

Effects of Resistance Exercise on Slow-Twitch Soleus Muscle of Infarcted Rats

 , , ,
, , , 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Groups
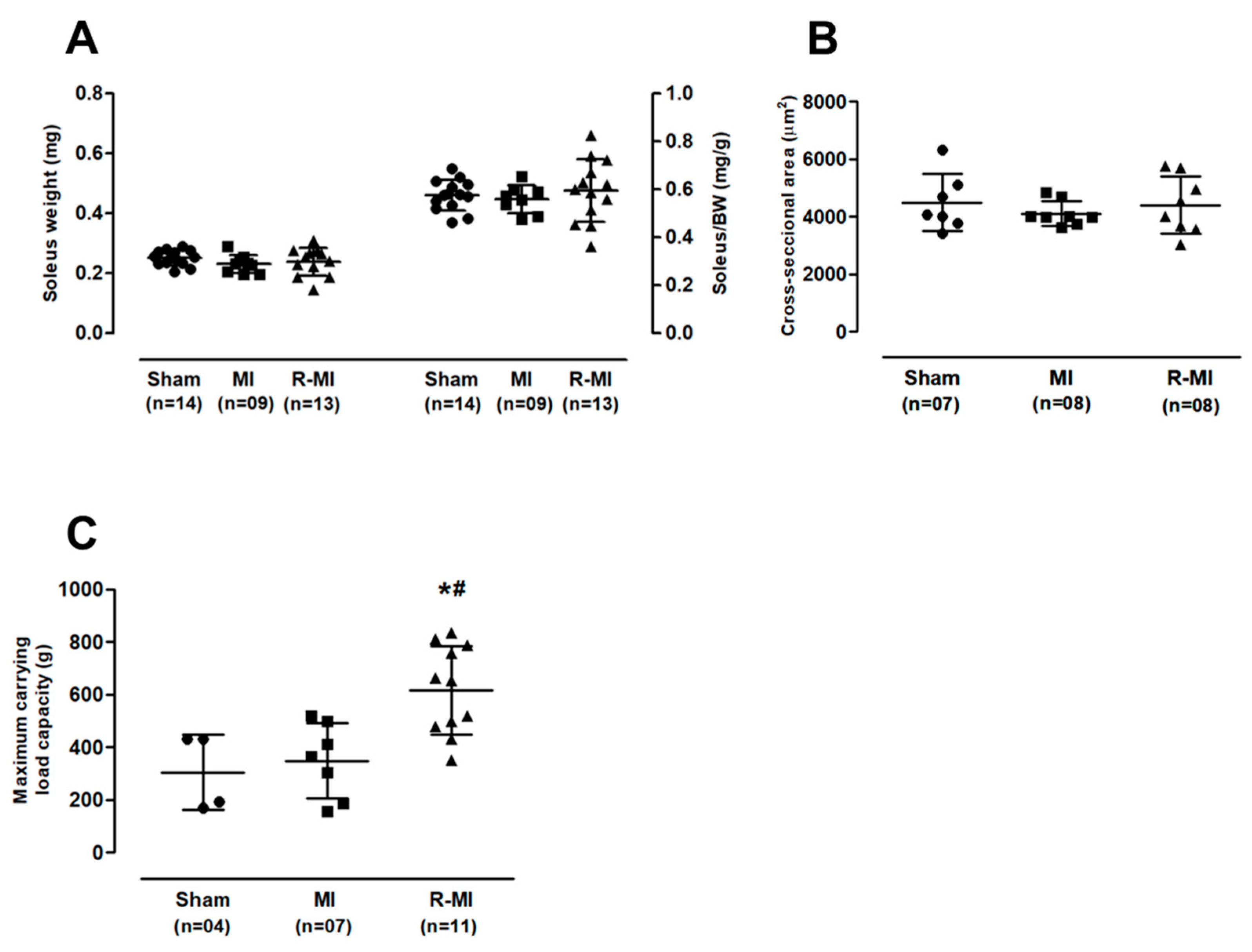
2.2. Maximum Carrying Load Test
2.3. Resistance Exercise Training
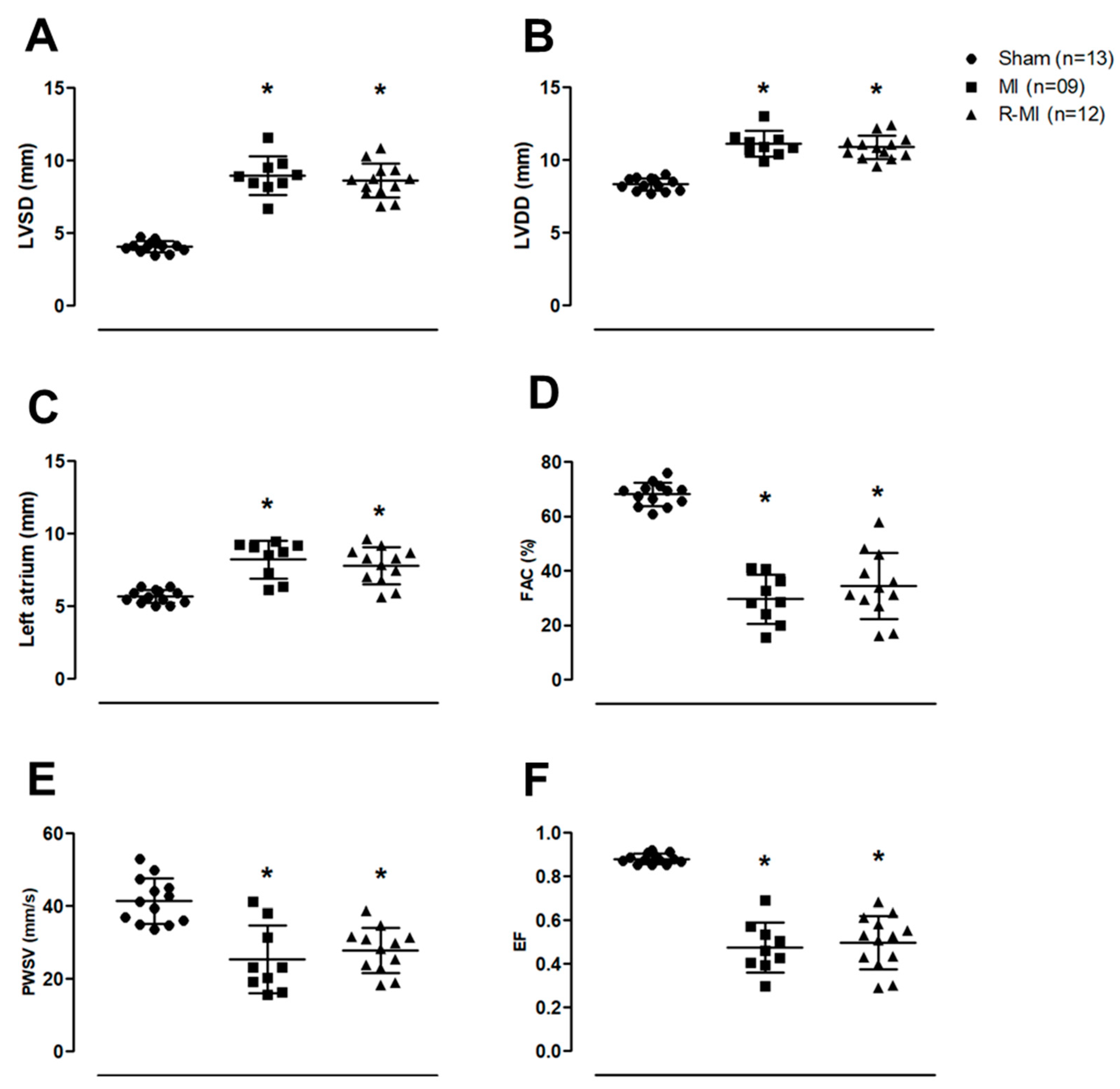
2.4. Echocardiographic Evaluation
2.5. Collection of Skeletal Muscle and Other Tissues
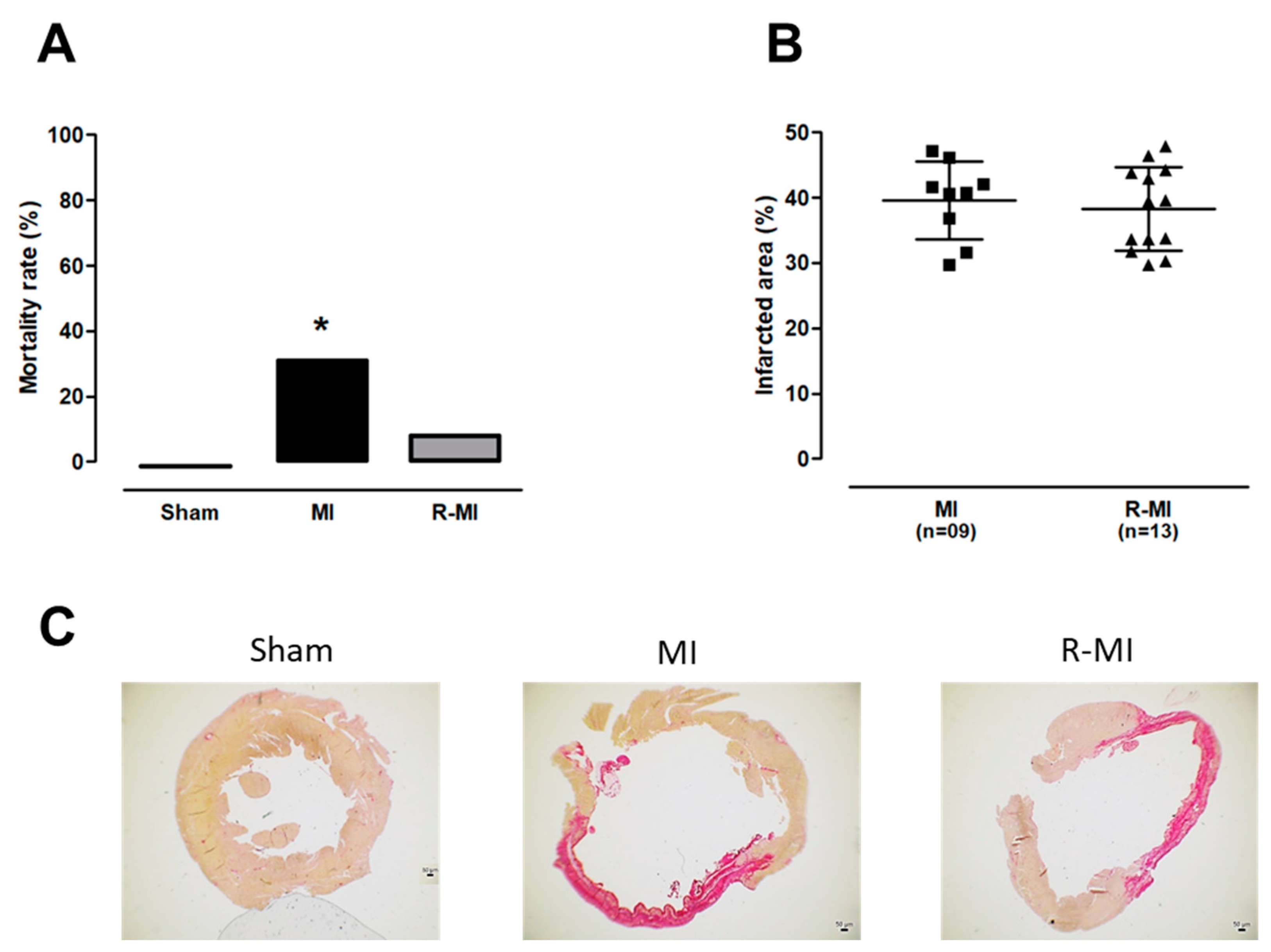
2.6. Infarct Size
2.7. Skeletal Muscle Morphology
2.8. Antioxidant Enzyme Activity and Lipid Hydroperoxide Concentration
2.9. Assessment of Energy Metabolism
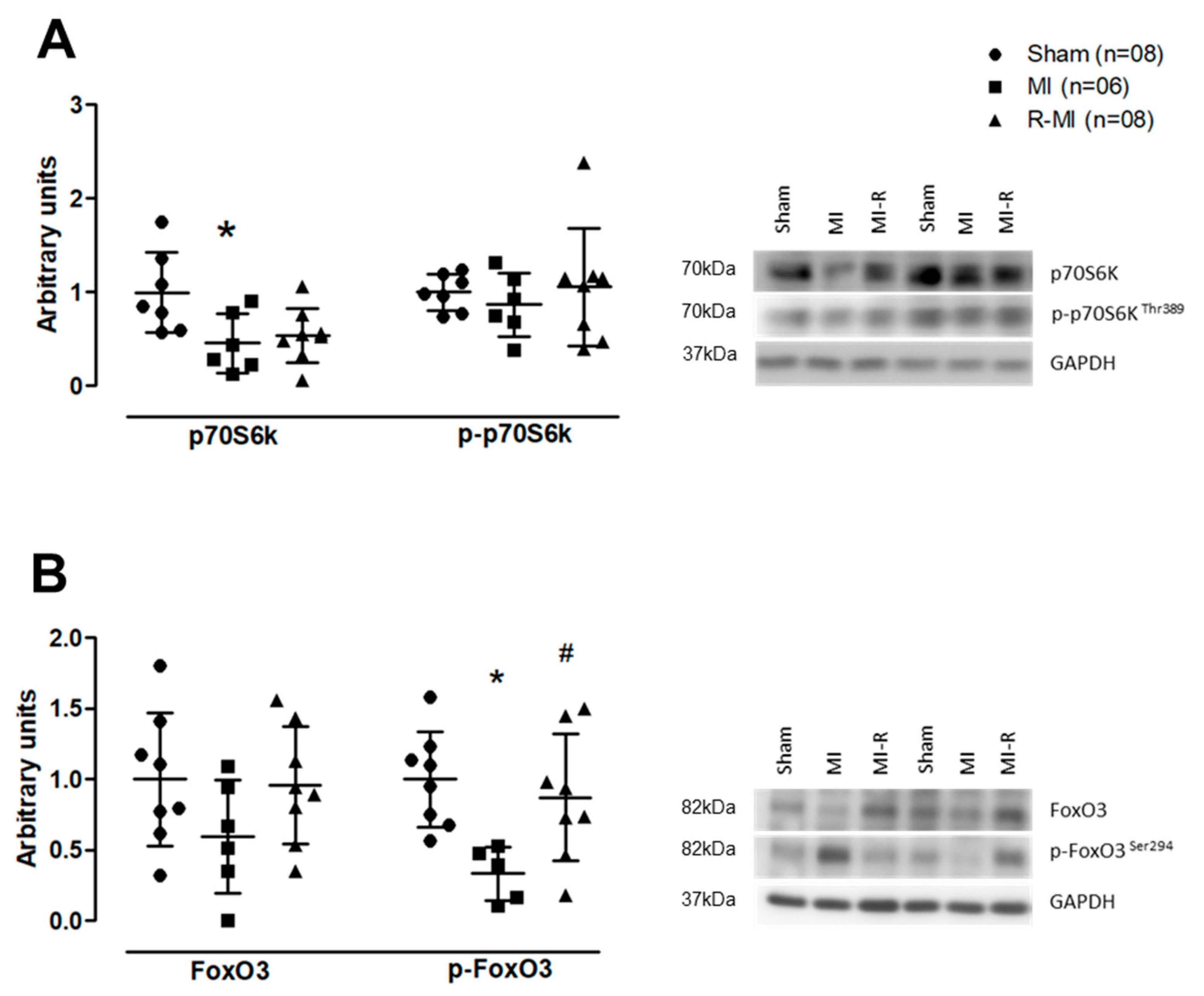
2.10. Protein Expression
2.11. Statistical Analysis
3. Results
3.1. Resistance Exercise Does Not Change Cardiac Remodeling and Ventricular Function in Infarcted Rats
3.2. Resistance Exercise Preserves Pathways Involved in Skeletal Muscle Protein Turnover
3.3. Resistance Exercise Modulates Antioxidant Activity and Glycolytic Metabolism in Soleus Muscle of Infarcted Rats
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics-2022 Update: A Report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [PubMed]
- Jenča, D.; Melenovský, V.; Stehlik, J.; Staněk, V.; Kettner, J.; Kautzner, J.; Adámková, V.; Wohlfahrt, P. Heart failure after myocardial infarction: Incidence and predictors. ESC Heart Fail. 2021, 8, 222–237. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Mendoza, D.P.; Lara-Ribeiro, A.C.; Verano-Braga, T. Pathological cardiac remodeling seen by the eyes of proteomics. Biochim. Biophys. Acta Proteins Proteom. 2021, 1869, 140622. [Google Scholar] [CrossRef] [PubMed]
- Cohn, J.N.; Ferrari, R.; Sharpe, N. Cardiac remodeling—Concepts and clinical implications: A consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J. Am. Coll. Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef] [Green Version]
- Del Buono, M.G.; Arena, R.; Borlaug, B.A.; Carbone, S.; Canada, J.M.; Kirkman, D.L.; Garten, R.; Rodriguez-Miguelez, P.; Guazzi, M.; Lavie, C.J.; et al. Exercise intolerance in patients with heart failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2209–2225. [Google Scholar] [CrossRef] [PubMed]
- Von Haehling, S. The wasting continuum in heart failure: From sarcopenia to cachexia. Proc. Nutr. Soc. 2015, 74, 367–377. [Google Scholar] [CrossRef]
- Damatto, R.L.; Lima, A.R.R.; Martinez, P.F.; Cezar, M.D.M.; Okoshi, K.; Okoshi, M.P. Myocardial myostatin in spontaneously hypertensive rats with heart failure. Int. J. Cardiol. 2016, 215, 384–387. [Google Scholar] [CrossRef] [Green Version]
