
Computational Fluid Dynamics (CFD) and Finite Element Analysis (FEM) of a Customized Stent-Graft for Endovascular (EVAR) Treatment of Abdominal Aortic Aneurism (AAA)

 , ,
, ,
Abstract
:1. Introduction
- Diameter and length of the infrarenal aorta and neck of the aorta,
- Diameter and length of the iliac attachments,
- Tortuosity and size of the access vessels, and
- Critical vessel anatomy.
- Neck length ≥ 15 mm,
- Neck diameter < 30 mm,
- Neck angulation < 60–80 degrees, and
- Iliac diameter ≤ 7 mm.
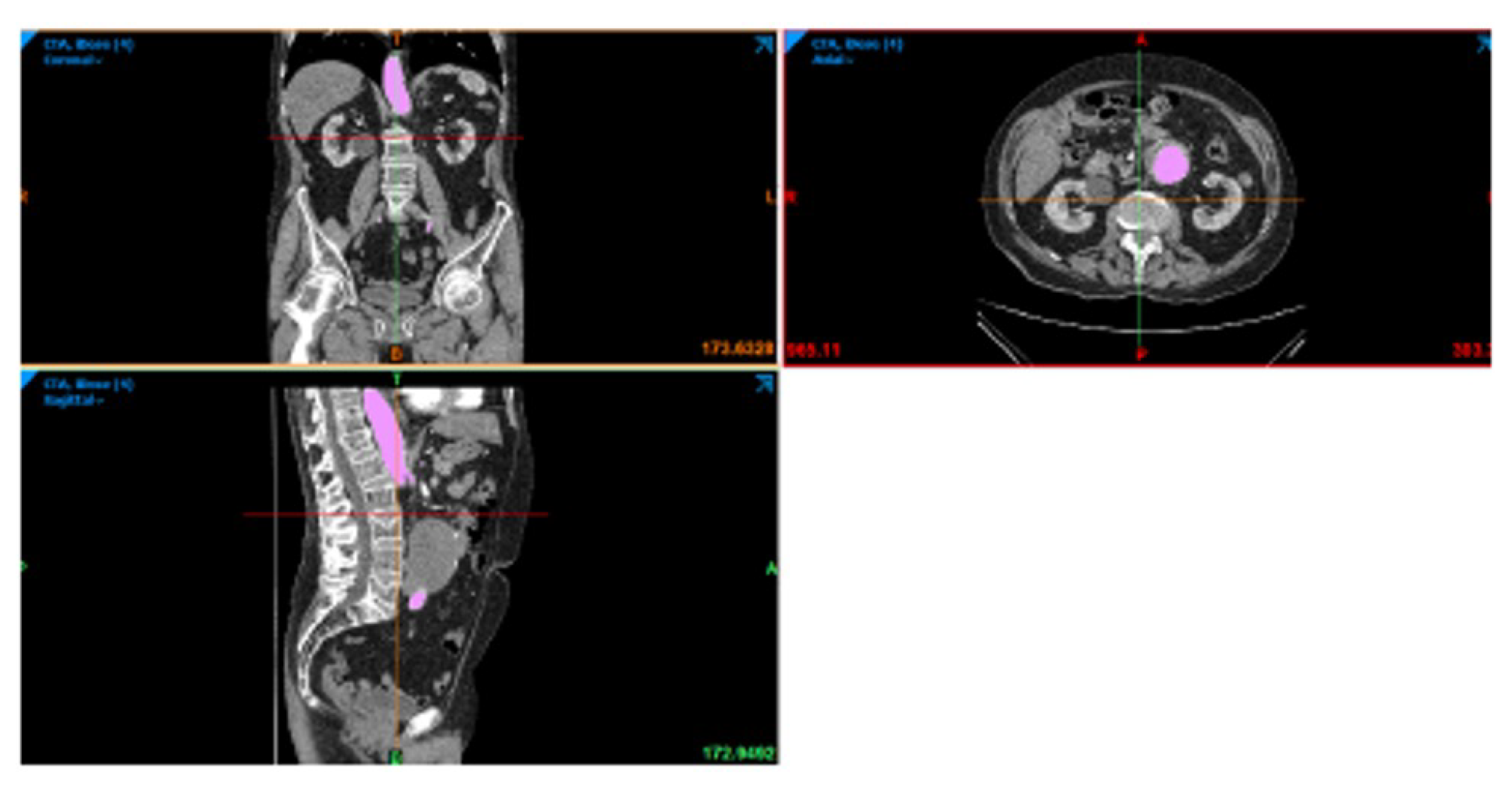
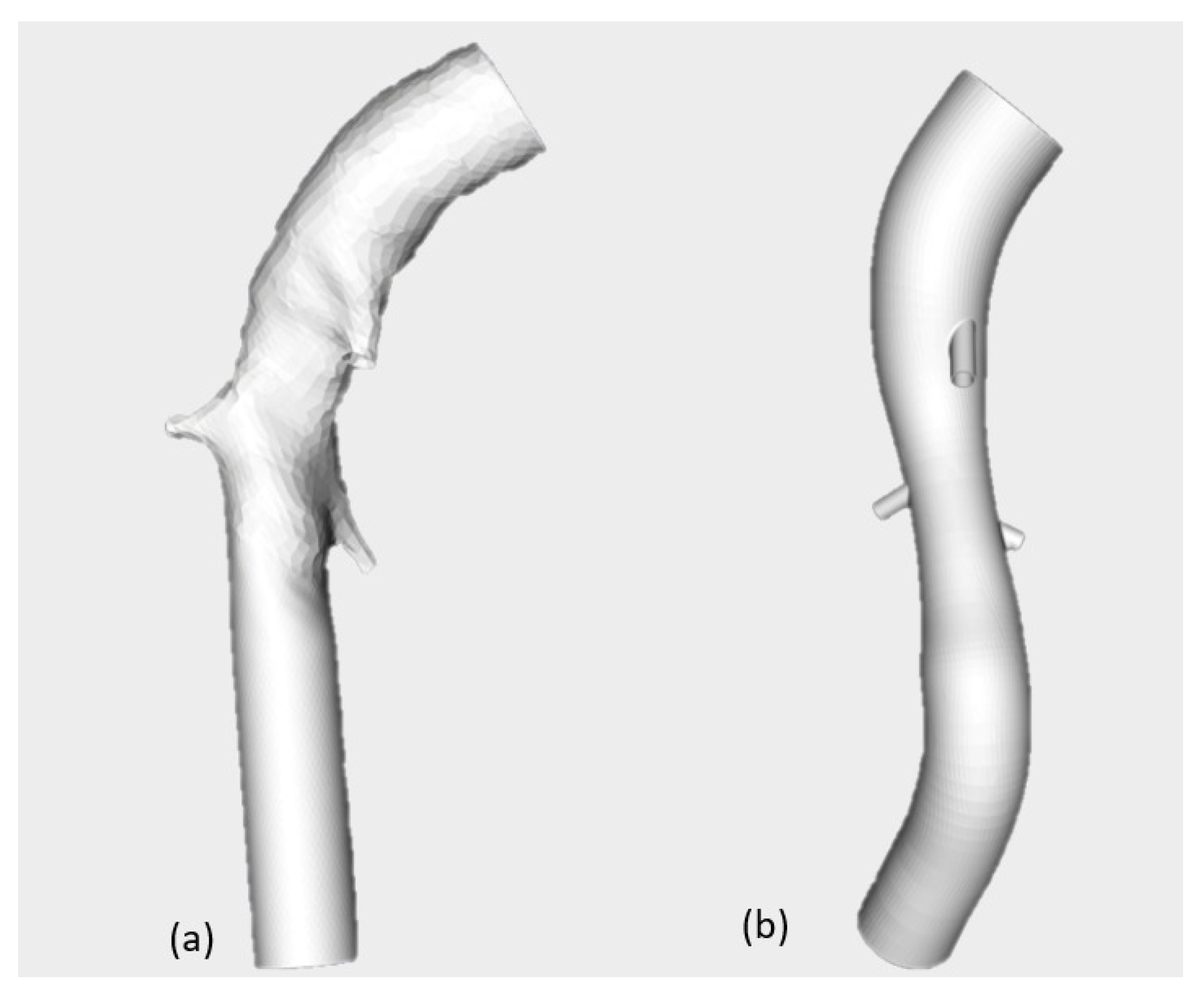
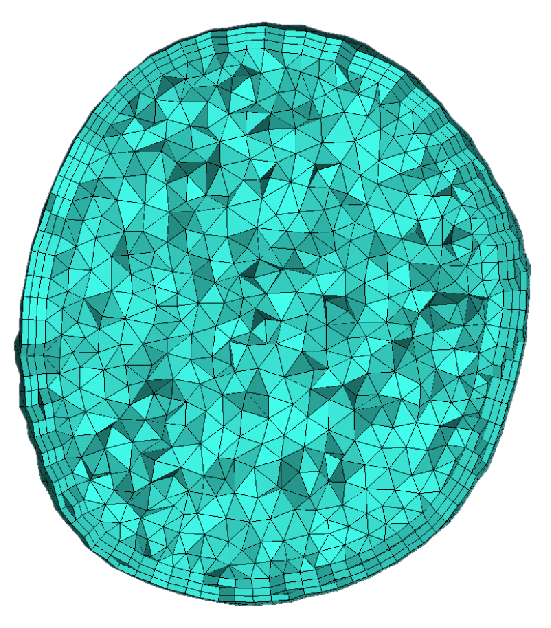
2. Materials and Methods
- The blood flow was assumed incompressible and Newtonian with a density of 1060 and viscosity of 0.003 .
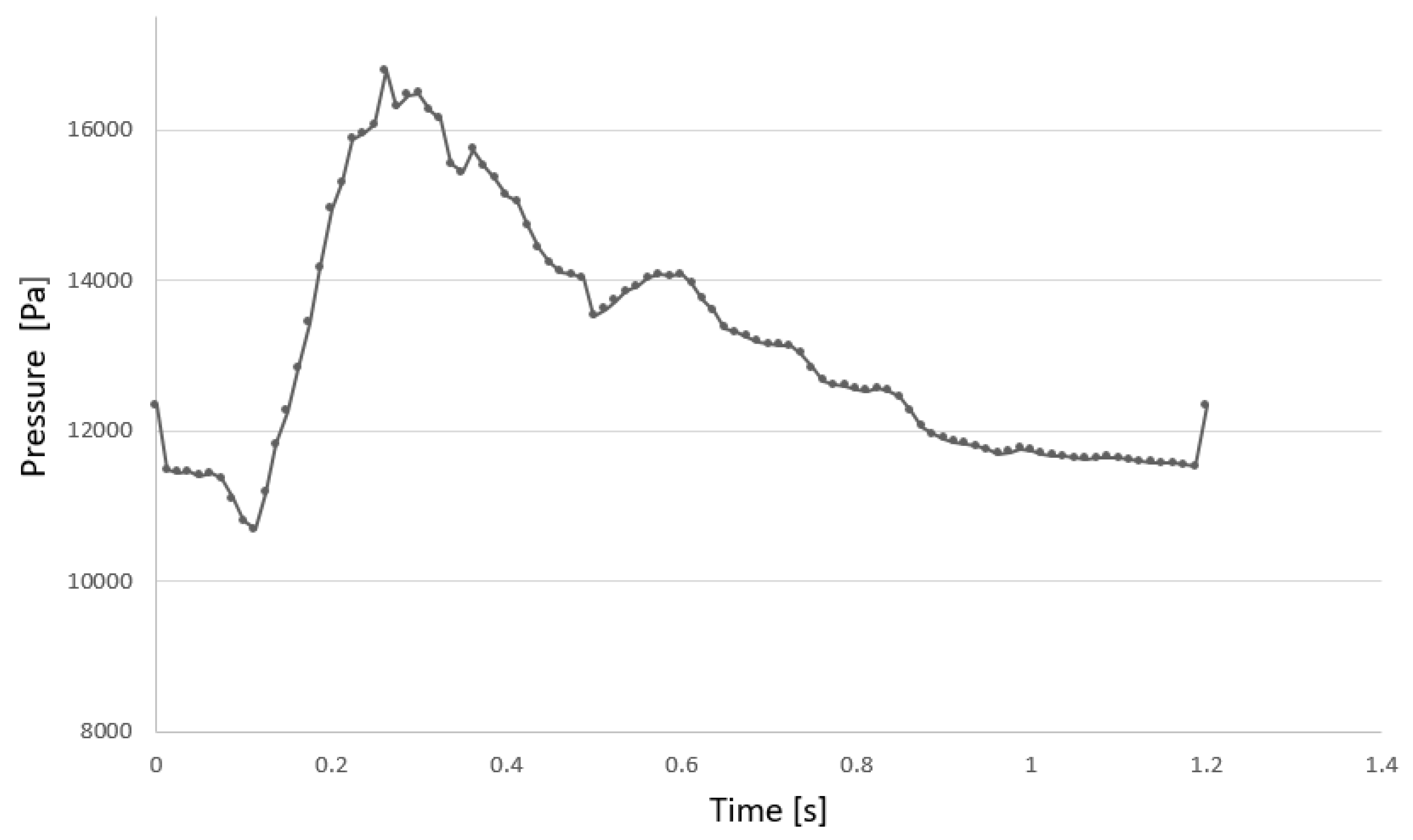
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Kravchenko, I. ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [PubMed]
- Daugherty, A.; Cassis, L.A. Mechanisms of abdominal aortic aneurysm formation. Curr. Atheroscler. Rep. 2002, 4, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, S.; Qamar, A.; Sharma, V.; Sharma, A. Abdominal aortic aneurysm: A comprehensive review. Exp. Clin. Cardiol. 2002, 16, 11–15. [Google Scholar]
- Xenos, M.; Rambhia, S.H.; Alemu, Y.; Einav, S.; Labropoulos, N.; Tassiopoulos, A.; Bluestein, D. Patient-based abdominal aortic aneurysm rupture risk prediction with fluid structure interaction modeling. Ann. Biomed. Eng. 2010, 38, 3323–3337. [Google Scholar] [CrossRef]
- Alaimo, G.; Auricchio, F.; Conti, M.; Zingales, M. Multi-objective optimization of nitinol stent design. Med. Eng. Phys. 2017, 47, 13–24. [Google Scholar] [CrossRef]
- Wolters, B.J.B.M.; Rutten, M.C.M.; Schurink, G.W.H.; Kose, U.; de Hart, J.; van de Vosse, F.N. A patient-specific computational model of fluid–structure interaction in abdominal aortic aneurysms. Med. Eng. Phys. 2005, 871–883. [Google Scholar] [CrossRef]
- Fillinger, M.F.; Marra, S.P.; Raghavan, M.L.; Kennedy, F.E. Prediction of rupture risk in abdominal aortic aneurysm during observation: Wall stress versus diameter. J. Vasc. Surg. 2003, 37, 724–732. [Google Scholar] [CrossRef]
