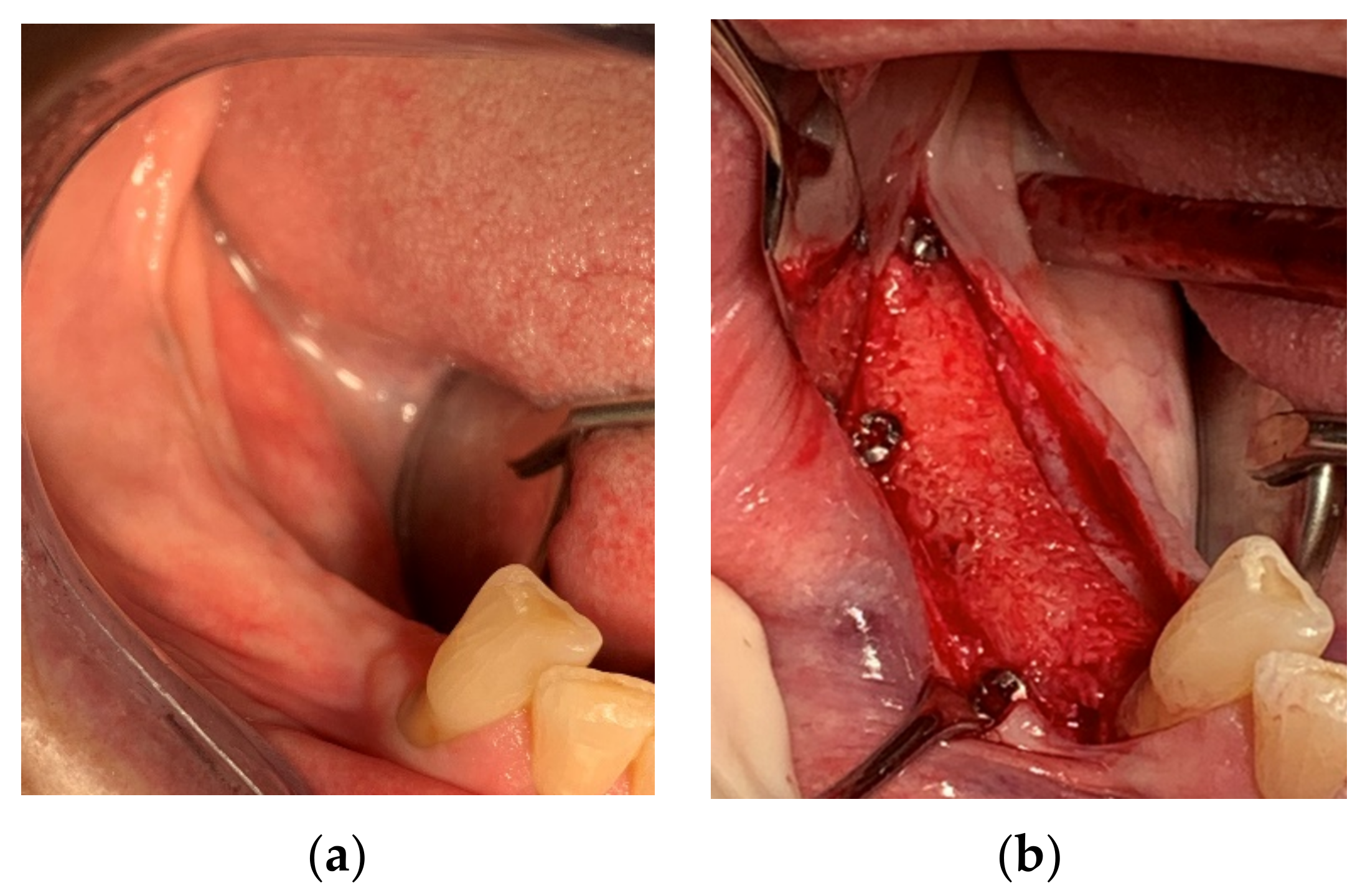
4. Materials and Methods
5. Postoperative Case Management
6. Clinical Outcome
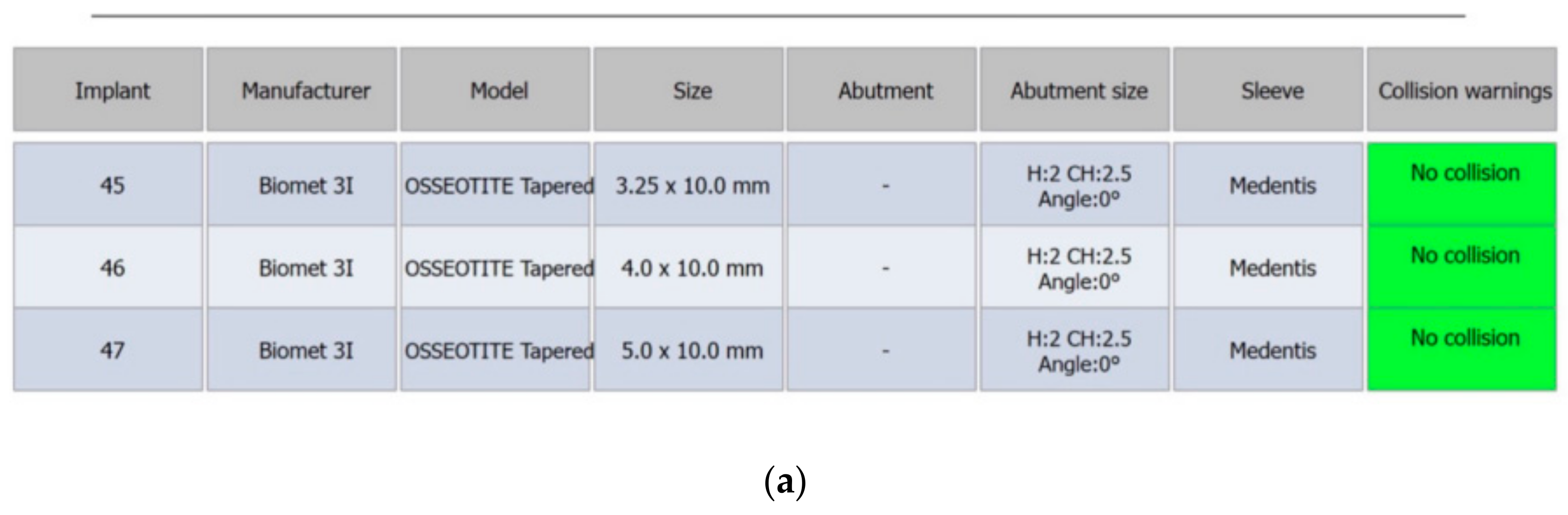
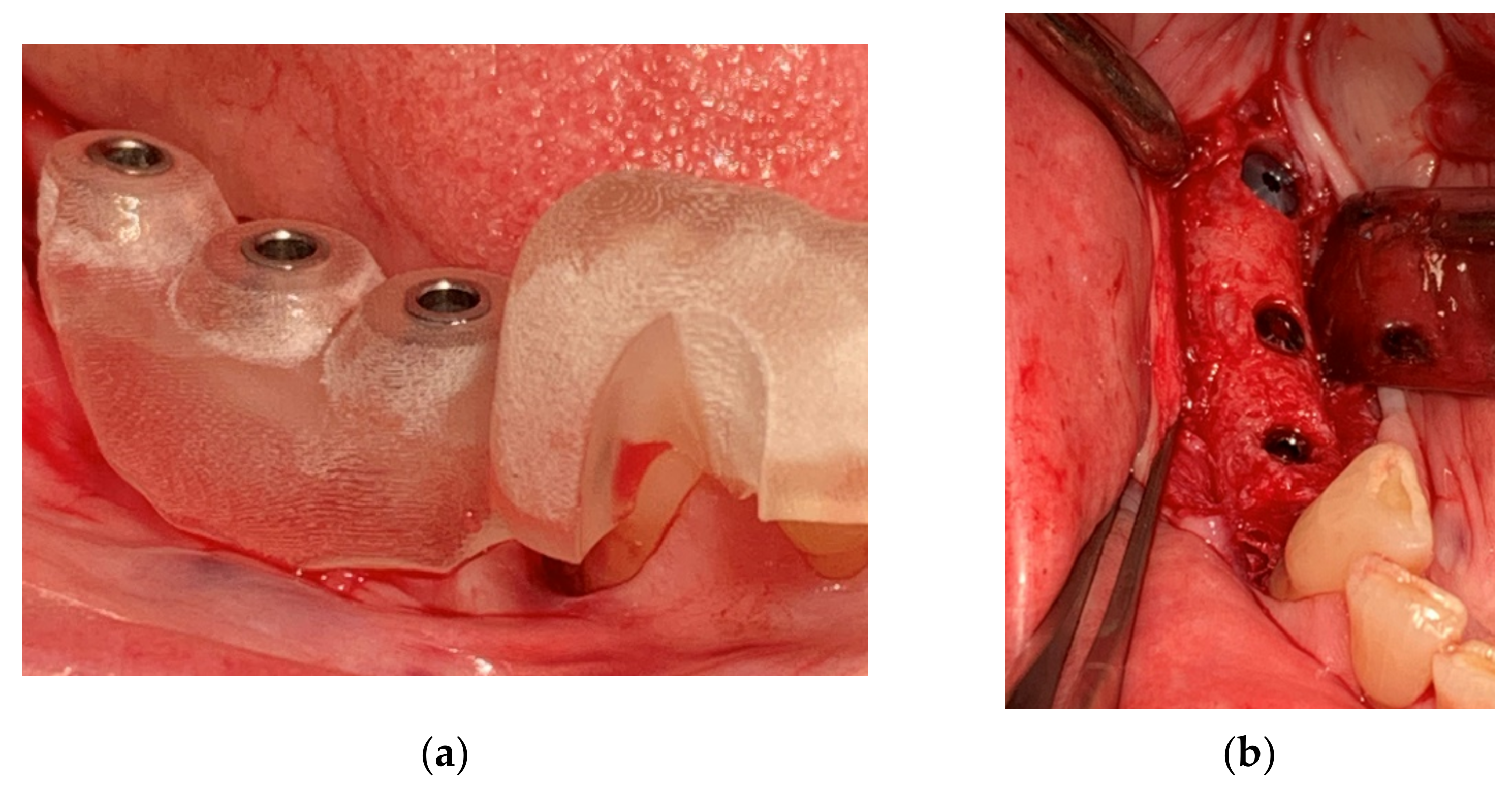
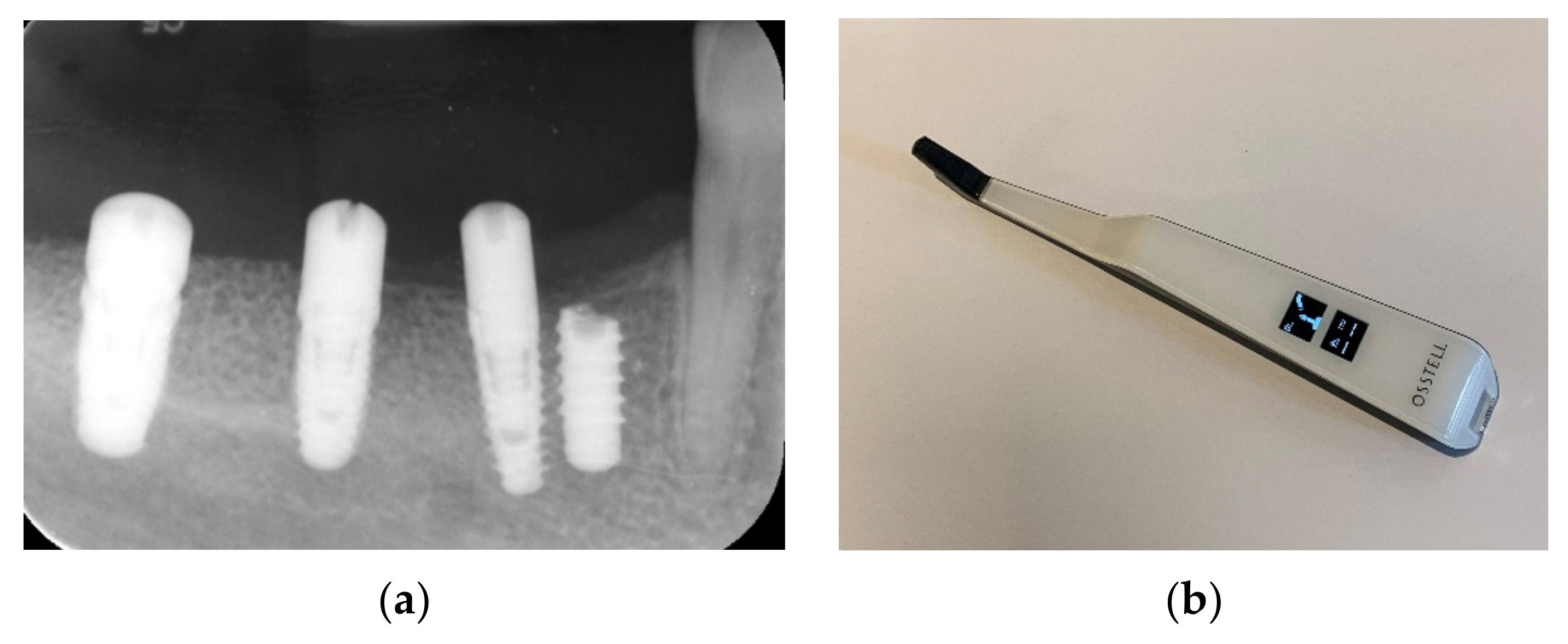
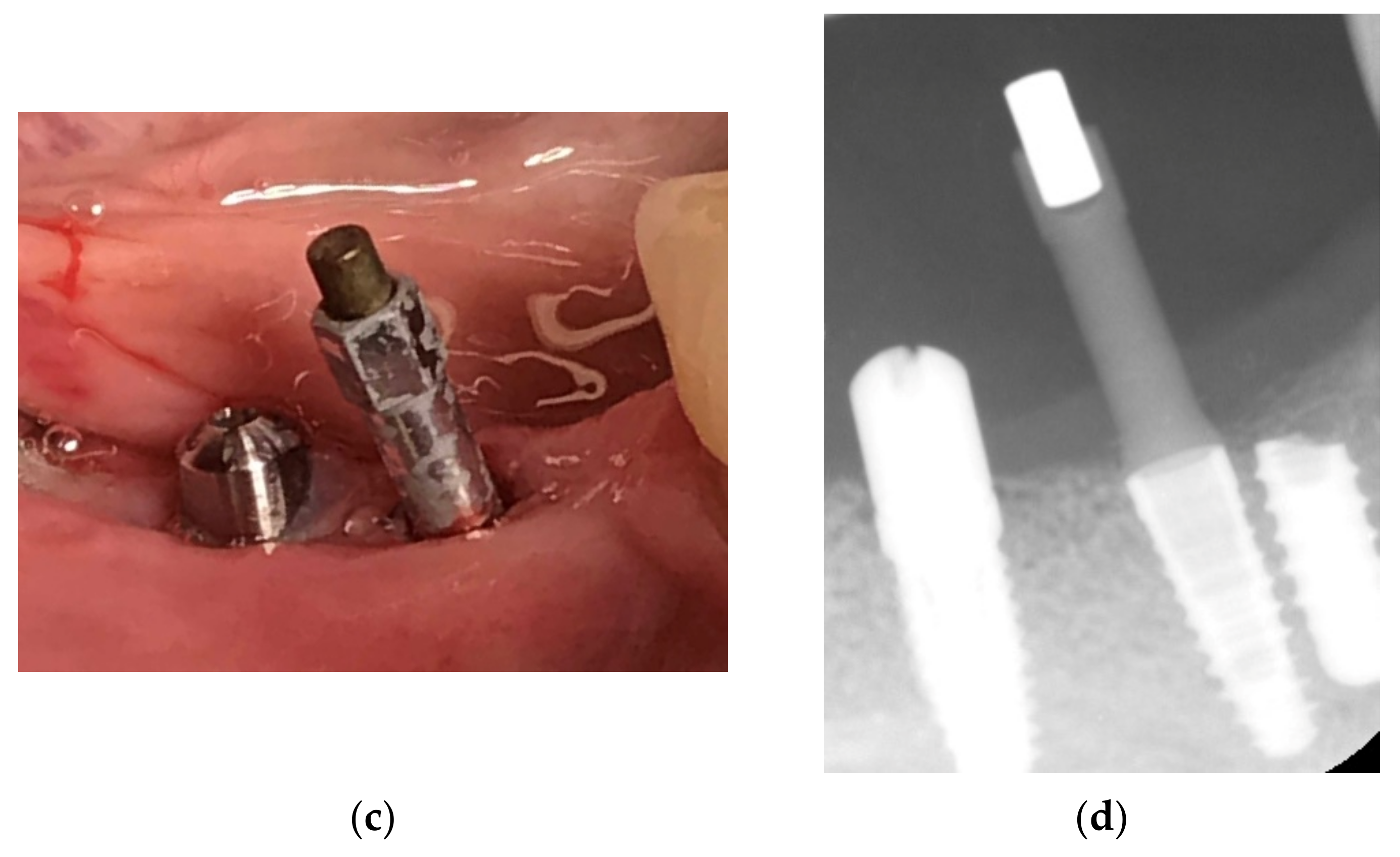
7. Implant Placement
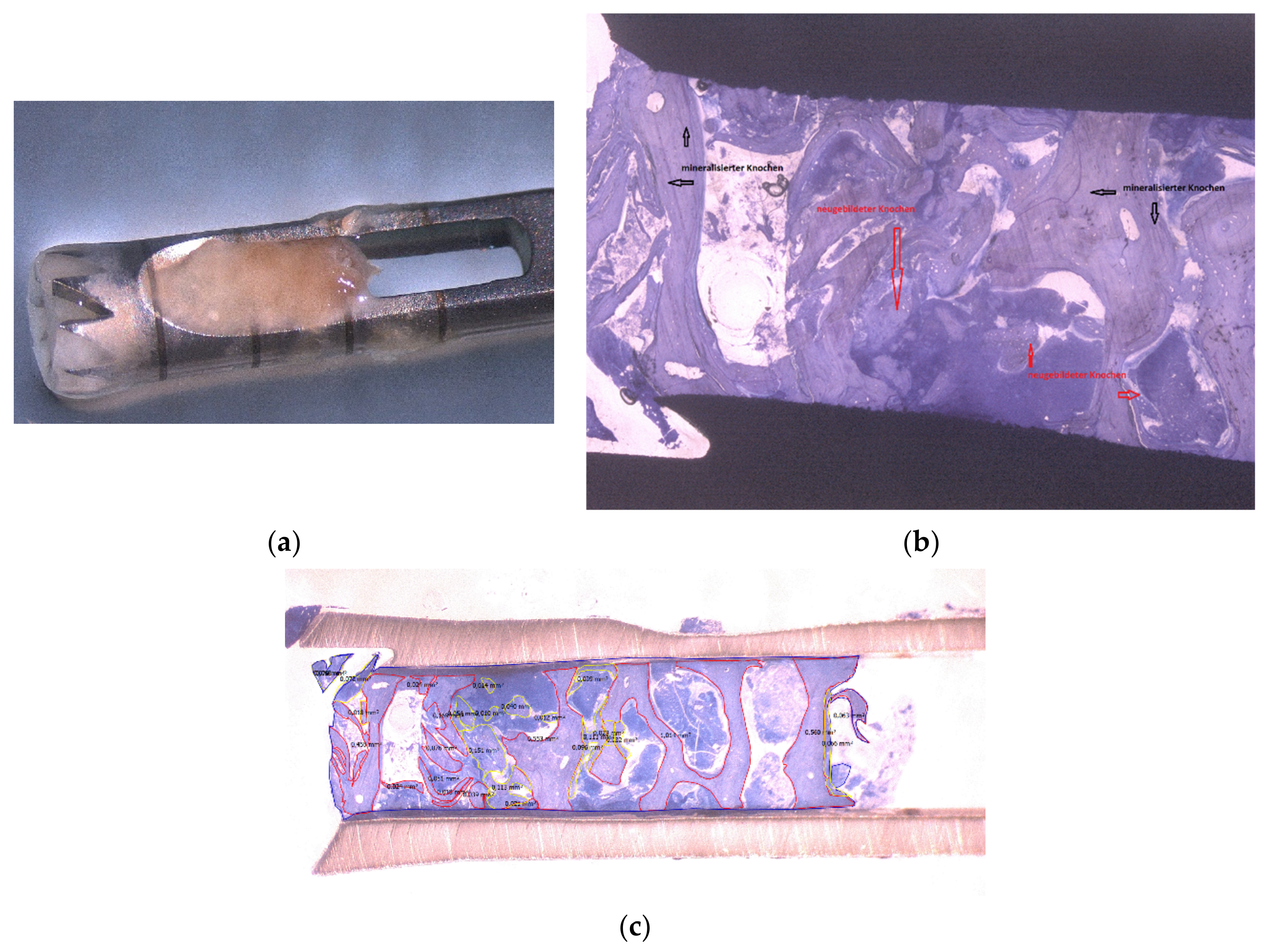
8. Histology
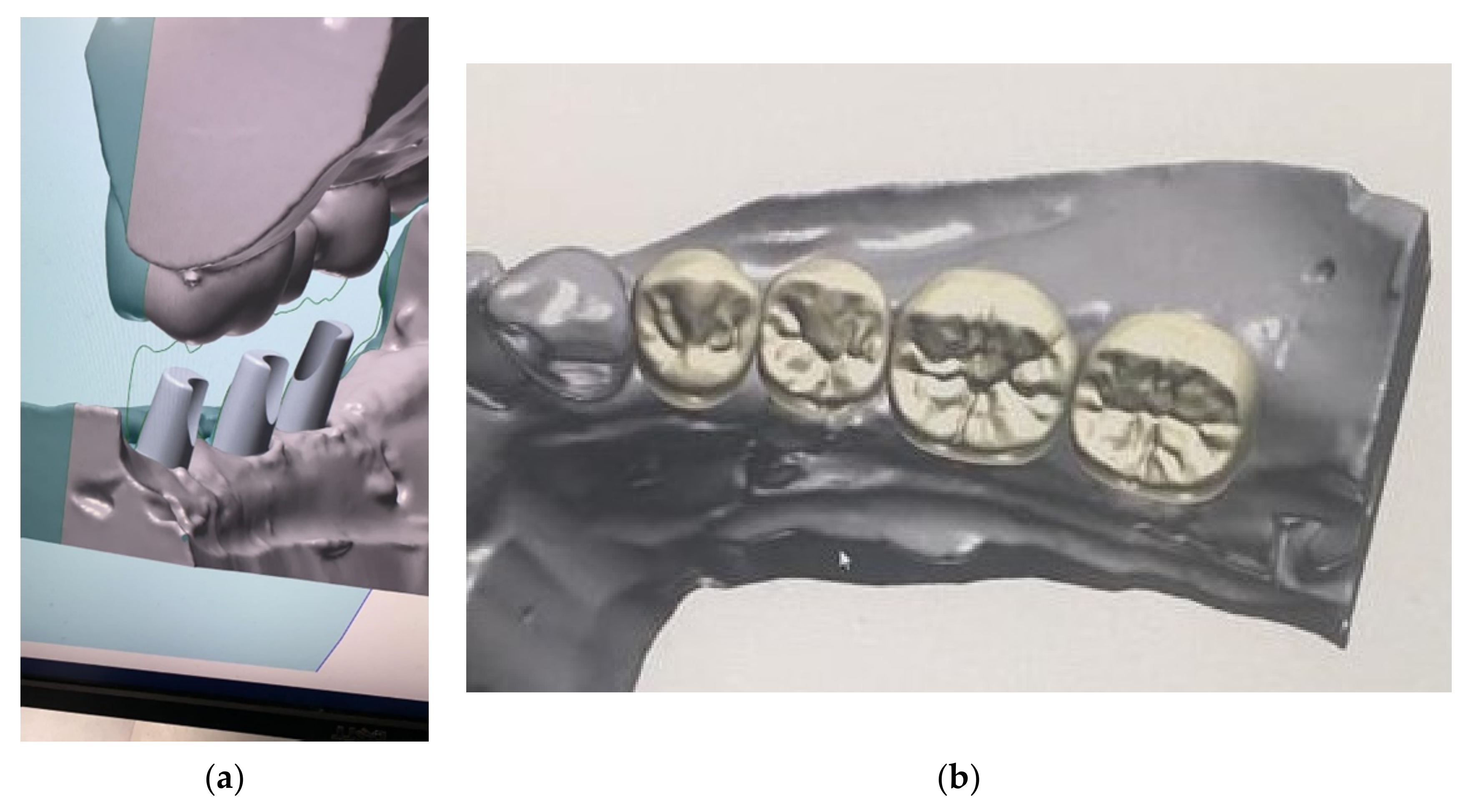
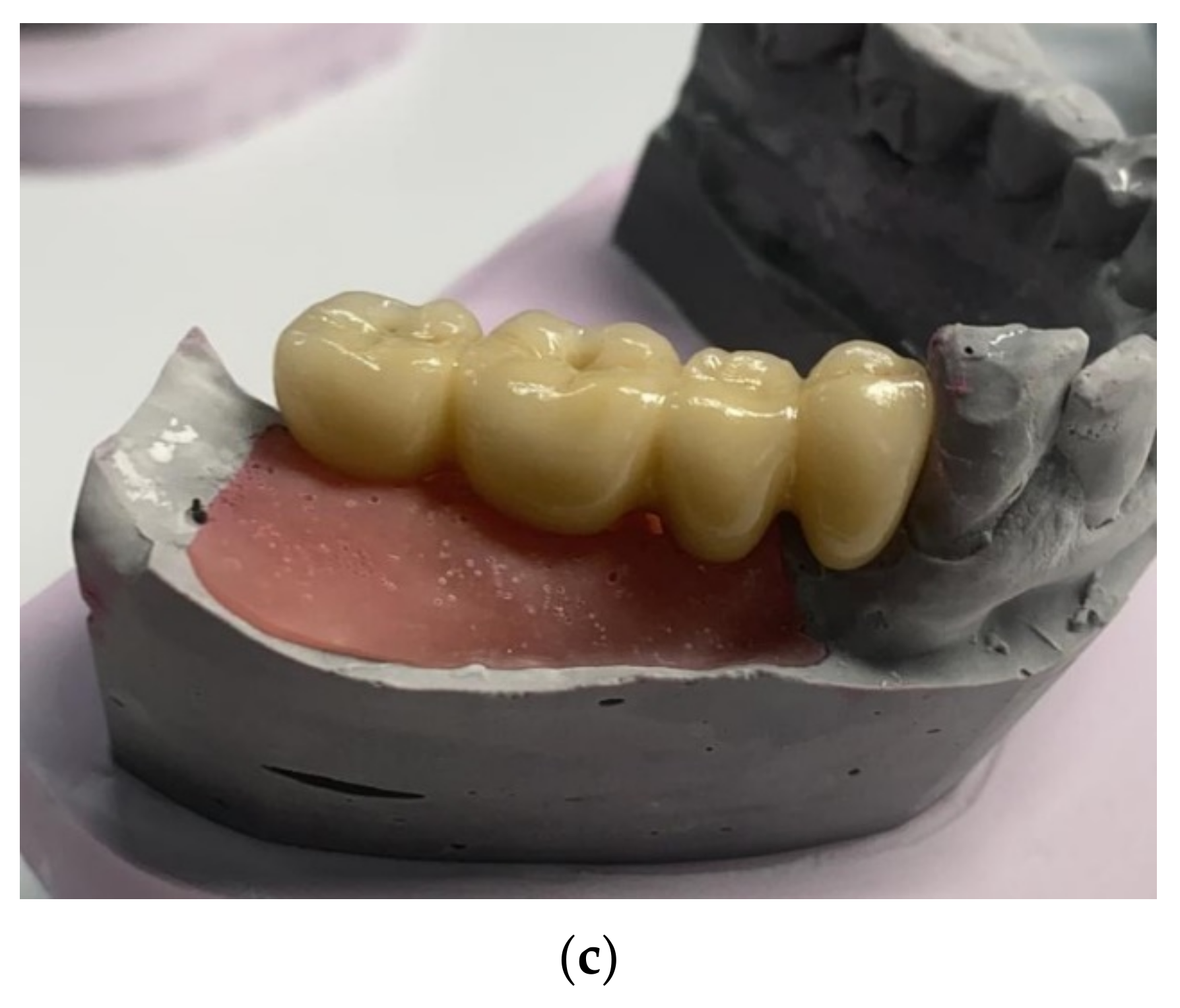
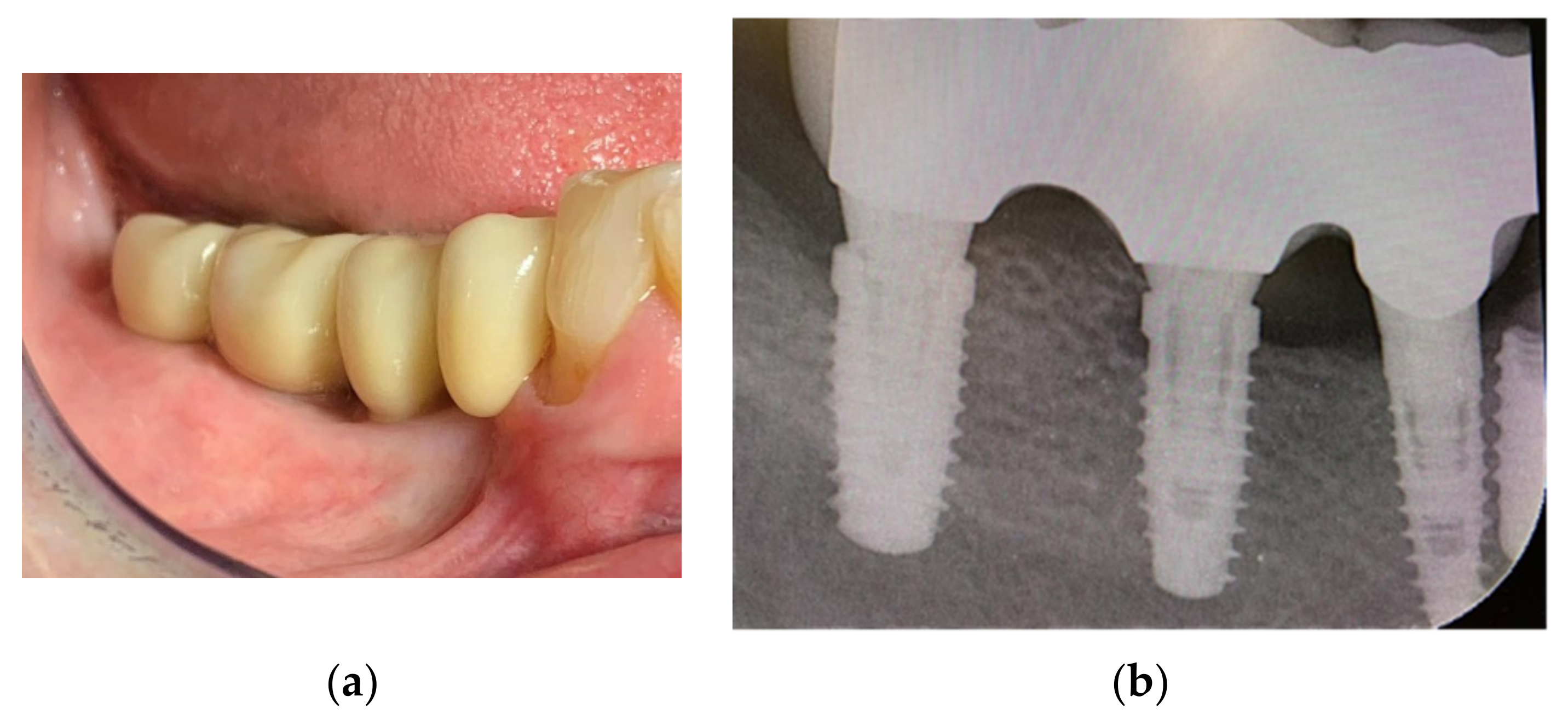
9. Prosthetic Treatment
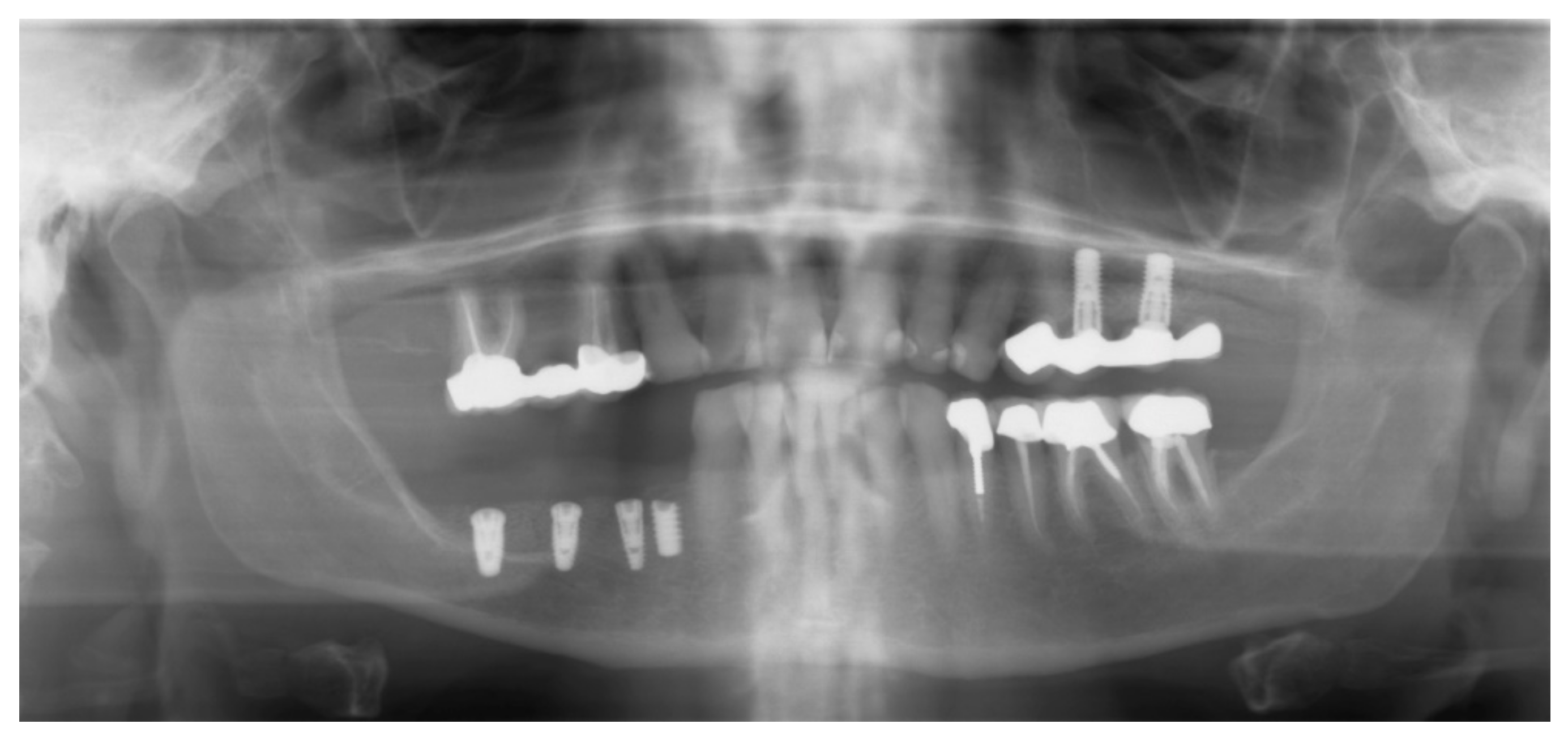
10. Follow-Up
11. Discussion
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Romanos, G.E. Severely Atrophy of the Posterior Mandible and Inferior Alveolar Nerve Transposition. Int. J. Periodontics Restor. Dent. 2021, 41, e199–e204. [Google Scholar] [CrossRef] [PubMed]
- Jacotti, M.; Barausse, C.; Felice, P. Posterior Atrophic Mandible Rehabilitation with Onlay Allograft Created with CAD-CAM Procedure: A Case Report. Implant Dent. 2014, 23, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlee, M.; Rothamel, D. Ridge augmentation using customized allogenic bone blocks: Proof of concept and histological findings. Implant Dent. 2013, 22, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blume, O.; Back, M.; Born, T.; Smeets, R.; Jung, O.; Barbeck, M. Treatment of a bilaterally severely resorbed posterior mandible due to early tooth loss by Guided Bone Regeneration using customized allogeneic bone blocks: A case report with 24 months follow-up data. J. Esthet. Restor. Dent. 2018, 30, 474–479. [Google Scholar] [CrossRef]
