
The Influence of Diabetes on Multisensory Integration and Mobility in Aging


Abstract
:1. Introduction
2. Materials and Methods
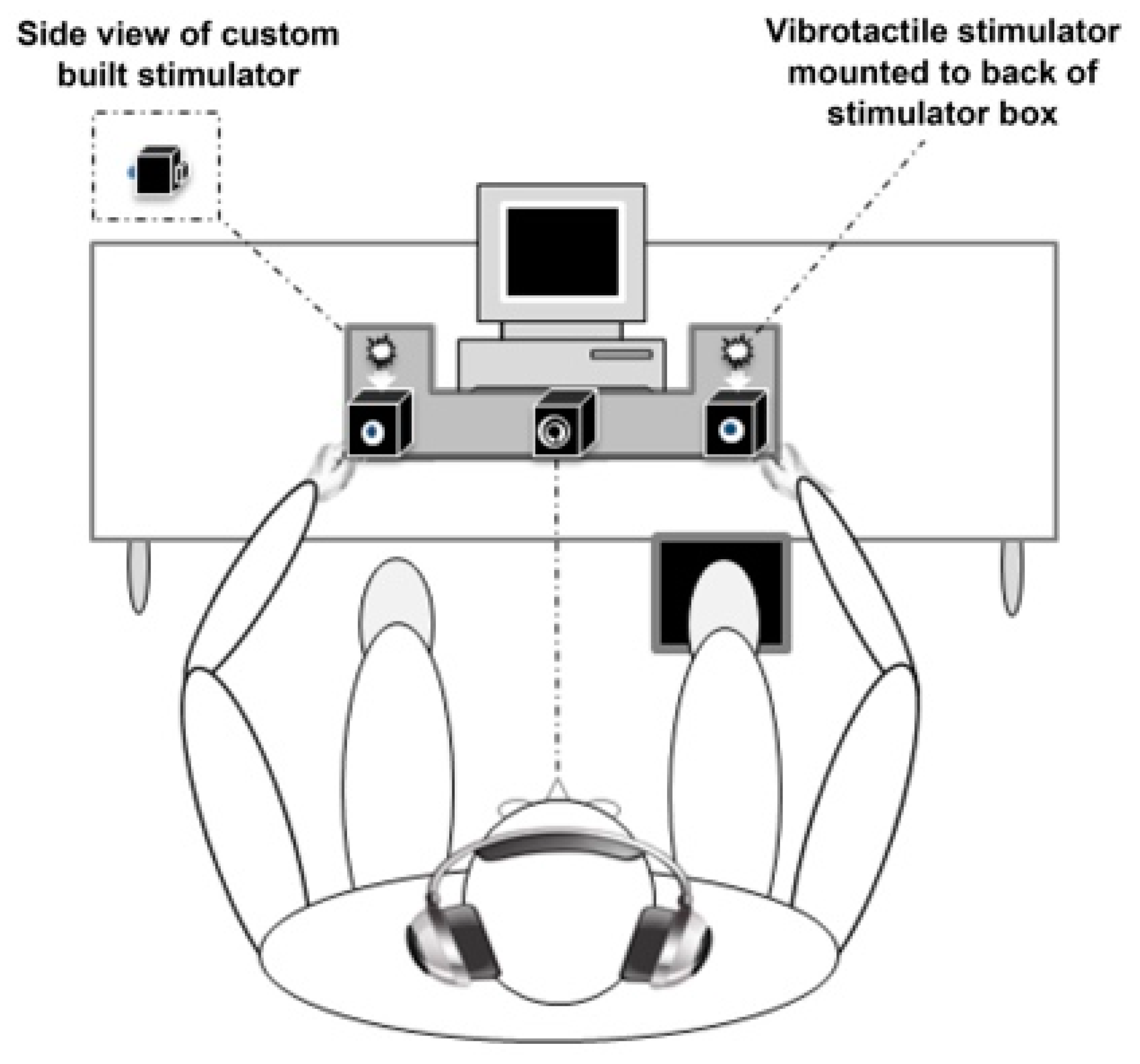
2.1. Experimental Design
2.2. Clinical Evaluation
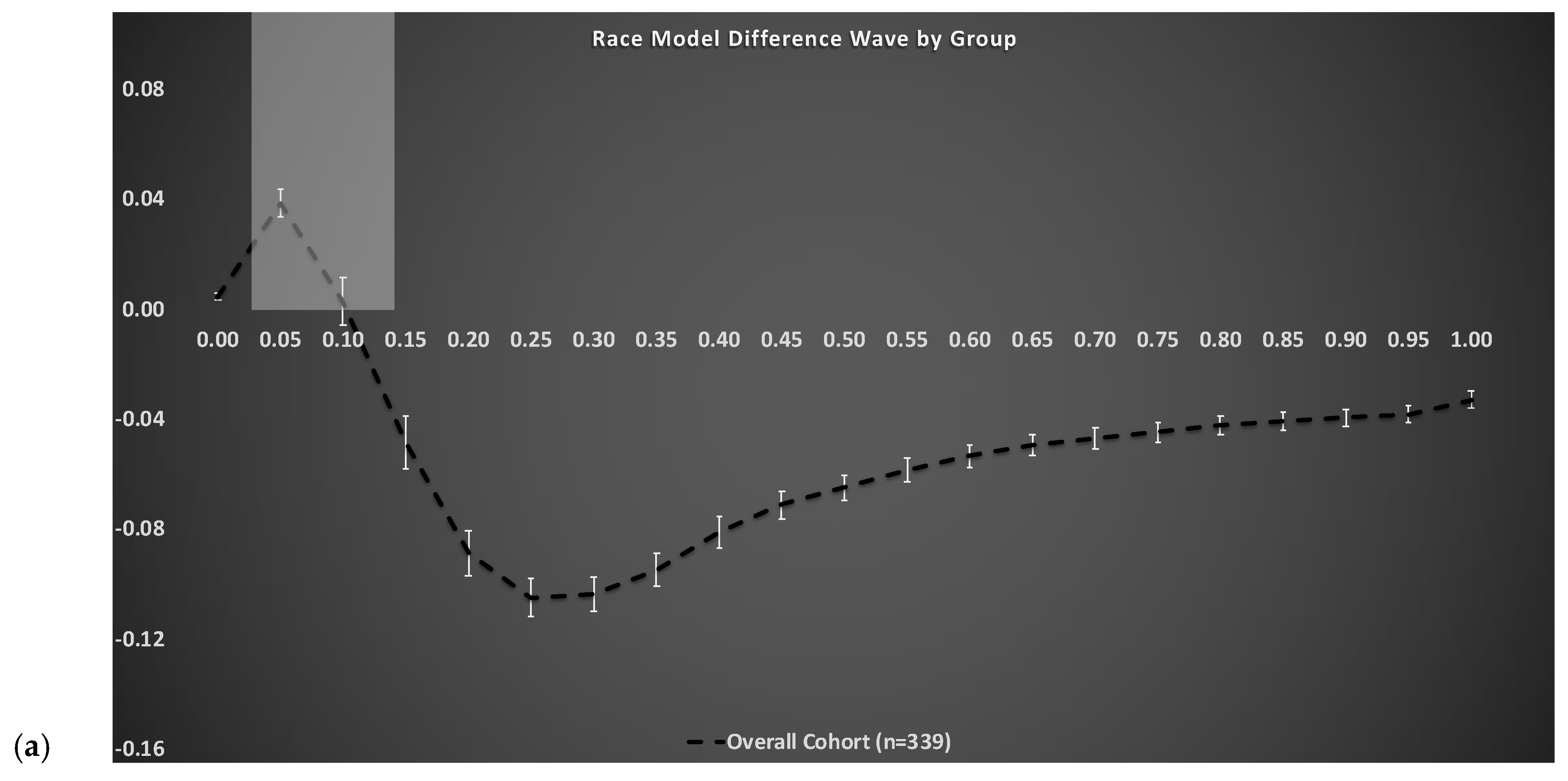