- Leung, J.H.; Wright, A.R.; Cheshire, N.; Crane, J.; Thom, S.A.; Hughes, A.D.; Xu, Y. Fluid structure interaction of patient specific abdominal aortic aneurysms: A comparison with solid stress models. Biomed. Eng. Online 2006, 5, 33. [Google Scholar] [CrossRef]
- Vorp, D.A.; Raghavan, M.L.; Webster, M.W. Mechanical wall stress in abdominal aortic aneurysm: Influence of diameter and asymmetry. J. Vasc. Surg. 1998, 27, 632–639. [Google Scholar] [CrossRef]
- Wang, D.H.; Makaroun, M.S.; Webster, M.W.; Vorp, D.A. Effect of intraluminal thrombus on wall stress in patient-specific models of abdominal aortic aneurysm. J. Vasc. Surg. 2002, 36, 598–604. [Google Scholar] [CrossRef]
- Jayendiran, R.; Nour, B.; Ruimi, A. Computational fluid–structure interaction analysis of blood flow on patient-specific reconstructed aortic anatomy and aneurysm treatment with Dacron graft. J. Fluids Struct. 2018, 81, 693–711. [Google Scholar] [CrossRef]
- Raghavan, M.L.; Vorp, D.A.; Federle, M.P.; Makaroun, M.S.; Webster, M.W. Wall stress distribution on three-dimensionally reconstructed models of human abdominal aortic aneurysm. J. Vasc. Surg. 2000, 31, 760–769. [Google Scholar] [CrossRef]
- Soudah, E.; Ng, E.Y.; Loong, T.H.; Bordone, M.; Pua, U.; Narayanan, S. CFD Modelling of Abdominal Aortic Aneurysm on Hemodynamic Loads Using a Realistic Geometry with CT. Comput. Math. Methods Med. 2013, 2013, 472564. [Google Scholar] [CrossRef]
- Stergiou, Y.G.; Kanaris, A.G.; Mouza, A.A.; Paras, S.V. Fluid-structure interaction in abdominal aortic aneurysms: Effect of haematocrit. Fluids 2019, 4, 11. [Google Scholar] [CrossRef]
- Lin, S.; Han, X.; Bi, Y.; Ju, S.; Gu, L. Fluid-structure interaction in abdominal aortic aneurysm: Effect of modeling techniques. BioMed Res. Int. 2017, 2017, 7023078. [Google Scholar] [CrossRef]
- Philip, N.T.; Patnaik, B.S.V.; Sudhir, B.J. Hemodynamic simulation of abdominal aortic aneurysm on idealised models: Investigation of stress parameters during disease progression. Comput. Methods Programs Biomed. 2021, 213, 106508. [Google Scholar] [CrossRef]
