
Sero-Epidemiological Study of Bordetella pertussis Infection in the Italian General Population
 , ,
, ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Collection
2.2. Measurement of Antibody Titers
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tan, T.; Dalby, T.; Forsyth, K.; Halperin, S.A.; Heininger, U.; Hozbor, D.; Plotkin, S.; Ulloa-Gutierrez, R.; von König, C.W. Pertussis across the globe. Recent epidemiologic trends from 2000 to 2013. Pediatr. Infect. Dis. J. 2015, 34, e222–e232. [Google Scholar] [CrossRef] [PubMed]
- Cherry, J.D. Pertussis in young infants throughout the world. Clin. Infect. Dis. 2016, 63, S119–S122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsyth, K.D.; Tan, T.; von König, C.W.; Heininger, U.; Chitkara, A.J.; Plotkin, S. Recommendations to control pertussis prioritized relative to economies: A Global Pertussis Initiative update. Vaccine 2018, 36, 7270–7275. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Piano Nazionale di Prevenzione Vaccinale 2017–2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 31 December 2021).
- Wilson, S.E.; Deeks, S.L.; Hatchette, T.F.; Crowcroft, N.S. The role of seroepidemiology in the comprehensive surveillance of vaccine-preventable diseases. CMAJ 2012, 184, E70–E76. [Google Scholar] [CrossRef] [Green Version]
- Cutts, F.T.; Hanson, M. Seroepidemiology: An underused tool for designing and monitoring vaccination programmes in low- and middle-income countries. Trop. Med. Int. Health 2016, 21, 1086–1098. [Google Scholar] [CrossRef]
- Pebody, R.G.; Gay, N.J.; Giammanco, A.; Baron, S.; Schellekens, J.; Tischer, A.; Olander, R.M.; Andrews, N.J.; Edmunds, W.J.; Lecoeur, H.; et al. The seroepidemiology of Bordetella pertussis infection in Western Europe. Epidemiol. Infect. 2005, 133, 159–171. [Google Scholar] [CrossRef]
- Pezzotti, P.; Bellino, S.; Prestinaci, F.; Iacchini, S.; Lucaroni, F.; Camoni, L.; Barbieri, M.M.; Ricciardi, W.; Stefanelli, P.; Rezza, G. The impact of immunization programs on 10 vaccine preventable diseases in Italy: 1900–2015. Vaccine 2018, 365, 1435–1443. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Pertussis. In ECDC Annual Epidemiological Report for 2017; ECDC: Stockholm, Sweden, 2019. [Google Scholar]
- World Health Organization (WHO). Pertussis Vaccines—WHO Position Paper 2015. Available online: https://www.who.int/immunization/policy/position_papers/pertussis/en/ (accessed on 31 December 2021).
- Palazzo, R.; Carollo, M.; Fedele, G.; Rizzo, C.; Rota, M.C.; Giammanco, A.; Iannazzo, S.; Ausiello, C.M.; Sero-Epidemiology Working Group. Evidence of increased circulation of Bordetella pertussis in the Italian adult population form seroprevalence data (2012–2013). J. Med. Microbiol. 2016, 65, 649–657. [Google Scholar] [CrossRef] [Green Version]
- Osborne, K.; Weinburg, J.; Miller, E. The European Seroepidemiology Network. Eurosurveill 1997, 2, 29–31. [Google Scholar] [CrossRef]
- The Development of a European Sero-Epidemiology Collaboration for the Investigation of Vaccine Preventable Disease: Fcat Sheet. Available online: https://cordis.europa.eu/project/id/BMH4961039 (accessed on 31 December 2021).
