
Earth Mover’s Distance-Based Tool for Rapid Screening of Cervical Cancer Using Cervigrams

 , ,
, , 
Abstract
:1. Introduction
Our Contributions
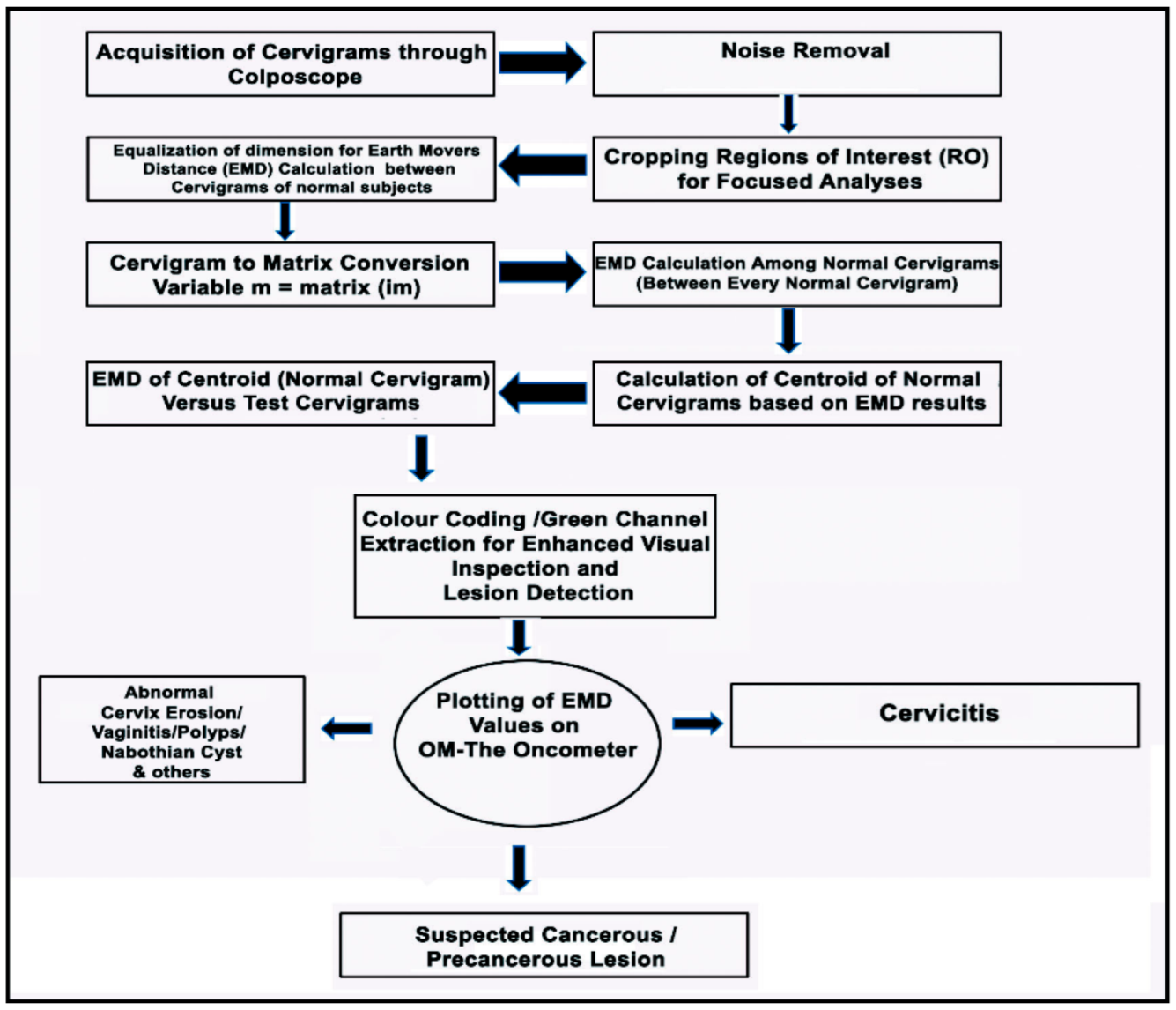
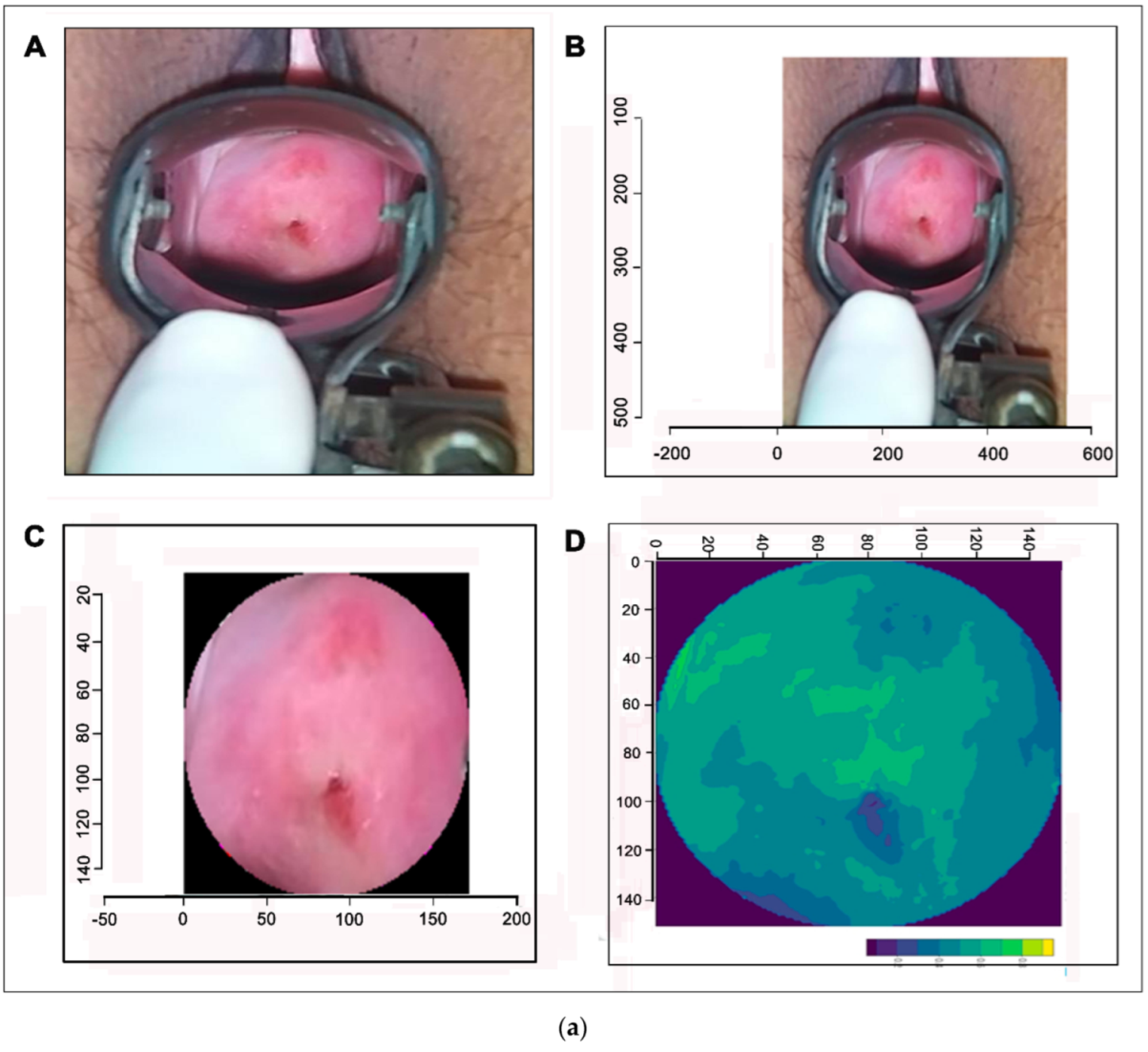