- Salman, H.E.; Yalcin, H.C. Computational Investigation of the Effect of Wall Thickness on Rupture Risk in Abdominal Aortic Aneurysms. J. Appl. Fluid Mech. 2021, 14, 499–513. [Google Scholar]
- Đorovic, S.; Filipovic, N. Computational analysis of abdominal aortic aneurysm before and after endovascular aneurysm repair. Comput. Model. Bioeng. Bioinform. 2019, 353. [Google Scholar]
- Li, Z.; Kleinstreuer, C. Blood flow and structure interactions in a stented abdominal aortic aneurysm model. Med. Eng. Phys. 2005, 27, 369–382. [Google Scholar] [CrossRef]
- Dinoto, E.; Mirabella, D.; Ferlito, F.; Tortomasi, G.; Turchino, D.; Evola, S.; Zingales, M.; Bologna, E.; Pecoraro, F. Carotid Artery Disease in the Era of Biomarkers: A Pilot Study. Diagnostics 2023, 13, 644. [Google Scholar] [CrossRef]
- Bologna, E.; Di Paola, M.; Zingales, M. Analysis of a Beck’s column over fractional-order restraints via extended Routh-Hurwitz theorem. In Modern Trends in Structural and Solid Mechanics 1: Statics and Stability; Challamel, N., Kaplunov, J., Takewaki, I., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2021; pp. 43–66. [Google Scholar]
- Alotta, G.; Bologna, E.; Zingales, M. Exact mechanical hierarchy of non-linear fractional-order hereditariness. Symmetry 2020, 12, 673. [Google Scholar] [CrossRef]
- Bologna, E.; Di Paola, M.; Zingales, M. A single integral approach to fractional order non-linear hereditariness. In Lecture Notes in Mechanical Engineering; Springer: Cham, Switzerland, 2020; pp. 932–944. [Google Scholar]
- Alotta, G.; Bologna, E.; Failla, G.; Zingales, M. A Fractional Approach to Non-Newtonian Blood Rheology in Capillary Vessels. J. Peridynamics Nonlocal Model. 2019, 1, 88–96. [Google Scholar] [CrossRef]
- Bologna, E.; Graziano, F.; Deseri, L.; Zingales, M. Power-Laws hereditariness of biomimetic ceramics for cranioplasty neurosurgery. Int. J. -Non-Linear Mech. 2019, 115, 61–67. [Google Scholar] [CrossRef]