- Blume, O.; Donkiewicz, P.; Back, M.; Born, T. Bilateral maxillary augmentation using CAD/CAM manufactured allogenic bone blocks for restoration of congenitally missing teeth: A case report. J. Esthet. Restor. Dent. 2019, 31, 171–178. [Google Scholar] [CrossRef]
- Kloss, F.R.; Offermanns, V.; Donkiewicz, P.; Kloss-Brandstätter, A. Customized allogeneic bone grafts for maxillary horizontal augmentation: A 5-year follow-up radiographic and histologic evaluation. Clin. Case Rep. 2020, 8, 886–893. [Google Scholar] [CrossRef] [Green Version]
- Landsberg, C.; Moses, O. Ridge Augmentation Using Customized Allogeneic Bone Block: A 3-Year Follow-up of Two Case Reports. Int. J. Periodontics Restor. Dent. 2020, 40, 881–889. [Google Scholar] [CrossRef]
- Schoepf, C. Allograft Safety: The efficacy of the Tutoplast Process. Int. Mag. Oral Implantol. 2006, 1, 10–15. [Google Scholar]
- Romanos, G.E. Periosteal Releasing Incision for Successful Coverage of Augmented Sites. A Technical Note. J. Oral Implantol. 2010, 36, 25–30. [Google Scholar] [CrossRef]
- Ronda, M.; Stacchi, C. Management of a coronally advanced lingual flap in regenerative osseous surgery: A case series introducing a novel technique. Int. J. Periodontics Restor. Dent. 2011, 31, 505–513. [Google Scholar]