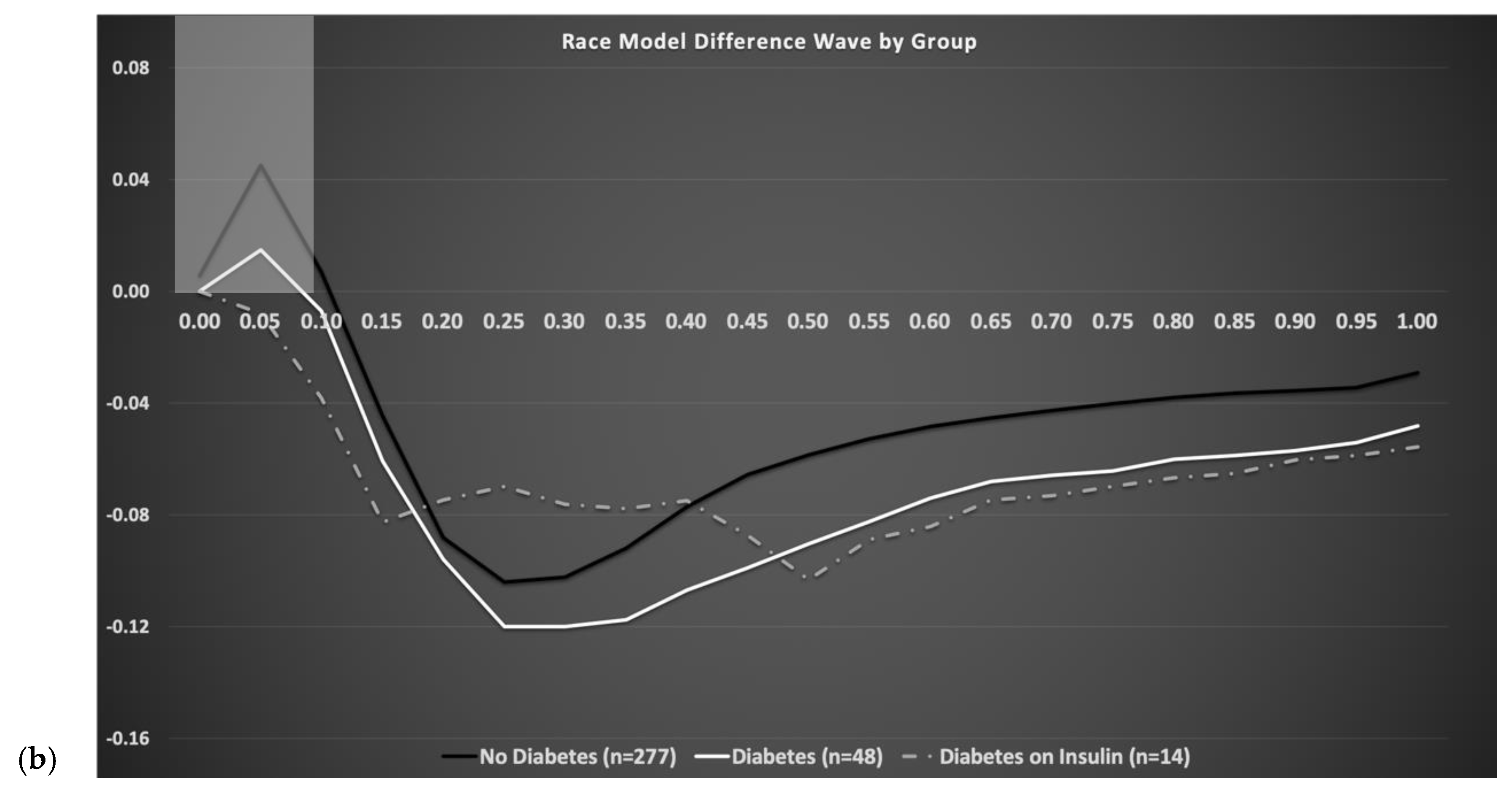
2.3. Quantification of Multisensory Integration Using the Race Model Inequality