- Edmunds, W.J.; Pebody, R.G.; Aggerback, H.; Baron, S.; Berbers, G.; Conyn-van Spaendonck, M.A.; Hallander, H.O.; Olander, R.; Maple, P.A.; Melker, H.E.; et al. The sero-epidemiology of diphtheria in Western Europe. ESEN Project. European Sero-Epidemiology Network. Epidemiol. Infect. 2000, 125, 113–125. [Google Scholar] [CrossRef]
- De Melker, H.; Pebody, R.G.; Edmunds, W.J.; Levy-Bruhl, D.; Valle, M.; Rota, M.C.; Salmaso, S.; van den Hof, S.; Berbers, G.; Saliou, P.; et al. The seroepidemiology of measles in Western Europe. Epidemiol. Infect. 2001, 126, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Nardone, A.; de Ory, F.; Carton, M.; Cohen, D.; van Damme, P.; Davidkin, I.; Rota, M.C.; de Melker, H.; Mossong, J.; Slacikova, M.; et al. The comparative sero-epidemiology of varicella zozter in 11 countries in the European region. Vaccine 2007, 25, 7866–7872. [Google Scholar] [CrossRef] [PubMed]
- Wendelboe, A.M.; van Rie, A.; Salmaso, S.; Englund, J.A. Duration of immunity against pertussis after natural infection or vaccination. Pediatr. Infect. Dis. J. 2005, 24, S58–S61. [Google Scholar] [CrossRef] [PubMed]
- Gabutti, G.; Azzari, C.; Bonanni, P.; Prato, R.; Tozzi, A.E.; zanetti, A.; Zuccotti, G. Pertussis. Hum. Vaccin. Immunother. 2015, 11, 108–117. [Google Scholar] [CrossRef] [Green Version]
- WHO. Pertussis. Available online: https://www.who.int/health-topics/pertussis#tab=tab_1 (accessed on 31 December 2021).
- European Centre for Disease Prevention and Control. Pertussis—Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Rota, M.C.; D’Ancona, F.; Massari, M.; Mandolini, D.; Giammanco, A.; Carbonari, P.; Salmaso, S.; Ciofi degli Atti, M.L. How increased pertussis vaccination coverage is changing the epidemiology of pertussis in Italy. Vaccine 2005, 23, 5299–5305. [Google Scholar] [CrossRef]
- Vitucci, A.C.; Spuri Vennarucci, V.; Grandin, A.; Russo, C.; lancella, L.; Tozzi, A.E.; Bartuli, A.; Villani, A. Pertussis in infants: An underestimated disease. BMC Infect. Dis. 2016, 16, 414. [Google Scholar] [CrossRef] [Green Version]
- Fedele, G.; Stefanelli, P. Pertussis in infants and the resurgence of a vaccine preventable disease: What to do? Commentary. Ann. Ist. Super Sanità 2017, 53, 100–103. [Google Scholar]