- Keith, J.D.; Petrungaro, P.; Leonetti, J.A.; Elwell, C.W.; Zeren, K.J.; Caputo, C.; Nikitakis, N.G.; Schopf, C.; Warner, M.M. Clinical and histologic evaluation of a mineralized block allograft: Results from the developmental period (2001–2004). Int. J. Periodontics Restor. Dent. 2006, 26, 321–327. [Google Scholar]
- Leonetti, J.A.; Koup, R. Localized maxillary ridge augmentation with a block allograft for dental implant placement: Case reports. Implant Dent. 2003, 12, 217–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanos, G. Anatomical and Biologic Considerations of Autogenous Bone Blocks Harvested from the Ramus Region. Int. J. Oral Maxillofac. Implant. 2019, 34, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Park, J.S.; Lim, S.C. Placement of implant after bone graft using J block allograft. Implant Dent. 2010, 19, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Schlee, M. Augmentation with a customized milled bone graft. Digit. Dent. News 2013, 3, 40–48. [Google Scholar]
- Donath, K. The diagnostic value of the new method for the study of undecalcified bones and teeth with attached soft tissue (Sage-Schliff (sawing and grinding) technique). Pathol. Res. Pract. 1985, 179, 631–633. [Google Scholar] [CrossRef]
- Donath, K.; Breuner, G. A method for the study of undecalcified bones and teeth with attached soft tissues. The Sage-Schliff (sawing and grinding) technique. J. Oral Pathol. 1982, 11, 318–326. [Google Scholar]
