
Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Sample Size
2.3. Data Collection Tool
2.4. Operational Definitions
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Participants’ Demographics
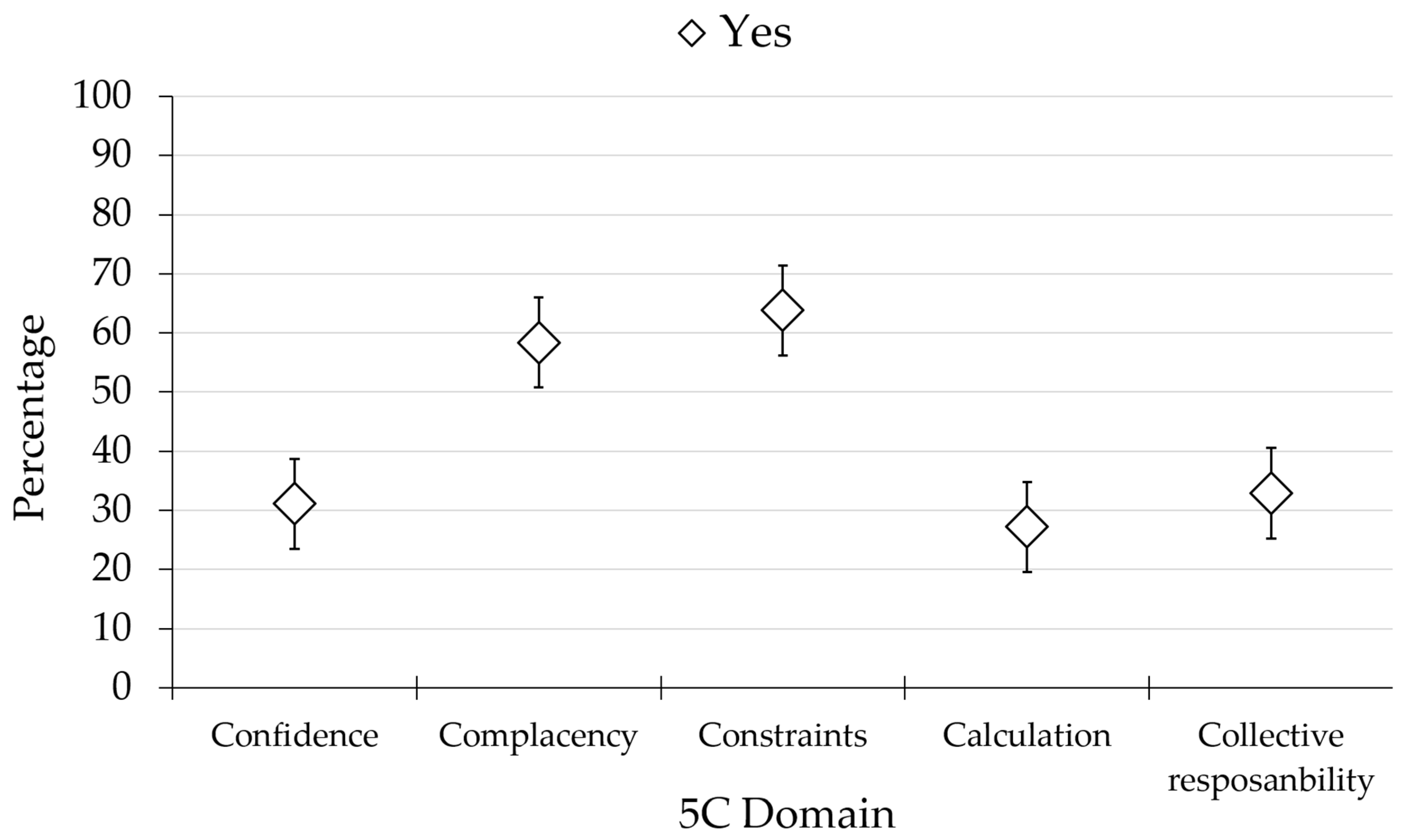
3.2. Overall Results of 5C Psychological Antecedents for MPX Vaccination among Nigerian HCWs
3.2.1. Confidence
3.2.2. Complacency
3.2.3. Collective Responsibility
3.3. The Determinants of 5C Antecedents of MPX Vaccination in the Study Sample
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harapan, H.; Ophinni, Y.; Megawati, D.; Frediansyah, A.; Mamada, S.S.; Salampe, M.; Bin Emran, T.; Winardi, W.; Fathima, R.; Sirinam, S.; et al. Monkeypox: A Comprehensive Review. Viruses 2022, 14, 2155. [Google Scholar] [CrossRef] [PubMed]
- Mauldin, M.R.; McCollum, A.M.; Nakazawa, Y.J.; Mandra, A.; Whitehouse, E.R.; Davidson, W.; Zhao, H.; Gao, J.; Li, Y.; Doty, J. Exportation of monkeypox virus from the African continent. J. Infect. Dis. 2022, 225, 1367–1376. [Google Scholar] [CrossRef]
- Ligon, B.L. Monkeypox: A review of the history and emergence in the Western hemisphere. Semin. Pediatr. Infect. Dis. 2004, 14, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Durski, K.N.; McCollum, A.M.; Nakazawa, Y.; Petersen, B.W.; Reynolds, M.G.; Briand, S.; Djingarey, M.H.; Olson, V.; Damon, I.K.; Khalakdina, A. Emergence of monkeypox—West and central Africa, 1970–2017. Morb. Mortal. Wkly. Rep. 2018, 67, 306. [Google Scholar] [CrossRef]
- Kaler, J.; Hussain, A.; Flores, G.; Kheiri, S.; Desrosiers, D. Monkeypox: A Comprehensive Review of Transmission, Pathogenesis, and Manifestation. Cureus 2022, 14, e26531. [Google Scholar] [CrossRef]
- World Health Organization. Multi-Country Monkeypox Outbreak: Situation Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396 (accessed on 23 November 2022).
