
Complexity Analysis in the PR, QT, RR and ST Segments of ECG for Early Assessment of Severity in Cardiac Autonomic Neuropathy


 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. ECG Data
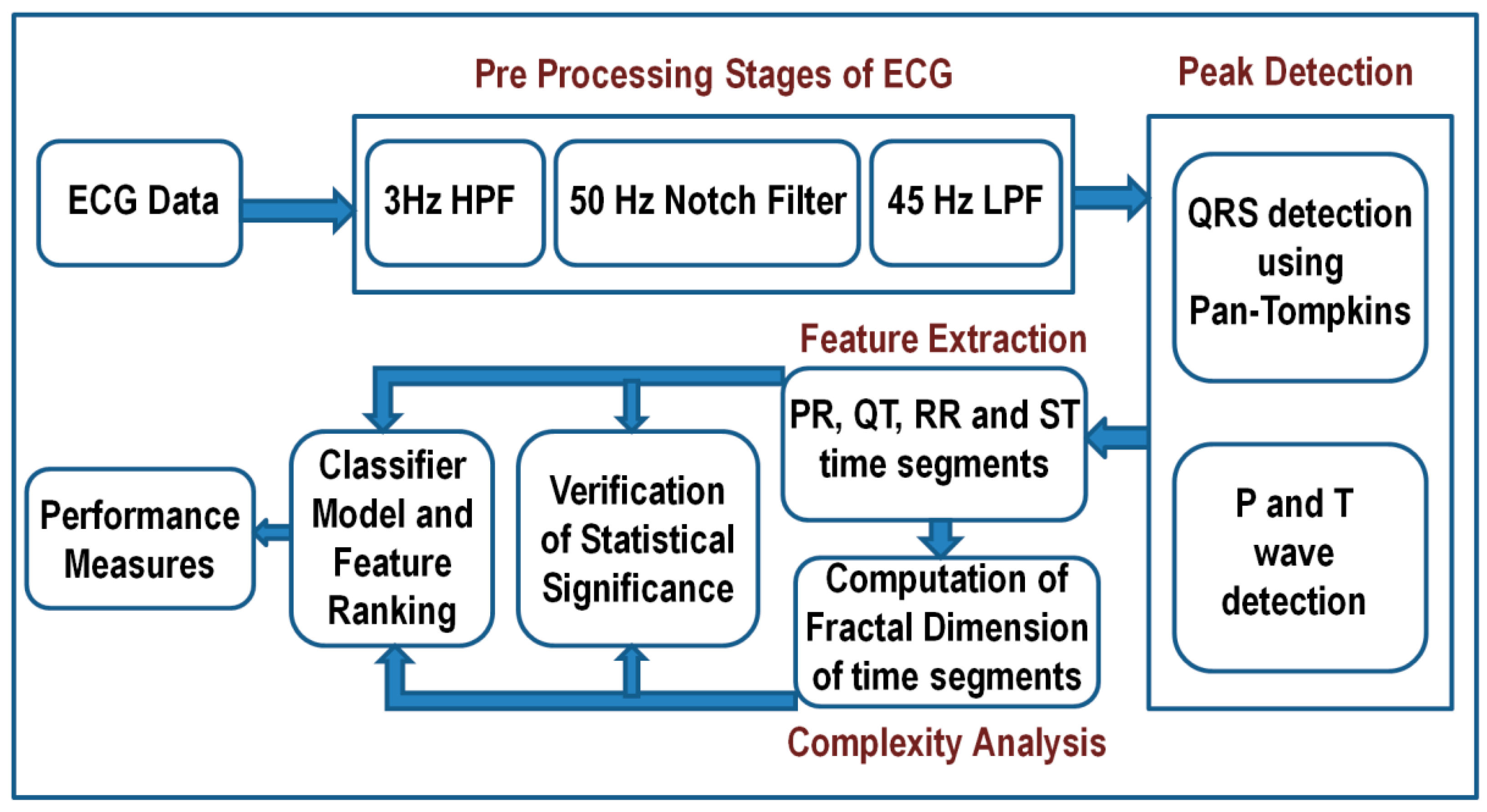
2.2. The Schematic of Data Analysis
- Read the ECG signal.
- Implement signal preprocessing to remove noise.
- Feature extraction (QRS complex, P and T point) from ECG.