- Garnier, A.; Fortin, D.; Zoll, J.; N’Guessan, B.; Mettauer, B.; Lampert, E.; Veksler, V.; Ventura-Clapier, R. Coordinated changes in mitochondrial function and biogenesis in healthy and diseased human skeletal muscle. FASEB J. 2005, 19, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Tsuda, M.; Fukushima, A.; Matsumoto, J.; Takada, S.; Kakutani, N.; Nambu, H.; Yamanashi, K.; Furihata, T.; Yokota, T.; Okita, K.; et al. Protein acetylation in skeletal muscle mitochondria is involved in impaired fatty acid oxidation and exercise intolerance in heart failure. J. Cachexia Sarcopenia Muscle 2018, 9, 844–859. [Google Scholar] [CrossRef]
- Cunha, T.F.; Bechara, L.R.G.; Bacurau, A.V.N.; Jannig, P.R.; Voltarelli, V.A.; Dourado, P.M.; Vasconcelos, A.R.; Scavone, C.; Ferreira, J.C.; Brum, P.C. Exercise training decreases NADPH oxidase activity and restores skeletal muscle mass in heart failure rats. J. Appl. Physiol. 2017, 122, 817–827. [Google Scholar] [CrossRef] [Green Version]
- Petretta, M.; Colao, A.; Sardu, C.; Scopacasa, F.; Marzullo, P.; Pivonello, R.; Fontanella, L.; de Caterina, M.; de Simone, A.; Bonaduce, D. NT-proBNP, IGF-I and survival in patients with chronic heart failure. Growth Horm. IGF Res. 2007, 17, 288–296. [Google Scholar] [CrossRef]
- Niebauer, J.; Pflaum, C.D.; Clark, A.L.; Strasburger, C.J.; Hooper, J.; Poole-Wilson, P.A.; Coats, A.J.; Anker, S.D. Deficient insulin-like growth factor I in chronic heart failure predicts altered body composition, anabolic deficiency, cytokine and neurohormonal activation. J. Am. Coll. Cardiol. 1998, 32, 393–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, P.F.; Bonomo, C.; Guizoni, D.M.; Junior, S.A.O.; Damatto, R.L.; Cezar, M.D.M.; Lima, A.R.R.; Pagan, L.U.; Seiva, F.R.; Fernandes, D.C.; et al. Influence of N-acetylcysteine on oxidative stress in slow-twitch soleus muscle of heart failure rats. Cell. Physiol. Biochem. 2015, 35, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Kinugawa, S.; Matsushima, S. Oxidative stress and heart failure. Am. J. Physiol. Circ. Physiol. 2011, 301, H2181–H2190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, R.F.; Dariolli, R.; Justulin Junior, L.A.; Sugizaki, M.M.; Okoshi, M.P.; Cicogna, A.C.; Felisbino, S.L.; Dal Pai-Silva, M. Heart failure alters matrix metalloproteinase gene expression and activity in rat skeletal muscle. Int. J. Exp. Pathol. 2006, 87, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Gimenes, C.; Gimenes, R.; Rosa, C.M.; Xavier, N.P.; Campos, D.H.S.; Fernandes, A.A.H.; Cezar, M.D.M.; Guirado, G.N.; Cicogna, A.C.; Takamoto, A.H.; et al. Low intensity physical exercise attenuates cardiac remodeling and myocardial oxidative stress and dysfunction in diabetic rats. J. Diabetes Res. 2015, 2015, 457848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guizoni, D.M.; Oliveira-Junior, S.A.; Noor, S.L.R.; Pagan, L.U.; Martinez, P.F.; Lima, A.R.R.; Gomes, M.J.; Damatto, R.L.; Cezar, M.D.; Bonomo, C.; et al. Effects of late exercise on cardiac remodeling and myocardial calcium handling proteins in rats with moderate and large size myocardial infarction. Int. J. Cardiol. 