2.4. Motor Outcomes
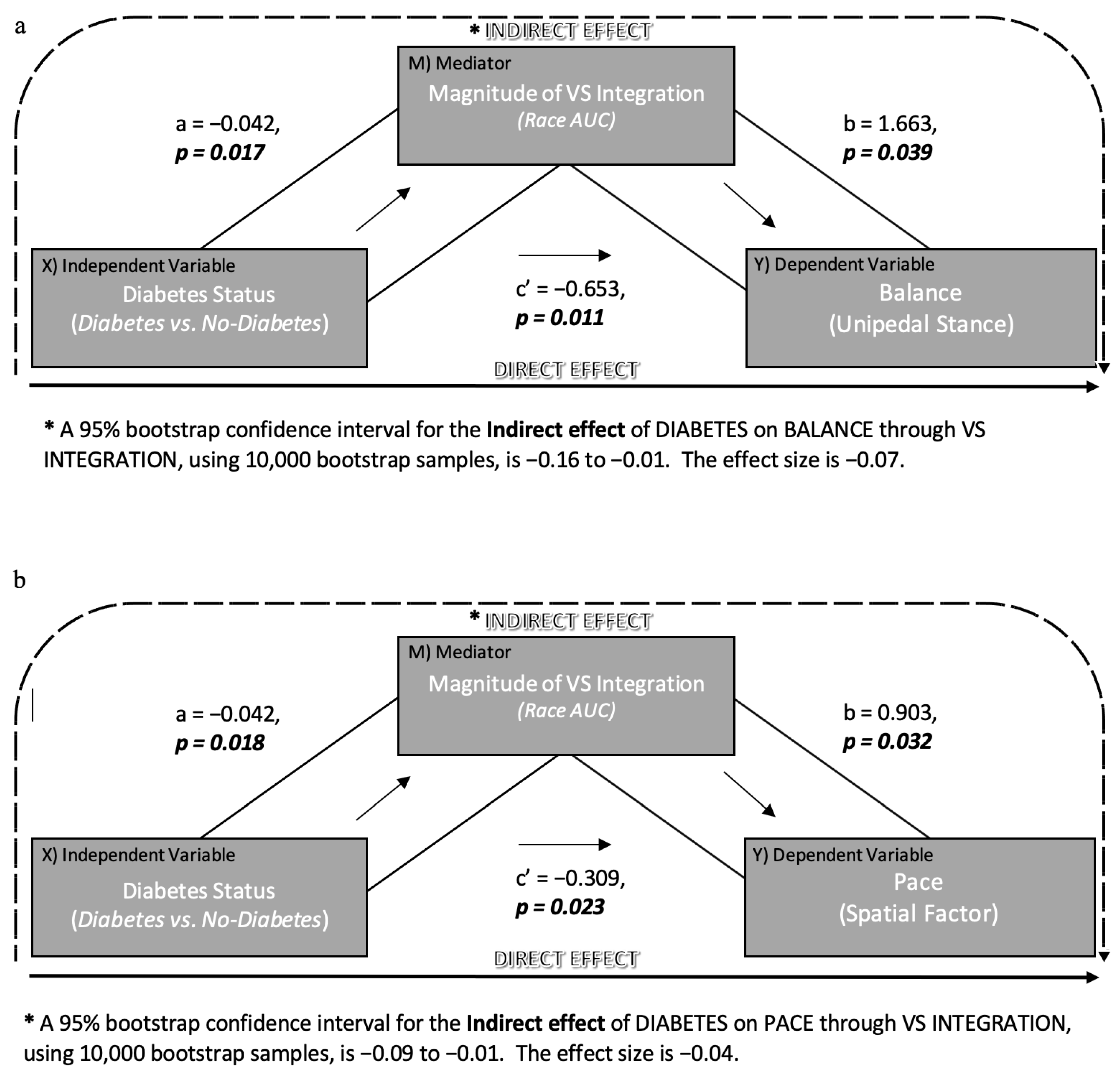
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2020.