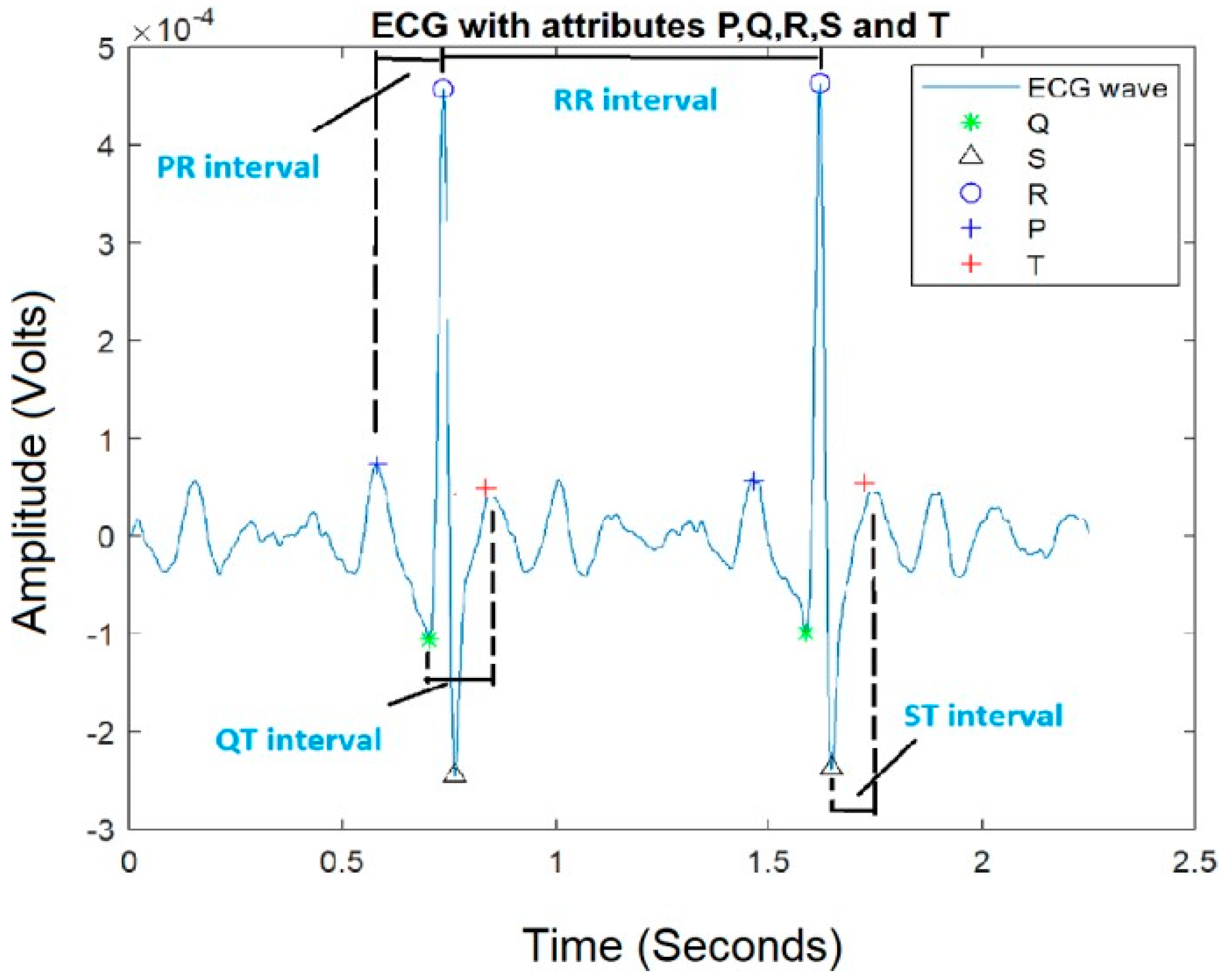
- Extract time intervals from ECG segments (say, PR, QT, RR, and ST).
- Analyze the data at four instants of time within the same signal for each segment to study the complexity variation.
- Statistical validation for the analyzed time segments for identification of CAN.
- Classification of time and complexity features with different classifier models and feature ranking.
- Performance measure of classifiers used.
