
COVID-19 Vaccination and Related Determinants of Hesitancy among Pregnant Women: A Systematic Review and Meta-Analysis
 ,
,
Abstract
:1. Introduction
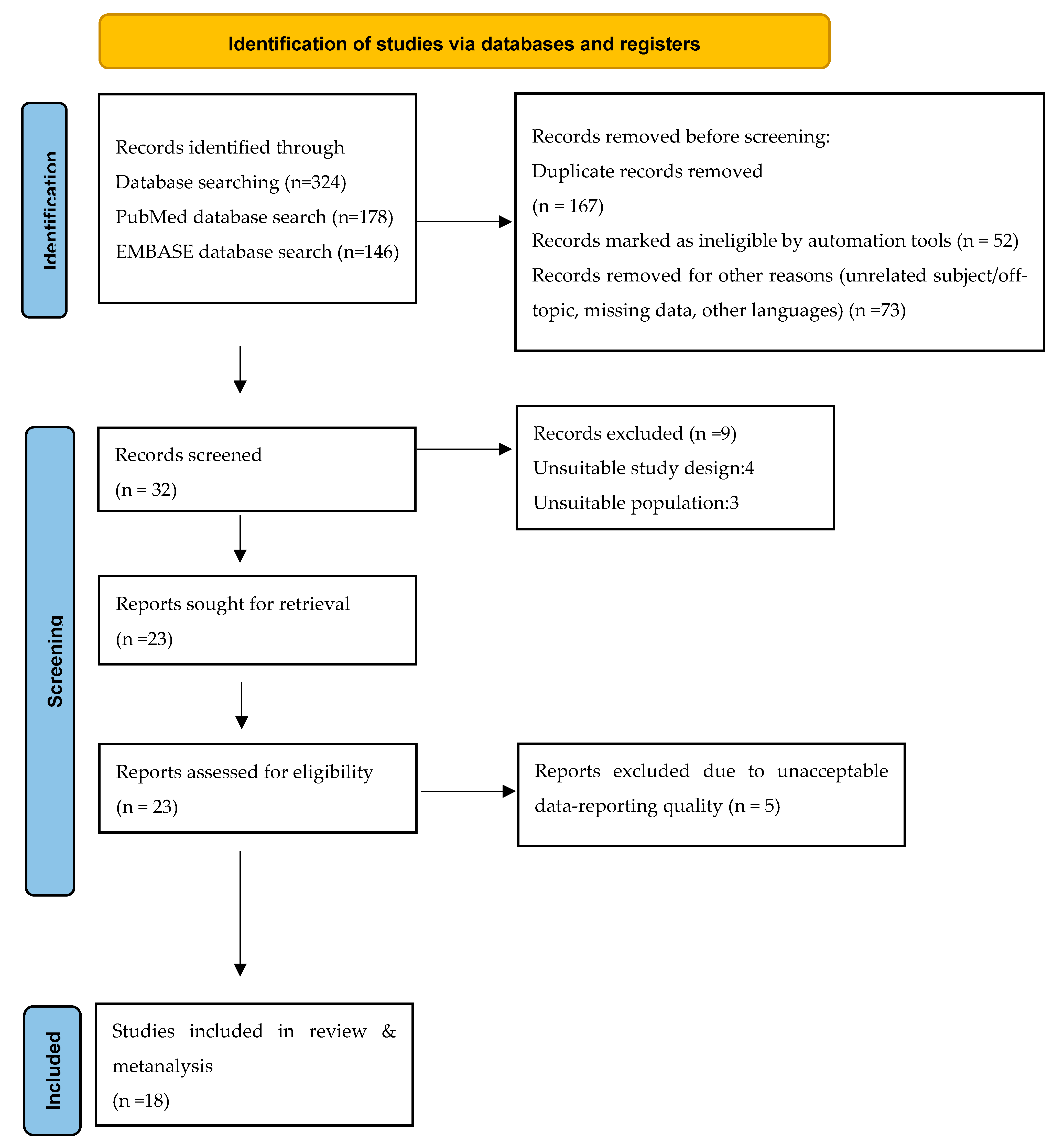
2. Materials and Methods
- Population: Studies involved pregnant women or women who had recently given birth.
- Intervention: Investigating pregnant women’s attitudes towards vaccination against COVID-19 through a questionnaire. Studies investigating pregnant women’s attitudes towards vaccines for diseases other than COVID-19 were rejected.
- Comparison: Studies compared demographic, social, and occupational characteristics of pregnant women with their attitudes toward vaccination against COVID-19.