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- World Health Organization. 2022 Monkeypox Outbreak: Global Trends. Available online: https://worldhealthorg.shinyapps.io/mpx_global/ (accessed on 11 November 2022).
- Yinka-Ogunleye, A.; Aruna, O.; Ogoina, D.; Aworabhi, N.; Eteng, W.; Badaru, S.; Mohammed, A.; Agenyi, J.; Etebu, E.N.; Numbere, T.W.; et al. Reemergence of Human Monkeypox in Nigeria, 2017. Emerg. Infect. Dis. 2018, 24, 1149–1151. [Google Scholar] [CrossRef]
- Fowotade, A.; Fasuyi, T.; Bakare, R. Re-emergence of monkeypox in Nigeria: A cause for concern and public enlightenment. Afr. J. Clin. Exp. Microbiol. 2018, 19, 307–313. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization—Nigeria. WHO Supports Bayelsa State to Rapidly Contain Outbreak of Monkeypox Virus. Available online: https://www.afro.who.int/news/who-supports-bayelsa-state-rapidly-contain-outbreak-monkeypox-virus (accessed on 27 November 2022).
- Alakunle, E.; Moens, U.; Nchinda, G.; Okeke, M.I. Monkeypox Virus in Nigeria: Infection Biology, Epidemiology, and Evolution. Viruses 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Silenou, B.C.; Tom-Aba, D.; Adeoye, O.; Arinze, C.C.; Oyiri, F.; Suleman, A.K.; Yinka-Ogunleye, A.; Dörrbecker, J.; Ihekweazu, C.; Krause, G. Use of Surveillance Outbreak Response Management and Analysis System for Human Monkeypox Outbreak, Nigeria, 2017–2019. Emerg. Infect. Dis. 2020, 26, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Center for Diseases Control and Prevention. Monkeypox in Nigeria. Available online: https://wwwnc.cdc.gov/travel/notices/watch/monkeypox-nigeria (accessed on 23 November 2022).
- Center for Diseases Control and Prevention. 2022 Monkeypox Outbreak Global Map. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 27 November 2022).
- ReliefWeb. Monkeypox Outbreak in Nigeria: Situation Report #2. Available online: https://reliefweb.int/report/nigeria/monkeypox-outbreak-nigeria-situation-report-2-16-october-2017?gclid=CjwKCAiApvebBhAvEiwAe7mHSGeDYGl30_2wi06rRy1M6gwE5QRy6HkRk8lKXqUiNxqH4zIaRJNCfhoCx3gQAvD_BwE (accessed on 23 November 2022).
- Nigeria Centre for Disease Control and Prevention. An Update of Monkeypox Outbreak in Nigeria [Internet]. Available online: https://ncdc.gov.ng/diseases/sitreps/?cat=8&name=An%20Update%20of%20Monkeypox%20Outbreak%20in%20Nigeria (accessed on 23 November 2022).
- Nigeria Centre for Disease Control and Prevention. Public Health Advisory on Monkeypox. Available online: https://ncdc.gov.ng/news/367/public-health-advisory-on-monkeypox (accessed on 27 November 2022).
- World Health Organization—Nigeria. Adamawa State strengthens Awareness Campaign on Monkeypox. Available online: https://www.afro.who.int/countries/nigeria/news/adamawa-state-strengthens-awareness-campaign-monkeypox (accessed on 27 November 2022).
- Rizk, J.G.; Lippi, G.; Henry, B.M.; Forthal, D.N.; Rizk, Y. Prevention and treatment of monkeypox. Drugs 2022, Epub, 1–7. [Google Scholar] [CrossRef]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.; Duncan, C.J. Clinical features and management of human monkeypox: A retrospective observational study in the UK. Lancet Infect. Dis. 2022, 22, P1153–P1162. [Google Scholar] [CrossRef]
- Ophinni, Y.; Frediansyah, A.; Sirinam, S.; Megawati, D.; Stoian, A.M.; Enitan, S.S.; Akele, R.Y.; Sah, R.; Pongpirul, K.; Abdeen, Z.; et al. Monkeypox: Immune response, vaccination and preventive efforts. Narra J. 2022, 2, e90. [Google Scholar] [CrossRef]
- Xiang, Y.; White, A. Monkeypox virus emerges from the shadow of its more infamous cousin: Family biology matters. Emerg. Microbes Infect. 2022, 11, 1768–1777. [Google Scholar] [CrossRef]
- Siddiqui, M.O.; Syed, M.A.; Tariq, R.; Mansoor, S. Multicounty outbreak of monkeypox virus—Challenges and recommendations. J. Med. Virol. 2022, 95, e27966. [Google Scholar] [CrossRef]
- Rao, A.K.; Petersen, B.W.; Whitehill, F.; Razeq, J.H.; Isaacs, S.N.; Merchlinsky, M.J.; Campos-Outcalt, D.; Morgan, R.L.; Damon, I.; Sánchez, P.J. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 734. [Google Scholar] [CrossRef]
- Pittman, P.R.; Hahn, M.; Lee, H.S.; Koca, C.; Samy, N.; Schmidt, D.; Hornung, J.; Weidenthaler, H.; Heery, C.R.; Meyer, T.P.H.; et al. Phase 3 Efficacy Trial of Modified Vaccinia Ankara as a Vaccine against Smallpox. New Engl. J. Med. 2019, 381, 1897–1908. [Google Scholar] [CrossRef]
