
Treatment, Outcome, and Relapse of Spontaneous and Nonspontaneous Cerebrospinal Fluid Leak

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khurana, R.K. Intracranial hypotension. Semin. Neurol. 1996, 16, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Wang, Y.-F.; Fuh, J.-L.; Lirng, J.-F.; Chen, S.-P.; Hseu, S.-S.; Wu, J.-C.; Wang, S.-J. Cerebrospinal fluid leakage and headache after lumbar puncture: A prospective non-invasive imaging study. Brain 2015, 138, 1492–1498. [Google Scholar] [CrossRef] [Green Version]
- Mehta, G.; Oldfield, E.H. Prevention of intraoperative cerebrospinal fluid leaks by lumbar cerebrospinal fluid drainage during surgery for pituitary macroadenomas. J. Neurosurg. 2012, 116, 1299–1303. [Google Scholar] [CrossRef]
- Selesnick, S.H.; Liu, J.; Jen, A.; Newman, J. The Incidence of Cerebrospinal Fluid Leak after Vestibular Schwannoma Surgery. Otol. Neurotol. 2004, 25, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Hannallah, D.; Lee, J.; Khan, M.; Donaldson, W.F.; Kang, J.D. Cerebrospinal Fluid Leaks Following Cervical Spine Surgery. J. Bone Jt. Surg. 2008, 90, 1101–1105. [Google Scholar] [CrossRef] [Green Version]
- Heiler, U.P.T.; Ruf, M. Iatrogenic Intracranial Hypotension after Surgery of Adolescent Idiopathic Scoliosis due to a Misplaced Screw within the Thoracic Thecal Sac. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2021. [Google Scholar] [CrossRef]
- Menon, S.K.; Onyia, C.U. A short review on a complication of lumbar spine surgery: CSF leak. Clin. Neurol. Neurosurg. 2015, 139, 248–251. [Google Scholar] [CrossRef]
- Soyka, M.B.; Annen, A.; Holzmann, D. Where endoscopy fails: Indications and experience with the frontal sinus fat obliteration. Rhinology 2009, 47, 136–140. [Google Scholar]
- Sun, M.; Zuo, D.; Wang, H.; Sheng, J.; Ma, X.; Wang, C.; Zan, P.; Hua, Y.; Sun, W.; Cai, Z. Surgical Treatment of Sacral Meta-static Tumors. Front. Oncol. 2021, 11, 640933. [Google Scholar] [CrossRef]
- Kranz, P.G.; Gray, L.; Malinzak, M.D.; Amrhein, T.J. Spontaneous Intracranial Hypotension: Pathogenesis, Diagnosis, and Treatment. Neuroimaging Clin. N. Am. 2019, 29, 581–594. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.M.; Chodakiewitz, Y.G.; Maya, M.M.; Schievink, W.I.; Moser, F.G. Intracranial Hypotension and Cerebrospinal Fluid Leak. Neuroimaging Clin. N. Am. 2019, 29, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W.I. Spontaneous Spinal Cerebrospinal Fluid Leaks. Cephalalgia 2008, 28, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Guerin, P.; El Fegoun, A.B.; Obeid, I.; Gille, O.; Lelong, L.; Luc, S.; Bourghli, A.; Cursolle, J.C.; Pointillart, V.; Vital, J.M. Incidental durotomy during spine surgery: Incidence, management and complications. A retrospective review. Injury 2012, 43, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.P.; Shih, P.; Smith, T.R.; Slimack, N.P.; Dahdaleh, N.S.; Aoun, S.G.; El Ahmadieh, T.Y.; Smith, Z.A.; Scheer, J.K.; Koski, T.R.; et al. Comparison of Symptomatic Cerebral Spinal Fluid Leak between Patients Undergoing Minimally Invasive versus Open Lumbar Foraminotomy, Discectomy, or Laminectomy. World Neurosurg. 2014, 81, 634–640. [Google Scholar] [CrossRef]
- Liu, W.-C.; Choi, G.; Lee, S.-H.; Kwon, A.M.; Kim, K.H.; Park, J.; Park, H.S. Epidural Fluid Collection After Percutaneous Endoscopic Lumbar Discectomy. World Neurosurg. 2018, 111, e756–e763. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Bohlman, H.H.; Riew, K.D. Dural Tears Secondary to Operations on the Lumbar Spine. Management and Results after a Two-Year-Minimum Follow-up of Eighty-eight Patients*. J. Bone Jt. Surg. 1998, 80, 1728–1732. [Google Scholar] [CrossRef]
- Patel, M.R.; Louie, W.; Rachlin, J. Postoperative cerebrospinal fluid leaks of the lumbosacral spine: Management with percutaneous fibrin glue. AJNR Am. J. Neuroradiol. 1996, 17, 495–500. [Google Scholar]
- Ishimoto, Y.; Kawakami, M.; Curtis, E.; Cooper, C.; Moriguchi, N.; Nakao, S.-I.; Nakagawa, Y. The New Strategy for the Treatment of Cerebrospinal Fluid Leak Following Lumbar Surgery. Spine Surg. Relat. Res. 2020, 4, 95–98. [Google Scholar] [CrossRef] [Green Version]
- Schievink, W.I.; Schwartz, M.S.; Maya, M.M.; Moser, F.G.; Rozen, T.D. Lack of causal association between spontaneous intracranial hypotension and cranial cerebrospinal fluid leaks. J. Neurosurg. 2012, 116, 749–754. [Google Scholar] [CrossRef]
- Tam, E.K.; Gilbert, A.L. Spontaneous cerebrospinal fluid leak and idiopathic intracranial hypertension. Curr. Opin. Ophthalmol. 2019, 30, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Schievink, W.I. Spontaneous Spinal Cerebrospinal Fluid Leaks and Intracranial Hypotension. JAMA 2006, 295, 2286–2296. [Google Scholar] [CrossRef] [PubMed]
