
Non-Melanoma Skin Cancer and Vitamin D: The “Lost Sunlight” Paradox and the Oxidative Stress Explanation


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient and Control Population
2.2. Blood Sample
2.3. Blood Sample Fractionation and Redox Parameters Determination
2.4. Statistical Methods
3. Results
3.1. Patients’ Characteristics
3.2. Vitamin D and Oxidative Stress Parameters
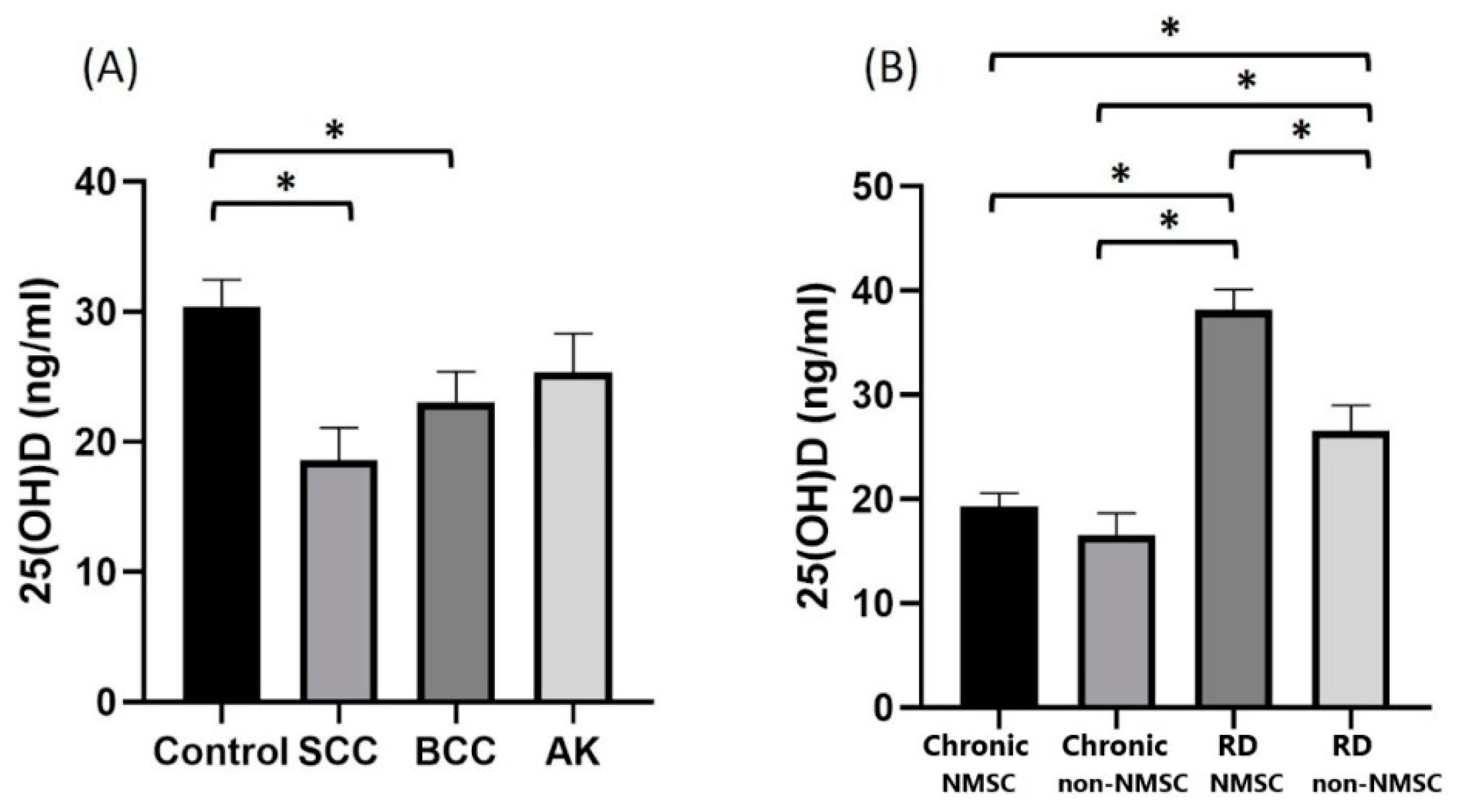
3.3. Vitamin D and Skin Cancer
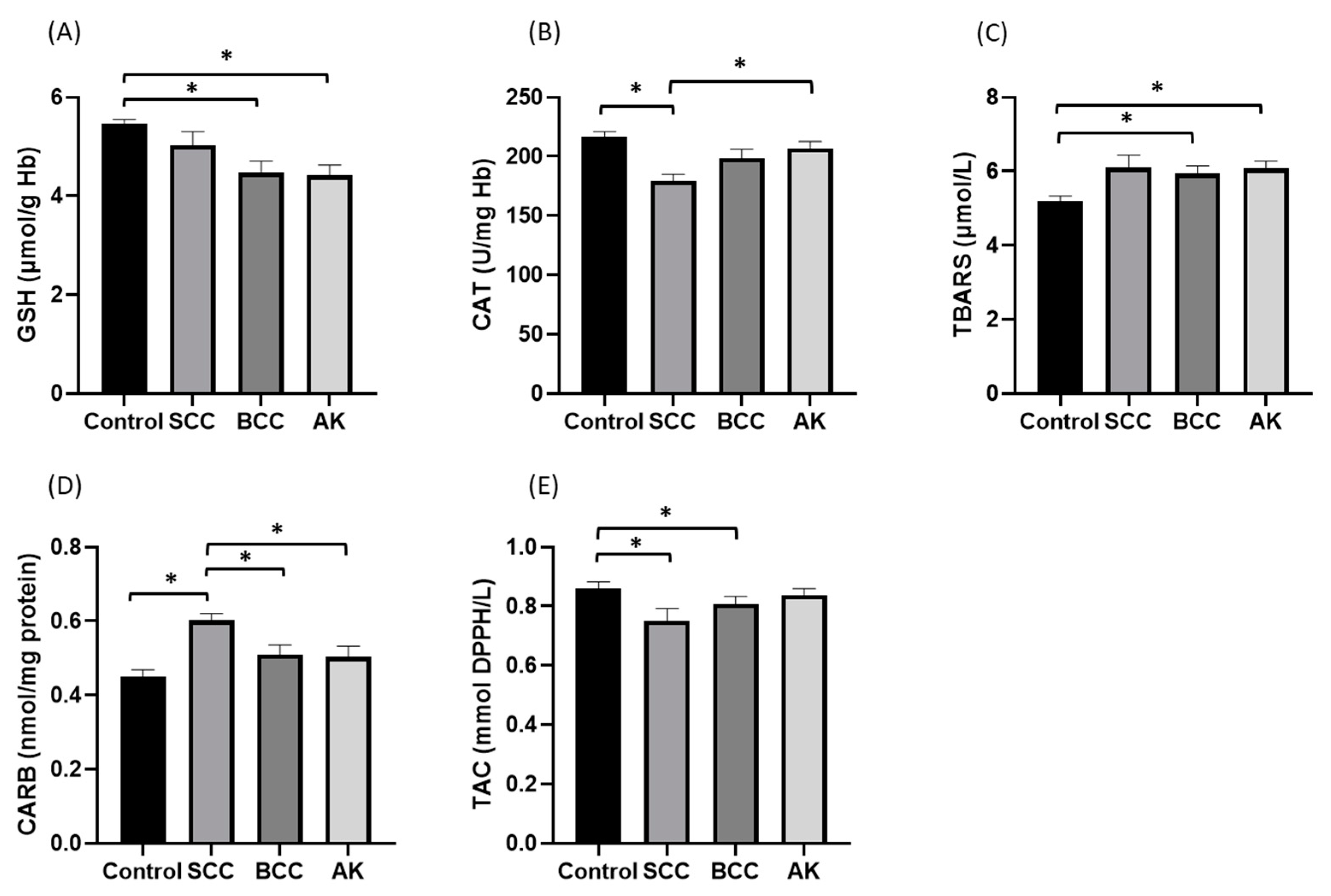
3.4. Redox Status of the Non-Melanoma Skin Cancer Patients and Controls
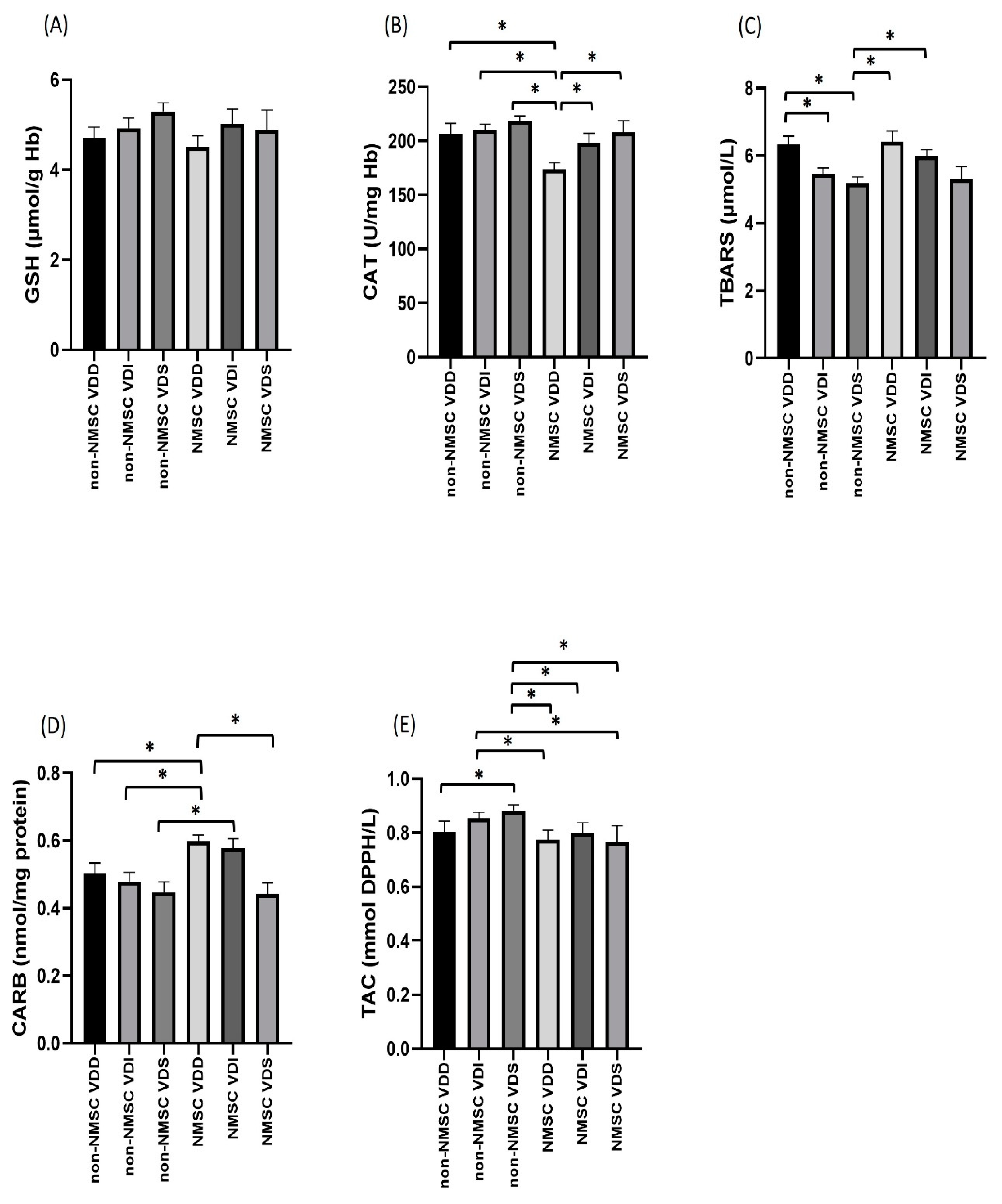
3.5. Oxidative Stress Parameters, Skin Cancer and Vitamin D
3.6. Oxidative Stress and Time of the Lesion Appearance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Apalla, Z.; Nashan, D.; Weller, R.B.; Castellsagué, X. Skin Cancer: Epidemiology, Disease Burden, Pathophysiology, Diagnosis, and Therapeutic Approaches. Dermatol. Ther. 2017, 7, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Fania, L.; Didona, D.; Morese, R.; Campana, I.; Coco, V.; Di Pietro, F.R.; Ricci, F.; Pallotta, S.; Candi, E.; Abeni, D.; et al. Basal Cell Carcinoma: From Pathophysiology to Novel Therapeutic Approaches. Biomedicines 2020, 8, 449. [Google Scholar] [CrossRef] [PubMed]
- Fania, L.; Didona, D.; Di Pietro, F.R.; Verkhovskaia, S.; Morese, R.; Paolino, G.; Donati, M.; Ricci, F.; Coco, V.; Ricci, F.; et al. Cutaneous Squamous Cell Carcinoma: From Pathophysiology to Novel Therapeutic Approaches. Biomedicines 2021, 9, 171. [Google Scholar] [CrossRef]
- Dodds, A.; Chia, A.; Shumack, S. Actinic Keratosis: Rationale and Management. Dermatol. Ther. 2014, 4, 11–31. [Google Scholar] [CrossRef]
- Sinha, R.P.; Häder, D.-P. UV-Induced DNA Damage and Repair: A Review. Photochem. Photobiol. Sci. 2002, 1, 225–236. [Google Scholar] [CrossRef]
- Nishisgori, C. Current Concept of Photocarcinogenesis. Photochem. Photobiol. Sci. 2015, 14, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Goorochurn, R.; Viennet, C.; Granger, C.; Fanian, F.; Varin-Blank, N.; Roy, C.L.; Humbert, P. Biological Processes in Solar Lentigo: Insights Brought by Experimental Models. Exp. Dermatol. 2016, 25, 174–177. [Google Scholar] [CrossRef]