- Keckler, M.S.; Salzer, J.S.; Patel, N.; Townsend, M.B.; Nakazawa, Y.J.; Doty, J.B.; Gallardo-Romero, N.F.; Satheshkumar, P.S.; Carroll, D.S.; Karem, K.L.; et al. IMVAMUNE® and ACAM2000® Provide Different Protection against Disease When Administered Postexposure in an Intranasal Monkeypox Challenge Prairie Dog Model. Vaccines 2020, 8, 396. [Google Scholar] [CrossRef]
- Overton, E.T.; Stapleton, J.; Frank, I.; Hassler, S.; Goepfert, P.A.; Barker, D.; Wagner, E.; von Krempelhuber, A.; Virgin, G.; Weigl, J.; et al. Safety and Immunogenicity of Modified Vaccinia Ankara-Bavarian Nordic Smallpox Vaccine in Vaccinia-Naive and Experienced Human Immunodeficiency Virus-Infected Individuals: An Open-Label, Controlled Clinical Phase II Trial. Open Forum Infect. Dis. 2015, 2, ofv040. [Google Scholar] [CrossRef]
- Frey, S.E.; Winokur, P.L.; Salata, R.A.; El-Kamary, S.S.; Turley, C.B.; Walter, E.B.; Hay, C.M.; Newman, F.K.; Hill, H.R.; Zhang, Y.; et al. Safety and immunogenicity of IMVAMUNE® smallpox vaccine using different strategies for a post event scenario. Vaccine 2013, 31, 3025–3033. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Hammad, E.; Hall, M.A.; Mahboob, A.; Zeina, S.; Elbanna, E.H.; Fadl, N.; Abdelmoneim, S.A.; ElMakhzangy, R.; Hammad, H.M.; et al. How can imported Monkeypox break the borders? A rapid systematic Review. Comp. Immunol. Microbiol. Infect. Dis. 2022; 101923, in press. [Google Scholar] [CrossRef]
- Sallam, M.; Ghazy, R.M.; Al-Salahat, K.; Al-Mahzoum, K.; AlHadidi, N.M.; Eid, H.; Kareem, N.; Al-Ajlouni, E.; Batarseh, R.; Ababneh, N.A.; et al. The Role of Psychological Factors and Vaccine Conspiracy Beliefs in Influenza Vaccine Hesitancy and Uptake among Jordanian Healthcare Workers during the COVID-19 Pandemic. Vaccines 2022, 10, 1355. [Google Scholar] [CrossRef] [PubMed]
- Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.W.C.; Liow, Y.; Loh, V.W.K.; Liew, S.J.; Chan, Y.-H.; Young, D. COVID-19 vaccine acceptance and hesitancy among primary healthcare workers in Singapore. BMC Prim. Care 2022, 23, 81. [Google Scholar] [CrossRef] [PubMed]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef] [PubMed]
- Ackah, M.; Ameyaw, L.; Gazali Salifu, M.; Afi Asubonteng, D.P.; Osei Yeboah, C.; Narkotey Annor, E.; Abena Kwartemaa Ankapong, E.; Boakye, H. COVID-19 vaccine acceptance among health care workers in Africa: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0268711. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Abd ElHafeez, S.; Elbarazi, I.; Shaaban, R.; ElMakhzangy, R.; Ossama Aly, M.; Alnagar, A.; Yacoub, M.; El Saeh, H.M.; Eltaweel, N.; Alqutub, S.T. Arabic validation and cross-cultural adaptation of the 5C scale for assessment of COVID-19 vaccines psychological antecedents. PLoS ONE 2021, 16, e0254595. [Google Scholar] [CrossRef]
- Betsch, C.; Habersaat, K.B.; Deshevoi, S.; Heinemeier, D.; Briko, N.; Kostenko, N.; Kocik, J.; Böhm, R.; Zettler, I.; Wiysonge, C.S. Sample study protocol for adapting and translating the 5C scale to assess the psychological antecedents of vaccination. BMJ Open 2020, 10, e034869. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Abd ElHafeez, S.; Shaaban, R.; Elbarazi, I.; Abdou, M.S.; Ramadan, A.; Kheirallah, K.A. Determining the cutoff points of the 5C scale for assessment of COVID-19 vaccines psychological antecedents among the Arab population: A multinational study. J. Prim. Care Comm. Health 2021, 12, 21501327211018568. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.Y.; Li, J.; Gao, R.D. 2022 Monkeypox outbreak: Why is it a public health emergency of international concern? What can we do to control it? World J. Clin. Cases 2022, 10, 10873–10881. [Google Scholar] [CrossRef] [PubMed]
- Uwishema, O.; Adekunbi, O.; Peñamante, C.A.; Bekele, B.K.; Khoury, C.; Mhanna, M.; Nicholas, A.; Adanur, I.; Dost, B.; Onyeaka, H. The burden of monkeypox virus amidst the Covid-19 pandemic in Africa: A double battle for Africa. Ann. Med. Surg. 2022, 80, 104197. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Statement at the Press Conference Following IHR Emergency Committee Regarding the Multi-Country Outbreak of Monkeypox—23 July 2022. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-statement-on-the-press-conference-following-IHR-emergency-committee-regarding-the-multi--country-outbreak-of-monkeypox--23-july-2022 (accessed on 25 July 2022).
