In this sense, in this section, a human tibia was modeled in 3D, on which the simulation of the OWHTO operation was performed virtually. Three-dimensional models of the osteosynthesis plate and the fixing screws were also made and, finally, using these 3D models, the 3D assembly of the tibia operated with the applied fixing system was made.
2.1.1. Three-Dimensional Modeling of the Tibia Taking into Account the Real Structures of the Bone
Regarding the 3D modeling of the tibia, there is a trend in the literature for using 3D bone models without taking into account the real heterogeneous structure of human bones [
28,
29]. Given the use of such models, a number of important research limitations may arise. Therefore, in this research, the aim was to create the CAD model of a real human tibia, constituted as a set of several structural entities with different dimensional, geometric, anatomical and mechanical characteristics.
To achieve this goal, we started from a 3D professional model of a human tibia purchased from the ZYGOTE company, a world leader in 3D anatomical modeling.
Figure 1 shows this initial model, highlighting from a dimensional point of view, the total length of the tibia, measured from the tibiotalar joint to the tibial spine (376 mm), its width in the tibial plateau area (78 mm) and the length of the diaphysis, which is 272 mm. Additionally, the three important areas of the bone are presented, namely, distal epiphysis, diaphysis and proximal epiphysis, respectively. The mentioned dimensions are important, being reference elements in the dimensional characterization of the tibia. Starting from these and using quantitative computed tomography (hereinafter QCT) and images or previous research [
30,
31,
32,
33], it was possible to make the necessary correlations to model the real entities of which the tibia is constituted.
As is known [
31,
32], the 3 components of the tibia mentioned above are structurally different. The diaphysis has a tubular structure made of cortical bone, is compact, with a variable thickness. Inside this structure is the medullary cavity filled with bone marrow. The two epiphyses that form the extremities of the tibia have a heterogeneous bone structure, being formed both of the cortical bone hard to the outside, and of the trabecular or spongy bone inside.
CAD modeling was performed in Catia V5R20 software, taking into account the elements mentioned above.
The main stages of modeling were:
A. CAD Modeling of the Epiphysis
Figure 2 shows the 3D models obtained for the two epiphyses, each of which is the set of two entities corresponding to the areas of cortical and trabecular bone.