- Fiasca, F.; Gabutti, G.; Mattei, A. Trends in hospital admissions for pertussis infection: A nationwide retrospective observational study in Italy, 2002–2016. Int. J. Environ. Res. Public Health 2019, 16, 4531. [Google Scholar] [CrossRef] [Green Version]
- Marchi, S.; Montomoli, E.; Remarque, E.J.; Monteverde Spencer, G.T.; Azzarello, A.; Viviani, S.; Trombetta, C.M. Pertussis over two decades: Seroepidemiological study in a large population of the Siena Province, Tuscany Region, Central Italy. BMJ Open 2019, 9, e032987. [Google Scholar] [CrossRef] [Green Version]
- Barkoff, A.M.; Grondahl-Yil_Hannuksela, K.; He, Q. Seroprevalence studies of pertussis: What we have learned from different immunized populations. FEMS Pathog. Dis. 2015, 73, ftv050. [Google Scholar] [CrossRef] [Green Version]
- Berbers, G.; van Gageldonk, P.; van de Kassteele, J.; Wiedermann, U.; Desombere, I.; Dalby, T.; Toubiana, J.; Tsiodras, S.; Ferencz, I.P.; Mullan, K.; et al. Circulation of pertussis and poor protection against diphthteria among middle-aged adults in 18 European countries. Nat. Commun. 2021, 12, 2871. [Google Scholar] [CrossRef] [PubMed]
- Wehlin, L.; Ljungman, M.; Kulmann-Berenzon, S.; Galanis, I.; Huygen, K.; Pierard, D.; Dalby, T.; Petridou, E.; Molnar, Z.; Carollo, M.; et al. Pertussis seroprevalence among adults of reproductive age (20–39 years) in fourteen European countries. APMIS 2021, 129, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Boey, L.; Bosmans, E.; Braz Ferreira, L.; Heyvaert, N.; Nelen, M.; Smans, L.; Tuerlinckx, H.; Roelants, M.; Claes, K.; Derdelinckx, I.; et al. Seroprevalence of antibodies against diphtheria, tetanus and pertussis in adult at-risk patients. Vaccines 2021, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Farahat, F.; Althaqafi, A.; Al-Amri, A.; Alsaedi, A.; Abouremsh, M.; Alshaamrani, M. Cross-sectional seroprevalence study of antibody to Bordetella pertussis toxin in western Saudi Arabia: Is there a need for a vaccine booster dose for adolescents and young adults? BMJ Open 2021, 11, e042711. [Google Scholar] [CrossRef]