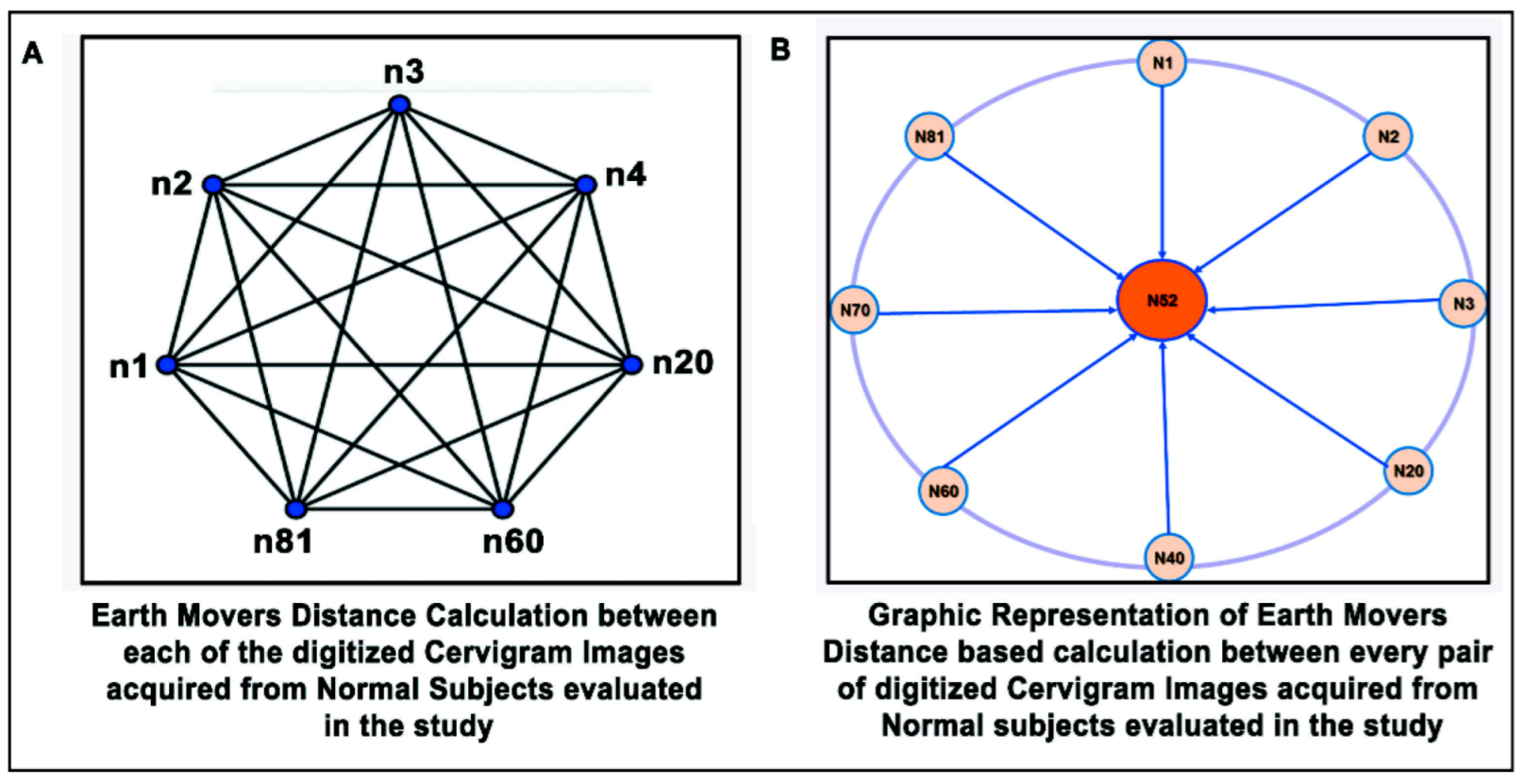
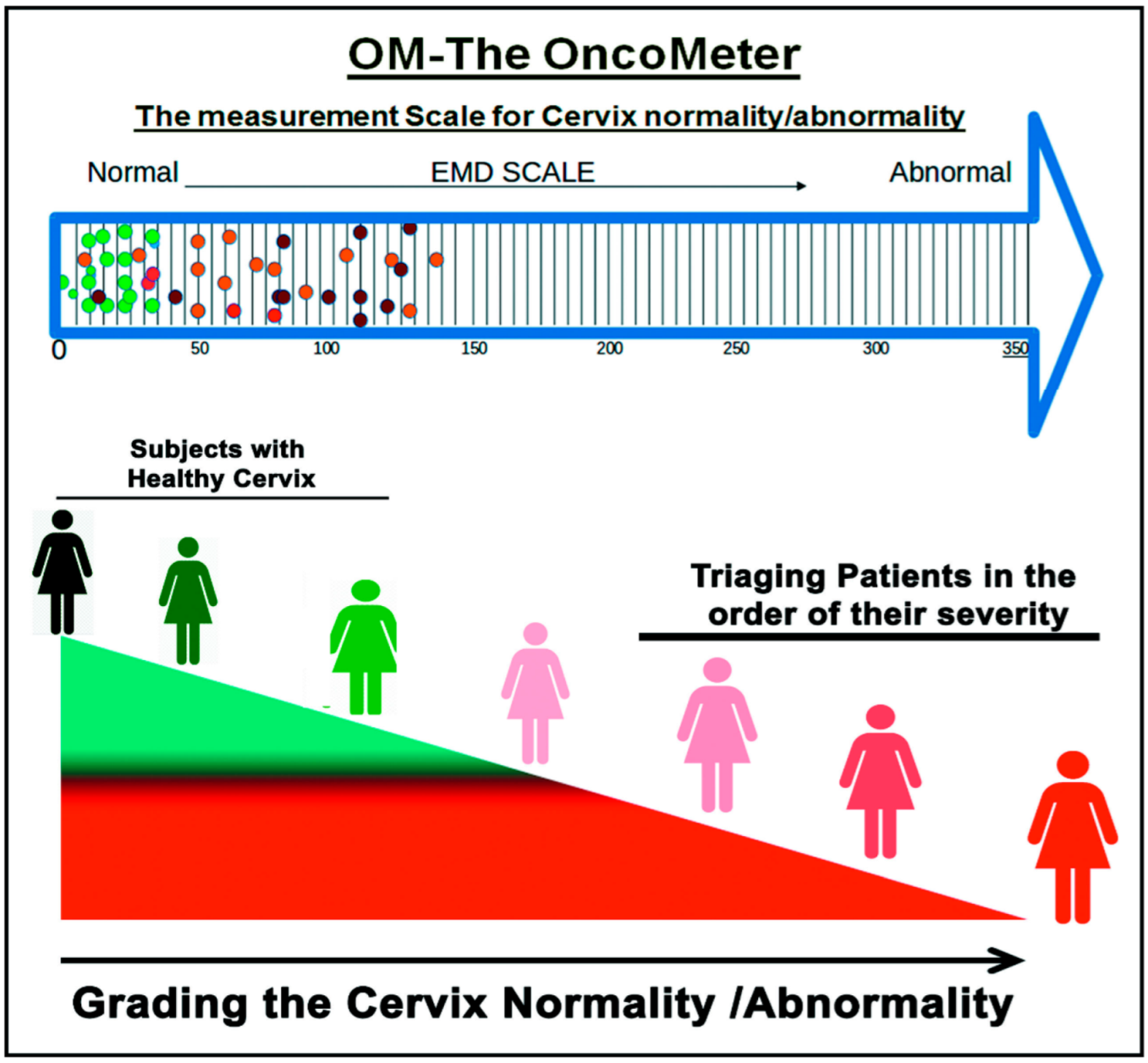
2. Materials and Methods
- The first and foremost key feature of the algorithm, being free;
- Image similarity-based detection;
- Open source implementation in R;
- Robust application to noisy images;
- Cloud-based storage accessibility and ubiquitous provisioning of services from a collected repository at the local, regional, and global levels;
- This cloud-based information provisioning facilitates automated closed-loop-resource allocation, which in turn provides affordable and accessible healthcare technology platforms for effective management of disease burden.
