

Effect of Carotid Stenosis Severity on Patterns of Brain Activity in Patients after Cardiac Surgery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
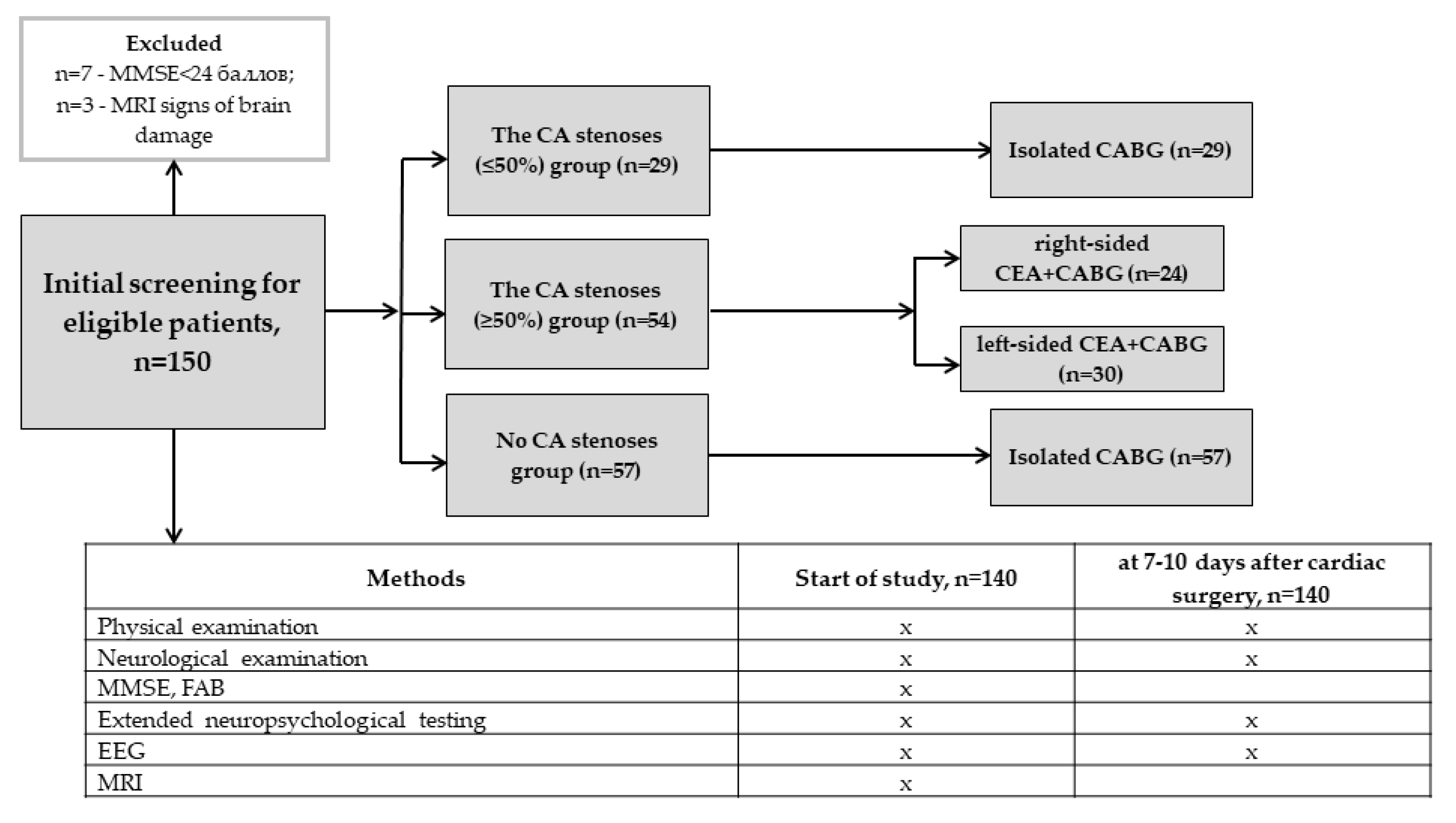
2.1. Subjects
2.2. Neurophysiological Assessment
2.3. Statistical Analysis
3. Results
3.1. The Effect of Small Stenoses CA (≤50%) on the Postoperative Neurophysiological Changes in On-Pump CABG Patients
3.1.1. Neurophysiological Data
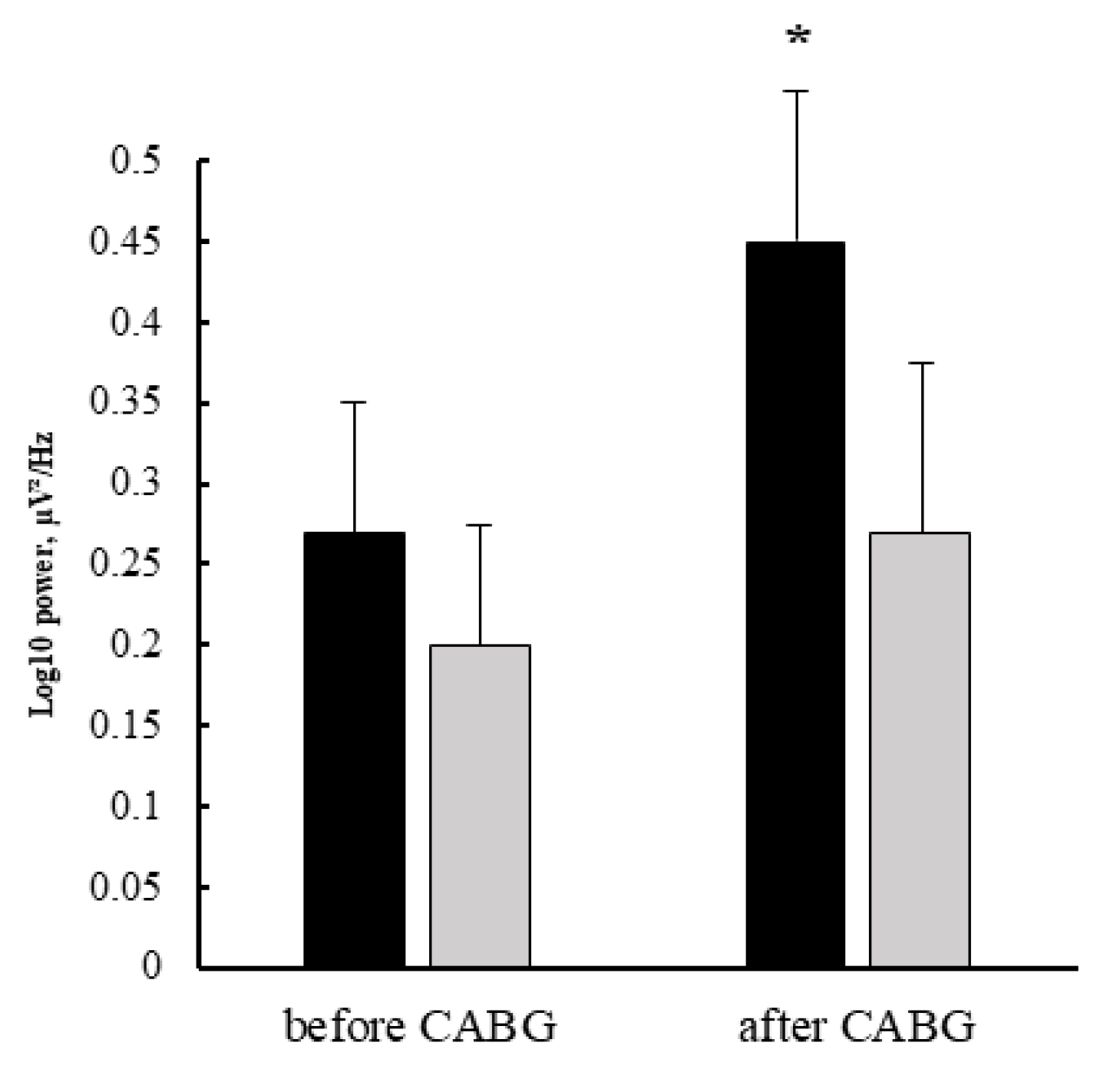
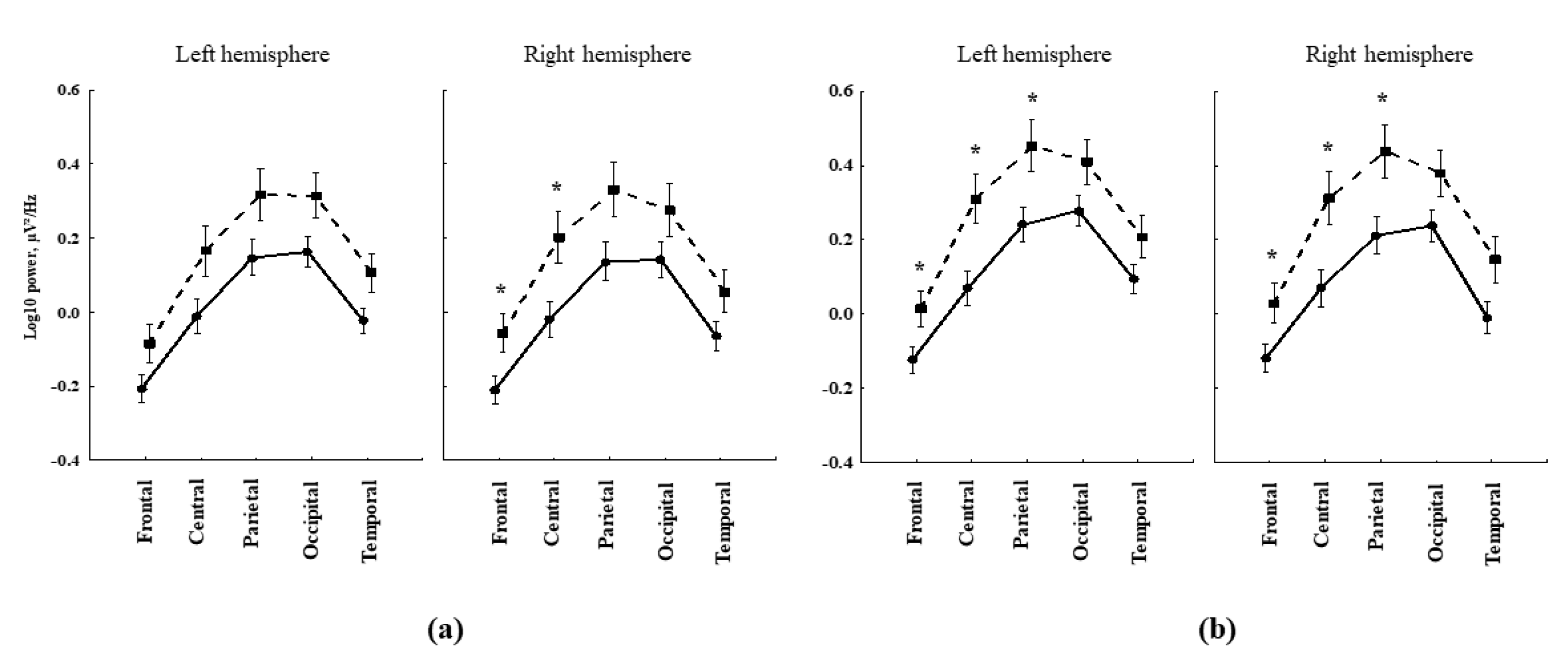
3.1.2. EEG Data
3.2. The Postoperative Neurophysiological Status Changes in the Patients after Combined On-Pump CABG and CEA
3.2.1. Neurophysiological Data
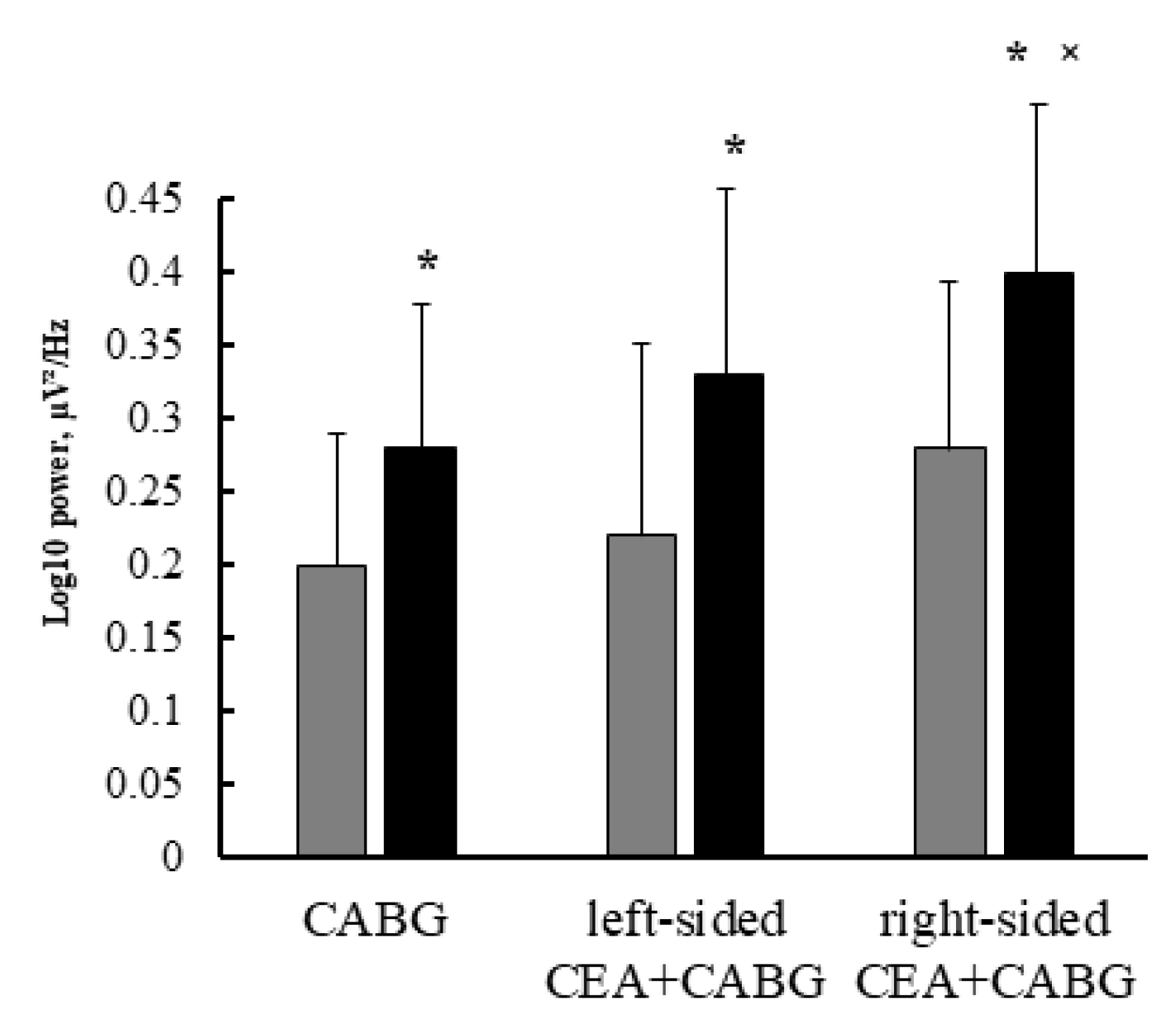
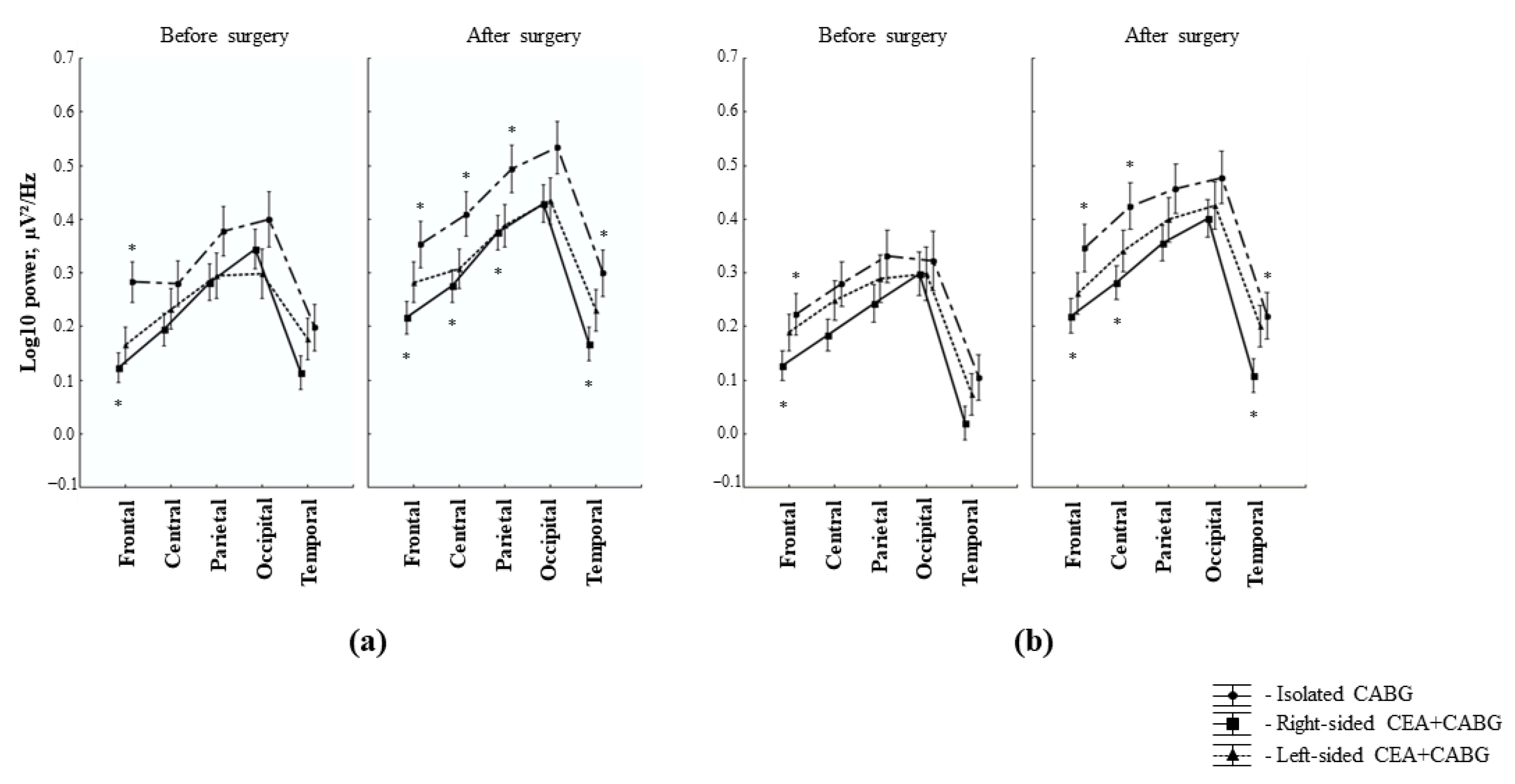
3.2.2. EEG Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Efimova, E.V.; Konobeevskaya, I.N.; Maksimenko, G.V.; Karpov, R.S. smoking and cardiovascular mortality in tomsk inhabitants as a typical city of western siberia. Cardiovasc. Ther. Prev. 2017, 16, 115–121. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Lopez, J.; Silva-Pereyra, J.; Fernández, T.; Alatorre-Cruz, G.C.; Castro-Chavira, S.A.; González-López, M.; Sánchez-Moguel, S.M. High levels of incidental physical activity are positively associated with cognition and EEG activity in aging. PLoS ONE 2018, 13, e0191561. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, M.; Okonkwo, O.C.; Resnick, S.M.; Jagust, W.J.; Benzinger, T.L.; Rapp, P.R. What are the threats to successful brain and cognitive aging? Neurobiol. Aging 2019, 83, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Alosco, M.L.; Spitznagel, M.B.; Sweet, L.H.; Josephson, R.; Hughes, J.; Gunstad, J. Atrial Fibrillation Exacerbates Cognitive Dysfunction and Cerebral Perfusion in Heart Failure. Pacing Clin. Electrophysiol. 2014, 38, 178–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorelick, P.B.; Counts, S.E.; Nyenhuis, D. Vascular cognitive impairment and dementia. Biochim. et Biophys. Acta (BBA)-Mol. Basis Dis. 2015, 1862, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Tarasova, I.V.; Trubnikova, O.A.; Barbarash, O.L. EEG and Clinical Factors Associated with Mild Cognitive Impairment in Coronary Artery Disease Patients. Dement. Geriatr. Cogn. Disord. 2018, 46, 275–284. [Google Scholar] [CrossRef]