- Versteegen, P.; Berbers, G.A.M.; Smits, G.; Sanders, E.A.M.; van der Klis, F.R.M.; de Mleker, H.E.; van der Maas, N.A.T. More than 10 years after introduction of an acellular pertussis vaccine in infancy: A cross-sectional serosurvey of pertussis in the Netherlands. Lancet Reg. Health-Eur. 2021, 10, 100196. [Google Scholar] [CrossRef]
- Von Linstow, M.L.; Nielsen, A.Y.; Kirby, N.; Eltvedt, A.; Nordmann Winther, T.; Bybeck Nielsen, A.; Bang, D.; Poulsen, A. Immunity to vaccine-preventable diseases among paediatric healthcare workers in Denmark, 2019. Euro Surveill. 2021, 26, 2001167. [Google Scholar] [CrossRef]
- Fedele, G.; Carollo, M.; Palazzo, R.; Stefanelli, P.; Pandolfi, E.; Gesualdo, F.; Tozzi, A.E.; Carsetti, R.; Villani, A.; Nicolai, A.; et al. Parents as source of pertussis transmission in hospitalized young infants. Infection 2017, 45, 171–178. [Google Scholar] [CrossRef]
- Farizo, K.M.; Cochi, S.L.; Zell, E.R.; Brink, E.R.; Wassilak, S.G.; Patriarca, P.A. Epidemiological features of pertussis in the United States, 1980–1989. Clin. Infect. Dis. 1992, 14, 708–719. [Google Scholar] [CrossRef]
- Conde-Glez, C.; Lazcano-Ponce, E.; Rojas, R.; DeAntonio, R.; Romano-Mazzotti, L.; Crevantes, Y.; Ortega-Barria, E. Seroprevalence of Bordetella pertussis in the Mexican population: A cross-sectional study. Epidemiol. Infect. 2014, 142, 706–713. [Google Scholar] [CrossRef] [Green Version]
- Torzsa, P.; Devadiga, R.; Tafalla, M. Seroprevalence of Bordetella pertussis antibodies in adults in Hungary: Results of an epidemiological cross-sectional study. BMC Infect. Dis. 2017, 17, 242. [Google Scholar] [CrossRef] [Green Version]
- Ataei, B.; Nokhodian, Z.; Zahraei, S.M.; Gouya, M.M.; Hoseini, S.G.; Yarasn, M.; Mansourian, M.; Motlagh, M.E.; Heshmat, R.; Kelishadi, R. Seroprevalence of Bordetella pertussis among a nationally representative sample of Iranian pediatric population: The childhood and adolescence surveillance and prevention of adult noncommunicable disease-V study. J. Res. Med. Sci. 2021, 26, 21. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Principi, N. Immunization against pertussis in adolescents and adults. Clin. Microbiol: Infect. 2016, 22 (Suppl. S5), s89–s95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiasca, F.; Necozione, S.; Mattei, A. Pertussis in Italy: How to protect the “unprotectable”? Hum. Vaccin. Immunother. 2021, 17, 1136–1141. [Google Scholar] [CrossRef]