3. Results
Sensitivity and Specificity
4. Discussion
- The computational part of the proposed algorithm heavily relies on cervigrams acquired by a colposcope; hence, its ability to correctly tag cervical conditions is limited by the truthfulness and resolution of the cervigrams.
- This tool was built on the basis of training data, which were used for concept development and its validated implementation. Large numbers of heterogeneous cervigrams from all across the country are required for refining the tool and then should be deployed in the community with proper settings for other lifestyle and genetic parameters.
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rao, J.; Escobar-Hoyos, L.; Shroyer, K.R. Unmet clinical needs in cervical cancer screening. MLO Med. Lab. Obs. 2016, 48, 8–10. Available online: https://www.mlo-online.com/ (accessed on 22 March 2022). [PubMed]
- World Health Organization. Who Cervical Cancer. Early Diagnosis and Screening. Available online: www.who.int/cancer/prevention/diagnosis-screening/cervical-cancer/en/ (accessed on 22 March 2022).
- The Global Cancer Observatory. India Factsheet, WHO. Available online: https://gco.iarc.fr/today/data/factsheets/populations/356-india-fact-sheets.pdf (accessed on 22 March 2022).
- Shrivastav, K.D.; Das, A.M.; Singh, H.; Ranjan, P.; Janardhanan, R. Classification of colposcopic cervigrams using EMD in R. In Proceedings of the International Symposium on Signal Processing and Intelligent Recognition Systems, Bangalore, India, 9–22 September 2018; pp. 298–308. [Google Scholar] [CrossRef]
- ICO/IARC. ICO/IARC Information Centre on HPV and Cancer, India Human Papillomavirus and Related Cancers, Fact Sheet. 2018. Available online: https://hpvcentre.net/statistics/reports/IND_FS.pdf (accessed on 22 March 2022).
- Kumar, P.; Gupta, S.; Das, A.M.; Das, B.C. Towards global elimination of cervical cancer in all groups of women. Lancet Oncol. 2019, 20, e237. [Google Scholar] [CrossRef] [Green Version]
- Shrivastav, K.D.; Taneja, N.; Das, A.M.; Rana, S.; Ranjan, P.; Singh, H.; Jaggi, V.K.; Janardhanan, R. Socio-demographic and Clinico-pathological Profile of Cervical Cancer Patients at a Tertiary Care Centre in New Delhi: A Five-Year Retrospective analysis. Indian J. Community Health 2021, 33, 634–639. [Google Scholar] [CrossRef]
- Tian, R.; Cui, Z.; He, D.; Tian, X.; Gao, Q.; Ma, X.; Yang, J.; Wu, J.; Das, B.C.; Severinov, K.; et al. Risk stratification of cervical lesions using capture sequencing and machine learning method based on HPV and human integrated genomic profiles. Carcinogenesis 2019, 40, 1220–1228. [Google Scholar] [CrossRef]
- Park, S.Y.; Follen, M.; Milbourne, A.; Rhodes, H.; Malpica, A.; MacKinnon, N.B.; MacAulay, C.; Markey, M.K.; Richards-Kortum, R.R. Automated image analysis of digital colposcopy for the detection of cervical neoplasia. J. Biomed. Opt. 2008, 13, 014029. [Google Scholar] [CrossRef]
- Lange, H.; Wolters, R.H. Uterine cervical cancer computer-aided-diagnosis (CAD). J. Biomed. Opt. 2010, 1–10. Available online: https://patents.google.com/patent/US7664300B2/en (accessed on 22 March 2022).