- Heaney, R.P. Vitamin D in Health and Disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1535–1541. [Google Scholar] [CrossRef]
- Ramasamy, I. Vitamin D Metabolism and Guidelines for Vitamin D Supplementation. Clin. Biochem. Rev. 2020, 41, 103–126. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Farruggia, M.; Veronese, N.; Barbagallo, M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites 2021, 11, 255. [Google Scholar] [CrossRef]
- Morgado-Águila, C.; Gil-Fernández, G.; Dávila-Villalobos, O.R.; Pérez-Rey, J.; Rey-Sánchez, P.; Rodríguez-Velasco, F.J. Vitamin D Serum Levels and Non-Melanoma Skin Cancer Risk. PeerJ 2021, 9, e12234. [Google Scholar] [CrossRef] [PubMed]
- Martin-Gorgojo, A.; Gilaberte, Y.; Nagore, E. Vitamin D and Skin Cancer: An Epidemiological, Patient-Centered Update and Review. Nutrients 2021, 13, 4292. [Google Scholar] [CrossRef] [PubMed]
- Abdelwahab, R.; Huang, R.; Potla, S.; Bhalla, S.; AlQabandi, Y.; Nandula, S.A.; Boddepalli, C.S.; Gutlapalli, S.D.; Lavu, V.K.; Mohammed, L. The Relationship between Vitamin D and Basal Cell Carcinoma: A Systematic Review. Cureus 2022, 14, e29496. [Google Scholar] [CrossRef] [PubMed]
- Denzer, N.; Vogt, T.; Reichrath, J. Vitamin D Receptor (VDR) Polymorphisms and Skin Cancer: A Systematic Review. Dermatoendocrinol 2011, 3, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Sies, H. Oxidative Stress: Concept and Some Practical Aspects. Antioxidants 2020, 9, 852. [Google Scholar] [CrossRef]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef]
- Sable, K. The Role of Dietary Antioxidants in Melanoma and Nonmelanoma Skin Cancer. Cutis 2023, 111, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Rad, M.; Anil Kumar, N.V.; Zucca, P.; Varoni, E.M.; Dini, L.; Panzarini, E.; Rajkovic, J.; Tsouh Fokou, P.V.; Azzini, E.; Peluso, I.; et al. Lifestyle, Oxidative Stress, and Antioxidants: Back and Forth in the Pathophysiology of Chronic Diseases. Front. Physiol. 2020, 11, 694. [Google Scholar] [CrossRef]