- Al Awaidy, S.T.; Khamis, F.; Sallam, M.; Ghazy, R.M.; Zaraket, H. Monkeypox Outbreak: More queries posed as cases globally soar. Sultan Qaboos Univ. Med. J. 2022; online first. [Google Scholar] [CrossRef]
- Vyas, K.J.; Delaney, E.M.; Webb-Murphy, J.A.; Johnston, S.L. Psychological Impact of Deploying in Support of the U.S. Response to Ebola: A Systematic Review and Meta-Analysis of Past Outbreaks. Mil. Med. 2016, 181, e1515–e1531. [Google Scholar] [CrossRef] [Green Version]
- Raven, J.; Wurie, H.; Witter, S. Health workers’ experiences of coping with the Ebola epidemic in Sierra Leone’s health system: A qualitative study. BMC Health Serv. Res. 2018, 18, 251. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Abubakar Fiidow, O.; Abdullah, F.S.A.; Elbarazi, I.; Ismail, I.I.; Alqutub, S.T.; Bouraad, E.; Hammouda, E.A.; Tahoun, M.M.; Mehdad, S.; et al. Quality of life among health care workers in Arab countries 2 years after COVID-19 pandemic. Front. Public Health 2022, 10, 917128. [Google Scholar] [CrossRef]
- Ulloque-Badaracco, J.R.; Alarcón-Braga, E.A.; Hernandez-Bustamante, E.A.; Al-kassab-Córdova, A.; Benites-Zapata, V.A.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Acceptance towards Monkeypox Vaccination: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1248. [Google Scholar] [CrossRef]
- Gonzales-Zamora, J.; Soriano-Moreno, D.R.; Soriano-Moreno, A.N.; Ponce-Rosas, L.; Sangster-Carrasco, L.; De-Los-Rios-Pinto, A.; Benito-Vargas, R.M.; Murrieta-Ruiz, V.; Morocho-Alburqueque, N.; Caira-Chuquineyra, B. Level of Knowledge regarding Monkeypox among Peruvian Physicians during the 2022 Outbreak: A Cross-Sectional Study. Res. Sq. 2022, preprint, 1–21. [Google Scholar] [CrossRef]
- Alsanafi, M.; Al-Mahzoum, K.; Sallam, M. Monkeypox Knowledge and Confidence in Diagnosis and Management with Evaluation of Emerging Virus Infection Conspiracies among Health Professionals in Kuwait. Pathogens 2022, 11, 994. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Al-Tammemi, A.B.; Alkurtas, M.; Mirzaei, F.; Kareem, N.; Al-Naimat, H.; Jardaneh, L.; Al-Majali, L.; AlHadidi, A.; et al. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare 2022, 10, 1722. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Al-Mahzoum, K.; Dardas, L.A.; Al-Tammemi, A.B.; Al-Majali, L.; Al-Naimat, H.; Jardaneh, L.; AlHadidi, F.; Al-Salahat, K.; Al-Ajlouni, E.; et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina 2022, 58, 924. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, S.; Dost, B.; Terzi, O.; Koksal, E.; Kaya, C.; Ustun, Y.B.; Tulgar, S. Evaluation of Knowledge and Attitudes of Anesthesiology Specialists and Residents Toward Patients Infected with the Monkeypox Disease: A National Survey Study. Surg. Infect. 2022. online ahead of print. [Google Scholar] [CrossRef]
- World Health Organization. Vaccines and Immunization for Monkeypox: Interim Guidance. 16 November 2022. Available online: https://www.who.int/publications/i/item/WHO-MPX-Immunization (accessed on 27 November 2022).
- Osterholm, M.T.; Gellin, B. Confronting 21st-century monkeypox. Science 2022, 377, 349. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhu, Z.; He, Y.; Lim, J.W.; Lane, B.; Wang, H.; Peng, Q.; Sun, L.; Lu, H. Monkeypox claims new victims: The outbreak in men who have sex with men. Infect. Dis. Poverty 2022, 11, 84. [Google Scholar] [CrossRef]
- Titanji, B.K.; Tegomoh, B.; Nematollahi, S.; Konomos, M.; Kulkarni, P.A. Monkeypox: A Contemporary Review for Healthcare Professionals. Open Forum Infect. Dis. 2022, 9, ofac310. [Google Scholar] [CrossRef]
- Lulli, L.G.; Baldassarre, A.; Mucci, N.; Arcangeli, G. Prevention, Risk Exposure, and Knowledge of Monkeypox in Occupational Settings: A Scoping Review. Trop. Med. Infect. Dis. 2022, 7, 276. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Alzahrani, F.; Alarifi, A.M.; Algethami, M.R.; Alhumam, M.N.; Ayied, H.A.M.; Awan, A.Z.; Almutairi, A.F.; Bamakhrama, S.A.; Almushari, B.S.; et al. Assessment of Knowledge of Monkeypox Viral Infection among the General Population in Saudi Arabia. Pathogens 2022, 11, 904. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Pathog. Glob. Health 2020, 114, 68–75. [Google Scholar] [CrossRef]