- Khoury, F.; Hanser, T. Three-Dimensional Vertical Alveolar Ridge Augmentation in the Posterior Maxilla: A 10-year Clinical Study. Int. J. Oral Maxillofac. Implant. 2019, 34, 471–480. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Mascellaro, A.; Ferrario, S.; Beretta, M. Dental implants placed in resorbed alveolar ridges reconstructed with iliac crest autogenous onlay grafts: A 26-year median follow-up retrospective study. J. Cranio Maxillofac. Surg. 2019, 47, 805–814. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Guidetti, F.; Califano, L.; Bufo, P.; Sbordone, L. Volume changes of autogenous bone after sinus lifting and grafting procedures: A 6-year computerized tomographic follow-up. J. Cranio Maxillofac. Surg. 2013, 41, 235–241. [Google Scholar] [CrossRef]
- Wiltfang, J.; Jatschmann, N.; Hedderich, J.; Neukam, F.W.; Schlegel, K.A.; Gierloff, M. Effect of deproteinized bovine bone matrix coverage on the resorption of iliac cortico-spongeous bone grafts—A prospective study of two cohorts. Clin. Oral Implant. Res. 2014, 25, e127–e132. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Finger, I.; Lytle, R. Human mineralized bone in extraction sites before implant placement: Preliminary results. J. Am. Dent. Assoc. 2002, 133, 1631–1638. [Google Scholar] [PubMed]
- Noumbissi, S.S.; Lozada, J.L.; Boyne, P.J.; Rohrer, M.D.; Clem, D.; Kim, J.S.; Prasad, H. Clinical, histologic, and histomorphometric evaluation of mineralized solvent-dehydrated bone allograf (Puros) in human maxillary sinus grafts. J. Oral Implantol. 2005, 31, 171–179. [Google Scholar] [PubMed]