- de Castro Hillmann, E.; Bacha, O.M.; Roy, M.; Paris, G.; Berbiche, D.; Nizard, V.; Ramos, J.G. Cervical digital photography: An alternative method to colposcopy. J. Obstet. Gynaecol. Can. 2019, 41, 1099–1107. [Google Scholar] [CrossRef]
- Agarwal, A.; Ali, F.; Kopparthi, A.; Ranjan, P.; Shrivastav, K.D.; Janardhanan, R. Specular reflection removal in cervigrams. In Contemporary Issues in Communication, Cloud and Big Data Analytics; Springer: Singapore, 2022; pp. 423–437. [Google Scholar]
- Rubner, Y.; Tomasi, C.; Guibas, L.J. The earth mover’s distance as a metric for image retrieval. Int. J. Comput. Vis. 2000, 40, 99–121. [Google Scholar] [CrossRef]
- Boltz, S.; Nielsen, F.; Soatto, S. Earth mover distance on superpixels. In Proceedings of the 2010 IEEE International Conference on Image Processing, Hong Kong, China, 26–29 September 2010; pp. 4597–4600. Available online: https://ieeexplore.ieee.org/abstract/document/5651708/metrics#metrics (accessed on 22 March 2022).
- Sun, Y.; Lei, M. Method for optical coherence tomography image classification using local features and earth mover’s distance. J. Biomed. Opt. 2009, 14, 054037. [Google Scholar] [CrossRef] [Green Version]
- Coughlin, S.S.; Trock, B.; Criqui, M.H.; Pickle, L.W.; Browner, D.; Tefft, M.C. The logistic modeling of sensitivity, specificity, and predictive value of a diagnostic test. J. Clin. Epidemiol. 1992, 45, 1–7. [Google Scholar] [CrossRef]
- Lalkhen, A.G.; McCluskey, A. Clinical tests: Sensitivity and specificity. Contin. Educ. Anaesth. Crit. Care Pain 2008, 8, 221–223. [Google Scholar] [CrossRef] [Green Version]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; De Vet, H.C.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. Clin. Chem. 2015, 61, 1446–1452. [Google Scholar] [CrossRef] [Green Version]
- Forhan, S.E.; Godfrey, C.C.; Watts, D.H.; Langley, C.L. A systematic review of the effects of visual inspection with acetic acid, cryotherapy, and loop electrosurgical excision procedures for cervical dysplasia in HIV-infected women in low-and middle-income countries. JAIDS J. Acquir. Immune Defic. Syndr. 2015, 68, S350–S356. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. The Challenge Ahead: Progress in Breast and Cervical Cancer. Institute of Health Metrics and Evaluation, IHME. Available online: https://www.healthdata.org/policy-report/challenge-ahead-progress-and-setbacks-breast-and-cervical-cancer. (accessed on 22 March 2022).
- Huh, W.K.; Papagiannakis, E.; Gold, M.A. Observed colposcopy practice in US community-based clinics: The retrospective control arm of the IMPROVE-COLPO study. J. Low. Genit. Tract Dis. 2019, 23, 110. [Google Scholar] [CrossRef]
- Hu, L.; Bell, D.; Antani, S.; Xue, Z.; Yu, K.; Horning, M.P.; Gachuhi, N.; Wilson, B.; Jaiswal, M.S.; Befano, B.; et al. An observational study of deep learning and automated evaluation of cervical images for cancer screening. JNCI J. Natl. Cancer Inst. 2019, 111, 923–932. [Google Scholar] [CrossRef]
- Taneja, A.; Ranjan, P.; Ujlayan, A. Multi-cell nuclei segmentation in cervical cancer images by integrated feature vectors. Multimed. Tools Appl. 2018, 77, 9271–9290. [Google Scholar] [CrossRef]
- Menezes, L.J.; Vazquez, L.; Mohan, C.K.; Somboonwit, C. Eliminating cervical cancer: A role for artificial intelligence. In Global Virology III: Virology in the 21st Century; Springer: Cham, Switzerland, 2019; pp. 405–422. [Google Scholar]
- CDC. Cervical Cancer Screening Guidelines for Average-Risk Women, CDC. Available online: https://www.cdc.gov/cancer/cervical/pdf/guidelines.pdf (accessed on 22 March 2022).