- Youssef, D.; Abboud, E.; Kawtharni, M.; Zheim, Z.; Abou Arrage, N.; Youssef, J. When a neglected tropical zoonotic disease emerges in non-endemic countries: Need to proactively fill the unveiled knowledge gaps towards human monkeypox among the Lebanese population. Res. Sq. 2022, preprint, 1–39. [Google Scholar] [CrossRef]
- Sallam, M.; Eid, H.; Awamleh, N.; Al-Tammemi, A.A.B.; Barakat, M.; Athamneh, R.Y.; Hallit, S.; Harapan, H.; Mahafzah, A. Conspiratorial Attitude of the General Public in Jordan towards Emerging Virus Infections: A Cross-Sectional Study Amid the 2022 Monkeypox Outbreak. Trop. Med. Infect. Dis. 2022, 7, 411. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop. Med. Infect. Dis. 2022, 7, 135. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Physicians’ willingness to be vaccinated with a smallpox vaccine to prevent monkeypox viral infection: A cross-sectional study in Indonesia. Clin. Epidemiol. Glob. Health 2020, 8, 1259–1263. [Google Scholar] [CrossRef]
- Hong, J.; Pan, B.; Jiang, H.J.; Zhang, Q.M.; Xu, X.W.; Jiang, H.; Ye, J.E.; Cui, Y.; Yan, X.J.; Zhai, X.F. Willingness of Chinese healthcare workers to receive monkeypox vaccine and its independent predictors: A cross-sectional survey. J. Med. Virol. 2022, e28294, online ahead of print. [Google Scholar] [CrossRef]
- Bates, B.R.; Grijalva, M.J. Knowledge, attitudes, and practices towards monkeypox during the 2022 outbreak: An online cross-sectional survey among clinicians in Ohio, USA. J. Infect. Public Health 2022, 15, 1459–1465. [Google Scholar] [CrossRef]
- Riad, A.; Drobov, A.; Rozmarinová, J.; Drapáčová, P.; Klugarová, J.; Dušek, L.; Pokorná, A.; Klugar, M. Monkeypox Knowledge and Vaccine Hesitancy of Czech Healthcare Workers: A Health Belief Model (HBM)-Based Study. Vaccines 2022, 10, 2022. [Google Scholar] [CrossRef]
- Elbarazi, I.; Yacoub, M.; Reyad, O.A.; Abdou, M.S.; Elhadi, Y.A.M.; Kheirallah, K.A.; Ababneh, B.F.; Hamada, B.A.; El Saeh, H.M.; Ali, N. Exploring enablers and barriers toward COVID-19 vaccine acceptance among Arabs: A qualitative study. Int. J. Disaster Risk Reduct. 2022, 82, 103304. [Google Scholar] [CrossRef]
- Poland, G.A.; Kennedy, R.B.; Tosh, P.K. Prevention of monkeypox with vaccines: A rapid review. Lancet Infect. Dis. 2022, 22, e349–e358. [Google Scholar] [CrossRef]
- Ecarnot, F.; Crepaldi, G.; Juvin, P.; Grabenstein, J.; Del Giudice, G.; Tan, L.; O’Dwyer, S.; Esposito, S.; Bosch, X.; Gavazzi, G.; et al. Pharmacy-based interventions to increase vaccine uptake: Report of a multidisciplinary stakeholders meeting. BMC Public Health 2019, 19, 1698. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Sudarmaji, N.; Kifli, N.; Hermansyah, A.; Yeoh, S.F.; Goh, B.H.; Ming, L.C. Prevention and Treatment of Monkeypox: A Systematic Review of Preclinical Studies. Viruses 2022, 14, 2496. [Google Scholar] [CrossRef]
- Kwon, S.L.; Ban, S.; Shin, J.; Bae, H.; Park, H.; Kwon, G.Y. Monkeypox Vaccination in the Republic of Korea: Identifying the High-Risk Target Group. J. Korean Med. Sci. 2022, 37, e239. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Baptista, S.; Naidoo, S.; Suliman, S.; Nepolo, E.; Kanoi, B.N.; Gitaka, J.; Blessing, O.M.; Enany, S. COVID-19 vaccinology landscape in Africa. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef]
- Wang, T.L.; Jing, L.; Bocchini, J.A., Jr. Mandatory influenza vaccination for all healthcare personnel: A review on justification, implementation and effectiveness. Curr. Opin. Pediatr. 2017, 29, 606–615. [Google Scholar] [CrossRef]
- Savulescu, J. Good reasons to vaccinate: Mandatory or payment for risk? J. Med. Ethics 2021, 47, 78. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Frequency (%) (N = 389) |