- Froum, S.J.; Wallace, S.S.; Elian, N.; Cho, S.C.; Tarnow, D.P. Comparison of mineralized cancellous bone allograft (Puros) and anorganic bovine bone matrix (Bio-Oss) for sinus augmentation: Histomorphometry at 26 to 32 weeks after grafting. Int. J. Periodontics Restor. Dent. 2006, 26, 543–551. [Google Scholar]
- Tsao, Y.P.; Neiva, R.; Al-Shammari, K.; Oh, T.J.; Wang, H.L. Effects of a mineralized human cancellous bone allograft in regeneration of mandibular Class II furcation defects. J. Periodontol. 2006, 77, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Brown, D.; Wang, H.L. Sandwich bone augmentation for predictable horizontal bone augmentation. Implant Dent. 2009, 18, 282–290. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Doering, H.; Schmidt, T.; Lutz, R.; Neukam, F.W.; Schlegel, K.A. Histological results after maxillary sinus augmentation with Straumann(R) BoneCeramic, Bio-Oss(R), Puros(R), and autologous bone. A randomized controlled clinical trial. Clin. Oral Implant. Res. 2013, 24, 576–585. [Google Scholar] [CrossRef]
- Soardi, C.M.; Suarez-Lopez del Amo, F.; Galindo-Moreno, P.; Catena, A.; Zaffe, D.; Wang, H.L. Reliability of Cone Beam Computed Tomography in Determining Mineralized Tissue in Augmented Sinuses. Int. J. Oral Maxillofac. Implant. 