- Camarda, L.; Bologna, E.; Pavan, D.; Morello, F.; Monachino, F.; Giacco, F.; Zingales, M. Posterior meniscal root repair: A biomechanical comparison between human and porcine menisci. Muscles Ligaments Tendons J. 2019, 9, 76–81. [Google Scholar] [CrossRef]
- De Caro, V.; Murgia, D.; Seidita, F.; Bologna, E.; Alotta, G.; Zingales, M.; Campisi, G. Enhanced in situ availability of Aphanizomenon Flos-Aquae constituents entrapped in buccal films for the treatment of oxidative stress-related oral diseases: Biomechanical characterization and in vitro/ex vivo evaluation. Pharmaceutics 2019, 11, 35. [Google Scholar] [CrossRef]
- Dintcheva, N.T.; Baiamonte, M.; Teresi, R.; Alotta, G.; Bologna, E.; Zingales, M. A Fractional-Order Model of Biopolyester Containing Naturally Occurring Compounds for Soil Stabilization. Adv. Mater. Sci. Eng. 2019, 2019, 5986564. [Google Scholar] [CrossRef]
- Alotta, G.; Bologna, E.; Di Giuseppe, M.; Zingales, M.; Dimitri, R.; Pinnola, F.P.; Zavarise, G. A Non-Local Mode-I Cohesive Model for Ascending Thoracic Aorta Dissections (ATAD). In Proceedings of the IEEE 4th International Forum on Research and Technologies for Society and Industry, RTSI 2018, Palermo, Italy, 10–13 September 2018; p. 8548349. [Google Scholar]
- Di Giuseppe, M.; Zingales, M.; Bologna, E.; Pasta, S.; Alotta, G. Hereditariness of Aortic Tissue: In-Vitro Time-Dependent Failure of Human and Porcine Specimens. In Proceedings of the IEEE 4th International Forum on Research and Technologies for Society and Industry, RTSI, Palermo, Italy, 10–13 September 2018; p. 8548387. [Google Scholar]
- Barrera, O.; Bologna, E.; Alotta, G.; Zingales, M. Experimental Characterization of the Human Meniscal Tissues. In Proceedings of the IEEE 4th International Forum on Research and Technologies for Society and Industry, RTSI, Palermo, Italy, 10–13 September 2018; p. 8548369. [Google Scholar]
- Bologna, E.; Zingales, M.; Alotta, G.; Deseri, L. Quasi-Fractional Models of Human Tendons Hereditariness. In Proceedings of the IEEE 4th International Forum on Research and Technologies for Society and Industry, RTSI, Palermo, Italy, 10–13 September 2018; p. 8548419. [Google Scholar]