- Outcome: The studied outcomes of the publications/studies were the rate of acceptance of the vaccine against COVID-19 and the factors related to hesitancy or refusal of vaccination.
- Study Design: The studies were primary quantitative studies. Secondary studies (reviews, meta-analyses), case studies, and qualitative studies were not included in the review.
- Timeframe: The studies must have been published by 31 December 2021 and written in English or Greek. Studies published in a language other than English and Greek were not included. Furthermore, studies in which the full text could not be located were also excluded.
- General characteristics of the study (name of 1st author, year of publication, country of conduct, type of study)
- Sample characteristics (sample size, average age of pregnant women, gestational week)
- Outcome (vaccination acceptance/refusal rate)
- Significant findings (finding, or non-statistically significant association of vaccination acceptance/hesitancy with demographic, social, and occupational characteristics)
Statistical Analysis
3. Results
Quantitative Synthesis of Studies–Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Michailidou, D.; Stavridou, A.; Panagouli, E.D.; Sergentanis, T.N.; Psaltopoulou, T.; Bacopoulou, F.; Baltag, V.; Greydanus, D.E.; Mastorakos, G.; Chrousos, G.P.; et al. The impact of COVID-19 during pregnancy on maternal and neonatal outcomes: A systematic review. EMBnet. J. 2021, 26, e969. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F., III; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status-United States. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; von Dadelszen, P.; Kalafat, E.; Sebghati, M.; Ladhani, S.; Ugwumadu, A.; Draycott, T.; O’Brien, P.; Magee, L. Change in obstetric attendance and activities during the COVID-19 pandemic. Lancet Infect. Dis. 2021, 21, e115. [Google Scholar] [CrossRef] [PubMed]
- Iacobucci, G. Covid-19 and pregnancy: Vaccine hesitancy and how to overcome it. BMJ 2021, 375, n2862. [Google Scholar] [CrossRef] [PubMed]
- Falsaperla, R.; Leone, G.; Familiari, M.; Ruggieri, M. COVID-19 vaccination in pregnant and lactating women: A systematic review. Expert Rev. Vaccines 2021, 20, 1619–1628. [Google Scholar] [CrossRef]
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. COVID-19 Vaccine in Pregnant and Lactating Women: A Review of Existing Evidence and Practice Guidelines. Infect. Dis. Rep. 2021, 13, 685–699. [Google Scholar] [CrossRef]
- Engjom, H.; Aabakke, A.J.M.; Klungsøyr, K.; Svanvik, T.; Äyräs, O.; Jonasdottir, E.; Thurn, L.; Jones, E.; Pettersson, K.; Nyfløt, L.T.; et al. COVID-19 in pregnancy—Characteristics and outcomes of pregnant women admitted to hospital because of SARS-CoV-2 infection in the Nordic countries. Acta Obstet. Gynecol. Scand. 2021, 100, 1611–1619. [Google Scholar] [CrossRef]
- Artymuk, N.V.; Belokrinitskaya, T.E.; Filippov, O.S.; Frolova, N.I.; Surina, M.N. Perinatal outcomes in pregnant women with COVID-19 in Siberia and the Russian Far East. J. Matern.-Fetal Neonatal Med. 2021, 35, 5427–5430. [Google Scholar] [CrossRef]
- Ayala-Ramírez, P.; González, M.; Escudero, C.; Quintero-Arciniegas, L.; Giachini, F.R.; Alves de Freitas, R.; Damiano, A.E.; García-Robles, R. Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Pregnancy. A Non-systematic Review of Clinical Presentation, Potential Effects of Physiological Adaptations in Pregnancy, and Placental Vascular Alterations. Front. Physiol. 2022, 13, 384. [Google Scholar] [CrossRef]
- Prasad, S.; Kalafat, E.; Blakeway, H.; Townsend, R.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Le Doare, K.; Ladhani, S.; et al. Systematic review and meta-analysis of the effectiveness and perinatal outcomes of COVID-19 vaccination in pregnancy. Nat. Commun. 2022, 13, 2414. [Google Scholar] [CrossRef]
- RCOG. COVID-19 Vaccines, Pregnancy and Breastfeeding FAQs. Royal College of Obstetricians & Gynaecologists. 2021. Available online: https://www.rcog.org.uk/guidance/coronavirus-covid-19-pregnancy-and-women-s-health/vaccination/covid-19-vaccines-pregnancy-and-breastfeeding-faqs/ (accessed on 5 March 2022).
- World Health Organization (WHO). Update on WHO Interim Recommendations on COVID-19 Vaccination of Pregnant and Lactating Women. 2021. Available online: https://www.who.int/publications/m/item/update-on-who-interim-recommendations-on-covid-19-vaccination-of-pregnant-and-lactating-women (accessed on 24 August 2022).