2016, 31, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Monje, A.; O’Valle, F.; Monje-Gil, F.; Ortega-Oller, I.; Mesa, F.; Wang, H.L.; Galindo-Moreno, P. Cellular, Vascular, and Histomorphometric Outcomes of Solvent-Dehydrated vs Freeze-Dried Allogeneic Graft for Maxillary Sinus Augmentation: A Randomized Case Series. Int. J. Oral Maxillofac. Implant. 2017, 32, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Silva, F.; Lipton, D.; Tanello, B.; Duarte, W.; Witek, L.; Coelho, P.G.; Neiva, R. Clinical, Radiographic, and Histologic Comparison of Regular Mineralized and Tutoplast-derived Allograft for Alveolar Ridge Preservation. In Proceedings of the Academy of Osseointegration Annual Meeting 2019, Washington, DC, USA, 13–16 March 2019. [Google Scholar]
- Converse, J.M. Restoration of facial contour by bone grafts introduced through the oral cavity. Plast. Reconstr. Surg. 1950, 6, 295–300. [Google Scholar]
- Laino, L.; Iezzi, G.; Piattelli, A.; Lo Muzio, L.; Cicciu, M. Vertical ridge augmentation of the atrophic posterior mandible with sandwich technique: Bone block from the chin area versus corticocancellous bone block allograft—Clinical and histological prospective randomized controlled study. Biomed. Res. Int. 2014, 2014, 982104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motamedian, S.R.; Khojaste, M.; Khojasteh, A. Success rate of implants placed in autogenous bone blocks versus allogenic bone blocks: A systematic literature review. Ann. Maxillofac. Surg. 2016, 6, 78–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacotti, M.; Wang, H.L.; Fu, J.H.; Zamboni, G.; Bernardello, F. Ridge augmentation with mineralized block allografts: Clinical and histological evaluation of 8 cases treated with the 3-dimensional block technique. Implant Dent. 2012, 21, 444–448. [Google Scholar] [CrossRef]