- Bologna, E.; Zingales, M. Stability analysis of beck’s column over a fractional-order hereditary foundation. Proc. R. Soc. A Math. Phys. Eng. Sci. 2018, 474, 2218. [Google Scholar] [CrossRef]
- Palumbo, F.S.; Fiorica, C.; Pitarresi, G.; Zingales, M.; Bologna, E.; Giammona, G. Multifibrillar bundles of a self-assembling hyaluronic acid derivative obtained through a microfluidic technique for aortic smooth muscle cell orientation and differentiation. Biomater. Sci. 2018, 6, 2518–2526. [Google Scholar] [CrossRef]
- Bologna, E.; Deseri, L.; Zingales, M. A state-space approach to dynamic stability of fractional-order systems: The extended Routh-Hurwitz theorem. In Proceedings of the AIMETA 2017—Proceedings of the 23rd Conference of the Italian Association of Theoretical and Applied Mechanics, Salerno, Italy, 4–7 September 2017; Volume 5, pp. 969–976. [Google Scholar]
- Holzapfel, G.A.; Ogden, R.W. (Eds.) Biomechanics of Soft Tissue in Cardiovascular Systems; Springer: Berlin/Heidelberg, Germany, 2014; Volume 441. [Google Scholar]
- Holzapfel, G.A.; Ogden, R.W. Biomechanical relevance of the microstructure in artery walls with a focus on passive and active components. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H540–H549. [Google Scholar] [CrossRef]
- Holzapfel, G.A. Biomechanics of soft tissue. In The Handbook of Materials Behavior Models; Academic Press: Cambridge, MA, USA, 2001; Volume 3, pp. 1049–1063. [Google Scholar]
- Yamamoto, E.; Hayashi, K.; Yamamoto, N. Mechanical properties of collagen fascicles from the rabbit patellar tendon. J. Biomech. Eng. 1999, 121, 124–131. [Google Scholar] [CrossRef]
- Marchiori, G.; Lopomo, N.F.; Bologna, E.; Spadaro, D.; Camarda, L.; Berni, M.; Zingales, M. How preconditioning and pretensioning of grafts used in ACLigaments surgical reconstruction are influenced by their mechanical time-dependent characteristics: Can we optimize their initial loading state? Clin. Biomech. 2021, 83, 105294. [Google Scholar] [CrossRef]
- Bologna, E.; Di Paola, M.; Dayal, K.; Deseri, L.; Zingales, M. Fractional-order nonlinear hereditariness of tendons and ligaments of the human knee. Philos. Trans. R. Soc. A 2020, 378, 20190294. [Google Scholar] [CrossRef]