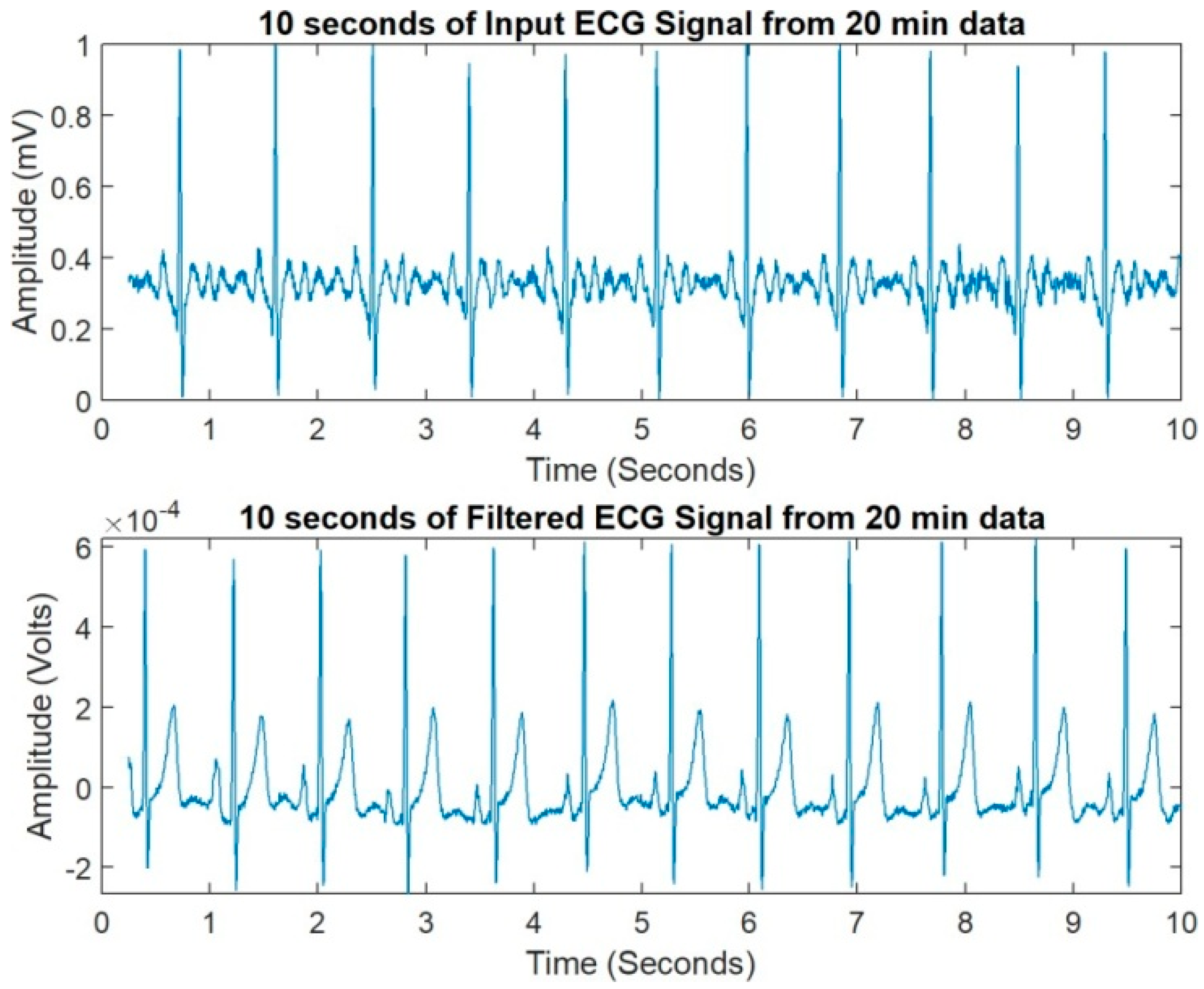
2.3. Signal Preprocessing
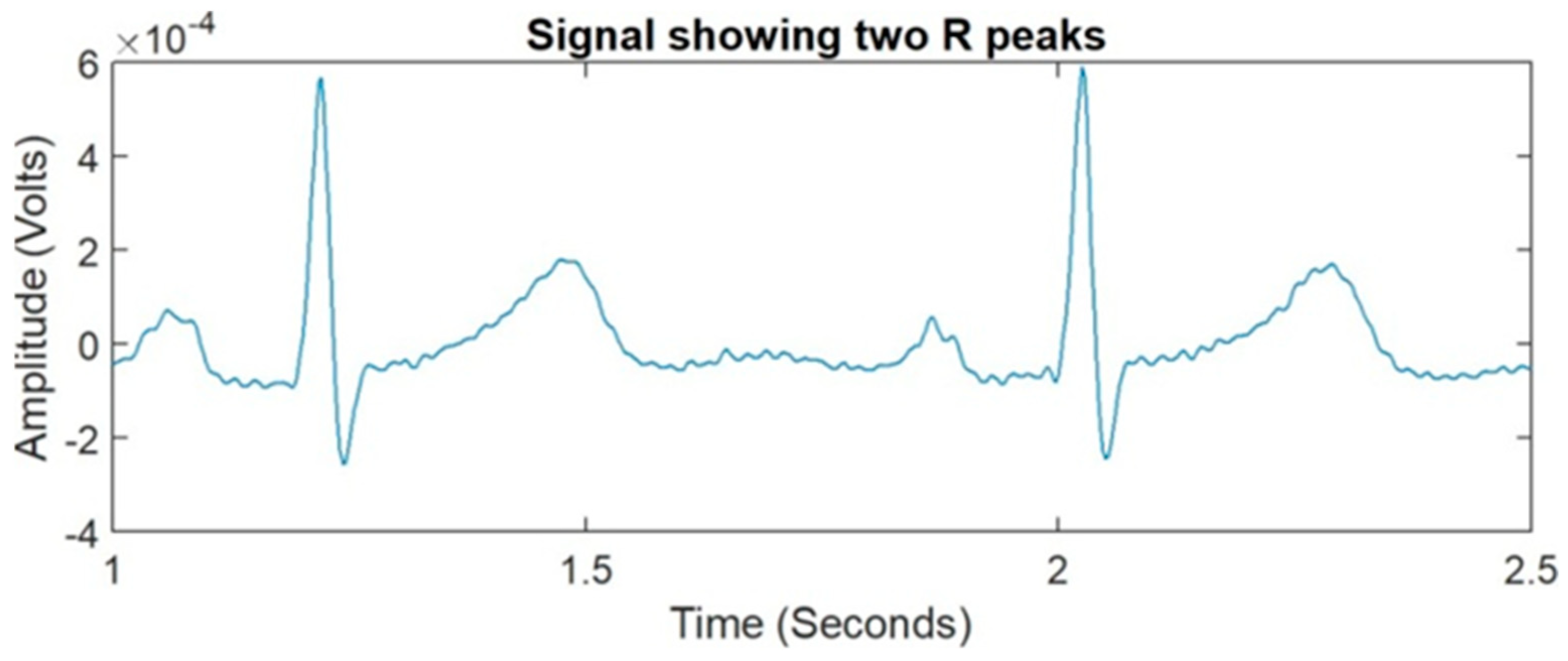
2.4. Segment Extraction from ECG
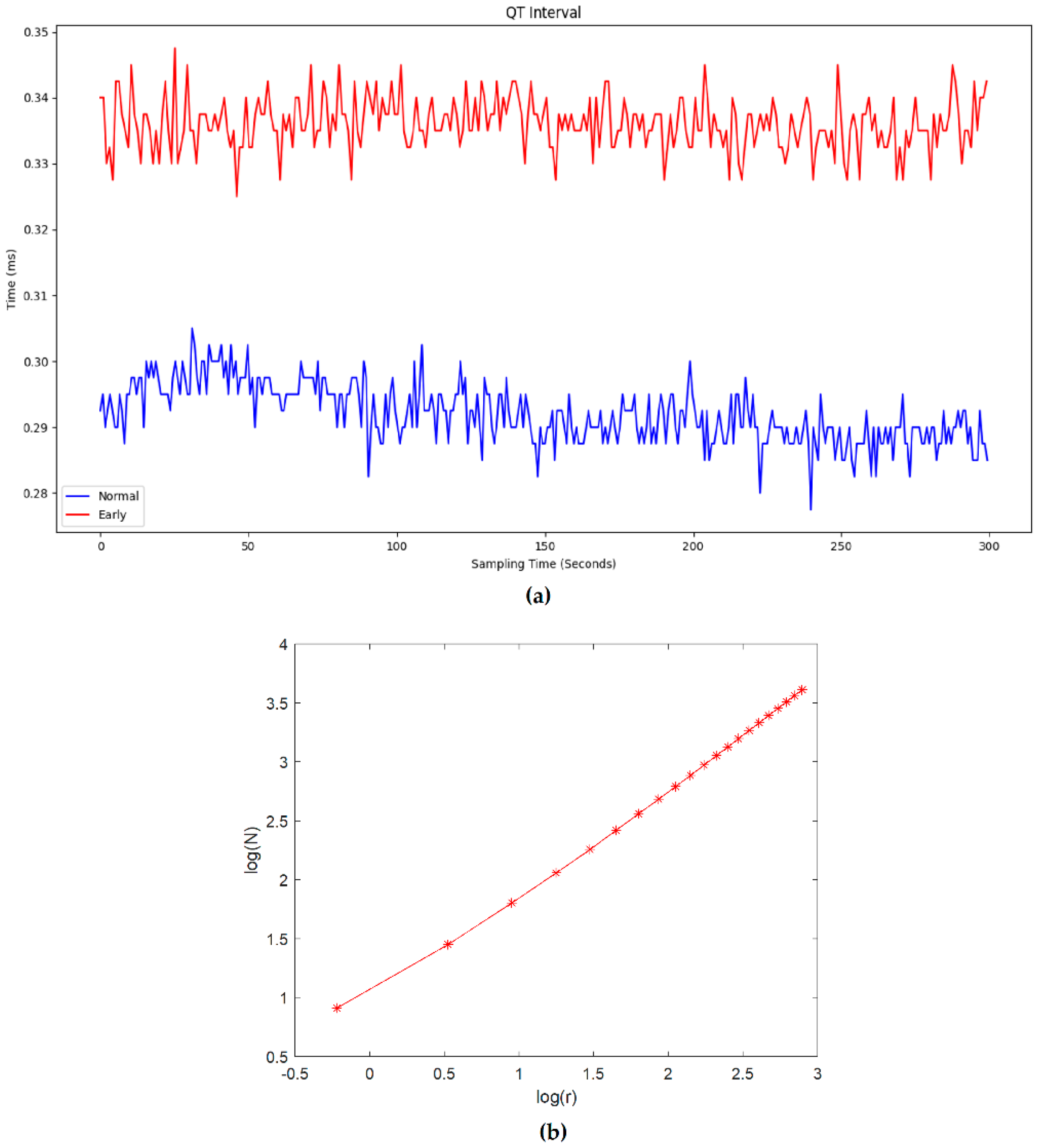
2.5. Complexity Analysis
2.6. Statistical Analysis
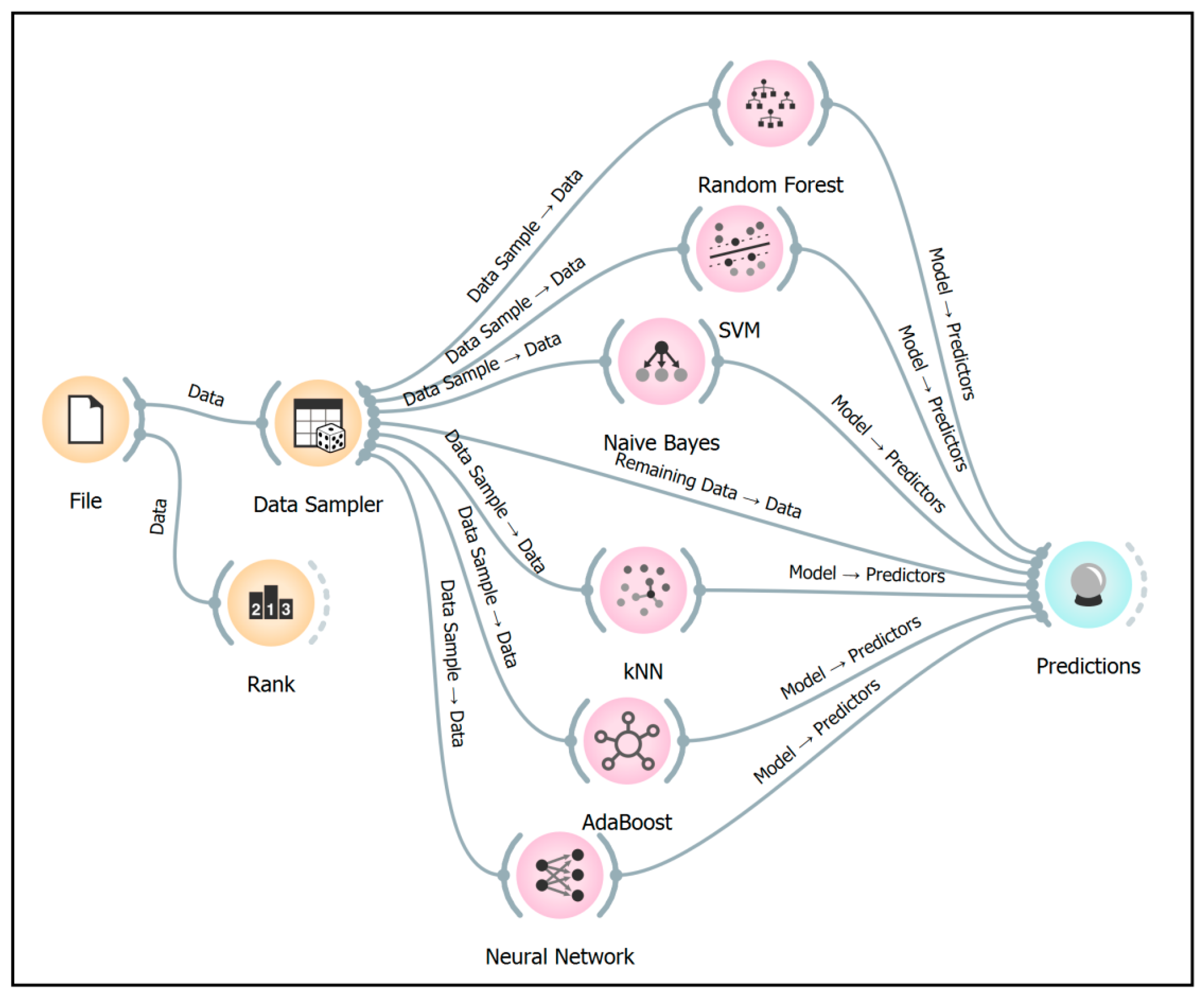
2.7. Classifier and Feature Validation
- File upload: Consisting of ECG signal of one subject, split at every 5th interval. In each signal, approximately 44 PR, QT, RR, and ST segments were extracted and given to the classifier as separate instances (inputs). A total of 120 instances (30 signals × 4 intervals) were classified based on 180 features (4 time segments × 44 and 4 FD values).
- Data sampler: A total of 70% of data were used for training and 30% for testing, with 10-fold cross validation performed to identify the accuracy.Data sample → Data: indicates the data given to the classifier model.Remaining data → Data: indicates the test data given to the prediction.Model → Predictors: indicates the trained data from model given to prediction.
- Different supervised models, including random forest (RF), support vector machine (SVM), K-nearest neighbor (KNN), naïve Bayes (NB), AdaBoost (AB), and neural network (NN) [32], were used to classify.
- Prediction: All the models are linked to the prediction for identifying the classification accuracy. The remaining data mentioned in the model are used as the test data for computing the classification accuracy.