In order to obtain the models for the compact cortical bone area, a spatial off-setting (from the initial model) of the external surfaces of the two epiphyses was performed. The size of the offset, which represents the thickness of the cortical bone at the level of the epiphyses, was adopted of 2.5 mm, a value taken from the literature [
30].
For the modeling of the areas formed by the trabecular bone, Boolean operations were used to extract from the initial model of the previously modeled compact cortical bone entities, the extracted part (the green one in
Figure 2) thus becoming the 3D model of the trabecular structure of the epiphyses.
B. CAD Modeling of the Diaphysis and Metaphysis
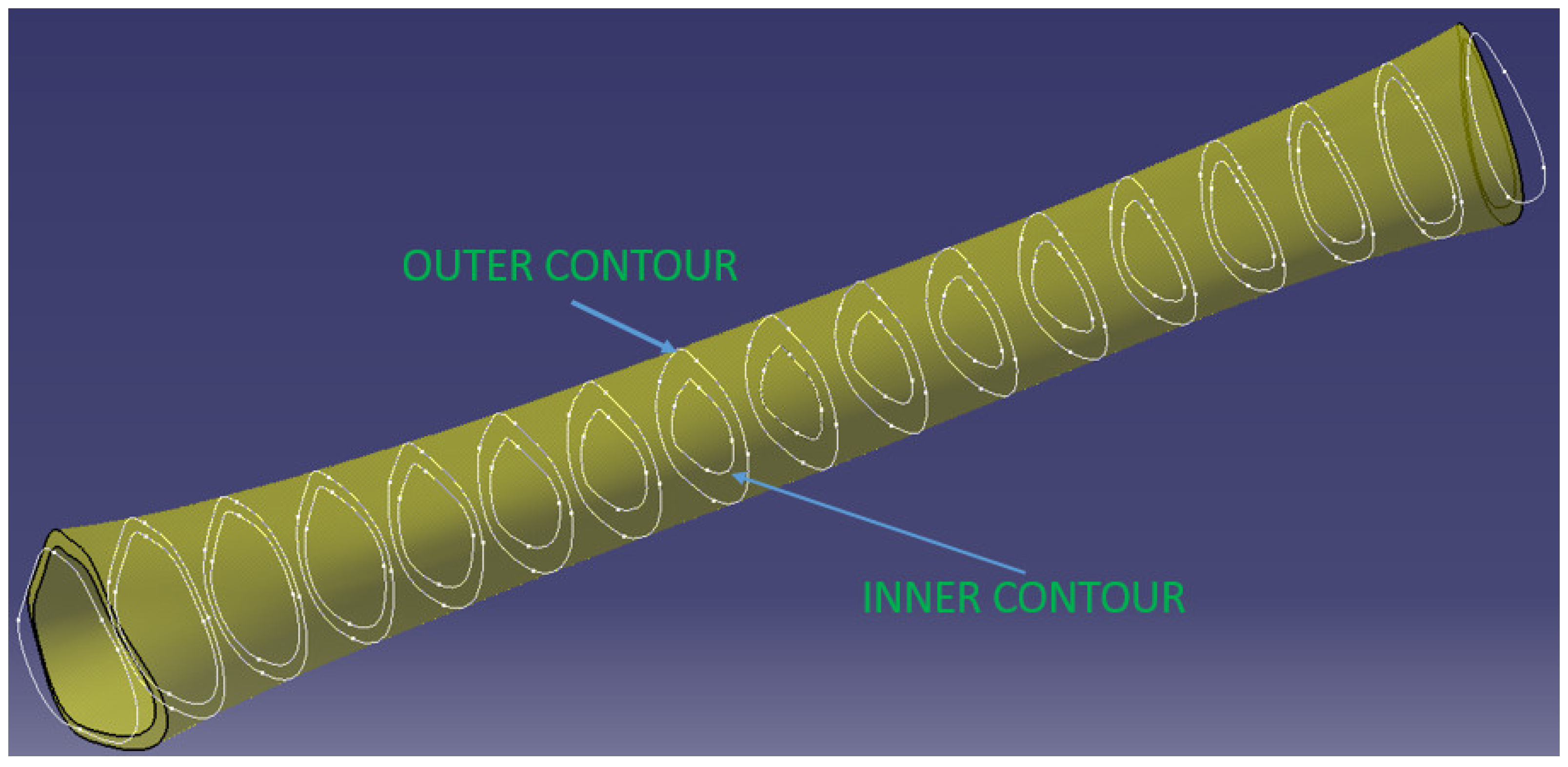
The diaphysis’ modeling was more complex due to its variable geometry. In order to obtain the real tubular structure, a sectioning of the initial model of the diaphysis was first performed, which has a length of 272 mm, with 17 planes perpendicular to the tibia, positioned equidistantly. In the case of the real diaphysis, each of these sections is characterized by an outer and an inner contour. Determining these contours and then linking them to CatiaV5R20-specific Solid MultiSection functions makes it possible to obtain the CAD model of the diaphysis entity.
Specifically, the outer contours of each of the 17 sections were first determined using the initial model, resulting in intersections between the sectioned planes corresponding to each section and the body of the diaphysis (
Figure 3).
To model the inner surface, and the separation between the medullary canal and the area of compact cortical bone, the inner contours of the 17 sections must be defined. The geometry of these contours is variable in both shape and dimensions. In order to be able to make the model, several evaluations with QCT images and work from the specialized literature were studied [
30,
31,
32,
33], resulting in the following aspects:
in the areas from the ends of the diaphysis (approximately 1/4–1/3 of its length) the inner contours are equidistant with the outer ones and the offset between them (cortical bone thickness) increases from the extremities to the middle;
in the middle area of the diaphysis, the equidistance is easily lost, the inner contours tend towards an elliptical shape, and the thickness of the cortical bone (in the same section) is not constant but increases in the anterior and posterior–lateral area of the tibia.
the thickness of the cortical bone increases by more than 100% from the ends (where it connects with the cortical bone of the epiphyses) to the middle of the diaphysis.