- Barker, P.; Hartley, D.; Beck, A.F.; Oliver, G.; Sampath, B.; Roderick, T.; Miff, S. Rethinking Herd Immunity: Managing the Covid-19 Pandemic in a Dynamic Biological and Behavioral Environment. NEJM Catalyst. 2021, 10, 5. [Google Scholar]
- Schaal, N.K.; Zöllkau, J.; Hepp, P.; Fehm, T.; Hagenbeck, C. Pregnant and breastfeeding women’s attitudes and fears regarding the COVID-19 vaccination. Arch. Gynecol. Obstet. 2022, 306, 365–372. [Google Scholar] [CrossRef]
- Mappa, I.; Luviso, M.; Distefano, F.A.; Carbone, L.; Maruotti, G.M.; Rizzo, G. Women perception of SARS-CoV-2 vaccination during pregnancy and subsequent maternal anxiety: A prospective observational study. J. Matern.-Fetal Neonatal Med. 2021, 35, 6302–6305. [Google Scholar] [CrossRef]
- Battarbee, A.N.; Stockwell, M.S.; Varner, M.; Newes-Adeyi, G.; Daugherty, M.; Gyamfi-Bannerman, C.; Tita, A.T.; Vorwaller, K.; Vargas, C.; Subramaniam, A.; et al. Attitudes Toward COVID-19 Illness and COVID-19 Vaccination among Pregnant Women: A Cross-Sectional Multicenter Study during August-December 2020. Am. J. Perinatol. 2020, 39, 75–83. [Google Scholar] [CrossRef]
- Citu, C.; Chiriac, V.D.; Citu, I.M.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Popescu, D.E.; Ratiu, A.; Buca, O.; Gorun, F. Appraisal of COVID-19 Vaccination Acceptance in the Romanian Pregnant Population. Vaccines 2022, 10, 952. [Google Scholar] [CrossRef]
- Ghamri, R.A.; Othman, S.S.; Alhiniah, M.H.; Alelyani, R.H.; Badawi, A.M.; Alshahrani, A.A. Acceptance of COVID-19 Vaccine and Associated Factors Among Pregnant Women in Saudi Arabia. Patient Prefer. Adherence 2022, 16, 861–873. [Google Scholar] [CrossRef]
- Ayhan Goncu, S.; Oluklu, D.; Atalay, A.; Menekse Beser, D.; Tanacan, A.; Moraloglu Tekin, O.; Sahin, D. COVID-19 vaccine acceptance in pregnant women. Int. J. Gynaecol. Obstet. 2021, 154, 291–296. [Google Scholar] [CrossRef]
- Levy, A.T.; Singh, S.; Riley, L.E.; Prabhu, M. Acceptance of COVID-19 vaccination in pregnancy: A survey study. Am. J. Obstet. Gynecol. Mfm 2021, 3, 100399. [Google Scholar] [CrossRef]
- Mattocks, K.M.; Kroll-Desrosiers, A.; Moore Simas, T.A.; Bastian, L.A.; Marteeny, V.; Walker, L.; Sheahan, K.; Elwy, A.R. Examining Pregnant Veterans’ Acceptance and Beliefs Regarding the COVID-19 Vaccine. J. Gen. Intern. Med. 2022, 37 (Suppl. S3), 671–678. [Google Scholar] [CrossRef]
- Mohan, S.; Reagu, S.; Lindow, S.; Alabdulla, M. COVID-19 vaccine hesitancy in perinatal women: A cross-sectional survey. J. Perinat. Med. 2021, 49, 678–685. [Google Scholar] [CrossRef]
- Pairat, K.; Phaloprakarn, C. Acceptance of COVID-19 vaccination during pregnancy among Thai pregnant women and their spouses: A prospective survey. Reprod. Health 2022, 19, 74. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Jouzová, A.; Üstün, B.; Lagová, E.; Hruban, L.; Janků, P.; Pokorná, A.; Klugarová, J.; Koščík, M.; Klugar, M. COVID-19 Vaccine Acceptance of Pregnant and Lactating Women (PLW) in Czechia: An Analytical Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 13373. [Google Scholar] [CrossRef] [PubMed]
- Regan, A.K.; Kaur, R.; Nosek, M.; Swathi, P.A.; Gu, N.Y. COVID-19 vaccine acceptance and coverage among pregnant persons in the United States. Prev. Med. Rep. 2022, 29, 101977. [Google Scholar] [CrossRef]
- Reifferscheid, L.; Marfo, E.; Assi, A.; Dubé, E.; MacDonald, N.E.; Meyer, S.B.; Bettinger, J.A.; Driedger, S.M.; Robinson, J.; Sadarangani, M.; et al. COVID-19 vaccine uptake and intention during pregnancy in Canada. Can. J. Public Health 2022, 113, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Siegel, M.R.; Lumbreras-Marquez, M.I.; James, K.; McBay, B.R.; Gray, K.J.; Schantz-Dunn, J.; Diouf, K.; Goldfarb, I.T. Perceptions and Attitudes toward COVID-19 Vaccination among Pregnant and Postpartum Individuals. Am. J. Perinatol. 2022, 29, 1489–1495. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Sutton, D.; D’Alton, M.; Zhang, Y.; Kahe, K.; Cepin, A.; Goffman, D.; Staniczenko, A.; Yates, H.; Burgansky, A.; Coletta, J.; et al. COVID-19 vaccine acceptance among pregnant, breastfeeding, and nonpregnant reproductive-aged women. Am. J. Obstet. Gynecol. MFM 2021, 3, 100403. [Google Scholar] [CrossRef]