2016, 221, 406–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagan, L.U.; Damatto, R.L.; Gomes, M.J.; Lima, A.R.R.; Cezar, M.D.M.; Damatto, F.C.; Reyes, D.R.A.; Caldonazo, T.M.M.; Polegato, B.F.; Okoshi, M.P.; et al. Low-intensity aerobic exercise improves cardiac remodelling of adult spontaneously hypertensive rats. J. Cell. Mol. Med. 2019, 23, 6504–6507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagan, L.U.; Gomes, M.J.; Damatto, R.L.; Lima, A.R.R.; Cezar, M.D.M.; Damatto, F.C.; Reyes, D.R.A.; Campos, D.H.S.; Caldonazo, T.M.M.; Polegato, B.F.; et al. Aerobic exercise during advance stage of uncontrolled arterial hypertension. Front. Physiol. 2021, 12, 675778. [Google Scholar] [CrossRef]
- Sullivan, M.; Higginbotham, M.; Coob, F. Exercise training in patients with severe left ventricular dysfunction. Hemodynamic and metabolic effects. Circulation 1988, 78, 506–515. [Google Scholar] [CrossRef] [Green Version]
- Palau, P.; Núñez, E.; Domínguez, E.; Sanchis, J.; Núñez, J. Physical therapy in heart failure with preserved ejection fraction: A systematic review. Eur. J. Prev. Cardiol. 2016, 23, 4–13. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.M.; Whellan, D.J.; Lee, K.L.; Keteyian, S.J.; Cooper, L.S.; Ellis, S.J.; Leifer, E.S.; Kraus, W.E.; Kitzman, D.W.; Blumenthal, J.A.; et al. Efficacy and safety of exercise training in patients with chronic heart failure. JAMA 2009, 301, 1439. [Google Scholar] [CrossRef] [PubMed]
- Collado-Mateo, D.; Lavín-Pérez, A.M.; Peñacoba, C.; Del Coso, J.; Leyton-Román, M.; Luque-Casado, A.; Gasque, P.; Fernández-Del-Olmo, M.Á.; Amado-Alonso, D. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: An umbrella review. Int. J. Environ. Res. Public Health 2021, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- Karlsdottir, A.E.; Foster, C.; Porcari, J.P.; Palmer-McLean, K.; White-Kube, R.; Backes, R.C. Hemodynamic responses during aerobic and resistance exercise. J. Cardiopulm. Rehabil. 2002, 22, 170–177. [Google Scholar] [CrossRef]
- Mandic, S.; Myers, J.; Selig, S.E.; Levinger, I. Resistance versus aerobic exercise training in chronic heart failure. Curr. Heart Fail. Rep. 2012, 9, 57–64. [Google Scholar] [CrossRef]
- Reyes, D.R.A.; Gomes, M.J.; Rosa, C.M.; Pagan, L.U.; Zanati, S.G.; Damatto, R.L.; Rodrigues, E.A.; Carvalho, R.F.; Fernandes, A.A.H.; Martinez, P.F.; et al. Exercise during transition from compensated left ventricular hypertrophy to heart failure in aortic stenosis rats. J. Cell. Mol. Med. 2019, 23, 1235–1245. [Google Scholar] [CrossRef] [Green Version]
- Fisher, S.; Smart, N.A.; Pearson, M.J. Resistance training in heart failure patients: A systematic review and meta-analysis. Heart Fail. Rev. 2021, 27, 1665–1682. [Google Scholar] [CrossRef]
- Lena, A.; Ebner, N.; Coats, A.J.S.; Anker, M.S. Cardiac cachexia: The mandate to increase clinician awareness. Curr. Opin. Support. Palliat. Care 2019, 13, 298–304. [Google Scholar] [CrossRef]