A simplification of the modeling that has been adopted is that the two contours (interior and exterior) were considered equidistant in all 17 sections described above. Basically, the tendency to ovalize the inner contours in the sections from the middle of the tibia was neglected. However, in order to compensate for this, the dimensional increases of the cortical bone in the middle area of the diaphysis on the anterior and posterior–lateral direction were taken into account. This started at the ends with a thickness of 2.5 mm, which connect with the cortical bone of the epiphyses, with a continuous growth from the extremities to the middle of the diaphysis, resulting in the 3D model in
Figure 3.
Figure 4 shows a section through 3D models of the cortical area of the epiphyses and diaphysis.
Taking into account the real structure of the tibia, it should be noted that the trabecular bone area at the level of the epiphyses does not end abruptly, as shown in the models presented above, but decreases slowly towards the diaphysis, there is in this sense an area of interference between the epiphyses and diaphyses called the metaphysis. At the level of the metaphysis, the trabecular bone mass not only decreases quantitatively but there is also a decrease in its density.
Consequently, for the accuracy of the model, we considered it important to complete the modeled assembly with 2 more entities corresponding to the metaphyses (the red ones in
Figure 5). These were modeled using the inner geometries placed towards the ends of the shaft, where the inner surfaces of the shaft became outer surfaces for the metaphyses. For the modeling of the inner surfaces of the metaphyses, two inner surfaces of revolution were generated in the form of ellipsoid parts to represent the passage from the medullary canal to the first trabecular formations.
Thus, the 5 entities modeled in CAD are: proximal epiphysis—cortical bone, proximal epiphysis—trabecular bone, proximal metaphysis, diaphysis, distal metaphysis, distal epiphysis—trabecular bone, distal epiphysis—cortical bone.
The final 3D model of the tibia that takes into account the actual bone structure is the result of assembling the entities presented above (
Figure 5).
2.1.2. Virtual Simulation of the OWHTO
The modeling of the OWHTO was conducted taking into account the steps that are taken in the case of real surgery, with the highlighting (
Figure 6a,b) of the geometric parameters that characterize the geometrical planning of this operation. Thus, the Center Of Rotation of Angulation Axis (CORA hereinafter), which is the hinge around which the creation of open wedge osteotomy takes place, is characterized by two parameters, V2, which represents the distance from the lateral tibial plateau to CORA, and V3, which represents the distance from the lateral cortex of the tibia to CORA (
Figure 6a). Medial cortex (
Figure 6b) is a curve located on the medial surface of the tibia, in a plane that intersects half of the tibial plateaus in the frontal plane, and cutting point (
Figure 6a) is a point located on the medial cortex from which the initiation of the cut of the osteotomy plane takes place. The distance from this point to the tibial plateau V1 is also one of the parameters that characterize geometric planning. Finally, the fourth parameter V4 is the correction angle of the osteotomy wedge. CAD modeling of OWHTO surgery was performed parameterized so that it can be obtained from the generalized model how many customized models we want in order to optimize the geometric planning of the operation and obtain the best combination of parameters that ensure the correction angle in the best conditions.
In order to complete the modeling of the OWHTO operation, CAD models were made for the 440.834S TomoFix osteosynthesis plate (standard) and the necessary fixing screws (
Figure 7b), elements that preserve the obtained axial correction. The tibial model with the osteotomy pen created, the TomoFix plate and the screws were assembled according to the instruction on the surgical technique of the TomoFix Medial High Tibial Plate (DePuy Synthes; Synthes GmbH, Oberdorf, Switzerland) [
33] resulting in the 3D assembly from
Figure 7a. The CAD models made and presented will be used as geometric models in the CAE simulations in the
Section 2.2.


 ,
, 



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}