- Perthen, J.E.; Dorman, P.J.; Morland, D.; Redfern, N.; Butteriss, D.J. Treatment of spontaneous intracranial hypotension: Experiences in a UK regional neurosciences Centre. Clin. Med. 2021, 21, e247–e251. [Google Scholar] [CrossRef]
- Wu, J.-W.; Hseu, S.-S.; Fuh, J.-L.; Lirng, J.-F.; Wang, Y.-F.; Chen, W.-T.; Chen, S.-P.; Wang, S.-J. Factors predicting response to the first epidural blood patch in spontaneous intracranial hypotension. Brain 2016, 140, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Davidson, B.; Nassiri, F.; Mansouri, A.; Badhiwala, J.H.; Witiw, C.D.; Shamji, M.F.; Peng, P.W.; Farb, R.I.; Bernstein, M. Spontaneous Intracranial Hypotension: A Review and Introduction of an Algorithm For Management. World Neurosurg. 2017, 101, 343–349. [Google Scholar] [CrossRef]
- Umana, G.E.; Pucci, R.; Palmisciano, P.; Cassoni, A.; Ricciardi, L.; Tomasi, S.O.; Strigari, L.; Scalia, G.; Valentini, V. Cerebro-spinal Fluid Leaks Following Anterior Skull Base Trauma: A Systematic Review of the Literature. World Neurosurg. 2021, 83, P016. [Google Scholar]
- Zhang, F.; Zeng, T.; Gao, L.; Cui, D.-M.; Wang, K.; Xu, Z.-J.; Cao, X.-Y. Treatment of traumatic cerebrospinal fluid rhinorrhea via extended extradural anterior skull base approach. Chin. J. Traumatol. (Engl. Ed.) 2021, 24, 280–285. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Spontaneous | Nonspontaneous | p-Value | |
|---|---|---|---|
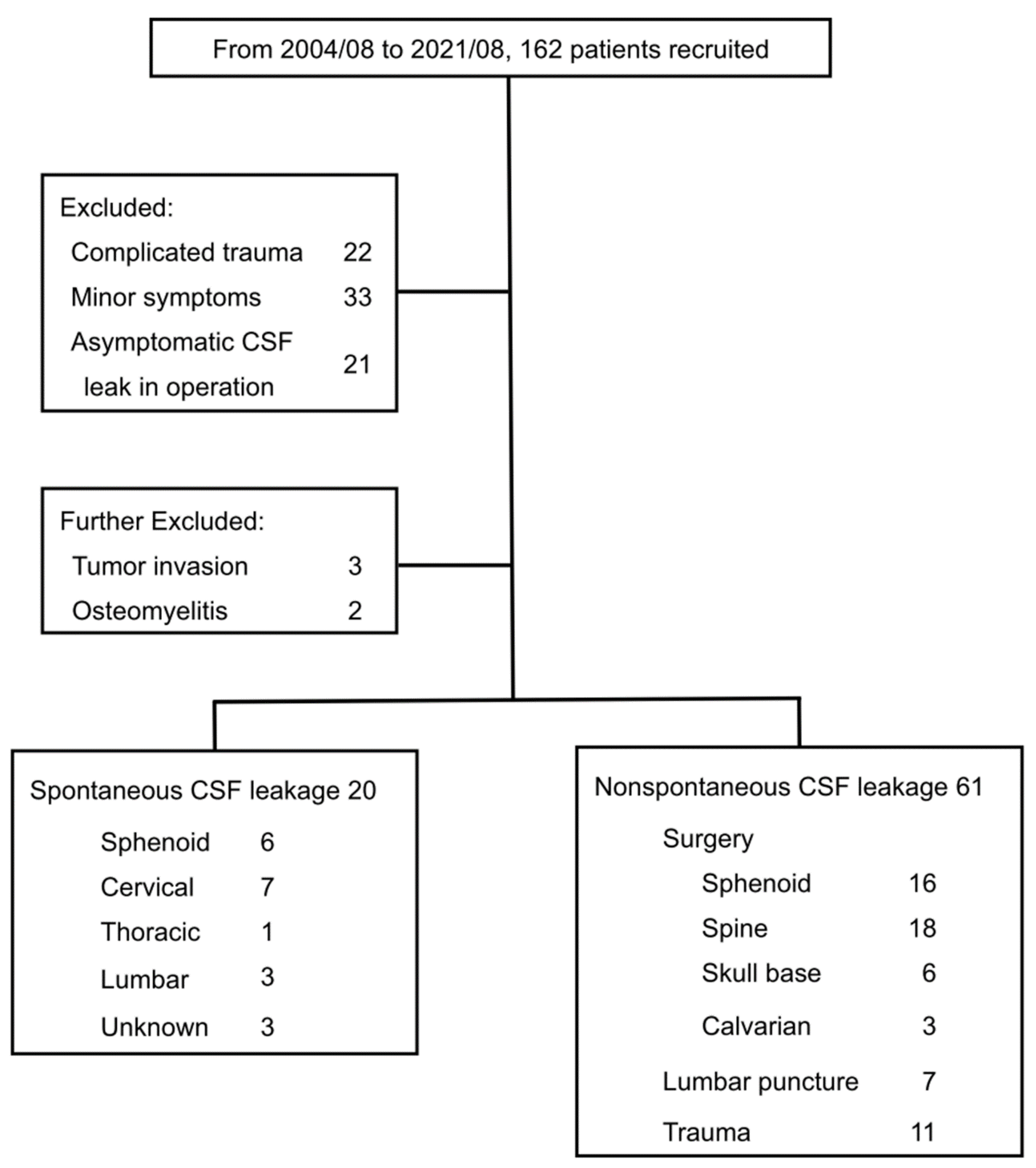
| Patient number | 20 | 61 | |
| Age | 43.6 ± 9.2 | 43.1 ± 15.2 | 0.888 |
| Gender (M:F) | 6:14 | 31:30 | 0.105 |
| Onset duration (days) | 8.9 ± 9.4 | 3.6 ± 4.7 | 0.033 |
| Headache as the first symptom | 14 (70%) | 29 (47.5%) | 0.081 |
| Headache pain score | 5.4 ± 2.4 | 4.3 ± 2.1 | 0.093 |
| Meningitis | 2 (10%) | 10 (16.4%) | 0.721 |
| MRI of CSF accumulation | 16 (80%) | 31 (51%) | 0.035 |
| Management | |||
| Conservative | 8 (40%) | 21 (34.4%) | 0.652 |
| Blood patch | 7 (35%) | 2 (3.2%) | <0.001 |
| Surgery | 5 (25%) | 38 (62.4%) | 0.047 |
| Conservative treatment duration (days) | 6.5 ± 4.5 | 11.6 ± 18.1 | 0.048 |
| Hospitalization (days) | 10.6 ± 4.2 | 13.7 ± 13.2 | 0.109 |
| Recurrence | 8 (40%) | 13 (21.3%) | 0.098 |
| Days before recurrence | 58.9 ± 87.0 | 34.5 ± 38.4 | 0.517 |
| Recurrence management Supportive | 3 | 2 | 0.325 |