|---|---|
| Age | |
| Median | 37 (IQR) 1: 28–48 |
| Range | 18–68 |
| Gender | |
| Male | 211 (54.2) |
| Female | 169 (43.4) |
| Prefer not to say | 9 (2.3) |
| Nationality | |
| Nigerian | 386 (99.1) |
| Dominican | 1 (0.3) |
| Cuban | 1 (0.3) |
| Spanish | 1 (0.3) |
| Marital status | |
| Having a partner | 25 (6.4) |
| Married | 236 (60.7) |
| Single | 115 (29.6) |
| Widow | 13 (3.3) |
| Living area | |
| Urban | 358 (92.0) |
| Rural | 31 (8.0) |
| Financial status | |
| Low-income | 247 (63.5) |
| Middle-income | 118 (30.3) |
| High-income | 19 (4.9) |
| Missing | 5 (1.3) |
| Education | |
| Pre-college/High school | 39 (10.0) |
| Professional/technical | 53 (13.6) |
| Undergraduate (Bachelor) | 148 (38.0) |
| Diploma | 48 (12.3) |
| Postgraduate (Master) | 74 (19.0) |
| Postgraduate (PhD) | 27 (6.9) |
| Chronic diseases | |
| Yes | 44 (11.3) |
| No | 345 (88.7) |
| Have you had monkeypox? | |
| Yes | 32 (8.2) |
| No | 316 (81.2) |
| I do not know | 41 (10.5) |
| Has anyone that you know of died due to monkeypox? | |
| Yes | 16 (4.1) |
| No | 232 (59.6) |
| I do not know | 141 (36.2) |
| Variables | Confidence N (%) | Complacency N (%) | Constraints N (%) | Calculation N (%) | Collective Responsibility N (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | OR (95% CI) p-Value | Yes | No | OR (95% CI) p-Value | Yes | No | OR (95% CI) p-Value | Yes | No | OR (95% CI) p-Value | Yes | No | OR (95% CI) p-Value | |
| Gender | 1.11 (0.72–1.71) 0.630 | 0.81 (0.54–1.21) 0.305 | 1.36 (0.89–2.06) 0.155 | 0.80 (0.51–1.26) 0.343 | 0.76 (0.49–1.1) 0.198 | ||||||||||
| Male | 151 (69.9) | 65 (30.1) | 85 (39.4) | 131 (60.6) | 85 (39.4) | 131 (60.6) | 153 (70.8) | 63 (29.2) | 139 (64.4) | 77 (35.6) | |||||
| Female ref. | 117 (67.6) | 56 (32.4) | 77 (44.5) | 96 (55.5) | 56 (32.4) | 117 (67.6) | 130 (75.1) | 43 (24.9) | 122 (70.5) | 51 (29.5) | |||||
| Age | 0.215 | 0.617 | 0.561 | 0.085 | 0.008 * | ||||||||||
| 18–30 ref. | 93 (73.2) | 34 (26.8) | 50 (39.4) | 77 (60.6) | 48 (37.8) | 79 (62.2) | 102 (80.3) | 25 (19.7) | 76 (59.8) | 51 (40.2) | |||||
| 31–45 | 101 (67.8) | 48 (32.2) | 0.77 (0.46–1.29) | 66 (44.3) | 83 (55.7) | 1.23 (0.76–1.98) | 55 (36.9) | 94 (63.1) | 0.96 (0.59–1.57) | 105 (70.5) | 44 (29.5) | 0.59 (0.33–1.03) | 113 (75.8) | 36 (24.2) | 2.11 (1.26–3.53) |
| 46–60 | 60 (62.5) | 36 (37.5) | 0.61 (0.35–1.08) | 41 (42.7) | 55 (57.3) | 1.15 (0.67–1.97) | 30 (31.3) | 66 (68.8) | 0.75 (0.43–1.31) | 63 (65.6) | 33 (34.4) | 0.47 (0.26–0.86) | 58 (60.4) | 38 (39.6) | 1.02 (0.59–1.76) |
| >60 | 14 (82.4) | 3 (17.6) | 1.71 (0.46–6.31) | 5 (29.4) | 12 (70.6) | 0.64 (0.21–1.93) | 8 (47.1) | 9 (52.9) | 1.46 (0.53–4.05) | 13 (76.5) | 4 (23.5) | 0.79 (0.24–2.65) | 14 (82.4) | 3 (17.6) | 3.13 (0.86–11.45) |
| Marital Status | 0.034 * | 0.495 | 0.780 | 0.372 | 0.714 | ||||||||||
| Having partner | 15 (60.0) | 10 (40.0) | 2.40 (0.61–9.49) | 9 (36.0) | 16 (64.0) | 1.88 (0.41–8.63) | 9 (36.0) | 16 (64.0) | 0.90 (0.23–3.59) | 17 (68.0) | 8 (32.0) | 1.33 (0.33–5.38) | 15 (60.0) | 10 (40.0) | 0.94 (0.24–3.71) |
| Married | 162 (68.6) | 74 (31.4) | 3.50 (1.11–11.07) | 102 (43.2) | 134 (56.8) | 2.54 (0.68–9.46) | 81 (34.3) | 155 (65.7) | 0.84 (0.27–2.64) | 168 (71.2) | 68 (28.8) | 1.54 (0.49–4.89) | 163 (69.1) | 73 (30.9) | 1.40 (0.44–4.41) |
| Single | 86 (74.8) | 29 (25.2) | 4.75 (1.44–15.66) | 48 (41.7) | 67 (58.3) | 2.39 (0.62–9.14) | 46 (40.0) | 69 (60.0) | 1.07 (0.33–3.46) | 90 (78.3) | 25 (21.7) | 2.25 (0.68–7.49) | 75 (65.2) | 40 (34.8) | 1.17 (0.36–3.82) |
| Widow ref. | 5 (38.5) | 8 (61.5) | 3 (23.1) | 10 (76.9) | 5 (38.5) | 8 (61.5) | 8 (61.5) | 5 (38.5) | 8 (61.5) | 5 (38.5) | |||||
| Living area | 0.030 * 2.23 (1.06–4.67) | 0.269 1.55 (0.71–3.39) | 0.207 1.70 (0.74–3.91) | 0.147 0.49 (0.18–1.31) | 0.056 2.03 (0.97–4.26) | ||||||||||