- Pu, C.T.; Johnson, M.T.; Forman, D.E.; Hausdorff, J.M.; Roubenoff, R.; Foldvari, M.; Fielding, R.A.; Singh, M.A. Randomized trial of progressive resistance training to counteract the myopathy of chronic heart failure. J. Appl. Physiol. 2001, 90, 2341–2350. [Google Scholar] [CrossRef] [Green Version]
- Levinger, I.; Bronks, R.; Cody, D.V.; Linton, I.; Davie, A. Resistance training for chronic heart failure patients on beta blocker medications. Int. J. Cardiol. 2005, 102, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Vezzoli, A.; Mrakic-Sposta, S.; Montorsi, M.; Porcelli, S.; Vago, P.; Cereda, F.; Longo, S.; Maggio, M.; Narici, M. Moderate Intensity Resistive Training Reduces Oxidative Stress and Improves Muscle Mass and Function in Older Individuals. Antioxidants 2019, 26, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: A scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef]
- Grans, C.F.; Feriani, D.J.; Abssamra, M.E.V.; Rocha, L.Y.; Carrozzi, N.M.; Mostarda, C.; Figueroa, D.M.; Angelis, K.D.; Irigoyen, M.C.; Rodrigues, B. Resistance training after myocardial infarction in rats: Its role on cardiac and autonomic function. Arq. Bras. Cardiol. 2014, 103, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Wang, Q.; Liu, Z.; Jia, D.; Feng, R.; Tian, Z. Effects of different types of exercise on skeletal muscle atrophy, antioxidant capacity and growth factors expression following myocardial infarction. Life Sci. 2018, 213, 40–49. [Google Scholar] [CrossRef]
- Gomes, M.J.; Pagan, L.U.; Lima, A.R.R.; Reyes, D.R.A.; Martinez, P.F.; Damatto, F.C.; Pontes, T.H.D.; Rodrigues, E.A.; Souza, L.M.; Tosta, I.F.; et al. Effects of aerobic and resistance exercise on cardiac remodelling and skeletal muscle oxidative stress of infarcted rats. J. Cell. Mol. Med. 2020, 24, 5352–5362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, P.F.; Okoshi, K.; Zornoff, L.A.M.; Carvalho, R.F.; Oliveira Junior, S.A.; Lima, A.R.R.; Campos, D.H.; Damatto, R.L.; Padovani, C.R.; Nogueira, C.R.; et al. Chronic heart failure-induced skeletal muscle atrophy, necrosis, and changes in myogenic regulatory factors. Med. Sci. Monit. 2010, 16, BR374–BR383. [Google Scholar]
- Cassilhas, R.C.; Reis, I.T.; Venâncio, D.; Fernandes, J.; Tufik, S.; De Mello, M.T. Animal model for progressive resistance exercise: A detailed description of model and its implications for basic research in exercise. Motriz. Rev. Educ. Fis. 2013, 19, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Hornberger, T.A.; Farrar, R.P. Physiological hypertrophy of the FHL muscle following 8 weeks of progressive resistance exercise in the rat. Can. J. Appl. Physiol. 2004, 29, 16–31. [Google Scholar] [CrossRef]