| Blood patch | 3 | 0 | 0.042 |
| Surgery | 2 | 11 | 0.018 |
| Recurrence management duration (days) | 9.4 ± 3.0 | 17.5 ± 9.3 | 0.02 |
| 3rd recurrence | 1 (5%) | 1 (1.6%) | 1 |
| Nonspontaneous CSF Leak | |||||||
|---|---|---|---|---|---|---|---|
| Sphenoid Surgery | Spine Surgery | Skull Base Surgery | Calvarial Surgery | Lumbar Puncture | Trauma | p Value | |
| Patient number | 16 | 18 | 6 | 3 | 7 | 11 | |
| Open procedure | 10 (62.5%) | 15 (83.3%) | 6 (100%) | 3 (100%) | N/A | N/A | 0.229 |
| Number of operations | 1 ± 0 | 1.1 ± 0.2 | 1.2 ± 0.4 | 3.7 ± 0.9 | 1 | N/A | <0.001 |
| From last procedure to symptom onset (days) | 13 ± 20.7 | 18.6 ± 18.3 | 31.2 ± 37.8 | 201 ± 196 | 1.7 ± 0.8 | N/A | <0.001 |
| Symptom onset duration (days) | 2 ± 2.3 | 6.6 ± 6.5 | 3.7 ± 4.6 | 4.7 ± 3.9 | 1.9 ± 0.8 | 2 ± 1.7 | 0.048 |
| Headache: rhinorrhea | 6:10 | 11:0 1 | 1:4 2 | 1:0 3 | 7:0 | 3:8 | 6/15 5 |
| Headache VAS | 2.2 ± 2.4 | 5.9 ± 1.5 | 0.75 ± 1.3 | 0 | 2.6 ± 0.7 | 2.3 ± 0.5 | <0.001 4 |
| Meningitis | 5 (31.25%) | 0 | 2 (33.3%) | 1 (33.3%) | 0 | 2 (18.2%) | 1/15 5 |
| Treatment | |||||||
| Conservative | 4 (25%) | 8 (44.4%) | 1 (16.7%) | 1 (33.3%) | 5 (71.4%) | 2 (18.2%) | 1/15 5 |
| Surgery | 12 (75%) | 10 (55.6%) | 5 (83.3%) | 2 (66.7%) | 0 | 9 (81.8%) | 4/15 5 |
| Blood patch | 0 | 0 | 0 | 0 | 2 (28.6%) | 0 | 1/15 5 |
| Conservative treatment duration (days) | 9 ± 10.4 | 11.3 ± 14.8 | 4.2 ± 3.2 | 11.3 ± 5.7 | 4 ± 2.9 | 24.7 ± 31.6 | 0.131 |
| Hospitalization days | 21.9 ± 25.2 | 14.5 ± 18.5 | 10.3 ± 4.2 | 21 ± 7.3 | 4.6 ± 3.1 | 14.9 ± 7.9 | 0.372 |
| MRI with CSF accumulation | 6 (18.75%) | 15 (83.3%) | 0 | 0 | 0 | 6 (54.5%) | 5/15 5 |
| Recurrence | 3 (18.75%) | 6 (33.3%) | 0 | 0 | 0 | 4 (36.4%) | 0/15 5 |
| Days before recurrence | 23 ± 22.0 | 20.3 ± 14.9 | N/A | N/A | N/A | 67.5 ± 51.2 | 0.157 |
| Recurrence management | 0.692 | ||||||
| Conservative | 1 (33.3%) | 1 (16.7%) | N/A | N/A | N/A | 0 | |
| Surgery | 2 (66.7%) | 5 (83.3%) | N/A | N/A | N/A | 4 (100%) | |
| Recurrence management duration (days) | 30.3 ± 5.6 | 10.2 ± 1.6 | N/A | N/A | N/A | 16.8 ± 6.4 | 0.002 |
| Spontaneous CSF Leak | |||||||
|---|---|---|---|---|---|---|---|
| Sphenoid | Spinal | Unknown | p Value * | ||||
| Cervical | Thoracic | Lumbar | Total | ||||
| Patient number | 6 | 7 | 1 | 3 | 11 | 3 | |