- Holliman, G.; Lowe, D.; Cohen, H.; Felton, S.; Raj, K. Ultraviolet Radiation-Induced Production of Nitric Oxide:A Multi-Cell and Multi-Donor Analysis. Sci. Rep. 2017, 7, 11105. [Google Scholar] [CrossRef]
- Rajnochová Svobodová, A.; Galandáková, A.; Šianská, J.; Doležal, D.; Ulrichová, J.; Vostálová, J. Acute Exposure to Solar Simulated Ultraviolet Radiation Affects Oxidative Stress-Related Biomarkers in Skin, Liver and Blood of Hairless Mice. Biol. Pharm. Bull. 2011, 34, 471–479. [Google Scholar] [CrossRef]
- Obrador, E.; Liu-Smith, F.; Dellinger, R.W.; Salvador, R.; Meyskens, F.L.; Estrela, J.M. Oxidative Stress and Antioxidants in the Pathophysiology of Malignant Melanoma. Biol. Chem. 2019, 400, 589–612. [Google Scholar] [CrossRef]
- Chen, J.; Liu, Y.; Zhao, Z.; Qiu, J. Oxidative Stress in the Skin: Impact and Related Protection. Int. J. Cosmet. Sci. 2021, 43, 495–509. [Google Scholar] [CrossRef]
- Ferrera, L.; Barbieri, R.; Picco, C.; Zuccolini, P.; Remigante, A.; Bertelli, S.; Fumagalli, M.R.; Zifarelli, G.; La Porta, C.A.M.; Gavazzo, P.; et al. TRPM2 Oxidation Activates Two Distinct Potassium Channels in Melanoma Cells through Intracellular Calcium Increase. Int. J. Mol. Sci. 2021, 22, 8359. [Google Scholar] [CrossRef]
- Remigante, A.; Spinelli, S.; Marino, A.; Pusch, M.; Morabito, R.; Dossena, S. Oxidative Stress and Immune Response in Melanoma: Ion Channels as Targets of Therapy. Int. J. Mol. Sci. 2023, 24, 887. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Vitamin D Deficiency: Effects on Oxidative Stress, Epigenetics, Gene Regulation, and Aging. Biology 2019, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.T.; Brożyna, A.A.; Zmijewski, M.A.; Janjetovic, Z.; Kim, T.-K.; Slominski, R.M.; Tuckey, R.C.; Mason, R.S.; Jetten, A.M.; Guroji, P.; et al. The Role of Classical and Novel Forms of Vitamin D in the Pathogenesis and Progression of Nonmelanoma Skin Cancers. Adv. Exp. Med. Biol. 2020, 1268, 257–283. [Google Scholar] [CrossRef]