- Masseria, C.; Krishnarajah, G. The estimated incidence of pertussis in people aged 50 years old in the United States, 2006–2010. BMC Infect Dis. 2015, 15, 534, Erratum in: BMC Infect. Dis. 2016, 16, 181. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, T.M.A.; van den Steen, P.; Cheuvart, B.; Baudson, N.; Dodet, M.; Turriani, E.; Harrington, L.; Meyer, N.; Rondini, S.; Taddei, L.; et al. Seroprevalence of Bordetella pertussis infection in patients with chronic obstructive pulmonary disease in England: Analysis of the AERIS Cohort. Chronic Obstr. Pulm. Dis. 2021, 18, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Guiso, N.; Taieb, F. Pertussis in Low and Medium Income Countries: A pragmatic approach. Adv. Exp. Med. Biol. 2019, 1183, 137–149. [Google Scholar]
- Di Mattia, G.; Nicolai, A.; Frassanito, A.; Petrarca, L.; Nenna, R.; Midulla, F. Pertussis: New preventive strategies for an old disease. Paediatr. Respir. Rev. 2019, 29, 68–73. [Google Scholar] [CrossRef]
- Martinón-Torres, F.; Heininger, U.; Thomson, A.; Von König, C.H.W. Controlling pertussis: How can we do it? A focus on immunization. Expert Rev. Vaccines 2018, 17, 289–297. [Google Scholar] [CrossRef]
- Antonelli Incalzi, R.; Bernabei, R.; Bonanni, P.; Conversano, M.; Ecarnot, F.; Gabutti, G.; Maggi, S.; Paolini, D.; Sandri, F. Vaccines in older age: Moving from current practice to optimal coverage—A multidisciplinary consensus conference. Aging Clin. Exp. Res. 2020, 32, 1405–1415. [Google Scholar] [CrossRef]
- Antonelli Incalzi, R.; Blasi, F.; Conversano, M.; Gabutti, G.; Giuffrida, S.; maggi, S.; Marano, C.; Rossi, A.; Vicentini, M. Manifesto on the value of adult immunization: “We know, we intend, we advocate”. Vaccines 2021, 9, 1232. [Google Scholar] [CrossRef]
- Macina, D.; Evans, K.E. Pertussis in individuals with co-morbidities: A systematic review. Infect. Dis. Ther. 2021, 10, 1141–1170. [Google Scholar] [CrossRef] [PubMed]