| Symptom onset (days) | 17 ± 11.1 | 3.3 ± 2.8 | 4 | 3 ± 1 | 3.3 ± 2.4 | 14 ± 5.1 | |
| Headache: rhinorrhea | 0:6 | 7:0 | 1:0 | 3:0 | 11:0 | 3:0 | <0.001 |
| Headache VAS | N/A | 5.1 ± 2 | 3 | 5.3 ± 3.4 | 5 ± 2.5 | 7 ± 0.8 | |
| Meningitis | 2 (33.3%) | 0 | 0 | 0 | 0 | 0 | 0.5 |
| Treatment | |||||||
| Conservative | 1 (16.7%) | 3 (42.9%) | 0 | 1 (33.3%) | 4 (36.4%) | 3 (100%) | 0.6 |
| Nonconservative | 5 (83.3%) | 4 (57.1%) | 1 (100%) | 2 (66.7%) | 7 (63.6%) | 0 | |
| Conservative treatment duration (days) | 5.6 ± 5.1 | 7.6 ± 5 | 13 | 5.3 ± 1.9 | 6.7 ± 4.3 | 7.3 ± 2.6 | |
| Hospitalization days | 12.8 ± 3.9 | 9.4 ± 4.4 | 13 | 11 ± 2.2 | 10.2 ± 3.9 | 7.3 ± 2.6 | |
| MRI with intracranial hypotension | 6 (100%) | 6 (85.7%) | 1 (100%) | 3 (100%) | 10 (91%) | 1 (33.3%) | 1 |
| MRI with CSF accumulation | 6 (100%) | 6 (85.7%) | 1 (100%) | 3 (100%) | 10 (91%) | 0 | 1 |
| Recurrence | 3 | 2 | 0 | 2 | 4 (36.3%) | 1 | 0.80 |
| Days before recurrence | 128 ± 112 | 22.5 ± 15.3 | 0 | 3 | 12 ± 15.2 | 30 | |
| Recurrence management Conservative | 1 | 1 | 0 | 0 | 1 | 1 | 0.786 |
| Blood patch | 0 | 1 | 0 | 2 | 3 | 0 | 0.125 |
| Surgery | 2 | 0 | 0 | 0 | 0 | 0 | 0.429 |
| Recurrence management duration (days) | 9 ± 0 | 9.5 ± 5.6 | 0 | 15 | 8.5 ± 5.7 | 5 | |
| 3rd recurrence | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tai, Y.-C.; Tai, Y.-S.; Ou, C.-H.; Lui, C.-C.; Wang, H.-K.; Kuo, H.-C.; Hsu, S.-P. Treatment, Outcome, and Relapse of Spontaneous and Nonspontaneous Cerebrospinal Fluid Leak. Brain Sci. 2022, 12, 340. https://doi.org/10.3390/brainsci12030340
Tai Y-C, Tai Y-S, Ou C-H, Lui C-C, Wang H-K, Kuo H-C, Hsu S-P. Treatment, Outcome, and Relapse of Spontaneous and Nonspontaneous Cerebrospinal Fluid Leak. Brain Sciences. 2022; 12(3):340. https://doi.org/10.3390/brainsci12030340
Chicago/Turabian StyleTai, Yi-Cheng, Yi-Sheng Tai, Chang-Hsien Ou, Chun-Chung Lui, Hao-Kuang Wang, Hung-Chang Kuo, and Shih-Pin Hsu. 2022. "Treatment, Outcome, and Relapse of Spontaneous and Nonspontaneous Cerebrospinal Fluid Leak" Brain Sciences 12, no. 3: 340. https://doi.org/10.3390/brainsci12030340
APA StyleTai, Y. -C., Tai, Y. -S., Ou, C. -H., Lui, C. -C., Wang, H. -K., Kuo, H. -C., & Hsu, S. -P. (2022). Treatment, Outcome, and Relapse of Spontaneous and Nonspontaneous Cerebrospinal Fluid Leak. Brain Sciences, 12(3), 340. https://doi.org/10.3390/brainsci12030340