- Chaiprasongsuk, A.; Janjetovic, Z.; Kim, T.-K.; Schwartz, C.J.; Tuckey, R.C.; Tang, E.K.Y.; Raman, C.; Panich, U.; Slominski, A.T. Hydroxylumisterols, Photoproducts of Pre-Vitamin D3, Protect Human Keratinocytes against UVB-Induced Damage. Int. J. Mol. Sci. 2020, 21, 9374. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.; Brożyna, A.; Kim, T.-K.; Elsayed, M.; Janjetovic, Z.; Qayyum, S.; Slominski, R.; Oak, A.; Li, C.; Podgorska, E.; et al. CYP11A1-derived Vitamin D Hydroxyderivatives as Candidates for Therapy of Basal and Squamous Cell Carcinomas. Int. J. Oncol. 2022, 61, 96. [Google Scholar] [CrossRef] [PubMed]
- Chaiprasongsuk, A.; Janjetovic, Z.; Kim, T.-K.; Jarrett, S.G.; D’Orazio, J.A.; Holick, M.F.; Tang, E.K.Y.; Tuckey, R.C.; Panich, U.; Li, W.; et al. Protective Effects of Novel Derivatives of Vitamin D3 and Lumisterol against UVB-Induced Damage in Human Keratinocytes Involve Activation of Nrf2 and P53 Defense Mechanisms. Redox Biol. 2019, 24, 101206. [Google Scholar] [CrossRef]
- Slominski, R.M.; Raman, C.; Elmets, C.; Jetten, A.M.; Slominski, A.T.; Tuckey, R.C. The Significance of CYP11A1 Expression in Skin Physiology and Pathology. Mol. Cell. Endocrinol. 2021, 530, 111238. [Google Scholar] [CrossRef]
- Gracia-Darder, I.; Carrera, C.; Alamon-Reig, F.; Puig, S.; Malvehy, J.; Podlipnik, S. Vitamin D Deficiency in Melanoma Patients Is Associated with Worse Overall Survival: A Retrospective Cohort Study. Melanoma Res. 2022, 32, 384–387. [Google Scholar] [CrossRef]
- Reddy, Y.N.; Murthy, S.V.; Krishna, D.R.; Prabhakar, M.C. Role of Free Radicals and Antioxidants in TB Patients. Indian J. Tuberc 2004, 51, 213–218. [Google Scholar]
- Veskoukis, A.S.; Kyparos, A.; Paschalis, V.; Nikolaidis, M.G. Spectrophotometric Assays for Measuring Redox Biomarkers in Blood. Biomarkers 2016, 21, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Janaszewska, A.; Bartosz, G. Assay of Total Antioxidant Capacity: Comparison of Four Methods as Applied to Human Blood Plasma. Scand. J. Clin. Lab. Investig. 2002, 62, 231–236. [Google Scholar] [CrossRef]
- Keles, M.S.; Taysi, S.; Sen, N.; Aksoy, H.; Akçay, F. Effect of Corticosteroid Therapy on Serum and CSF Malondialdehyde and Antioxidant Proteins in Multiple Sclerosis. Can. J. Neurol. Sci. 2001, 28, 141–143. [Google Scholar] [CrossRef]