- American Diabetes Association, Introduction: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41 (Suppl. 1), S1–S2. [CrossRef] [PubMed] [Green Version]
- Morley, J.E. Diabetes and aging: Epidemiologic overview. Clin. Geriatr. Med. 2008, 24, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Saxton, S.V.; Etten, M.J.; Perkins, E.A. Physical Change & Aging: A Guide for the Helping Professions, 5th ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Baltes, P.B.; Lindenberger, U. Emergence of a powerful connection between sensory and cognitive functions across the adult life span: A new window to the study of cognitive aging? Psychol. Aging 1997, 12, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Lindenberger, U.; Baltes, P.B. Intellectual functioning in old and very old age: Cross-sectional results from the Berlin Aging Study. Psychol. Aging 1997, 12, 410–432. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, J.R.; Verghese, J. Does Cognitive Impairment Influence Visual-Somatosensory Integration and Mobility in Older Adults? J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.M. Diabetes, aging, and cognitive decline. Neurobiol. Aging 2005, 26 (Suppl. 1), 21–25. [Google Scholar] [CrossRef]
- Sims-Robinson, C.; Kim, B.; Rosko, A.; Feldman, E.L. How does diabetes accelerate Alzheimer’s disease pathology? Nat. Rev. Neurol. 2010, 6, 551–559. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; George, C.J.; Izzetoglu, M.; Wang, C. The effect of diabetes on prefrontal cortex activation patterns during active walking in older adults. Brain Cogn. 2018, 125, 14–22. [Google Scholar] [CrossRef]
- Brach, J.S.; Talkowski, J.B.; Strotmeyer, E.S.; Newman, A.B. Diabetes Mellitus and Gait Dysfunction: Possible Explanatory Factors. Phys. Ther. 2008, 88, 1365–1374. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; Mahoney, J.; Verghese, J. Intraindividual Variability in Executive Functions but Not Speed of Processing or Conflict Resolution Predicts Performance Differences in Gait Speed in Older Adults. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2014, 69, 980–986. [Google Scholar] [CrossRef]
- Holtzer, R.; Wang, C.; Verghese, J. Performance variance on walking while talking tasks: Theory, findings, and clinical implications. AGE 2014, 36, 373–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, J.R.; Verghese, J. Using the Race Model Inequality to Quantify Behavioral Multisensory Integration Effects. J. Vis. Exp. 2019, e59575. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, J.R.; Dumas, K.; Holtzer, R. Visual-Somatosensory Integration is Linked to Physical Activity Level in Older Adults. Multisensory Res. 2015, 28, 11–29. [Google Scholar] [CrossRef]
- Mahoney, J.R.; Verghese, J. Visual-Somatosensory Integration and Quantitative Gait Performance in Aging. Front. Aging Neurosci. 2018, 10, 377. [Google Scholar] [CrossRef]
- Mahoney, J.R.; Cotton, K.; Verghese, J. Multisensory Integration Predicts Balance and Falls in Older Adults. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2018, 74, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Holtzer, R.; Goldin, Y.; Zimmerman, M.; Katz, M.; Buschke, H.; Lipton, R.B. Robust norms for selected neuropsychological tests in older adults. Arch. Clin. Neuropsychol. 2008, 23, 531–541. [Google Scholar] [CrossRef] [Green Version]