- Leite, R.D.; Durigan, R.D.C.M.; Lino, A.D.S.; Campos, M.V.S.; Souza, M.D.G.; Selistre-De-Araújo, H.S.; Bouskela, E.; Kraemer-Aguiar, L.G. Resistance training may concomitantly benefit body composition, blood pressure and muscle MMP-2 activity on the left ventricle of high-fat fed diet rats. Metabolism 2013, 62, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Cezar, M.D.M.; Damatto, R.L.; Martinez, P.F.; Lima, A.R.R.; Campos, D.H.S.; Rosa, C.M.; Guizoni, D.M.; Bonomo, C.; Cicogna, A.C.; Gimenes, R.; et al. Aldosterone blockade reduces mortality without changing cardiac remodeling in spontaneously hypertensive rats. Cell. Physiol. Biochem. 2013, 32, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Gimenes, R.; Gimenes, C.; Rosa, C.M.; Xavier, N.P.; Campos, D.H.S.; Fernandes, A.A.H.; Cezar, M.D.M.; Guirado, G.N.; Pagan, L.U.; Chaer, I.D.; et al. Influence of apocynin on cardiac remodeling in rats with streptozotocin-induced diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Okoshi, K.; Fioretto, J.R.; Okoshi, M.P.; Cicogna, A.C.; Aragon, F.F.; Matsubara, L.S.; Matsubara, B.B. Food restriction induces in vivo ventricular dysfunction in spontaneously hypertensive rats without impairment of in vitro myocardial contractility. Braz. J. Med. Biol. Res. 2004, 15, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okoshi, K.; Cezar, M.D.M.; Polin, M.A.M.; Paladino, J.R.; Martinez, P.F.; Oliveira, S.A.; Lima, A.R.R.; Damatto, R.L.; Paiva, S.A.R.; Zornoff, L.A.M.; et al. Influence of intermittent fasting on myocardial infarction-induced cardiac remodeling. BMC Cardiovasc. Disord. 2019, 19, 126. [Google Scholar] [CrossRef]
- Martinez, P.F.; Bonomo, C.; Guizoni, D.M.; Oliveira, S.A.; Damatto, R.L.; Cezar, M.D.M.; Lima, A.R.R.; Pagan, L.U.; Seiva, F.R.; Bueno, R.T.; et al. Modulation of MAPK and NF-κB signaling pathways by antioxidant therapy in skeletal muscle of heart failure rats. Cell. Physiol. Biochem. 2016, 39, 371–384. [Google Scholar] [CrossRef]
- Okoshi, M.P.; Matsubara, L.S.; Franco, M.; Cicogna, A.C.; Matsubara, B.B. Myocyte necrosis is the basis for fibrosis in renovascular hypertensive rats. Braz. J. Med. Biol. Res. 1997, 30, 1135–1144. [Google Scholar] [CrossRef] [Green Version]
- Reyes, D.R.A.; Gomes, M.J.; Rosa, C.M.; Pagan, L.U.; Damatto, F.C.; Damatto, R.L.; Depra, I.; Campos, D.H.S.; Fernandez, A.A.H.; Martinez, P.F.; et al. N-Acetylcysteine influence on oxidative stress and cardiac remodeling in rats during transition from compensated left ventricular hypertrophy to heart failure. Cell. Physiol. Biochem. 2017, 44, 2310–2321. [Google Scholar] [CrossRef]
- Gomes, M.J.; Martinez, P.F.; Campos, D.H.S.; Pagan, L.U.; Bonomo, C.; Lima, A.R.R.; Damatto, R.L.; Cezar, M.D.; Damatto, F.C.; Rosa, C.M.; et al. Beneficial effects of physical exercise on functional capacity and skeletal muscle oxidative stress in rats with aortic stenosis-induced heart failure. Oxid. Med. Cell. Longev. 2016, 2016, 8695716. [Google Scholar] [CrossRef] [Green Version]