- Sznajder, K.K.; Kjerulff, K.H.; Wang, M.; Hwang, W.; Ramirez, S.I.; Gandhi, C.K. COVID-19 vaccine acceptance and associated factors among pregnant women in Pennsylvania 2020. Prev. Med. Rep. 2022, 26, 101713. [Google Scholar] [CrossRef]
- Tao, L.; Wang, R.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Liu, M.; Liu, J. Acceptance of a COVID-19 vaccine and associated factors among pregnant women in China: A multi-center cross-sectional study based on health belief model. Hum. Vaccines Immunother. 2021, 17, 2378–2388. [Google Scholar] [CrossRef]
- Niemi, M.E.K.; Karjalainen, J.; Liao, R.G.; Neale, B.M.; Daly, M.; Ganna, A.; Pathak, G.A.; Andrews, S.J.; Kanai, M.; Veerapen, K.; et al. Mapping the human genetic architecture of COVID-19. Nature 2021, 600, 472–477. [Google Scholar] [CrossRef]
- Carbone, L.; Di Girolamo, R.; Mappa, I.; Saccone, G.; Raffone, A.; Di Mascio, D.; De Vivo, V.; D’Antonio, F.; Guida, M.; Rizzo, G.; et al. Worldwide beliefs among pregnant women on SARS-CoV-2 vaccine: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 268, 144–164. [Google Scholar] [CrossRef]
- Nikpour, M.; Sepidarkish, M.; Omidvar, S.; Firouzbakht, M. Global prevalence of acceptance of COVID-19 vaccines and associated factors in pregnant women: A systematic review and meta-analysis. Expert Rev. Vaccines 2022, 21, 843–851. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Uptake of COVID-19 Vaccines among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 766. [Google Scholar] [CrossRef]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Effectiveness and Safety of COVID-19 Vaccine among Pregnant Women in Real-World Studies: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 246. [Google Scholar] [CrossRef]
- Singh, S.; Sedgh, G.; Hussain, R. Unintended pregnancy: Worldwide levels, trends, and outcomes. Stud. Fam. Plann. 2010, 41, 241–250. [Google Scholar] [CrossRef]
- Saito, S.; Nakashima, A.; Shima, T.; Ito, M. Th1/Th2/Th17 and regulatory T-cell paradigm in pregnancy. Am. J. Reprod. Immunol. 2010, 63, 601–610. [Google Scholar] [CrossRef]
- Stock, S.J.; Carruthers, J.; Calvert, C.; Denny, C.; Donaghy, J.; Goulding, A.; Hopcroft, L.E.M.; Hopkins, L.; McLaughlin, T.; Pan, J.; et al. SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland. Nat. Med. 2022, 28, 504–512. [Google Scholar] [CrossRef]
- Wolf, M.E.; Luz, B.; Niehaus, L.; Bhogal, P.; Bäzner, H.; Henkes, H. Thrombocytopenia and Intracranial Venous Sinus Thrombosis after “COVID-19 Vaccine AstraZeneca” Exposure. J. Clin. Med. 2021, 10, 1599. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author/s (Year, Country) | Research Type | Time Period | Aim | Research Tools | Sample | Results |
|---|---|---|---|---|---|---|
| Ν/Age/Gestational Age | ||||||
| Battarbee et al. (2022, USA) [16] | cross-sectional survey | 9 August–10 December 2020 | To evaluate pregnant women’s attitudes toward COVID-19 illness and vaccination and identify factors associated with vaccine acceptability | Pregnant women filled out questionnaires when enrolled in a prospective COVID-19 cohort | Ν = 915/81% was 18–34 yrs/<28 weeks of gestation | Although most pregnant women worried about COVID-19 illness, <50% were willing to get vaccinated during pregnancy. Racial and ethnic disparities in plans to accept the COVID-19 vaccine highlight the need to prioritize strategies to address perceived barriers among high-risk groups at high risk for COVID-19. |
| Citu et al. (2022, Romania) [17] | cross-sectional study | 1 January–1 May 2022 | Το determine the scale of acceptance of the COVID-19 vaccination campaign among pregnant women in Romania, as well as the variables affecting their choices | online survey including standardized and unstandardized questionnaires | Ν = 345/Not specified/not specified | The statistically significant determinant factors for COVID-19 vaccination acceptance were the urban area of residence, having a higher level of education, the third trimester of pregnancy, trusting the government, being a frequent traveler, fearing the severity of COVID-19, the higher availability of COVID-19 vaccines nearby, and seeing more people getting vaccinated. |