- Hsu, C.L.; Best, J.R.; Davis, J.C.; Nagamatsu, L.S.; Wang, S.; Boyd, L.A.; Hsiung, G.R.; Voss, M.W.; Eng, J.J.; Liu-Ambrose, T. Aerobic exercise promotes executive functions and impacts functional neural activity among older adults with vascular cognitive impairment. Br. J. Sports Med. 2017, 52, 184–191. [Google Scholar] [CrossRef]
- Rosenberg, G.A. Binswanger’s disease: Biomarkers in the inflammatory form of vascular cognitive impairment and dementia. J. Neurochem. 2018, 144, 634–643. [Google Scholar] [CrossRef]
- de la Torre, J. The Vascular Hypothesis of Alzheimer’s Disease: A Key to Preclinical Prediction of Dementia Using Neuroimaging. J. Alzheimer’s Dis. 2018, 63, 35–52. [Google Scholar] [CrossRef] [PubMed]
- Fulop, G.A.; Tarantini, S.; Yabluchanskiy, A.; Molnar, A.; Prodan, C.I.; Kiss, T.; Csipo, T.; Lipecz, A.; Balasubramanian, P.; Farkas, E.; et al. Role of age-related alterations of the cerebral venous circulation in the pathogenesis of vascular cognitive impairment. Am. J. Physiol. Circ. Physiol. 2019, 316, H1124–H1140. [Google Scholar] [CrossRef]
- Anazodo, U.C.; Shoemaker, K.; Suskin, N.; Essali, T.; Wang, D.; Lawrence, K.S.S. Impaired Cerebrovascular Function in Coronary Artery Disease Patients and Recovery Following Cardiac Rehabilitation. Front. Aging Neurosci. 2016, 7, 224. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Cao, W.; Ding, W.; Wang, Y.; Han, X.; Zhou, Y.; Xu, Q.; Zhang, Y.; Xu, J. Cerebral Blood Flow Alterations as Assessed by 3D ASL in Cognitive Impairment in Patients with Subcortical Vascular Cognitive Impairment: A Marker for Disease Severity. Front. Aging Neurosci. 2016, 8, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bangen, K.J.; Werhane, M.L.; Weigand, A.J.; Edmonds, E.C.; Delano-Wood, L.; Thomas, K.; Nation, D.A.; Evangelista, N.D.; Clark, A.L.; Liu, T.T.; et al. Reduced Regional Cerebral Blood Flow Relates to Poorer Cognition in Older Adults With Type 2 Diabetes. Front. Aging Neurosci. 