| Urban | 252 (70.4) | 106 (29.6) | 152 (42.5) | 206 (57.5) | 133 (37.2) | 225 (62.8) | 257 (71.8) | 101 (28.2) | 245 (68.4) | 113 (31.6) | |||||
| Rural ref. | 16 (51.6) | 15 (48.4) | 10 (32.3) | 21 (67.7) | 8 (25.8) | 23 (74.2) | 26 (83.9) | 5 (16.1) | 16 (51.6) | 15 (48.4) | |||||
| Financial Status | 0.043 * | 0.013 * | 0.127 | 0.695 | 0.009 * | ||||||||||
| Low-income ref. | 161 (64.9) | 87 (35.1) | 117 (47.2) | 131 (52.8) | 99 (39.9) | 149 (60.1) | 179 (72.2) | 69 (27.8) | 153 (61.7) | 95 (38.3) | |||||
| Middle-income | 89 (74.2) | 31 (25.8) | 1.55 (0.96–2.52) | 39 (32.5) | 81 (67.5) | 0.54 (0.34–0.85) | 35 (29.2) | 85 (70.8) | 0.62 (0.39–0.99) | 87 (72.5) | 33 (27.5) | 1.02 (0.62–1.66) | 93 (77.5) | 27 (22.5) | 2.14 (1.30–3.52) |
| High-income | 18 (85.7) | 3 (14.3) | 3.24 (0.93–11.31) | 6 (28.6) | 15 (71.4) | 0.45 (0.17–1.19) | 7 (33.3) | 14 (66.7) | 0.75 (0.29–1.93) | 17 (81.0) | 4 (19.0) | 1.64 (0.53–5.04) | 15 (71.4) | 6 (28.6) | 1.55 (0.58–4.14) |
| Education | 0.001 * | 0.177 | 0.578 | 0.175 | 0.001 * | ||||||||||
| Pre-college/High school ref. | 15 (38.5) | 24 (61.5) | 12 (30.8) | 27 (69.2) | 15 (38.5) | 24 (61.5) | 33 (84.6) | 6 (15.4) | 13 (33.3) | 26 (66.7) | |||||
| Professional/technical | 38 (71.7) | 15 (28.3) | 4.05 (1.68–9.77) | 25 (47.2) | 28 (52.8) | 2.01 (0.84–4.79) | 19 (35.8) | 34 (64.2) | 0.89 (0.38–2.10) | 37 (69.8) | 16 (30.2) | 0.42 (0.15–1.20) | 34 (64.2) | 19 (35.8) | 3.58 (1.50–8.55) |
| Bachelor | 103 (69.6) | 45 (30.4) | 3.66 (1.76–7.63) | 67 (45.3) | 81 (54.7) | 1.86 (0.88–3.95) | 59 (39.9) | 89 (60.1) | 1.06 (0.51–2.19) | 101 (68.2) | 47 (31.8) | 0.39 (0.15–0.99) | 110 (74.3) | 38 (25.7) | 5.79 (2.71–12.39) |
| Post-graduate studies | 112 (75.2) | 37 (24.8) | 4.84 (2.30–10.20) | 58 (38.9) | 91 (61.1) | 1.43 (0.67–3.05) | 48 (32.2) | 101 (67.8) | 0.76 (0.37–1.58) | 37 (24.8) | 112 (75.2) | 0.55 (0.21–1.42) | 104 (69.8) | 45 (30.2) | 4.62 (2.18–9.81) |
| Chronic diseases | 0.001 * 2.76 (1.46–5.22) | 0.280 1.44 (0.74–2.77) | 0.516 1.25 (0.64–2.44) | 0.716 1.14 (0.57–2.27) | 0.026 * 2.03 (1.08–3.83) | ||||||||||
| Yes ref. | 21 (47.7) | 23 (52.3) | 15 (34.1) | 29 (65.9) | 14 (31.8) | 30 (68.2) | 31 (70.5) | 13 (29.5) | 23 (52.3) | 21 (47.7) | |||||
| No | 247 (71.6) | 98 (28.4) | 147 (42.6) | 198 (57.4) | 127 (36.8) | 218 (63.2) | 252 (73.0) | 93 (27.0) | 238 (69.0) | 107 (31.0) | |||||
| Have you had MPX? | 0.0183.41 (1.17–9.96) | 0.105 0.52 (0.24–1.16) | 0.539 0.78 (0.36–1.71) | 0.123 2.13 (0.80–5.69) | 0.030 * 2.84 (1.07–7.56) | ||||||||||
| Yes | 28 (87.5) | 4 (12.5) | 9 (28.1) | 23 (71.9) | 10 (31.3) | 22 (68.8) | 27 (84.4) | 5 (15.6) | 27 (84.4) | 5 (15.6) | |||||
| No/I do not know ref. | 240 (67.2) | 117 (32.8) | 153 (42.9) | 204 (57.1) | 131 (36.7) | 226 (63.3) | 256 (71.7) | 101 (28.3) | 234 (65.5) | 123 (34.5) | |||||
| Knowing anyone who died due to MPX | 0.165 3.28 (0.73–14.66) | 0.016 * 0.19 (0.04–0.85) | 0.137 0.39 (0.11–1.40) | 0.837 1.13 (0.36–3.58) | 0.346 0.62 (0.23–1.70) | ||||||||||
| Yes | 14 (87.5) | 2 (12.5) | 2 (12.5) | 14 (87.5) | 3 (18.8) | 13 (81.2) | 12 (75.0) | 4 (25.0) | 9 (56.3) | 7 (43.8) | |||||
| No/I do not know ref. | 254 (68.1) | 119 (31.9) | 160 (42.9) | 213 (57.1) | 138 (37.0) | 235 (63.0) | 271 (72.7) | 102 (27.3) | 252 (67.6) | 121 (32.4) | |||||
| 5C Domain, Variables | Category | OR | 95% CI | p Value |
|---|---|---|---|---|
| Confidence | ||||
| Marital Status | 0.025 * | |||
| Widow | 1 | |||
| Having partner | 1.8 | (0.37–8.71) | 0.465 | |
| Married | 2.73 | (0.72–10.40) | 0.142 | |
| Single | 5.07 | (1.26–20.34) | 0.022 * | |
| Living area | ||||
| Rural | 1 | |||
| Urban | 1.63 | (0.68–3.88) | 0.274 | |
| Financial Status | 0.107 | |||
| Low-income | 1 | |||
| Middle-income | 1.42 | (0.83–2.44) | 0.205 | |
| High-income | 3.7 | (0.96–14.07) | 0.058 | |
| Education | 0.015 * | |||
| Pre-college/High school | 1 | |||
| Professional/technical | 4.12 | (1.57–10.73) | 0.004 * | |
| Undergraduate | 2.94 | (1.32–6.55) | 0.008 * | |