- Alp, P.R.; Newsholme, E.A.; Zammit, V.A. Activities of citrate synthase and NAD+-linked and NADP+-linked isocitrate dehydrogenase in muscle from vertebrates and invertebrates. Biochem. J. 1976, 154, 689–700. [Google Scholar] [CrossRef] [Green Version]
- Zammit, V.A.; Beis, I.; Newsholme, E.A. Maximum activities and effects of fructose bisphosphate on pyruvate kinase from muscles of vertebrates and invertebrates in relation to the control of glycolysis. Biochem. J. 1978, 174, 989–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hengartner, H.; Harris, J.I. Purification by affinity chromatography; properties and crystallisation of phosphofructokinase from thermophilic micro-organisms. FEBS Lett. 1975, 55, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bieber, L.L.; Abraham, T.; Helmrath, T. A rapid spectrophotometric assay for carnitine palmitoyltransferase. Anal. Biochem. 1972, 50, 509–518. [Google Scholar] [CrossRef]
- Rosa, C.M.; Campos, D.H.S.; Reyes, D.R.A.; Damatto, F.C.; Kurosaki, L.Y.; Pagan, L.U.; Gomes, M.J.; Corrêa, C.R.; Fernandes, A.A.H.; Okoshi, M.P.; et al. Effects of the SGLT2 inhibition on Cardiac Remodeling in Streptozotocin-Induced Diabetic Rats, a Model of Type 1 Diabetes Mellitus. Antioxidants 2022, 11, 982. [Google Scholar] [CrossRef]
- Minicucci, M.F.; Azevedo, P.S.; Martinez, P.F.; Lima, A.R.R.; Bonomo, C.; Guizoni, D.M.; Polegato, B.F.; Okoshi, M.P.; Okoshi, K.; Matsubara, B.B.; et al. Critical infarct size to induce ventricular remodeling, cardiac dysfunction and heart failure in rats. Int. J. Cardiol. 2011, 151, 242–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, T.; Palus, S.; Springer, J. Skeletal muscle wasting in chronic heart failure. ESC Heart Fail. 2018, 5, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Von Haehling, S.; Macedo, T.G.; Valentova, M.; Anker, M.S.; Ebner, N.; Bekfani, T.; Haarmann, H.; Schefold, J.C.; Lainscak, M.; Cleland, J.G.F.; et al. Muscle wasting as an independent predictor of survival in patients with chronic heart failure. J. Cachexia Sarcopenia Muscle 2020, 11, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Trouwborst, I.; Clark, B.C. Skeletal muscle performance and ageing. J. Cachexia Sarcopenia Muscle 2018, 9, 3–19. [Google Scholar] [CrossRef]
- Kinugawa, S.; Takada, S.; Matsushima, S.; Okita, K.; Tsutsui, H. Skeletal muscle abnormalities in heart failure. Int. Heart J. 2015, 56, 475–484. [Google Scholar] [CrossRef] [Green Version]
- Rom, O.; Reznick, A.Z. The role of E3 ubiquitin-ligases MuRF-1 and MAFbx in loss of skeletal muscle mass. Free Radic. Biol. Med. 2016, 98, 218–230. [Google Scholar] [CrossRef]
- Stitt, T.N.; Drujan, D.; Clarke, B.A.; Panaro, F.; Timofeyva, Y.; Kline, W.O.; Gonzalez, M.; Yancopoulos, G.D.; Glass, D.J. The IGF-1/PI3K/Akt pathway prevents expression of muscle atrophy-induced ubiquitin ligases by inhibiting FoxO transcription factors. Mol. Cell 2004, 14, 395–403. [Google Scholar] [CrossRef]