- Jakovljevic, M.; Liu, Y.; Cerda, A.; Simonyan, M.; Correia, T.; Mariita, R.M.; Kumaras, A.S.; Garcia, L.; Krstic, K.; Osabohien, R.; et al. The Global South political economy of health financing and spending landscape—History and presence. J. Med. Econ. 2021, 24, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Muloiwa, R.; Kagina, B.M.; Engel, M.E.; Hussey, G.D. The burden of laboratory-confirmed pertussis in low- and middle-income countries since the inception of the Expanded Programme on Immunisation (EPI) in 1974: A systematic review and meta-analysis. BMC Med. 2020, 18, 233. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, A.; Vaughan, K.; Clarke-Deelder, E.; Suharlim, C.; Resch, S.C.; Brenzel, L.; Menzies, N.A. Producing standardized country-level immunization delivery unit cost estimates. Pharmacoeconomics 2020, 38, 995–1005. [Google Scholar] [CrossRef]
- Echaniz-Aviles, G.; Garcia-Cisneros, S.; Sanchez-Aleman, M.A.; Olamendi-Portugasl, M.; Romero-Martinez, M.; Deantonio, R.; Cervantes-Apolinar, M.Y.; Ortega-Barria, E.; Cortes-Alcala, R.; Alpuche-Aranda, C.M. Estimating Bordetella pertussis seroprevalence in adolescents and young adults in Mexico using the 2012 National Health and Nutrition Survey (ENSANUT). Vaccine 2021, 39, 5839–5844. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Samples N | Mean IgG Titer ± SD (IU/mL) | <5 IU/mL % | 5–40 IU/mL % | 40–100 IU/mL % | ≥100 IU/mL % | p-Value * | |
|---|---|---|---|---|---|---|---|
| Gender | |||||||
| Males | 2010 | 14.1 ± 22.2 | 36.8 | 55.8 | 6.2 | 1.1 | 0.007 |
| Females | 2144 | 11.9 ± 17.1 | 40.9 | 53.8 | 4.5 | 0.8 | |
| Age group (years) | |||||||
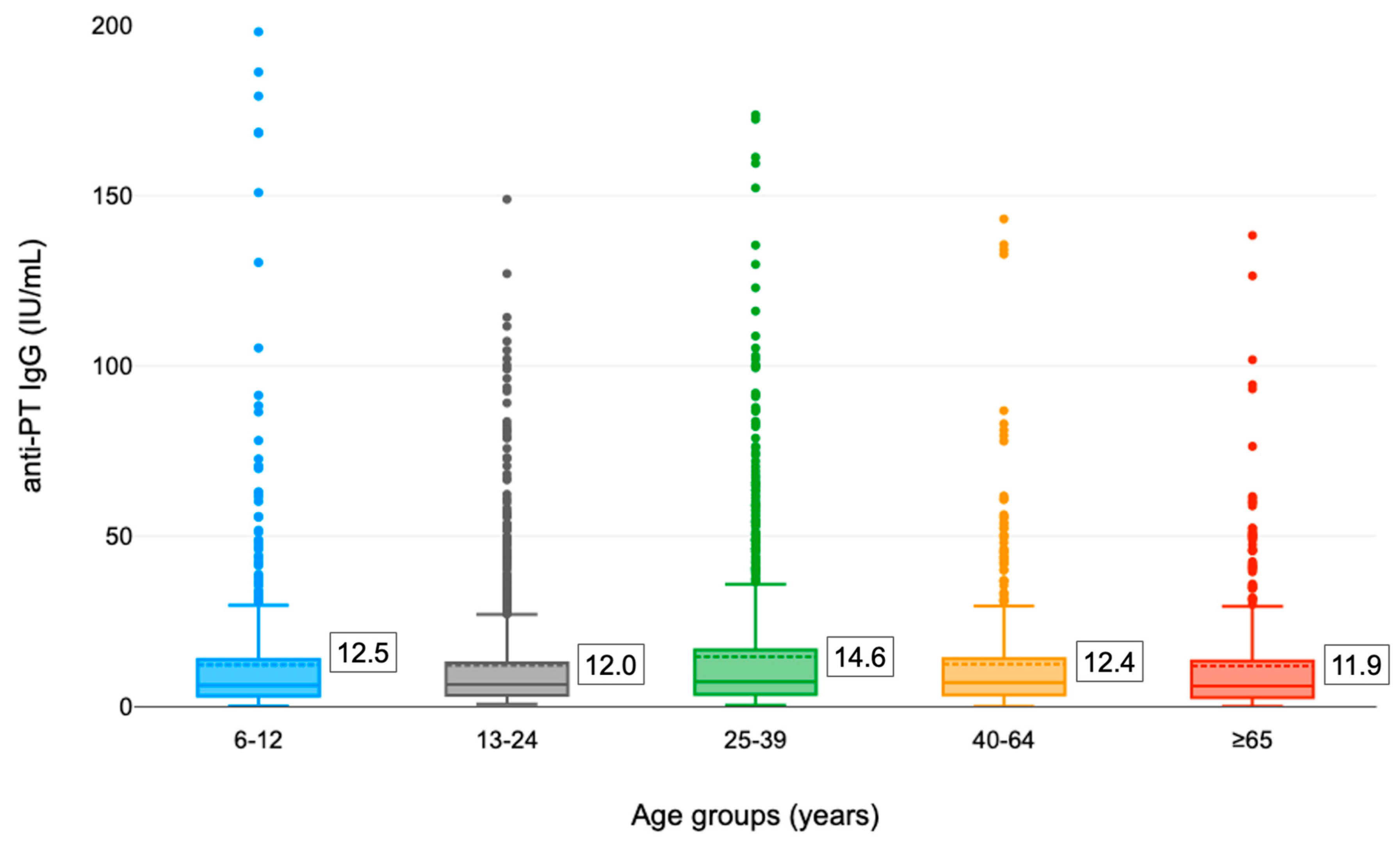
| 6–12 | 715 | 12.5 ± 24.3 | 41.1 | 54.0 | 3.8 | 1.1 | 0.993 |
| 13–24 | 1213 | 12.0 ± 16.2 | 38.7 | 55.8 | 4.9 | 0.7 | |
| 25–39 | 1277 | 14.6 ± 21.8 | 36.9 | 55.6 | 6.2 | 1.3 | |
| 40–64 | 545 | 12.4 ± 17.0 | 37.1 | 56.7 | 5.5 | 0.7 | |
| ≥65 | 404 | 11.9 ± 17.1 | 44.8 | 47.8 | 6.7 | 0.7 | |
| Geographical area | |||||||
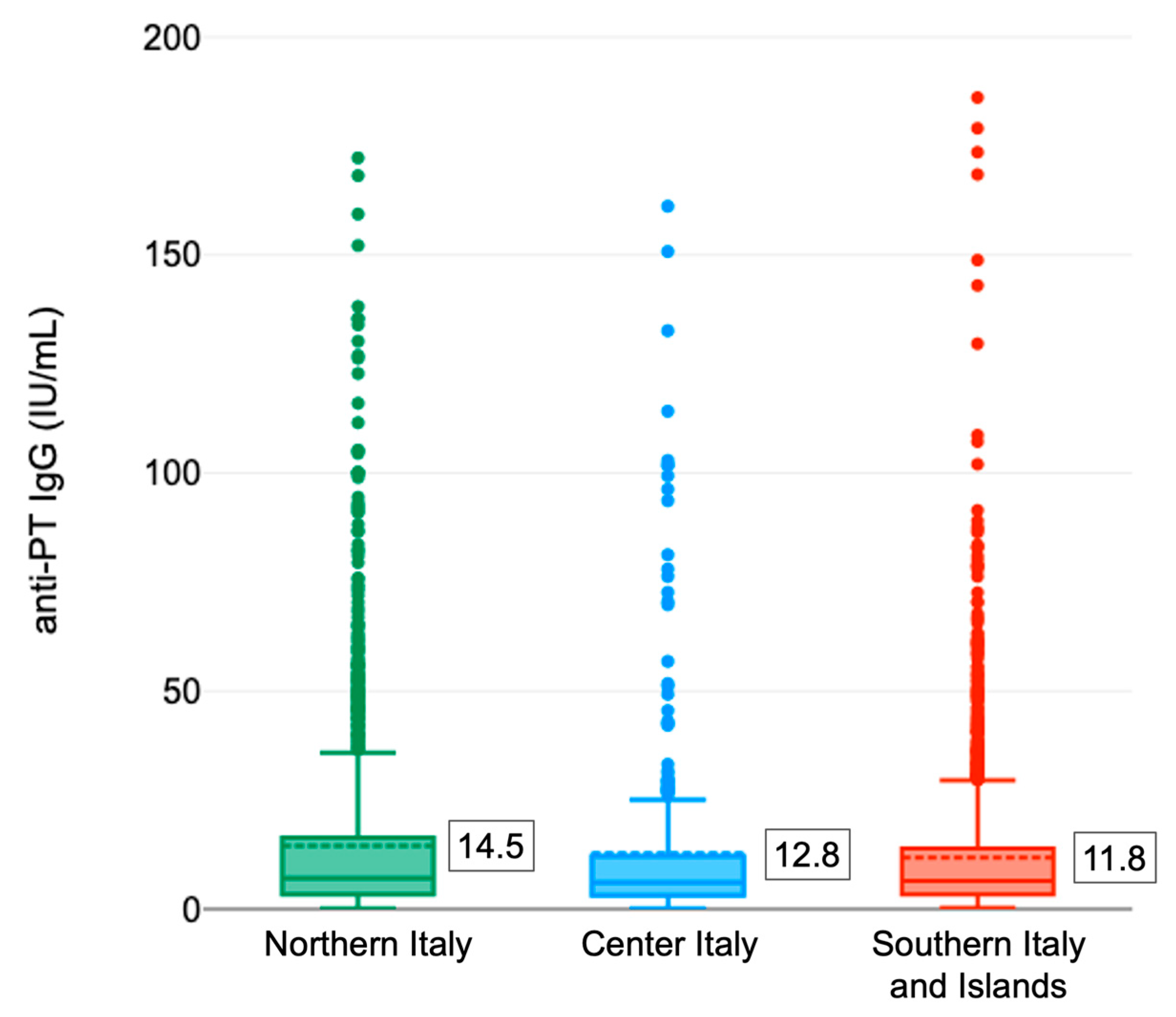
| Northern Italy | 1582 | 14.5 ± 23.6 | 37.9 | 53.5 | 7.3 | 1.3 | <0.001 |
| Center Italy | 430 | 12.8 ± 23.5 | 43.3 | 50.9 | 4.0 | 1.9 | |
| Southern Italy and Islands | 2142 | 11.8 ± 19.8 | 38.8 | 56.5 | 4.2 | 0.5 | |
| TOTAL | 4154 | 13.0 ± 19.8 | 38.9 | 54.8 | 5.3 | 1.0 | |
| Region | Samples N | Mean IgG Titer ± SD IU/mL | <5 IU/mL % | 5–40 IU/mL % | 40–100 IU/mL % | ≥100 IU/mL % |