2018, 10, 270. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Matsumoto, Y.; Ota, H.; Sugimura, K.; Takahashi, J.; Ito, K.; Miyata, S.; Furukawa, K.; Arai, H.; Fukumoto, Y.; et al. Hippocampal Blood Flow Abnormality Associated With Depressive Symptoms and Cognitive Impairment in Patients With Chronic Heart Failure. Circ. J. 2016, 80, 1773–1780. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Li, M.; Zhang, X.; Yang, S.; Fan, H.; Qin, W.; Yang, L.; Yuan, J.; Hu, W. Clinical features and the degree of cerebrovascular stenosis in different types and subtypes of cerebral watershed infarction. BMC Neurol. 2017, 17, 166. [Google Scholar] [CrossRef] [Green Version]
- Wåhlin, A.; Nyberg, L. At the Heart of Cognitive Functioning in Aging. Trends Cogn. Sci. 2019, 23, 717–720. [Google Scholar] [CrossRef]
- Bunch, T.J.; Galenko, O.; Graves, K.G.; Jacobs, V.; May, H.T. Atrial Fibrillation and Dementia: Exploring the Association, Defining Risks and Improving Outcomes. Arrhythmia Electrophysiol. Rev. 2019, 8, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Tschernatsch, M.; Juenemann, M.; Alhaidar, F.; El Shazly, J.; Butz, M.; Meyer, M.; Gerriets, T.; Schönburg, M.; Schramm, P. Epileptic seizure discharges in patients after open chamber cardiac surgery—A prospective prevalence pilot study using continuous electroencephalography. Intensiv. Care Med. 2020, 46, 1418–1424. [Google Scholar] [CrossRef]
- Tarasova, I.; Razumnikova, O.; Trubnikova, O.; Mezentsev, Y.; Kupriyanova, D.; Barbarash, O. Neurophysiological correlates of postoperative cognitive disorders. Zhurnal Nevrol. i psikhiatrii im. S.S. Korsakova 2021, 121, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Başar, E.; Gölbaşı, B.T.; Tülay, E.; Aydın, S.; Başar-Eroğlu, C. Best method for analysis of brain oscillations in healthy subjects and neuropsychiatric diseases. Int. J. Psychophysiol. 2016, 103, 22–42. [Google Scholar] [CrossRef] [Green Version]