- Patsoukis, N.; Zervoudakis, G.; Panagopoulos, N.T.; Georgiou, C.D.; Angelatou, F.; Matsokis, N.A. Thiol Redox State (TRS) and Oxidative Stress in the Mouse Hippocampus after Pentylenetetrazol-Induced Epileptic Seizure. Neurosci. Lett. 2004, 357, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Hellenic National Metereological Service Climate Data by City, Sunshine Duration. Available online: http://www.Emy.Gr/Emy/El/Agriculture/Agriculture_city?Poli=Larisa (accessed on 9 March 2023).
- Merrill, S.J.; Subramanian, M.; Godar, D.E. Worldwide Cutaneous Malignant Melanoma Incidences Analyzed by Sex, Age, and Skin Type over Time (1955–2007): Is HPV Infection of Androgenic Hair Follicular Melanocytes a Risk Factor for Developing Melanoma Exclusively in People of European-Ancestry? Dermatoendocrinol 2016, 8, e1215391. [Google Scholar] [CrossRef] [PubMed]
- Xyda, S.E.; Kotsa, K.; Doumas, A.; Papanastasiou, E.; Garyfallos, A.A.; Samoutis, G. Could the Majority of the Greek and Cypriot Population Be Vitamin D Deficient? Nutrients 2022, 14, 3778. [Google Scholar] [CrossRef]
- Manios, Y.; Moschonis, G.; Lambrinou, C.-P.; Tsoutsoulopoulou, K.; Binou, P.; Karachaliou, A.; Breidenassel, C.; Gonzalez-Gross, M.; Kiely, M.; Cashman, K.D. A Systematic Review of Vitamin D Status in Southern European Countries. Eur. J. Nutr. 2018, 57, 2001–2036. [Google Scholar] [CrossRef]
- Mahamat-Saleh, Y.; Aune, D.; Schlesinger, S. 25-Hydroxyvitamin D Status, Vitamin D Intake, and Skin Cancer Risk: A Systematic Review and Dose–Response Meta-Analysis of Prospective Studies. Sci. Rep. 2020, 10, 13151. [Google Scholar] [CrossRef]
- Tang, J.Y.; Parimi, N.; Wu, A.; John Boscardin, W.; Shikany, J.M.; Chren, M.-M.; Cummings, S.R.; Epstein, E.H.; Bauer, D.C. Inverse Association between Serum 25(OH) Vitamin D Levels and Non-Melanoma Skin Cancer in Elderly Men. Cancer Causes Control. 2010, 21, 387–391. [Google Scholar] [CrossRef]