| Ghamri et al. (2022, Saudi Arabia) [18] | cross-sectional study | July–September 2021 | To determine the level of acceptance of COVID-19 vaccination and detect the factors that influence vaccine acceptance among pregnant women in Saudi Arabia | web-based study | Ν = 5307/˃18/multi-stage sampling | High acceptance of COVID-19 vaccination. The two major reasons for refusal were concerns about a lack of data on COVID-19 vaccination safety and the possibility of harming the fetus. |
| Authors (Year, country) | Research type | Period | Aim | Research Tool | Sample | Results |
| Ν/Age/Gestational age | ||||||
| Ayhan Goncu et al. (2021, Τurkey) [19] | prospective observational study | 1 January–1 February 2021 | To determine vaccine acceptance and hesitancy attitudes toward coronavirus disease 2019 (COVID-19) vaccines in pregnant women | face to face interviews with 40 questions | Ν = 300/ 27.99 (±5.6) yrs/ 28.74 (±8.88) wks | Low acceptance of COVID-19 vaccination in the sample of pregnant women. Concern about vaccine safety was the major reason for hesitancy. |
| Levy et al. (2021, USA) [20] | cross-sectional study | 14 December 2020–14 January 2021 | To describe the COVID-19 vaccine acceptance rate among pregnant women | questionnaires of 31 questions | Ν = 662/82.9% >30 yrs/during the nuchal translucency or anatomic survey sonogram appointment | Young age, Black or African American race, Hispanic ethnicity, having less than a Bachelor’s degree, and declining the seasonal influenza vaccine were associated with nonacceptance of COVID-19 vaccination in pregnancy. Trust in the information received about vaccinations was the strongest predictor of COVID-19 vaccination acceptance. |
| Mappa et al. (2021, Italy) [15] | prospective observational study | December 2020 | To evaluate the propensity of a population of Italian women to receive the vaccine and its psychological impact | a multi-section questionnaire, State–Trait–Anxiety–Inventory (STAI) | Ν = 161/not specified/not specified | The majority of pregnant women were considered to have a positive attitude toward the SARS-CoV-2 vaccine. The vaccine campaign seems to increase the maternal level of anxiety and this increase is more marked by a negative attitude toward the vaccine. |
| Mattocks et al. (2022, USA) [21] | cross-sectional study | 1 January–31 May 2021 | To examine pregnant veterans’ acceptance of COVID-19 vaccines, along with perceptions and beliefs regarding vaccine safety and vaccine conspiracy beliefs | telephone surveys (~45 min in length) | Ν = 92/not specified/at 20 wks & 3 months postpartum | Those who received a vaccine had significantly greater vaccine knowledge and less belief in vaccine conspiracy theories. Greater knowledge of vaccines in general and fewer beliefs in vaccine conspiracies were the strongest predictors of acceptance of a COVID-19 vaccine during pregnancy. |
| Authors (year, country) | Research type | Period | Aim | Research tool | Sample | Results |
| Ν/Age/Gestational age | ||||||
| Mohan et al. (2021, Qatar) [22] | cross-sectional study | 15 October–15 November 2020 | To explore attitudes to COVID-19 vaccination among perinatal women | online survey; a composite questionnaire, a validated vaccine hesitancy measurement tool called VAX | Ν = 341/ 69.8% were 26–35 yrs/not specified | The sample exhibited a vaccine hesitancy rate of 25% toward COVID-19 immunization. The group’s main concerns were infection risks, and the main factor determining vaccine hesitancy was vaccine-specific safety concerns. Previous vaccine “acceptors” showed vaccine hesitancy to COVID-19 immunization A third of the group cited the non-availability of the vaccine as a concern. |