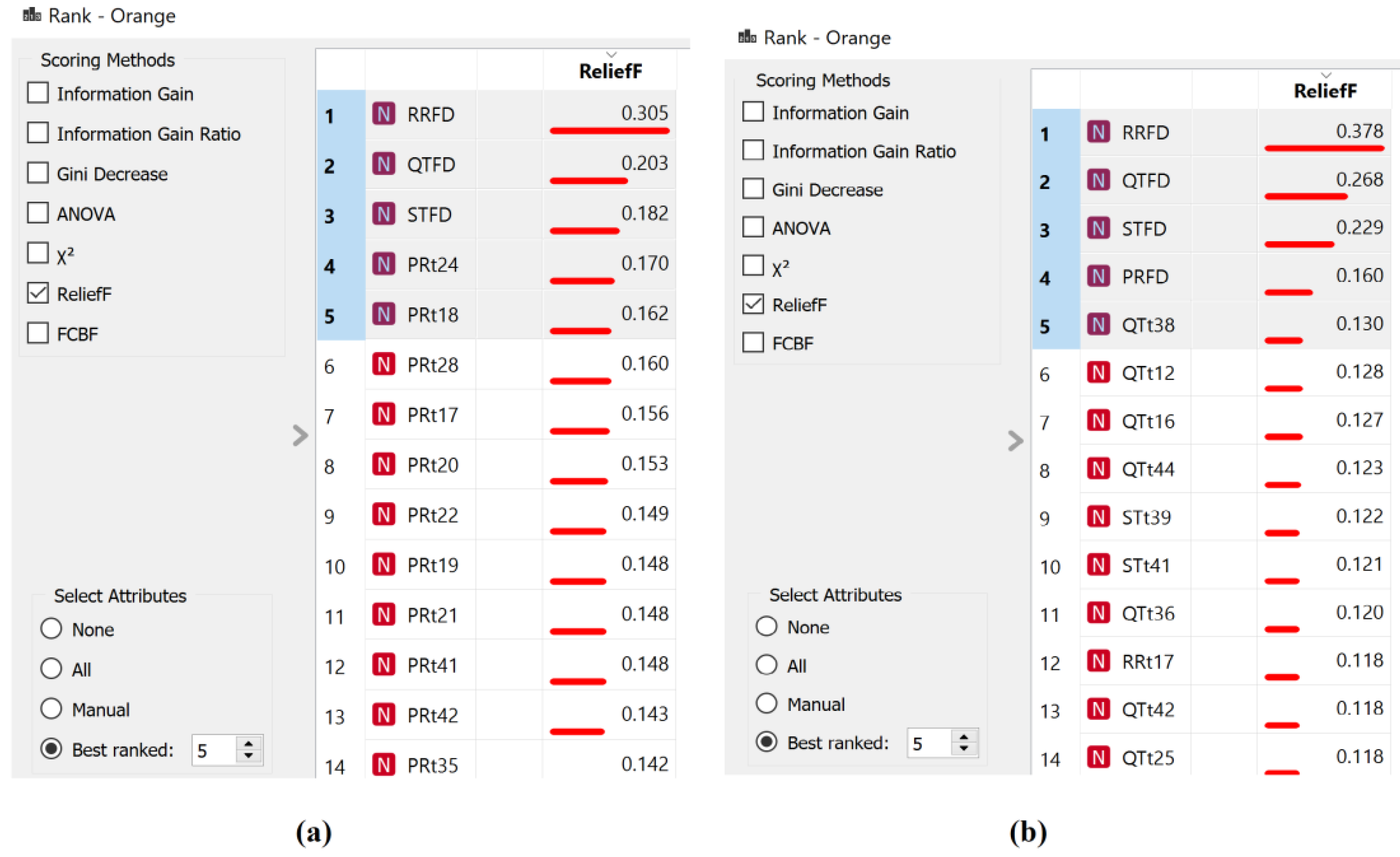
- Ranking using ReliefF estimator [33] was analyzed, which ranks the best contributing feature for classification.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bissinger, A. Cardiac Autonomic Neuropathy: Why Should Cardiologists Care about That? J. Diabetes Res. 2017, 2017, 5374176. [Google Scholar] [CrossRef] [Green Version]
- Bhuyan, A.K.; Baro, A.; Sarma, D.; Choudhury, B. A study of cardiac autonomic neuropathy in patients with type 2 diabetes mellitus: A North east India experience. Indian J. Endocrinol. Metab. 2019, 23, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Moţăţăianu, A.; Maier, S.; Bajko, Z.; Voidazan, S.; Bălaşa, R.; Stoian, A. Cardiac autonomic neuropathy in type 1 and type 2 diabetes patients. BMC Neurol. 2018, 18, 126. [Google Scholar] [CrossRef]
- Oakley, I.; Emond, L. Diabetic cardiac autonomic neuropathy and anesthetic management: Review of the literature. AANAJ. 2011, 79, 473–479. [Google Scholar]
- Imam, M.H.; Karmakar, C.K.; Jelinek, H.F.; Palaniswami, M.; Khandoker, A.H. Analyzing systolic-diastolic interval interaction characteristics in diabetic cardiac autonomic neuropathy progression. IEEE J. Transl. Eng. Health Med. 2015, 3, 1900510. [Google Scholar] [CrossRef]
- Serhiyenko, V.A.; Serhiyenko, A.A. Cardiac autonomic neuropathy: Risk factors, diagnosis and treatment. World J. Diabetes 2018, 9, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Vinik, A.I.; Erbas, T.; Casellini, C.M. Diabetic cardiac autonomic neuropathy, inflammation and cardiovascular disease. J. Diabetes Investig. 2013, 4, 4–18. [Google Scholar] [CrossRef]
- Sidek, K.A.; Jelinek, H.F.; Khalil, I. Identification of cardiac autonomic neuropathy patients using cardioid-based graph for ECG biometric. Comput. Cardiol. 2011, 38, 517–520. [Google Scholar]
- Tekeste, T.; Saleh, H.; Mohammad, B.; Khandoker, A.; Jelinek, H.; Ismail, M. A Nanowatt Real-Time Cardiac Autonomic Neuropathy Detector. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 739–750. [Google Scholar] [CrossRef] [PubMed]
- Bosen, D.; Flemming, M. Beyond ECGs: Understanding electrophysiology testing, part 2. Nursing 2003, 33, cc1–cc32. [Google Scholar] [CrossRef]
- Cornforth, D.; Jelinek, H.F.; Tarvainen, M. A comparison of nonlinear measures for the detection of cardiac autonomic neuropathy from heart rate variability. Entropy 2015, 17, 1425–1440. [Google Scholar] [CrossRef] [Green Version]
- Khandoker, A.H.; Jelinek, H.F.; Moritani, T.; Palaniswami, M. Association of cardiac autonomic neuropathy with alteration of sympatho vagal balance through heart rate variability analysis. Med. Eng. Phys. 2010, 32, 161–167. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Imam, M.H.; Couderc, J.P.; Palaniswami, M.; Jelinek, H.F. QT variability index changes with severity of cardiovascular autonomic neuropathy. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 900–906. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Boularaoui, S.; Alhussein, G.M.; Almatroushi, N.S.O.; Osman, E.A.A.; Widatalla, N.S.M.; Khalaf, K.; Jelinek, H. Screening ST segments in patients with cardiac autonomic neuropathy. Comput. Cardiol. 2012, 39, 621–623. [Google Scholar]
- Burguera, A. Fast QRS Detection and ECG Compression Based on Signal Structural Analysis. IEEE J. Biomed. Health Inform. 2019, 23, 123–131. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Jelinek, H.F.; Palaniswami, M. Heart rate variability and complexity in people with diabetes associated cardiac autonomic neuropathy. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2008, 2008, 4696–4699. [Google Scholar] [CrossRef] [PubMed]