- Bologna, E.; Lopomo, N.; Marchiori, G.; Zingales, M. A non-linear stochastic approach of ligaments and tendons fractional-order hereditariness. Probab. Eng. Mech. 2020, 60, 103034. [Google Scholar] [CrossRef]
- Nuzzo, G.; Amiri, F.; Russotto, S.; Bologna, E.; Zingales, M. A fractional-order theory of phase transformation in presence of anomalous heat transfer. Theor. Appl. Mech. AIMETA 2022 2023, 26, 77–82. [Google Scholar]
- Nuzzo, G.; Bologna, E.; Dayal, K.; Zingales, M. Fractional diffusion of membrane receptors in endocytosis pathway. Theor. Appl. Mech. AIMETA 2022 2023, 26, 305–310. [Google Scholar]
- Ragusa, S.; Siciliano, K.; Di Simone, F.P.; Russo, S.; Bologna, E.; Zingales, M. Fluid-structure interaction (FSI) analysis of 3D printing personalized stent-graft for aortic endovascular aneurysm repair (EVAR). Theor. Appl. Mech. AIMETA 2022 2023, 26, 299–304. [Google Scholar]
- Gasser, T.C.; Ogden, R.W.; Holzapfel, G.A. Hyperelastic modelling of arterial layers with distributed collagen fibre orientations. J. R. Soc. Interface 2006, 3, 15–35. [Google Scholar] [CrossRef]
- De Putter, S.; Wolters, B.J.B.M.; Rutten, M.C.M.; Breeuwer, M.; Gerritsen, F.A.; Van de Vosse, F.N. Patient-specific initial wall stress in abdominal aortic aneurysms with a backward incremental method. J. Biomech. 2007, 40, 1081–1090. [Google Scholar] [CrossRef]
- Scotti, C.M.; Finol, E.A. Compliant biomechanics of abdominal aortic aneurysms: A fluid–structure interaction study. Comput. Struct. 2007, 85, 1097–1113. [Google Scholar] [CrossRef]
- Li, Z.; Kleinstreuer, C. Computational analysis of type II endoleaks in a stented abdominal aortic aneurysm model. J. Biomech. 2006, 39, 2573–2582. [Google Scholar] [CrossRef]