| Pairat & Phaloprakarn (2022, Thailand) [23] | prospective survey | 1 July–30 September 2021 | To determine the rates and associated factors of accepting attitudes toward COVID-19 vaccination during pregnancy among pregnant Thai women and their spouses, and to evaluate the actual rate of vaccination during pregnancy among these women | Written self-answered questionnaires were completed by eligible couples (pregnant women and their husbands - separately) during their hospital visit. | Pregnant women Ν = 171/median age = 28 (23–33 yrs)/26 wks (18–31 wks of gestation) | Having a husband who favored COVID-19 vaccination for his wife was independently associated with COVID-19 vaccine acceptance among pregnant women. |
| Riad et al. (2021, Czech Republic) [24] | cross-sectional survey-based study | 1 August–31 October 2021 | To evaluate the attitudes of pregnant and lactating Czech women (PLW) towards COVID-19 vaccines and the determinants of their attitudes | a self-administered questionnaire (SAQ) consisting of 32 close-ended items, adapted from previous instruments used for the same purpose | Ν = 278 pregnant/ 51.5% was 19–31 yrs/85.6% were in the 3rd trimester | The overall COVID-19 vaccine acceptance (both immediate and delayed) level was substantially high, with a significant difference between pregnant women. The trimester, education level, employment status, and previous live births were significant determinants for COVID-19 vaccine acceptance among the target population. |
| Regan et al. (2022, USA) [25] | cross-sectional survey | 1 December 2020–31 July 2021 | To evaluate the acceptance of any dose of the COVID-19 vaccine during pregnancy | online questionnaire | Ν = 2213/not specified/not specified | Participants were more likely to receive or plan to receive the COVID-19 vaccine if they had group prenatal care, were employed in a workplace with a policy recommending vaccination, and believed COVID-19 vaccines are safe. |
| Authors (Year, Country) | Research Type | Period | Aim | Research tool | Sample | Results |
| Ν/Age/Gestational age | ||||||
| Reifferscheid et al. (2022, Canada) [26] | cross-sectional study | 28 May–7 June 2021 | To investigate COVID-19 vaccine uptake and intent among pregnant people in Canada and determine associated factors | online questionnaire | Ν = 193/ 31.0 (±6.2) yrs/ Not specified | Confidence in vaccine safety was the most significant predictor of COVID-19 vaccine acceptance among respondents, and vaccine safety concerns were the most cited reason for not accepting the COVID-19 vaccine during pregnancy. |
| Schaal et al. (2022, Germany) [14] | cross-sectional study | 30 March–19 April 2021 | To address COVID-19 vaccination attitudes among pregnant and breastfeeding women including the underlying reasons for their decision | online questionnaire | Pregnant women Ν = 1043/31.8 (±4.3) yrs/ 24.7 (±9.1) wks of gestation | The willingness to be vaccinated was significantly related to the women’s anxiety levels about getting infected and developing disease symptoms. The main reasons for vaccination hesitancy were women’s perception of vaccination-specific information, limited scientific evidence on vaccination safety, and the fear of harming the fetus or infant. |
| Siegel et al. (2022, USA) [27] | cross-sectional study | 1 June–31 August 2021 | To characterize attitudes toward novel coronavirus disease 2019 (COVID-19) vaccination and to evaluate factors associated with vaccine uptake among pregnant individuals | a convenience sample of pregnant individuals receiving prenatal care | Ν = 477/ Not specified/ Not specified | Overall, 233 (49.3%) had received or were scheduled to receive a COVID-19 vaccine. Age, White race, non-Hispanic or Latin ethnicity, working from home, and typical receipt of the influenza vaccine were factors associated with COVID-19 vaccination. |