- Duff, K.; Clark, H.J.D.; O’Bryant, S.E.; Mold, J.W.; Schiffer, R.B.; Sutker, P.B. Utility of the RBANS in detecting cognitive impairment associated with Alzheimer’s disease: Sensitivity, specificity, and positive and negative predictive powers. Arch. Clin. Neuropsychol. 2008, 23, 603–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvin, J.E.; Roe, C.M.; Powlishta, K.K.; Coats, M.A.; Muich, S.J.; Grant, E.; Miller, J.P.; Storandt, M.; Morris, J.C. The AD8: A brief informant interview to detect dementia. Neurology 2005, 65, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Galvin, J.E.; Roe, C.M.; Xiong, C.; Morris, J.C. Validity and reliability of the AD8 informant interview in dementia. Neurology 2006, 67, 1942–1948. [Google Scholar] [CrossRef] [PubMed]
- Buschke, H.; Kuslansky, G.; Katz, M.; Stewart, W.F.; Sliwinski, M.J.; Eckholdt, H.M.; Lipton, R.B. Screening for dementia with the Memory Impairment Screen. Neurology 1999, 52, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R. Within-Person Across-Neuropsychological Test Variability and Incident Dementia. JAMA 2008, 300, 823–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, R.C. Mild Cognitive Impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinchla, R.A. Detecting target elements in multielement arrays: A confusability model. Percept. Psychophys. 1974, 15, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Maris, G.; Maris, E. Testing the race model inequality: A nonparametric approach. J. Math. Psychol. 2003, 47, 507–514. [Google Scholar] [CrossRef]
- Colonius, H.; Diederich, A. The race model inequality: Interpreting a geometric measure of the amount of violation. Psychol. Rev. 2006, 113, 148–154. [Google Scholar] [CrossRef]
- Miller, J. Divided attention: Evidence for coactivation with redundant signals. Cogn. Psychol. 1982, 14, 247–279. [Google Scholar] [CrossRef]
- Gondan, M. A permutation test for the race model inequality. Behav. Res. Methods 2010, 42, 23–28. [Google Scholar] [CrossRef]
- Gondan, M.; Minakata, K. A tutorial on testing the race model inequality. Atten. Percept. Psychophys. 2015, 78, 723–735. [Google Scholar] [CrossRef]
- Hurvitz, E.A.; Richardson, J.K.; Werner, R.A. Unipedal stance testing in the assessment of peripheral neuropathy. Arch. Phys. Med. Rehabil. 2001, 82, 198–204. [Google Scholar] [CrossRef]
- Hurvitz, E.A.; Richardson, J.K.; Werner, R.A.; Ruhl, A.M.; Dixon, M.R. Unipedal stance testing as an indicator of fall risk among older outpatients. Arch. Phys. Med. Rehabil. 2000, 81, 587–591. [Google Scholar] [CrossRef]
- Menz, H.B.; Latt, M.D.; Tiedemann, A.; Kwan, M.M.S.; Lord, S.R. Reliability of the GAITRite walkway system for the quantification of temporo-spatial parameters of gait in young and older people. Gait Posture 2004, 20, 20–25. [Google Scholar] [CrossRef]