| Postgraduate degree | 3.48 | (1.51–8.04) | 0.003 * | |
| Chronic diseases | Yes | 1 | ||
| No | 2.57 | (1.27–5.22) | 0.009 * | |
| Have you had MPX? | No or do not know | 1 | ||
| Yes | 2.3 | (0.76–6.99) | 0.141 | |
| Knowing anyone who died due to MPX | ||||
| No or do not know | 1 | |||
| Yes | 2.68 | (0.57–12.67) | 0.212 | |
| Complacency | ||||
| Income | 0.017 * | |||
| Low-income | 1 | |||
| Middle-income | 0.53 | (0.33–0.89) | 0.008 * | |
| High-income | 0.46 | (0.16–1.25) | 0.123 | |
| Education | 0.161 | |||
| Pre-college/High school | 1 | |||
| Professional/technical | 2.37 | (0.99–5.72) | 0.054 | |
| Undergraduate | 2.37 | (1.10–5.11) | 0.027 * | |
| Postgraduate degree | 2.17 | (0.99–4.79) | 0.054 | |
| Have you had MPX? | ||||
| No or do not know | 1 | 0.271 | ||
| 0.63 | (0.27–1.44) | |||
| Yes | ||||
| Knowing anyone died due to MPX | ||||
| No or do not know | 1 | |||
| Yes | 0.2 | (0.05–0.93) | 0.040 * | |
| Constraints | ||||
| Gender | ||||
| Female | 1 | |||
| Male | 1.36 | (0.89–2.08) | 0.156 | |
| Living Area | ||||
| Rural | 1 | |||
| Urban | 1.71 | (0.74–3.98) | 0.210 | |
| Financial Status | ||||
| Low-income | 1 | 0.132 | ||
| Middle-income | 0.62 | (0.39–0.99) | 0.046 * | |
| High-income | 0.77 | (0.30–2.00) | 0.593 | |
| Knowing anyone who died due to MPX | ||||
| No or do not know | 1 | |||
| Yes | 0.43 | (0.12–1.56) | 0.200 | |
| Calculation | 0.251 | |||
| Age | ||||
| 18–30 | 1 | |||
| 31–45 | 0.69 | (0.386–1.24) | 0.214 | |
| 46–60 | 0.52 | (0.27–0.98) | 0.044 * | |
| >60 | 0.75 | (0.21–2.64) | 0.654 | |
| Living area | ||||
| Rural | 1 | |||
| Urban | 0.59 | (0.21–1.63) | 0.309 | |
| Education | 0.267 | |||
| Pre-college/High school | 1 | |||
| Professional/technical | 0.49 | (0.17–1.44) | 0.195 | |
| Undergraduate | 0.48 | (0.18–1.27) | 0.138 | |
| Postgraduate degree | 0.72 | (0.26–1.96) | 0.520 | |
| Have you had MPX? | ||||
| No or do not know | 1 | |||
| Yes | 2.03 | (0.75–5.51) | 0.163 | |
| Collective responsibility | ||||
| Age | 0.008 * | |||
| 18–30 | 1 | |||
| 31–45 | 1.74 | (0.99– 3.06) | 0.056 | |
| 46–60 | 0.67 | (0.36–1.24) | 0.201 | |
| >60 | 3.19 | (0.55–18.45) | 0.195 | |
| Living area | ||||
| Rural | 1 | |||
| Urban | 1.41 | (0.6–3.32) | 0.431 | |
| Financial Status | 0.031 * | |||
| Low-income | 1 | |||
| Middle-income | 2.1 | (1.19–3.69) | 0.010 * | |
| High-income | 0.91 | (0.22–3.72) | 0.890 | |
| Education | 0.006 * | |||
| Pre-college/High school | 1 | |||
| Professional/technical | 2.44 | (0.97–6.17) | 0.057 | |
| Undergraduate | 4.17 | (1.85–9.38) | 0.001 * | |
| Postgraduate degree | 3.45 | (1.50–7.90) | 0.003 * | |
| Chronic diseases | ||||
| Yes | 1 | |||
| No | 1.82 | (0.899–3.673) | 0.096 | |
| Have you had MPX? | ||||
| No or do not know | 1 | |||
| Yes | 2.01 | (0.69–5.82) | 0.198 | |
| Knowing anyone who died due to MPX | ||||
| No or do not know | 1 | |||
| Yes | 0.42 | (0.14–1.29) | 0.118 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghazy, R.M.; Okeh, D.U.; Sallam, M.; Hussein, M.; Ismail, H.M.; Yazbek, S.; Mahboob, A.; Abd ElHafeez, S. Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria. Vaccines 2022, 10, 2151. https://doi.org/10.3390/vaccines10122151
Ghazy RM, Okeh DU, Sallam M, Hussein M, Ismail HM, Yazbek S, Mahboob A, Abd ElHafeez S. Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria. Vaccines. 2022; 10(12):2151. https://doi.org/10.3390/vaccines10122151
Chicago/Turabian StyleGhazy, Ramy Mohamed, Debra Ukamaka Okeh, Malik Sallam, Mai Hussein, Horeya M. Ismail, Saja Yazbek, Amira Mahboob, and Samar Abd ElHafeez. 2022. "Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria" Vaccines 10, no. 12: 2151. https://doi.org/10.3390/vaccines10122151
APA StyleGhazy, R. M., Okeh, D. U., Sallam, M., Hussein, M., Ismail, H. M., Yazbek, S., Mahboob, A., & Abd ElHafeez, S. (2022). Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria. Vaccines, 10(12), 2151. https://doi.org/10.3390/vaccines10122151