- Lesiak, A.; Norval, M.; Wodz-Naskiewicz, K.; Pawliczak, R.; Rogowski-Tylman, M.; Sysa-Jedrzejowska, A.; Sobjanek, M.; Wlodarkiewicz, A.; Narbutt, J. An Enhanced Risk of Basal Cell Carcinoma Is Associated with Particular Polymorphisms in the VDR and MTHFR Genes. Exp. Dermatol. 2011, 20, 800–804. [Google Scholar] [CrossRef]
- Vornicescu, C.; Ungureanu, L.; Șenilă, S.; Vesa, Ș.; Cosgarea, R.; Baican, C.; Mihu, M. Assessment of Sun-related Behavior and Serum Vitamin&Nbsp;D in Basal Cell Carcinoma: Preliminary Results. Exp. Ther. Med. 2020, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.M.; Szejnfeld, V.L.; Enokihara, M.Y.; Michalany, N.; Castro, C.H. High Serum 25-Hydroxyvitamin D Concentration in Patients with a Recent Diagnosis of Non-Melanoma Skin Cancer: A Case-Control Study. Eur. J. Dermatol. 2018, 28, 649–653. [Google Scholar] [CrossRef]
- Jain, S.K.; Parsanathan, R.; Achari, A.E.; Kanikarla-Marie, P.; Bocchini, J.A. Glutathione Stimulates Vitamin D Regulatory and Glucose-Metabolism Genes, Lowers Oxidative Stress and Inflammation, and Increases 25-Hydroxy-Vitamin D Levels in Blood: A Novel Approach to Treat 25-Hydroxyvitamin D Deficiency. Antioxid. Redox Signal. 2018, 29, 1792–1807. [Google Scholar] [CrossRef]
- Paprocki, J.; Sutkowy, P.; Piechocki, J.; Woźniak, A. Association between Vitamin D Supplements, Oxidative Stress Biomarkers, and Hyperbaric Therapy in Patients with Sudden Sensorineural Hearing Loss. Oxid. Med. Cell. Longev. 2021, 2021, 8895323. [Google Scholar] [CrossRef] [PubMed]
- Spanidis, Y.; Mpesios, A.; Stagos, D.; Goutzourelas, n.; Baror, D.; Karapetsa, M.; Zakynthinos, E.; Spandidos, D.A.; Tsatsakis, A.M.; Leon, G.; et al. Assessment of the Redox Status in Patients with Metabolic Syndrome and Type 2 Diabetes Reveals Great Variations. Exp. Ther. Med. 2016, 11, 895–903. [Google Scholar] [CrossRef]
- Pompella, A.; Sies, H.; Wacker, R.; Brouns, F.; Grune, T.; Biesalski, H.K.; Frank, J. The Use of Total Antioxidant Capacity as Surrogate Marker for Food Quality and Its Effect on Health Is to Be Discouraged. Nutrition 2014, 30, 791–793. [Google Scholar] [CrossRef]