- Chong, C.; How, T.; Gilling-Smith, G.; Harris, P. Modeling endoleaks and collateral reperfusion following endovascular AAA exclusion. J. Endovasc. Ther. 2003, 10, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, E.S.; Guadagni, G.; Fumero, A.; Ballerini, G.; Spirito, R.; Biglioli, P.; Redaelli, A. Fluid–structure interaction within realistic three-dimensional models of the aneurysmatic aorta as a guidance to assess the risk of rupture of the aneurysm. Med. Eng. Phys. 2001, 23, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Jayendiran, R.; Nour, B.M.; Ruimi, A. Dacron graft as replacement to dissected aorta: A three-dimensional fluid-structure-interaction analysis. J. Mech. Behav. Biomed. Mater. 2018, 78, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Holzapfel, G.A.; Kauffmann, C.; Soulez, G. Finite element analysis of abdominal aortic aneurysms: Geometrical and structural reconstruction with application of an anisotropic material model. Ima J. Appl. Math. 2014, 79, 1011–1026. [Google Scholar] [CrossRef]
- Molony, D.S.; Callanan, A.; Kavanagh, E.G.; Walsh, M.T.; McGloughlin, T.M. Fluid-structure interaction of a patient-specific abdominal aortic aneurysm treated with an endovascular stent-graft. Biomed. Eng. Online 2009, 8, 24. [Google Scholar] [CrossRef]
- Auricchio, F.; Taylor, R.L. Shape-memory alloys: Modelling and numerical simulations of the finite-strain superelastic behavior. Comput. Methods Appl. Mech. Eng. 1997, 143, 175–194. [Google Scholar] [CrossRef]
- Molony, D.S.; Broderick, S.; Callanan, A.; McGloughlin, T.M.; Walsh, M.T. Fluid–Structure Interaction in Healthy, Diseased and Endovascularly Treated Abdominal Aortic Aneurysms. In Biomechanics and Mechanobiology of Aneurysms; Springer: Berlin/Heidelberg, Germany, 2011; pp. 163–179. [Google Scholar]
- Papaharilaou, Y.; Ekaterinaris, J.A.; Manousaki, E.; Katsamouris, A.N. A decoupled fluid structure approach for estimating wall stress in abdominal aortic aneurysms. J. Biomech. 2006, 40, 367–377. [Google Scholar] [CrossRef]
- Di Martino, E.S.; Vorp, D.A. Effect of variation in intraluminal thrombus constitutive properties on abdominal aortic aneurysm wall stress. Ann. Biomed. Eng. 2003, 31, 804–809. [Google Scholar] [CrossRef]
- Scotti, C.M. Computational Modeling of Patient-Specific AAAs: A Comparison of Pre- and Post-Operative Flow Hemodynamics and Wall Mechanics. Master’s Thesis, Carnegie Mellon University, Pittsburgh, PA, USA, 2004. [Google Scholar]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Description | Value |