- Brach, J.S.; Perera, S.; Studenski, S.; Newman, A.B. The Reliability and Validity of Measures of Gait Variability in Community-Dwelling Older Adults. Arch. Phys. Med. Rehabil. 2008, 89, 2293–2296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilney, B.; Morris, M.; Webster, K. Concurrent related validity of the GAITRite® walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture 2003, 17, 68–74. [Google Scholar] [CrossRef]
- Verghese, J.; Kuslansky, G.; Holtzer, R.; Katz, M.; Xue, X.; Buschke, H.; Pahor, M. Walking While Talking: Effect of Task Prioritization in the Elderly. Arch. Phys. Med. Rehabil. 2007, 88, 50–53. [Google Scholar] [CrossRef] [Green Version]
- Verghese, J.; Lipton, R.B.; Hall, C.B.; Kuslansky, G.; Katz, M.J.; Buschke, H. Abnormality of gait as a predictor of non-Alzheimer’s dementia. N. Engl. J. Med. 2002, 347, 1761–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Romanski, L.M. Convergence of Auditory, Visual, and Somatosensory Information in Ventral Prefrontal Cortex. In The Neural Bases of Multisensory Processes; Murray, M.M., Wallace, M.T., Eds.; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- Cao, Y.; Summerfield, C.; Park, H.; Giordano, B.L.; Kayser, C. Causal Inference in the Multisensory Brain. Neuron 2019, 102, 1076–1087.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchet, O.; Allali, G.; Annweiler, C.; Verghese, J. Association of Motoric Cognitive Risk Syndrome with Brain Volumes: Results from the GAIT Study. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2016, 71, 1081–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Zettel-Watson, L.; Suen, M.; Wehbe, L.; Rutledge, D.N.; Cherry, B.J. Aging well: Processing speed inhibition and working memory related to balance and aerobic endurance. Geriatr. Gerontol. Int. 2015. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; Wang, C.; Verghese, J. The Relationship between Attention and Gait in Aging: Facts and Fallacies. Mot. Control. 2012, 16, 64–80. [Google Scholar] [CrossRef] [Green Version]
- Verghese, J.; Wang, C.; Lipton, R.B.; Holtzer, R.; Xue, X. Quantitative gait dysfunction and risk of cognitive decline and dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; Robbins, M.; Holtzer, R.; Zimmerman, M.; Wang, C.; Xue, X.; Lipton, R.B. Gait Dysfunction in Mild Cognitive Impairment Syndromes. J. Am. Geriatr. Soc. 2008, 56, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Holtzer, R.; Friedman, R.; Lipton, R.B.; Katz, M.; Xue, X.; Verghese, J. The relationship between specific cognitive functions and falls in aging. Neuropsychology 2007, 21, 540–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausdorff, J.M.; Yogev, G. Cognitive Function May Be Important for Fall Injury Prevention Trials. J. Am. Geriatr. Soc. 2006, 54, 865, Author Reply 2006, 54, 865–866. [Google Scholar] [CrossRef] [PubMed]
- Tolle, K.A.; Rahman-Filipiak, A.M.; Hale, A.C.; Andren, K.A.K.; Spencer, R.J. Grooved Pegboard Test as a measure of executive functioning. Appl. Neuropsychol. Adult 2019, 27, 414–420. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 339) | No-Diabetes (n = 277) | Diabetes (n = 62) | or F Value | * p-Value | ||
|---|---|---|---|---|---|---|---|
| % Female | 52 | 53 | 45 | 1.39 | 0.24 | ||
| % Caucasian | 74 | 77 | 61 | 6.42 | 0.01 | ||