- Babiloni, C.; Barry, R.J.; Başar, E.; Blinowska, K.J.; Cichocki, A.; Drinkenburg, W.H.; Klimesch, W.; Knight, R.T.; da Silva, F.L.; Nunez, P.; et al. International Federation of Clinical Neurophysiology (IFCN)—EEG research workgroup: Recommendations on frequency and topographic analysis of resting state EEG rhythms. Part 1: Applications in clinical research studies. Clin. Neurophysiol. 2020, 131, 285–307. [Google Scholar] [CrossRef] [PubMed]
- Schleiger, E.; Wong, A.; Read, S.; Rowland, T.; Finnigan, S. Poststroke QEEG informs early prognostication of cognitive impairment. Psychophysiology 2017, 54, 301–309. [Google Scholar] [CrossRef]
- Al-Qazzaz, N.K.; Ali, S.H.B.M.; Ahmad, S.A.; Islam, M.S.; Escudero, J. Discrimination of stroke-related mild cognitive impairment and vascular dementia using EEG signal analysis. Med. Biol. Eng. Comput. 2017, 56, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Moretti, D.V. Electroencephalography-driven approach to prodromal Alzheimer’s disease diagnosis: From biomarker integration to network-level comprehension. Clin. Interv. Aging 2016, 11, 897–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moretti, D.V. Increase of EEG Alpha3/Alpha2 Power Ratio Detects Inferior Parietal Lobule Atrophy in Mild Cognitive Impairment. Curr. Alzheimer Res. 2018, 15, 443–451. [Google Scholar] [CrossRef]
- Moretti, D.V. Theta and alpha EEG frequency interplay in subjects with mild cognitive impairment: Evidence from EEG, MRI, and SPECT brain modifications. Front. Aging Neurosci. 2015, 7, 31. [Google Scholar] [CrossRef]
- Zappasodi, F.; Pasqualetti, P.; Rossini, P.M.; Tecchio, F. Acute Phase Neuronal Activity for the Prognosis of Stroke Recovery. Neural Plast. 2019, 2019, 1971875. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Belmonte, L.M.; Román-Terán, C.M.S.; Jiménez-Navarro, M.; Barbancho, M.A.; García-Alberca, J.M.; Lara, J.P. Assessment of Long-Term Cognitive Impairment After Off-Pump Coronary-Artery Bypass Grafting and Related Risk Factors. J. Am. Med. Dir. Assoc. 2015, 16, 263.e9–263.e11. [Google Scholar] [CrossRef]