|---|---|---|---|---|---|---|
| Apulia | 362 | 11.5 ± 17.1 | 39.2 | 56.9 | 3.0 | 0.6 |
| Basilicata | 308 | 10.5 ± 13.7 | 44.2 | 51.3 | 4.2 | 0.3 |
| Bolzano | 353 | 17.7 ± 22.4 | 33.4 | 52.1 | 13.3 | 1.1 |
| Calabria | 363 | 12.5 ± 17.8 | 40.2 | 53.7 | 5.8 | 0.3 |
| Campania | 275 | 9.1 ± 10.3 | 47.3 | 50.2 | 2.5 | 0.0 |
| Emilia-Romagna | 364 | 13.4 ± 20.4 | 37.1 | 56.3 | 5.2 | 1.4 |
| Liguria | 328 | 12.1 ± 15.3 | 40.2 | 53.4 | 6.1 | 0.3 |
| Marche | 99 | 9.2 ± 17.5 | 53.5 | 43.4 | 1.0 | 2.0 |
| Piedmont | 363 | 12.4 ± 20.0 | 41.6 | 53.7 | 3.0 | 1.7 |
| Sardinia | 396 | 15.3 ± 21.1 | 27.8 | 66.9 | 3.8 | 1.5 |
| Sicily | 438 | 11.1 ± 14.5 | 38.4 | 56.6 | 4.8 | 0.2 |
| Tuscany | 331 | 13.9 ± 24.9 | 40.2 | 53.2 | 4.8 | 1.8 |
| Veneto | 174 | 19.5 ± 37.6 | 36.2 | 50.0 | 10.9 | 2.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grassi, T.; Bagordo, F.; Savio, M.; Rota, M.C.; Vitale, F.; Arghittu, A.; Sticchi, L.; Gabutti, G.; on behalf of the Sero-Epidemiological Study Group. Sero-Epidemiological Study of Bordetella pertussis Infection in the Italian General Population. Vaccines 2022, 10, 2130. https://doi.org/10.3390/vaccines10122130
Grassi T, Bagordo F, Savio M, Rota MC, Vitale F, Arghittu A, Sticchi L, Gabutti G, on behalf of the Sero-Epidemiological Study Group. Sero-Epidemiological Study of Bordetella pertussis Infection in the Italian General Population. Vaccines. 2022; 10(12):2130. https://doi.org/10.3390/vaccines10122130
Chicago/Turabian StyleGrassi, Tiziana, Francesco Bagordo, Marta Savio, Maria Cristina Rota, Francesco Vitale, Antonella Arghittu, Laura Sticchi, Giovanni Gabutti, and on behalf of the Sero-Epidemiological Study Group. 2022. "Sero-Epidemiological Study of Bordetella pertussis Infection in the Italian General Population" Vaccines 10, no. 12: 2130. https://doi.org/10.3390/vaccines10122130
APA StyleGrassi, T., Bagordo, F., Savio, M., Rota, M. C., Vitale, F., Arghittu, A., Sticchi, L., Gabutti, G., & on behalf of the Sero-Epidemiological Study Group. (2022). Sero-Epidemiological Study of Bordetella pertussis Infection in the Italian General Population. Vaccines, 10(12), 2130. https://doi.org/10.3390/vaccines10122130