| % Moderate visual impairment | 28 | 25 | 39 | 4.57 | 0.03 | ||
| % Neuropathy | 5 | 3 | 15 | 14.38 | <0.01 | ||
| Age (years) | 76.59 (6.21) 65–93 | 76.71 (6.29) 65–93 | 76.05 (5.85) 67–92 | 0.62 | 0.43 | ||
| Education (years) | 14.97 (2.89) 5–21 | 15.05 (2.85) 5–21 | 14.63 (3.09) 7–21 | 0.51 | 0.33 | ||
| GHS Total score (0–8) | 1.29 (0.97) 0–5 | 1.27 (1.00) 0–5 | 1.35 (0.85) 0–3 | 2.10 | 0.50 | ||
| Glucose ~ | 110.96 (40.17) 68–385 | 101.54 (20.99) 68–183 | 154.64 (69.38) 73–385 | 75.00 | <0.01 | ||
| VS integration # | 0.04 (0.12) −0.33–0.34 | 0.05 (0.12) −0.32–0.34 | 0.00 (0.10) −0.33–0.22 | 7.26 | <0.01 | ||
| Overall RT (ms) | 400.25 (106.10) 243–954 | 397.26 (104.47) 243–945 | 413.60 (113.02) 262–954 | 0.47 | 0.30 | ||
| Somatosensory RT (ms) | 437.98 (113.05) 252–961 | 435.64 (113.66) 252–905 | 448.42 (110.57) 274–961 | 0.16 | 0.42 | ||
| Visual RT (ms) | 402.20 (113.77) 233–1050 | 399.03 (110.98) 233–1050 | 416.36 (125.44) 250–924 | 2.66 | 0.32 | ||
| VS RT (ms) | 361.70 (106.35) 213–1019 | 358.18 (103.98) 213–1019 | 377.38 (115.94) 244–975 | 0.71 | 0.23 | ||
| Unipedal stance Time (s) | 14.70 (11.09) 0–30 | 15.67 (11.28) 0–30 | 10.47 (9.12) 0–30 | 20.80 | <0.01 | ||
| PACE |  | Velocity (cm/s) | 99.82 (21.49) 49–167 | 101.19 (21.51) 49–167 | 93.70 (20.47) 49–139 | 0.77 | 0.01 |
| Stride length (cm) | 116.61 (19.02) 64–165 | 117.98 (18.65) 66–165 | 110.50 (19.59) 64–158 | 0.75 | <0.01 | ||
| Double support (%) | 31.61 (4.95) 18–49 | 31.26 (4.89) 18–48 | 33.19 (4.95) 24–49 | 0.17 | <0.01 | ||
| Model | B | S.E. | Wald | df | Sig. | Exp (B) | 95% CI for Exp (B) | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| VS Integration | −3.21 | 1.31 | 5.98 | 1.00 | 0.01 | 0.04 | 0.00 | 0.53 |
| Overall RT | 0.00 | 0.00 | 0.03 | 1.00 | 0.87 | 1.00 | 1.00 | 1.00 |
| Age | −0.03 | 0.03 | 1.27 | 1.00 | 0.26 | 0.97 | 0.92 | 1.02 |
| Gender | 0.54 | 0.32 | 2.85 | 1.00 | 0.09 | 1.72 | 0.92 | 3.24 |
| Education Level (years) | −0.03 | 0.06 | 0.36 | 1.00 | 0.55 | 0.97 | 0.87 | 1.08 |
| Ethnicity | −0.84 | 0.34 | 6.28 | 1.00 | 0.01 | 0.43 | 0.22 | 0.83 |
| GHS Score # | 0.01 | 0.16 | 0.00 | 1.00 | 0.97 | 1.01 | 0.74 | 1.37 |
| Visual Impairment | −0.69 | 0.33 | 4.45 | 1.00 | 0.04 | 0.50 | 0.26 | 0.95 |
| Neuropathy | −1.91 | 0.55 | 12.25 | 1.00 | 0.00 | 0.15 | 0.05 | 0.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahoney, J.R.; Verghese, J.; George, C. The Influence of Diabetes on Multisensory Integration and Mobility in Aging. Brain Sci. 2021, 11, 285. https://doi.org/10.3390/brainsci11030285
Mahoney JR, Verghese J, George C. The Influence of Diabetes on Multisensory Integration and Mobility in Aging. Brain Sciences. 2021; 11(3):285. https://doi.org/10.3390/brainsci11030285
Chicago/Turabian StyleMahoney, Jeannette R., Joe Verghese, and Claudene George. 2021. "The Influence of Diabetes on Multisensory Integration and Mobility in Aging" Brain Sciences 11, no. 3: 285. https://doi.org/10.3390/brainsci11030285
APA StyleMahoney, J. R., Verghese, J., & George, C. (2021). The Influence of Diabetes on Multisensory Integration and Mobility in Aging. Brain Sciences, 11(3), 285. https://doi.org/10.3390/brainsci11030285