- Bhamidipati, D.; Goldhammer, J.E.; Sperling, M.R.; Torjman, M.C.; McCarey, M.M.; Whellan, D.J. Cognitive Outcomes After Coronary Artery Bypass Grafting. J. Cardiothorac. Vasc. Anesthesia 2017, 31, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Hood, R.; Budd, A.; Sorond, F.A.; Hogue, C.W. Peri-operative neurological complications. Anaesthesia 2018, 73, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trubnikova, O.A.; Tarasova, I.V.; Mamontova, A.S.; Syrova, I.D.; Maleva, O.V.; Barbarash, O.L. A role of carotid stenoses in the structure of early postoperative cognitive dysfunction in patients underwent coronary artery bypass grafting. Zhurnal Nevrol. i psikhiatrii im. S.S. Korsakova 2014, 114, 36–42. [Google Scholar] [PubMed]
- Skhirtladze-Dworschak, K.; Felli, A.; Aull-Watschinger, S.; Jung, R.; Mouhieddine, M.; Zuckermann, A.; Tschernko, E.; Dworschak, M.; Pataraia, E. The Impact of Nonconvulsive Status Epilepticus after Cardiac Surgery on Outcome. J. Clin. Med. 2022, 11, 5668. [Google Scholar] [CrossRef]
- Kara, I.; Erkin, A.; Saclı, H.; Demirtas, M.; Percin, B.; Diler, M.S.; Kırali, K. The Effects of Near-Infrared Spectroscopy on the Neurocognitive Functions in the Patients Undergoing Coronary Artery Bypass Grafting with Asymptomatic Carotid Artery Disease: A Randomized Prospective Study. Ann. Thorac. Cardiovasc. Surg. 2015, 21, 544–550. [Google Scholar] [CrossRef] [Green Version]
- Hori, D.; Ono, M.; Adachi, H.; Hogue, C.W. Effect of carotid revascularization on cerebral autoregulation in combined cardiac surgery. Eur. J. Cardio-Thoracic Surg. 2015, 49, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Irqsusi, M.; Vannucchi, A.; Beckers, J.; Kasseckert, S.; Waldhans, S.; Moosdorf, R.G.H.; Vogt, S. Early Results of Surgical Simultaneous Therapy for Significant Carotid Artery Stenosis and Heart Disease. Thorac. Cardiovasc. Surg. 2017, 66, 261–265. [Google Scholar] [CrossRef]
- Trubnikova, O.A.; Tarasova, I.V.; Moskin, E.G.; Kupriyanova, D.S.; Argunova, Y.A.; Pomeshkina, S.A.; Gruzdeva, O.V.; Barbarash, O.L. Beneficial Effects of a Short Course of Physical Prehabilitation on Neurophysiological Functioning and Neurovascular Biomarkers in Patients Undergoing Coronary Artery Bypass Grafting. Front. Aging Neurosci. 2021, 13, 699259. [Google Scholar] [CrossRef]