- Chaisiriwong, L.; Wanitphakdeedecha, R.; Sitthinamsuwan, P.; Sampattavanich, S.; Chatsiricharoenkul, S.; Manuskiatti, W.; Panich, U. A Case-Control Study of Involvement of Oxidative DNA Damage and Alteration of Antioxidant Defense System in Patients with Basal Cell Carcinoma: Modulation by Tumor Removal. Oxid. Med. Cell. Longev. 2016, 2016, 5934024. [Google Scholar] [CrossRef]
- Omar, H.S.; Taha, F.M.; Fouad, S.; Ibrahim, F.A.; El Gendy, A.; Bassyouni, I.H.; El-Shazly, R. The Association between Vitamin D Levels and Oxidative Stress Markers in Egyptian Behcet’s Disease Patients. Orphanet J. Rare Dis. 2022, 17, 264. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Categories-Percentages |
|---|---|
| Sex | Female (40%, Ν = 40) Male (60%, Ν = 60) |
| BMI | Underweight (8%, Ν = 8) Normal (55%, Ν = 55) Overweight (30%, Ν = 30) Obese (7%, Ν = 7) |
| Skin disease category | Skin cancer (51%, Ν = 51) SCC (25%, Ν = 25) BCC (26%, Ν = 26) Precancerous lesion Actinic keratosis (22%, Ν = 22) Control-benign lesions (27%, Ν = 27) |
| Time of diagnosis | Recently diagnosed NMSC patients (22%, Ν = 22) Chronic NMSC patients (29%, Ν = 29) Recently diagnosed non-NMSC lesion patients (23%, Ν = 23) Chronic non-NMSC lesion patients (26%, Ν = 26) |
| Site of lesion | Face (56.2%, Ν = 41) Non facial lesions (43.8%, Ν = 32) |
| Previously diagnosed with skin cancer | No (73.6%, Ν = 53) Yes (26.4%, Ν = 19) |
| Fitzpatrick Classification | Type 2 (62.6%, Ν = 62) Type 3 (36.4%, Ν = 36) Type 4 (1%, Ν = 1) |
| Measured Parameter | Mean Value |
|---|---|
| GSH | 4.87 μmol/g Hb (S.D. = 1.13, Range = [2.34, 7.65]) |
| Catalase activity | 200.39 U/mg Hb (S.D. = 32.87, Range = [109.83, 282.19]) |
| TBARS | 5.82 μmol/L (S.D. = 1.17, Range = [3.05, 9.93]) |
| CARBS | 0.52 nmol/mg protein (S.D. = 0.13, Range = [0.21, 0.79]) |
| TAC | 0.81 mmol DPPH /L (S.D. = 0.15, Range = [0.14, 0.99]) |
| Vitamin D | 24.43 ng/mL (S.D.=12.80, Range= [3, 56]) |
| Vitamin D Classification | Deficiency (37%, Ν = 37) Insufficiency (35%, Ν = 35) Sufficiency (28%, Ν = 28) |
| Variables | GSH | Catalase | TBARS | CARBS | TAC | 25(OH) D |
|---|---|---|---|---|---|---|
| GSH | 1 | |||||
| Catalase | 0.140 | 1 | ||||
| TBARS | −0.273 | 0.061 | 1 | |||
| CARBS | −0.131 | −0.224 | 0.190 | 1 | ||