| Skjefte et al. (2021, 16 countries) [28] | cross-sectional study | 28 October–18 November 2020 | To assess acceptance of COVID-19 vaccination among pregnant women and mothers of children younger than 18 years old, as well as potential predictors | online questionnaire | Ν = 5282/ 34.4 (±7.3) yrs/ 20.0 (±9.4) wks | Vaccine acceptance was generally highest in India, the Philippines, and all sampled countries in Latin America; it was lowest in Russia, the United States, and Australia. The strongest predictors of vaccine acceptance included confidence in vaccine safety or effectiveness, worrying about COVID-19, belief in the importance of vaccines to their own country, compliance with mask guidelines, trust of public health agencies/health science, as well as attitudes towards routine vaccines. |
| Authors (Year, Country) | Research Type | Period | Aim | Research tool | Sample | Results |
| Ν/Age/Gestational age | ||||||
| Sutton et al. (2021, USA) [29] | cross-sectional study | 7 January–29 January 2021 | To understand vaccine acceptability among pregnant, nonpregnant, and breastfeeding respondents and elucidate factors associated with COVID-19 vaccine acceptance | online questionnaire of 23 items | Pregnant sample: Ν = 216/ 34.0 (±6.0)/ Not specified | Pregnant respondents of non-White or non-Asian races were more likely to decline vaccination than nonpregnant and breastfeeding respondents. Working in healthcare was not associated with vaccine acceptance. |
| Sznajder et al. (2022, USA) [30] | cross-sectional study | 15 May–1 December 2020 | Τo examine factors associated with vaccine acceptance | Pregnant women receiving prenatal care completed a questionnaire. | Ν = 196/ 80% aged <35 yrs/ 44% in the 3rd trimester | Women who had received an influenza vaccine within the past year were more likely to be willing to receive the COVID-19 vaccine than women who had never received an influenza vaccine or those who received it more than one year ago. Similarly, women who were employed full-time were more willing to receive the COVID-19 vaccine than women who were not employed full-time. |
| Tao et al. (2021, China) [31] | cross-sectional study | 13–17 November 2020 | To explore the acceptance of a COVID-19 vaccine and related factors among pregnant women | questionnaire distributed in 6 hospitals | Ν = 1392/ 55.4% <30 yrs/ 44% in the 3rd trimester | About one quarter of pregnant women have vaccine hesitancy. The acceptance rate was associated with young age, western region, low level of education, late pregnancy, high knowledge score on COVID-19, high level of perceived susceptibility, low level of perceived barriers, high level of perceived benefit, and high level of perceived cues to action. |
| Authors (Year) | (N) Number of Pregnant Women Who Would Get Vaccinated/Total Sample (%) | Maternal Age as a Factor of COVID-19 Vaccination Acceptance | Gestational Age as a Factor of COVID-19 Vaccination Acceptance | Educational Level as a Factor of COVID-19 Vaccination Acceptance | Race/Ethnicity as a Factor of COVID-19 Vaccination Acceptance | Marital Status as a Factor of COVID-19 Vaccination Acceptance | Occupational Status as a Factor of COVID-19 Vaccination Acceptance | Underlying Diseases/Comorbidities as a Factor of COVID-19 Vaccination Acceptance |
|---|---|---|---|---|---|---|---|---|
| Maternal Age/OR (95% CI) | Gestational Age/OR (95% CI) | Educational Level/OR (95% CI) | Race/Ethnicity /OR (95% CI) | Marital Status/OR (95% CI) | Occupational Status/OR (95% CI) | Underlying Diseases/Comorbidities OR (95% CI) | ||
| Battarbee et al. (2022) [16] | 374/915 (41%) | 18–34 years/0.8 (0.6–1.1) 35–50 years/Reference category |
|
|
|
| ||
| Citu et al. (2022) [17] | 184/345 (53.3%) | |||||||
| Ghamri et al. (2022) [18] | 3548/5307 (68%) | ≥18 years of age /1.02 (1.018–1.036) | All 3 trimesters/ 0.986 (0.981–0.991) |
|
|
| ||
| Goncu Ayhan et al. (2021) [19] | 111/300 (37%) | |||||||
| Levy et al. (2021) [20] | 381/362 (58.3%) |
|
|
|
| |||
| Mappa et al. (2021) [15] | 136/161 (84.5%) | |||||||
| Mattocks et al. (2022) [21] | 22/62 (69%) | |||||||
| Mohan et al. (2021) [22] | 158/316 (50.0%) | |||||||
| Pairat & Chadakarn (2022) [23] | 104/171 (60.8%) |
|
|
| ||||
| Riad et al. (2021) [24] | 254/316 (70.2%) |
|
| Living with a partner/5.43 (0.57–52.01) Without a partner/Reference category |
| |||
| Regan et al. (2022) [25] | 1238/2213 (55.4%) | |||||||