- Volf, N.; Tarasova, I. The influence of reward on the performance of verbal creative tasks: Behavioral and EEG effects. Hum. Physiol. 2013, 39, 302–308. [Google Scholar] [CrossRef]
- Tam, N.D. Improvement of Processing Speed in Executive Function Immediately following an Increase in Cardiovascular Activity. Cardiovasc. Psychiatry Neurol. 2013, 2013, 212767. [Google Scholar] [CrossRef]
- Snyder, S.M.; Hall, J.R.; Cornwell, S.L.; Falk, J.D. Addition of EEG improves accuracy of a logistic model that uses neuropsychological and cardiovascular factors to identify dementia and MCI. Psychiatry Res. 2011, 186, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Musha, T.; Kosugi, Y.; Kubo, M.; Horie, Y.; Kuwayama, N.; Kuroda, S.; Hayashi, K.; Kobayashi, Y.; Tanaka, M.; et al. Altered Neuronal Activity Topography Markers in the Elderly with Increased Atherosclerosis. Front. Aging Neurosci. 2017, 9, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, R.; Huang, X.; Qin, Y.; Li, Y.; Davis, T.P.; Hagemeyer, C.E.; Gao, M. Recent advances in molecular imaging of atherosclerotic plaques and thrombosis. Nanoscale 2020, 12, 8040–8064. [Google Scholar] [CrossRef] [PubMed]
- Manolis, A.S.; Manolis, T.A. Patients with Polyvascular Disease: A Very High-Risk Group. Curr. Vasc. Pharmacol. 2022, 20, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Song, T.-T.; Bi, Y.-H.; Gao, Y.-Q.; Huang, R.; Hao, K.; Xu, G.; Tang, J.-W.; Ma, Z.-Q.; Kong, F.-P.; Coote, J.H.; et al. Systemic pro-inflammatory response facilitates the development of cerebral edema during short hypoxia. J. Neuroinflammation 2016, 13, 63. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Chang, P.; Ding, W.; Bian, J.; Wang, D.; Wang, X.; Luo, Q.; Wu, X.; Zhu, L. Pharmacological inhibition of mitochondrial division attenuates simulated high-altitude exposure-induced cerebral edema in mice: Involvement of inhibition of the NF-κB signaling pathway in glial cells. Eur. J. Pharmacol. 2022, 929, 175137. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-W.; Lin, C.-H.; Hsu, R.-B. Mechanisms of early and delayed stroke after systematic off-pump coronary artery bypass. J. Formos. Med. Assoc. 2015, 114, 988–994. [Google Scholar] [CrossRef] [Green Version]