- Kim, S.J.; Shin, H.S.; Shin, S.W. Effect of bone block graft with rhBMP-2 on vertical bone augmentation. Int. J. Oral Maxillofac. Surg. 2010, 39, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Schlee, M.; Dehner, J.-F.; Baukloh, K.; Happe, A.; Seitz, O.; Sader, R. Esthetic outcome of implant-based reconstructions in augmented bone: Comparison of autologous and allogeneic bone block grafting with the pink esthetic score (PES). Head Face Med. 2014, 10, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAllister, B.S.; Haghighat, K. Bone augmentation techniques. J. Periodontol. 2007, 78, 377–396. [Google Scholar] [CrossRef] [Green Version]
- Engler-Hamm, D. Komplexe Rehabilitation mit CAD/CAM-Knochenblöcken: Auswertung mittels DVT nach 0, 6 und 21 Monaten. Implantologie 2018, 26, 231–242. [Google Scholar]
- Gedrange, T.; Dominiak, M. Orthodontic splint treatment of patients with limited bone supply. Ger. Med. J. 2018, 23, 44–53. [Google Scholar]
- Tresguerres, F.G.F.; Tresguerres, I.F.; Iglesias, O.; Leco, I.; Tamimi, F.; Torres, J. The role of cortical perforations in allogeneic block grafting for lateral augmentation in maxilla: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2021, 1–13. [Google Scholar] [CrossRef]