|---|---|---|
| Austenite Young’ Modulus | 53,001 MPa | |
| Austenite Poisson’s Ration | 0.3 | |
| Martensite Young’ Modulus | 21.500 MPa | |
| Martensite Poisson’s Ration | 0.3 | |
| Transformation Strain | 0.038 | |
| Start of Transformation Loading | 434 MPa | |
| End of Transformation Loading | 500 MPa | |
| Start of Transformation Unloading | 210 MPa | |
| End of Transformation Unloading | 138.7 MPa | |
| Start of Transformation Stress in Compression | 434.0 MPa | |
| Volumetric Transformation Strain | 0.038 MPa |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bologna, E.; Dinoto, E.; Di Simone, F.; Pecoraro, F.; Ragusa, S.; Siciliano, K.; Zingales, M. Computational Fluid Dynamics (CFD) and Finite Element Analysis (FEM) of a Customized Stent-Graft for Endovascular (EVAR) Treatment of Abdominal Aortic Aneurism (AAA). Appl. Sci. 2023, 13, 5712. https://doi.org/10.3390/app13095712
Bologna E, Dinoto E, Di Simone F, Pecoraro F, Ragusa S, Siciliano K, Zingales M. Computational Fluid Dynamics (CFD) and Finite Element Analysis (FEM) of a Customized Stent-Graft for Endovascular (EVAR) Treatment of Abdominal Aortic Aneurism (AAA). Applied Sciences. 2023; 13(9):5712. https://doi.org/10.3390/app13095712
Chicago/Turabian StyleBologna, Emanuela, Ettore Dinoto, Francesco Di Simone, Felice Pecoraro, Sara Ragusa, Katia Siciliano, and Massimiliano Zingales. 2023. "Computational Fluid Dynamics (CFD) and Finite Element Analysis (FEM) of a Customized Stent-Graft for Endovascular (EVAR) Treatment of Abdominal Aortic Aneurism (AAA)" Applied Sciences 13, no. 9: 5712. https://doi.org/10.3390/app13095712
APA StyleBologna, E., Dinoto, E., Di Simone, F., Pecoraro, F., Ragusa, S., Siciliano, K., & Zingales, M. (2023). Computational Fluid Dynamics (CFD) and Finite Element Analysis (FEM) of a Customized Stent-Graft for Endovascular (EVAR) Treatment of Abdominal Aortic Aneurism (AAA). Applied Sciences, 13(9), 5712. https://doi.org/10.3390/app13095712