| TAC | 0.155 | −0.032 | −0.171 | −0.127 | 1 | |
| 25(OH) D | 0.277 | 0.372 | −0.429 | −0.362 | 0.222 | 1 |
| Variable | Categories | N | Value | Statistics | p-Value |
|---|---|---|---|---|---|
| Skin disease category | NMSC Control | 51 49 | Mean value = 20.87 Mean value = 28.14 | t (98) = −2.945 | 0.004 |
| Skin cancer subtype | SCC BCC Actinic Keratosis Control | 25 26 22 27 | Median = 17.42 Median = 20.78 Median = 22.00 Median = 28.00 | H (3) = 12.555 | 0.006 |
| Time of diagnosis | Recently diagnosed skin cancer patients Chronic skin cancer patients Recently diagnosed non-NMSC lesion patients Chronic non-NMSC lesion patients | 22 29 23 26 | Median = 28.15 Median = 14.00 Median = 39.70 Median = 20.50 | H (3) = 42.257 | <0.001 |
| Site of lesion | Facial Non facial | 4132 | Mean value = 24.00 Mean value = 19.94 | t (71) = 1.342 | 0.184 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karampinis, E.; Aloizou, A.-M.; Zafiriou, E.; Bargiota, A.; Skaperda, Z.; Kouretas, D.; Roussaki-Schulze, A.-V. Non-Melanoma Skin Cancer and Vitamin D: The “Lost Sunlight” Paradox and the Oxidative Stress Explanation. Antioxidants 2023, 12, 1107. https://doi.org/10.3390/antiox12051107
Karampinis E, Aloizou A-M, Zafiriou E, Bargiota A, Skaperda Z, Kouretas D, Roussaki-Schulze A-V. Non-Melanoma Skin Cancer and Vitamin D: The “Lost Sunlight” Paradox and the Oxidative Stress Explanation. Antioxidants. 2023; 12(5):1107. https://doi.org/10.3390/antiox12051107
Chicago/Turabian StyleKarampinis, Emmanouil, Athina-Maria Aloizou, Efterpi Zafiriou, Alexandra Bargiota, Zoi Skaperda, Demetrios Kouretas, and Angeliki-Viktoria Roussaki-Schulze. 2023. "Non-Melanoma Skin Cancer and Vitamin D: The “Lost Sunlight” Paradox and the Oxidative Stress Explanation" Antioxidants 12, no. 5: 1107. https://doi.org/10.3390/antiox12051107
APA StyleKarampinis, E., Aloizou, A. -M., Zafiriou, E., Bargiota, A., Skaperda, Z., Kouretas, D., & Roussaki-Schulze, A. -V. (2023). Non-Melanoma Skin Cancer and Vitamin D: The “Lost Sunlight” Paradox and the Oxidative Stress Explanation. Antioxidants, 12(5), 1107. https://doi.org/10.3390/antiox12051107