- Arjunan, S.P.; Kumar, D.K. Decoding subtle forearm flexions using fractal features of surface electromyogram from single and multiple sensors. J. Neuroeng. Rehabil. 2010, 7, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magrans, R.; Gomis, P.; Caminal, P.; Voss, A. Higuchi’s fractal complexity of RR and QT interval series during transient myocardial ischemia. Comput.Cardiol. 2013, 40, 421–424. [Google Scholar]
- Escalona, O.J.; Mendoza, M.; Villegas, G.; Navarro, C. Real-time system for high-resolution ECG diagnosis based on 3D late potential fractal dimension estimation. Comput. Cardiol. 2011, 38, 789–792. [Google Scholar]
- Jallouli, M.; Arfaoui, S.; Ben Mabrouk, A.; Cattani, C. Clifford wavelet entropy for fetal ECG extraction. Entropy 2021, 23, 844. [Google Scholar] [CrossRef]
- Limaye, H.; Deshmukh, V.V. ECG Noise Sources and Various Noise Removal Techniques: A Survey. Int. J. Appl. Innov.Eng. Manag. 2016, 5, 2319–4847. [Google Scholar]
- Sedghamiz, H. Matlab Implementation of Pan Tompkins ECG QRS; 2014; pp. 1–3. Available online: https://www.researchgate.net/publication/313673153_Matlab_Implementation_of_Pan_Tompkins_ECG_QRS_detector (accessed on 25 April 2022).
- Mary, H.M.C.; Singh, D.; Deepak, K.K. Assessment of Scale Invariance Changes in Heart Rate Signal During Postural Shift. IETEJ. Res. 2019, 2063, 308–314. [Google Scholar] [CrossRef]
- Jelinek, H.F.; Fernandez, E. Neurons and fractals: How reliable and useful are calculations of fractal dimensions? J. Neurosci. Methods 1998, 81, 9–18. [Google Scholar] [CrossRef]
- Becker, D.E. Fundamentals of electrocardiography interpretation. Anesth. Prog. 2006, 53, 53–64. [Google Scholar] [CrossRef] [Green Version]
- Kiani, K.; Maghsoudi, F. Classification of 7 Arrhythmias from ECG Using Fractal Dimensions. J. Bioinforma. Syst. Biol. 2019, 2, 53–65. [Google Scholar] [CrossRef]
- Bouda, M.; Caplan, J.S.; Saiers, J.E. Box-counting dimension revisited: Presenting an efficient method of minimizing quantization error and an assessment of the self-similarity of structural root systems. Front. Plant Sci. 2016, 7, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jäntschi, L.; Bolboacă, S.D. Computation of probability associated with Anderson-Darling statistic. Mathematics 2018, 6, 88. [Google Scholar] [CrossRef] [Green Version]
- Van Hecke, T. Power study of ANOVA versus Kruskal-Wallis test. J. Stat. Manag. Syst. 2012, 15, 241–247. [Google Scholar] [CrossRef]
- Jelinek, H.F.; Abawajy, J.H.; Cornforth, D.J.; Kowalczyk, A.; Negnevitsky, M.; Chowdhury, M.U.; Krones, R.; Kelarev, A.V. Multi-layer Attribute Selection and Classification Algorithm for the Diagnosis of Cardiac Autonomic Neuropathy Based on HRV Attributes. AIMS Med. Sci. 2015, 2, 396–409. [Google Scholar] [CrossRef]
- Naik, A.; Samant, L. Correlation Review of Classification Algorithm Using Data Mining Tool: WEKA, Rapidminer, Tanagra, Orange and Knime. Procedia Comput. Sci. 2016, 85, 662–668. [Google Scholar] [CrossRef] [Green Version]
- Kavakiotis, I.; Tsave, O.; Salifoglou, A.; Maglaveras, N.; Vlahavas, I.; Chouvarda, I. Machine Learning and Data Mining Methods in Diabetes Research. Comput. Struct. Biotechnol. J. 2017, 15, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Robnik-Šikonja, M.; Kononenko, I. Theoretical and Empirical Analysis of ReliefF and RReliefF. Mach. Learn. 2003, 53, 23–69. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, Y.; Das, J.; Mazumder, P.M.; Kumar, R.; Sinha, R.K. Heart rate variability features from nonlinear cardiac dynamicsin the identification of diabetes using artificial neural network and support vector machine. Biocybern. Biomed. Eng. 2020, 40, 1002–1009. [Google Scholar] [CrossRef]