- Lan, L.; Leng, X.; Ip, V.; Soo, Y.; Abrigo, J.; Liu, H.; Fan, F.; Ma, S.H.; Ma, K.; Ip, B.Y.; et al. Sustaining cerebral perfusion in intracranial atherosclerotic stenosis: The roles of antegrade residual flow and leptomeningeal collateral flow. J. Cereb. Blood Flow Metab. 2018, 40, 126–134. [Google Scholar] [CrossRef]
- Liu, H.; Wang, D.; Leng, X.; Zheng, D.; Chen, F.; Wong, L.K.S.; Shi, L.; Leung, T.W.H. State-of-the-Art Computational Models of Circle of Willis With Physiological Applications: A Review. IEEE Access 2020, 8, 156261–156273. [Google Scholar] [CrossRef]
- Fang, H.; Leng, X.; Pu, Y.; Zou, X.; Pan, Y.; Song, B.; Soo, Y.O.Y.; Leung, T.W.H.; Wang, C.; Zhao, X.; et al. Hemodynamic Significance of Middle Cerebral Artery Stenosis Associated With the Severity of Ipsilateral White Matter Changes. Front. Neurol. 2020, 11, 214. [Google Scholar] [CrossRef]
- Li, L.; He, S.; Liu, H.; Pan, M.; Dai, F. Potential risk factors of persistent postural-perceptual dizziness: A pilot study. J. Neurol. 2021, 269, 3075–3085. [Google Scholar] [CrossRef] [PubMed]
- Zarrinkoob, L.; Wåhlin, A.; Ambarki, K.; Eklund, A.; Malm, J. Quantification and mapping of cerebral hemodynamics before and after carotid endarterectomy, using four-dimensional flow magnetic resonance imaging. J. Vasc. Surg. 2021, 74, 910–920.e1. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, M.; Engström, K.G. Stroke after cardiac surgery—Hemispheric distribution and survival. Scand. Cardiovasc. J. 2012, 47, 136–144. [Google Scholar] [CrossRef]
- van der Velpen, I.F.; Yancy, C.W.; Sorond, F.A.; Sabayan, B. Impaired Cardiac Function and Cognitive Brain Aging. Can. J. Cardiol. 2017, 33, 1587–1596. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
| Age, years, Me (Q25; Q75) | 59 (56; 64) |
| Mini-mental state, scores, | |
| Me (Q25; Q75) | 27 (26; 28) |
| Frontal assessment battery, scores, Me (Q25; Q75) | 16 (15; 17) |
| BDI-II, scores, Me (Q25; Q75) | 3 (2; 4) |