- Xue, Z.; Antani, S.; Long, L.R.; Jeronimo, J.; Thoma, G.R. Comparative performance analysis of cervix ROI extraction and specular reflection removal algorithms for uterine cervix image analysis. In Medical Imaging 2007: Image Processing; International Society for Optics and Photonics: Bellingham, WA, USA, 2007; Volume 6512, p. 65124I. [Google Scholar]
- Al-shamasneh, A.R.; Obaidellah, U.H. Artificial intelligence techniques for cancer detection and classification: Review study. Eur. Sci. J. 2017, 13, 342–370. [Google Scholar]
- Dvir, H.; Gordon, S.; Greenspan, H. Illumination correction for content analysis in uterine cervix images. In Proceedings of the 2006 Conference on Computer Vision and Pattern Recognition Workshop (CVPRW’06), New York, NY, USA, 17–22 June 2006; IEEE: Piscataway, NJ, USA, 2006; p. 95. [Google Scholar]
- Kim, E.; Huang, X. A data driven approach to cervigram image analysis and classification. In Color Medical Image Analysis; Springer: Dordrecht, The Netherlands, 2013; pp. 1–13. [Google Scholar]
- Huang, X.; Wang, W.; Xue, Z.; Antani, S.; Long, L.R.; Jeronimo, J. Tissue classification using cluster features for lesion detection in digital cervigrams. In Medical Imaging 2008: Image Processing; International Society for Optics and Photonics: Bellingham, WA, USA, 2008; Volume 6914, p. 69141Z. [Google Scholar]
- Muschelli, J.; Gherman, A.; Fortin, J.P.; Avants, B.; Whitcher, B.; Clayden, J.D.; Caffo, B.S.; Crainiceanu, C.M. Neuroconductor: An R platform for medical imaging analysis. Biostatistics 2019, 20, 218–239. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Zhang, H.; Xin, C.; Kim, E.; Long, L.R.; Xue, Z.; Antani, S.; Huang, X. Multi-feature based benchmark for cervical dysplasia classification evaluation. Pattern Recognit. 2017, 63, 468–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Cases (n = 296) | Control (n = 102) | p Value | |||
|---|---|---|---|---|---|---|
| Abnormal Cervix (Cervicitis, Vaginitis, Nabothian Cyst, Cervical Erosion) | Suspected Cancer, Precancerous | Ca Cx (Squamous Cell Carcinoma, Ca cx I, Ca cx II, Ca Cx III, Ca Cx IV) | Women with Normal Cervix | |||
| Age | <20 | 1 (0.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.000 |
| 21–40 | 145 (36.4%) | 8 (2.0%) | 8 (2.0%) | 58 (14.6%) | ||
| 41–60 | 76 (19.1%) | 15 (3.8%) | 23 (5.8%) | 36 (9.0%) | ||
| >60 | 2 (0.5%) | 5 (1.3%) | 13 (3.3%) | 8 (2.0%) | ||
| Education | Illiterate | 26 (6.5%) | 11 (2.8%) | 23 (5.8%) | 14 (3.5%) | 0.000 |
| Literate Primary/high school/senior secondary | 141 (35.4%) | 12 (3.0%) | 18 (4.5%) | 59 (14.8%) | ||
| graduation and above | 57 (14.3%) | 5 (1.3%) | 3 (0.8%) | 29 (7.3%) | ||
| Occupation | Housewife | 200 (50.3%) | 25 (6.3%) | 38 (9.5%) | 89 (22.4%) | 0.001 |
| Government job | 3 (0.8%) | 1 (0.3%) | 0 (0.0%) | 4 (1.0%) | ||
| Private job | 20 (5.0%) | 0 (0.0%) | 2 (0.5%) | 9 (2.3%) | ||