- Rolim, L.C.; de Souza, J.S.T.; Dib, S.A. Tests for early diagnosis of cardiovascular autonomic neuropathy: Critical analysis and relevance. Front. Endocrinol. 2013, 4, 2–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Age | Gender |
|---|---|---|
| Normal (10 participants) | 45–60 years | Male, 5: Female, 5 |
| Early (10 participants) | 50–62 years | Male, 5: Female, 5 |
| Definite (7 participants) | 52–61 years | Male, 4: Female, 3 |
| Severe (3 participants) | 55–60 years | Male, 2: Female, 1 |
| Sample for study: 480,000 participants | ||
| Type of Classifier | Parameter |
|---|---|
| Random Forest | Number of trees: 10 |
| Number of attributes at each split: 5 | |
| SVM | Regression loss (ε): 0.10 |
| Kernel: radial basis function (RBF) | |
| KNN | Weight: Euclidean uniform |
| Number of neighbors: 5 | |
| AdaBoost | Number of estimators: 50 |
| Regression loss function: linear | |
| Neural Network (NN) | Number of hidden layer neurons: 100 |
| Number of iterations: 200 | |
| Activation: ReLu |
| Segment | The p-Value for the Whole 20-Minute Recording | ||
|---|---|---|---|
| Normal vs. eCAN | eCAN vs. dCAN | Normal vs. Stages of CAN | |
| PR interval | 0.45 | 0.20 | 0.34 |
| QT interval | 0.46 | 0.20 | 0.33 |
| RR interval | 0.46 | 0.24 | 0.34 |
| ST interval | 0.46 | 0.25 | 0.34 |
| Segment | p-Value of FD Computed for Segments at Every 5th Minute | ||
|---|---|---|---|
| Normal vs. eCAN | eCAN vs. dCAN | Normal vs. Stages of CAN | |
| FD of PR interval | 0.013 | 0.005 * | 0.002 * |
| FD of QT interval | 0.007 * | 0.002 * | 0.0005 * |
| FD of RR interval | 0.007 * | 0.002 * | 0.0005 * |
| FD of ST interval | 0.009 * | 0.001 * | 0.0001 * |
| PR interval | 0.45 | 0.19 | 0.34 |
| QT interval | 0.45 | 0.19 | 0.34 |
| RR interval | 0.45 | 0.20 | 0.35 |
| ST interval | 0.45 | 0.20 | 0.34 |
| Model | Area under ROC Curve (AUC) | Classification Accuracy (CA) | ||
|---|---|---|---|---|
| Normal vs. Early CAN | Normal vs. Stages of CAN | Normal vs. Early CAN | Normal vs. Stages of CAN | |
| Random Forest | 0.97 | 0.88 | 87.5 | 88.9 |
| SVM | 0.99 | 0.92 | 96.8 | 94.4 |
| KNN | 0.85 | 0.97 | 71.9 | 88.9 |
| Naïve Bayes | 0.89 | 0.84 | 81.2 | 77.8 |
| AdaBoost | 0.87 | 0.87 | 87.5 | 88.9 |
| Neural Network (NN) | 0.99 | 0.99 | 96.9 | 97.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senthamil Selvan, S.; Arjunan, S.P.; Swaminathan, R.; Kumar, D.K. Complexity Analysis in the PR, QT, RR and ST Segments of ECG for Early Assessment of Severity in Cardiac Autonomic Neuropathy. Appl. Sci. 2022, 12, 5746. https://doi.org/10.3390/app12115746
Senthamil Selvan S, Arjunan SP, Swaminathan R, Kumar DK. Complexity Analysis in the PR, QT, RR and ST Segments of ECG for Early Assessment of Severity in Cardiac Autonomic Neuropathy. Applied Sciences. 2022; 12(11):5746. https://doi.org/10.3390/app12115746
Chicago/Turabian StyleSenthamil Selvan, Sharanya, Sridhar P. Arjunan, Ramakrishnan Swaminathan, and Dinesh Kant Kumar. 2022. "Complexity Analysis in the PR, QT, RR and ST Segments of ECG for Early Assessment of Severity in Cardiac Autonomic Neuropathy" Applied Sciences 12, no. 11: 5746. https://doi.org/10.3390/app12115746
APA StyleSenthamil Selvan, S., Arjunan, S. P., Swaminathan, R., & Kumar, D. K. (2022). Complexity Analysis in the PR, QT, RR and ST Segments of ECG for Early Assessment of Severity in Cardiac Autonomic Neuropathy. Applied Sciences, 12(11), 5746. https://doi.org/10.3390/app12115746