- Cassetta, M.; Stefanelli, L.V.; Giansanti, M.; Di Mambro, A.; Calasso, S. Accuracy of a computer-Aided Implant Surgical Technique. Int. J. Periodontics Restor. Dent. 2013, 33, 317–325. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F.; Giansanti, M.; Bellardini, M.; Brandetti, G.; Piccoli, L. Is there a learning curve in static computer-assisted implant surgery? A prospective clinical study. Int. J. Oral Maxillofac. Surg. 2020, 49, 1335–1342. [Google Scholar] [CrossRef] [PubMed]

























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implant Site (#) | Insertion Torque | ISQ Values |
|---|---|---|
| 29 | 25 Ncm | 73 |
| 30 | 50 Ncm | 83 |
| 31 | 50 Ncm | 86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boogaard, M.J.; Romanos, G.E. Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis. Appl. Sci. 2021, 11, 10413. https://doi.org/10.3390/app112110413
Boogaard MJ, Romanos GE. Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis. Applied Sciences. 2021; 11(21):10413. https://doi.org/10.3390/app112110413
Chicago/Turabian StyleBoogaard, Maarten J., and Georgios E. Romanos. 2021. "Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis" Applied Sciences 11, no. 21: 10413. https://doi.org/10.3390/app112110413
APA StyleBoogaard, M. J., & Romanos, G. E. (2021). Allograft Customized Bone Blocks for Ridge Reconstruction: A Case Report and Radiological Analysis. Applied Sciences, 11(21), 10413. https://doi.org/10.3390/app112110413