| Educational attainment, years, n (%) | |
| 8–10 | 101 (72) |
| ≥15 | 39 (28) |
| Functional class of angina, n (%) | |
| I-II | 94 (67) |
| III | 46 (33) |
| Functional class NYHA, n (%) | |
| I-II | 109 (78) |
| III | 31 (22) |
| History of myocardial infarction, n (%) | 104 (74) |
| Fraction of left ventricle ejection, %, Me (Q25; Q75) | 58 (54; 62) |
| Type 2 of diabetes mellitus, n (%) | 48 (34) |
| Carotid arteries stenoses, n (%) | |
| One-sided ≤50% | 29 (21) |
| One-sided 70–99% | 7 (5) |
| Two-sided ≥50% | 47 (34) |
| History of stroke, n (%) | 15 (11) |
| Cardiopulmonary bypass time, min, Me (Q25; Q75) | 90 (83; 97) |
| Aorta cross-clamping time, min, Me (Q25; Q75) | 68 (56; 50) |
| Medication, n (%) | |
| ACEi | 124 (89%) |
| Statin | 94 (67%) |
| Beta-blockers | 137 (98%) |
| Antiplatelet drugs | 135 (96%) |
| CCB | 59 (42%) |
| Nitrates | 23 (16%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarasova, I.; Trubnikova, O.; Kupriyanova, D.; Kukhareva, I.; Syrova, I.; Sosnina, A.; Maleva, O.; Barbarash, O. Effect of Carotid Stenosis Severity on Patterns of Brain Activity in Patients after Cardiac Surgery. Appl. Sci. 2023, 13, 20. https://doi.org/10.3390/app13010020
Tarasova I, Trubnikova O, Kupriyanova D, Kukhareva I, Syrova I, Sosnina A, Maleva O, Barbarash O. Effect of Carotid Stenosis Severity on Patterns of Brain Activity in Patients after Cardiac Surgery. Applied Sciences. 2023; 13(1):20. https://doi.org/10.3390/app13010020
Chicago/Turabian StyleTarasova, Irina, Olga Trubnikova, Darya Kupriyanova, Irina Kukhareva, Irina Syrova, Anastasia Sosnina, Olga Maleva, and Olga Barbarash. 2023. "Effect of Carotid Stenosis Severity on Patterns of Brain Activity in Patients after Cardiac Surgery" Applied Sciences 13, no. 1: 20. https://doi.org/10.3390/app13010020
APA StyleTarasova, I., Trubnikova, O., Kupriyanova, D., Kukhareva, I., Syrova, I., Sosnina, A., Maleva, O., & Barbarash, O. (2023). Effect of Carotid Stenosis Severity on Patterns of Brain Activity in Patients after Cardiac Surgery. Applied Sciences, 13(1), 20. https://doi.org/10.3390/app13010020