- Ismaeel, A.; Holmes, M.; Papoutsi, E.; Panton, L.; Koutakis, P. Resistance training, antioxidant status, and antioxidant supplementation. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Miotto, P.M.; Steinberg, G.R.; Holloway, G.P. Controlling skeletal muscle CPT-I malonyl-CoA sensitivity: The importance of AMPK-independent regulation of intermediate filaments during exercise. Biochem. J. 2017, 474, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Mor, I.; Cheung, E.C.; Vousden, K.H. Control of glycolysis through regulation of PFK1: Old friends and recent additions. Cold Spring Harb. Symp. Quant. Biol. 2011, 76, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; McGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The Effects of exercise and physical activity on weight loss and maintenance. Prog. Cardiovasc. Dis. 2018, 61, 206–213. [Google Scholar] [CrossRef]
- Martinez, P.F.; Okoshi, K.; Zornoff, L.A.M.; Oliveira, S.A.; Campos, D.H.S.; Lima, A.R.R.; Damatto, R.L.; Cezar, M.D.; Bonomo, C.; Guizoni, D.M.; et al. Echocardiographic detection of congestive heart failure in postinfarction rats. J. Appl. Physiol. 2011, 111, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Okoshi, M.P.; Romeiro, F.G.; Paiva, S.A.R.; Okoshi, K. Heart failure-induced cachexia. Arq. Bras. Cardiol. 2013, 100, 476–482. [Google Scholar] [CrossRef]
- Carbone, S.; Kirkman, D.L.; Garten, R.S.; Rodriguez-Miguelez, P.; Artero, E.G.; Lee, D.C.; Lavie, C.J. Muscular strength and cardiovascular disease: An Updated State-of-the-Art Narrative Review. J. Cardiopulm. Rehabil. Prev. 2020, 40, 302–309. [Google Scholar] [CrossRef]
- Carbone, S.; Billingsley, H.E.; Rodriguez-Miguelez, P.; Kirkman, D.L.; Garten, R.; Franco, R.L.; Lee, D.C.; Lavie, C.J. Lean mass abnormalities in heart failure: The role of sarcopenia, sarcopenic obesity, and cachexia. Curr. Probl. Cardiol. 2020, 45, 100417. [Google Scholar] [CrossRef]
- Sanchis-Gomar, F.; Lavie, C.J.; Marín, J.; Perez-Quilis, C.; Eijsvogels, T.M.H.; O’Keefe, J.H.; Perez, M.V.; Blair, S.N. Exercise effects on cardiovascular disease: From basic aspects to clinical evidence. Cardiovasc. Res. 2022, 118, 2253–2266. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J.; Grgic, J.; Ogborn, D.; Krieger, J.W. Strength and hypertrophy adaptations between low- vs. high-load resistance training: A systematic review and meta-analysis. J. Strength Cond. Res. 2017, 31, 3508–3523. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Herda, T.J. Resistance exercise training and the motor unit. Eur. J. Appl. Physiol. 2022, 122, 2019–2035. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Delafontaine, P. Mechanisms of IGF-1-mediated Regulation of skeletal muscle hypertrophy and atrophy. Cells 2020, 9, 1970. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Li, B.; Xi, Y.; Cai, M.; Tian, Z. Aerobic exercise and resistance exercise alleviate skeletal muscle atrophy through IGF-1/IGF-1R-PI3K/Akt pathway in mice with myocardial infarction. Am. J. Physiol.-Cell Physiol. 2022, 322, C164–C176. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Ellingsen, Ø.; Bathen, T.F.; Høydal, M.A.; Stølen, T.; Esmaeili, M. The effect of exercise training on myocardial and skeletal muscle metabolism by MR spectroscopy in rats with heart failure. Metabolites 2019, 19, 53. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.; Choi, Y.; Sajgalik, P.; No, M.H.; Lee, S.H.; Kim, S.; Heo, J.W.; Cho, E.J.; Chang, E.; Kang, J.H.; et al. Exercise as a therapeutic strategy for sarcopenia in heart failure: Insights into underlying mechanisms. Cells 2020, 9, 2284. [Google Scholar] [CrossRef]
- Portes, L.A.; Dos Santos, A.A.; Padovani, C.R.; de Oliveira, N.C.; Serra, A.J.; Tucci, P.J.F. Swimming training attenuates the decrease of calcium responsiveness in female infarcted rats. Front. Physiol. 2022, 13, 923603. [Google Scholar] [CrossRef]
- Tyni-Lenné, R.; Jansson, E.; Sylvén, C. Female-related skeletal muscle phenotype in patients with moderate chronic heart failure before and after dynamic exercise training. Cardiovasc. Res. 1999, 42, 99–103. [Google Scholar] [CrossRef] [Green Version]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souza, L.M.; Gomes, M.J.; Brandao, B.B.; Pagan, L.U.; Gatto, M.; Damatto, F.C.; Rodrigues, E.A.; Pontes, T.H.D.; Borim, P.A.; Fernandes, A.A.H.; et al. Effects of Resistance Exercise on Slow-Twitch Soleus Muscle of Infarcted Rats. Antioxidants 2023, 12, 291. https://doi.org/10.3390/antiox12020291
Souza LM, Gomes MJ, Brandao BB, Pagan LU, Gatto M, Damatto FC, Rodrigues EA, Pontes THD, Borim PA, Fernandes AAH, et al. Effects of Resistance Exercise on Slow-Twitch Soleus Muscle of Infarcted Rats. Antioxidants. 2023; 12(2):291. https://doi.org/10.3390/antiox12020291
Chicago/Turabian StyleSouza, Lidiane Moreira, Mariana Janini Gomes, Bruna Brasil Brandao, Luana Urbano Pagan, Mariana Gatto, Felipe Cesar Damatto, Eder Anderson Rodrigues, Thierres Hernani Dias Pontes, Patricia Aparecida Borim, Ana Angelica Henrique Fernandes, and et al. 2023. "Effects of Resistance Exercise on Slow-Twitch Soleus Muscle of Infarcted Rats" Antioxidants 12, no. 2: 291. https://doi.org/10.3390/antiox12020291
APA StyleSouza, L. M., Gomes, M. J., Brandao, B. B., Pagan, L. U., Gatto, M., Damatto, F. C., Rodrigues, E. A., Pontes, T. H. D., Borim, P. A., Fernandes, A. A. H., Murata, G. M., Zornoff, L. A. M., Azevedo, P. S., Okoshi, K., & Okoshi, M. P. (2023). Effects of Resistance Exercise on Slow-Twitch Soleus Muscle of Infarcted Rats. Antioxidants, 12(2), 291. https://doi.org/10.3390/antiox12020291