| Reifferscheid et al. (2022) [26] | 111/193 (55.5%) | ≥15 years of age/ 1.01 (0.96–1.06) |
|
|
|
| ||
| Schaal et al. (2022) [14] | 184/1043 (17.6%) | |||||||
| Siegel et al. (2022) [27] | 233/477 (49.3%) | |||||||
| Skjefte et al. (2021) [28] | 2747/5282 (52.0%) |
|
| Married/0.92 (0.82–1.03) Unmarried/Reference category |
|
| ||
| Sutton et al. (2021) [29] | 86/216 (21.3%) |
|
|
| ||||
| Sznajder et al. (2022) [30] | 127/196 (65%) | ≤35 years/1.87 (1.20–2.93) >35 years/Reference category |
| College degree/2.79 (1.48, 5.28) <College degree/Reference category |
|
| ||
| Tao et al. (2021) [31] | 1077/1392 (77.4%) | ≤35 years/1.87 (1.20–2.93) >35 years/Reference category |
|
|
|
|
| Authors (Year) | Influenza Vaccine | |
|---|---|---|
| OR (95% CI) | ||
| Battarbee et al. (2022) [16] | Yes | 2.6 (1.9–3.6) |
| No | Reference category | |
| Ghamri et al. (2022) [18] | Yes | 2.639 (1.847–3.771) |
| No | Reference category | |
| Levy et al. (2021) [20] | Yes | Reference category |
| Has not received the vaccine, but plans to receive it | 0.48 (0.28–0.82) | |
| No | 0.12 (0.07–0.21) | |
| Pairat & Chadakarn (2022) [23] | Yes | 1.61 (0.75–3.45) |
| No | Reference category | |
| Skjefte et al. (2021) [28] | Yes | 3.29 (2.91–3.72) |
| No | Reference category | |
| Sutton et al. (2021) [25] | Yes | 2.25 (1.66–3.05) |
| No | Reference category | |
| Sznajder et al. (2022) [30] | Yes | 5.25 (2.55–10.79) |
| No | Reference category | |
| Tao et al. (2021) [31] | Yes | 1.30 (0.74–2.28) |
| No | Reference category | |
| Authors (Year) | Positive COVID-19 Test | Knowledge of COVID-19 | Confidence That COVID-19 Vaccine Is Safe | Confidence That COVID-19 Vaccine Is Effective | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |||||
| Battarbee et al. (2022) [16] | Yes | 11.94 (2.72–52.36) | ||||||
| No | Reference category | |||||||
| Pairat & Chadakarn (2022) [23] | Yes | 4.42 (2.19–8.93) | Yes | 4.96 (2.45–10.05) | ||||
| No | Reference category | No | Reference category | |||||
| Reifferscheid et al. (2022) [26] | Yes | 1.81 (0.98, 3.36) | ||||||
| No | Reference category | |||||||
| Ghamri et al. (2022) [18] | Yes | 1.721 (1.332–2.223) | ||||||
| Νο | Reference category | |||||||
| Levy et al. (2021) [20] | Yes | 0.30 (0.16–0.59) | Yes | 1.194 (0.998–1.429) | ||||
| Νο | Reference category | No | Reference category | |||||
| Skjefte et al. (2021) [28] | Yes | 1.04 (0.93–1.17) | Yes | 8.42 (7.44–9.53) | Yes | 6.68 (5.90–7.26) | ||
| No | Reference category | No | Reference category | No | Reference category | |||
| Sutton et al. (2021) [29] | Yes | 0.46 (0.21–1.01) | ||||||
| No | Reference category | |||||||
| Sznajder et al. (2022) [30] | Yes | 0.90 (0.21–3.89) | ||||||
| No | Reference category | |||||||
| Mattocks et al. (2022) [21] | Non-stop | 1.76 (1.17–2.64) | ||||||
| Riad et al. (2021) [24] | Yes | 0.91 (0.34–2.48) | ||||||
| No | Reference category | |||||||
| Tao et al. (2021) [31] | Non-stop | 1.05 (1.01–1.10) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarantaki, A.; Kalogeropoulou, V.E.; Taskou, C.; Nanou, C.; Lykeridou, A. COVID-19 Vaccination and Related Determinants of Hesitancy among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 2055. https://doi.org/10.3390/vaccines10122055
Sarantaki A, Kalogeropoulou VE, Taskou C, Nanou C, Lykeridou A. COVID-19 Vaccination and Related Determinants of Hesitancy among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines. 2022; 10(12):2055. https://doi.org/10.3390/vaccines10122055
Chicago/Turabian StyleSarantaki, Antigoni, Vasiliki Evangelia Kalogeropoulou, Chrysoula Taskou, Christina Nanou, and Aikaterini Lykeridou. 2022. "COVID-19 Vaccination and Related Determinants of Hesitancy among Pregnant Women: A Systematic Review and Meta-Analysis" Vaccines 10, no. 12: 2055. https://doi.org/10.3390/vaccines10122055
APA StyleSarantaki, A., Kalogeropoulou, V. E., Taskou, C., Nanou, C., & Lykeridou, A. (2022). COVID-19 Vaccination and Related Determinants of Hesitancy among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines, 10(12), 2055. https://doi.org/10.3390/vaccines10122055