| Other | 1 (0.3%) | 2 (0.5%) | 4 (1.0%) | 0 (0.0%) | ||
| Socio-economic Status | Low income (below 1 lakh) | 52 (13.1%) | 9 (2.3%) | 28 (7.0%) | 25 (6.3%) | 0.000 |
| Middle income (1–10 lakhs) | 169 (42.5%) | 18 (4.5%) | 15 (3.8%) | 76 (19.1%) | ||
| High income (above 10 lakhs) | 0 (0.0%) | 1 (0.3%) | 1 (0.3%) | 1 (0.3%) | ||
| Do not know | 3 (0.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| Menstrual health | Normal | 11 (2.8%) | 3 (0.8%) | 2 (0.5%) | 38 (9.5%) | 0.000 |
| Abnormal (white discharge, heavy bleeding, irregular menstruation, heavy pain, itching, foul smelling) | 192 (48.2%) | 22 (6.1%) | 40 (10.1%) | 51 (12.8%) | ||
| Post-menopausal | 21 (5.3%) | 3 (0.8%) | 2 (0.5%) | 13 (3.3%) | ||
| Total | 398 | |||||
| Tagging of Cervigrams | No. of Cervigrams | Accurate Classification of Cervigrams by OM | EMD Range on OM—The OncoMeter |
|---|---|---|---|
| Normal | 102 | 68 | 0–26.77 |
| Abnormal (Nabothian cyst, vaginitis, cervical erosion, polyp) | 167 | 133 | 8.162584–146.8711 |
| Cervicitis | 57 | 53 | 19.41418–140.2637 |
| Precancerous | 3 | 3 | 34.65366–36.1091 |
| Suspected Cancer | 25 | 21 | 67.77164–78.53794 |
| Squamous Cell Ca cx | 25 | 24 | 21.01863–92.59932 |
| Ca cx I | 5 | 3 | 21.58473–68.71633 |
| Ca cx II | 9 | 9 | 27.55506–103.9834 |
| Ca cx III | 3 | 3 | 51.99892–106.1609 |
| Ca cx IV | 2 | 2 | 42.90317–75.26646 |
| Total | 398 | 319 |
| Cases (Abnormal Cervigrams)—296 | Controls (Normal Cervigrams)—102 | ||
|---|---|---|---|
| True Positive | 251 | True Negative | 68 |
| False Negative | 45 | False Positive | 34 |
| Sensitivity (251/296) | 84.79% | Specificity (68/102) | 66.66% |
| Accuracy (319/398) | 80.15% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrivastav, K.D.; Arambam, P.; Batra, S.; Bhatia, V.; Singh, H.; Jaggi, V.K.; Ranjan, P.; Abed, E.H.; Janardhanan, R. Earth Mover’s Distance-Based Tool for Rapid Screening of Cervical Cancer Using Cervigrams. Appl. Sci. 2022, 12, 4661. https://doi.org/10.3390/app12094661
Shrivastav KD, Arambam P, Batra S, Bhatia V, Singh H, Jaggi VK, Ranjan P, Abed EH, Janardhanan R. Earth Mover’s Distance-Based Tool for Rapid Screening of Cervical Cancer Using Cervigrams. Applied Sciences. 2022; 12(9):4661. https://doi.org/10.3390/app12094661
Chicago/Turabian StyleShrivastav, Kumar Dron, Priyadarshini Arambam, Shelly Batra, Vandana Bhatia, Harpreet Singh, Vinita Kumar Jaggi, Priya Ranjan, Eyad H. Abed, and Rajiv Janardhanan. 2022. "Earth Mover’s Distance-Based Tool for Rapid Screening of Cervical Cancer Using Cervigrams" Applied Sciences 12, no. 9: 4661. https://doi.org/10.3390/app12094661
APA StyleShrivastav, K. D., Arambam, P., Batra, S., Bhatia, V., Singh, H., Jaggi, V. K., Ranjan, P., Abed, E. H., & Janardhanan, R. (2022). Earth Mover’s Distance-Based Tool for Rapid Screening of Cervical Cancer Using Cervigrams. Applied Sciences, 12(9), 4661. https://doi.org/10.3390/app12094661