
Predictors of Survival after Vaccination in a Pneumonic Plague Model

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Challenge
2.3. Immunoassay
2.4. Survival and Immunogenicity Statistical Analysis
2.5. Statistical Modelling
3. Results
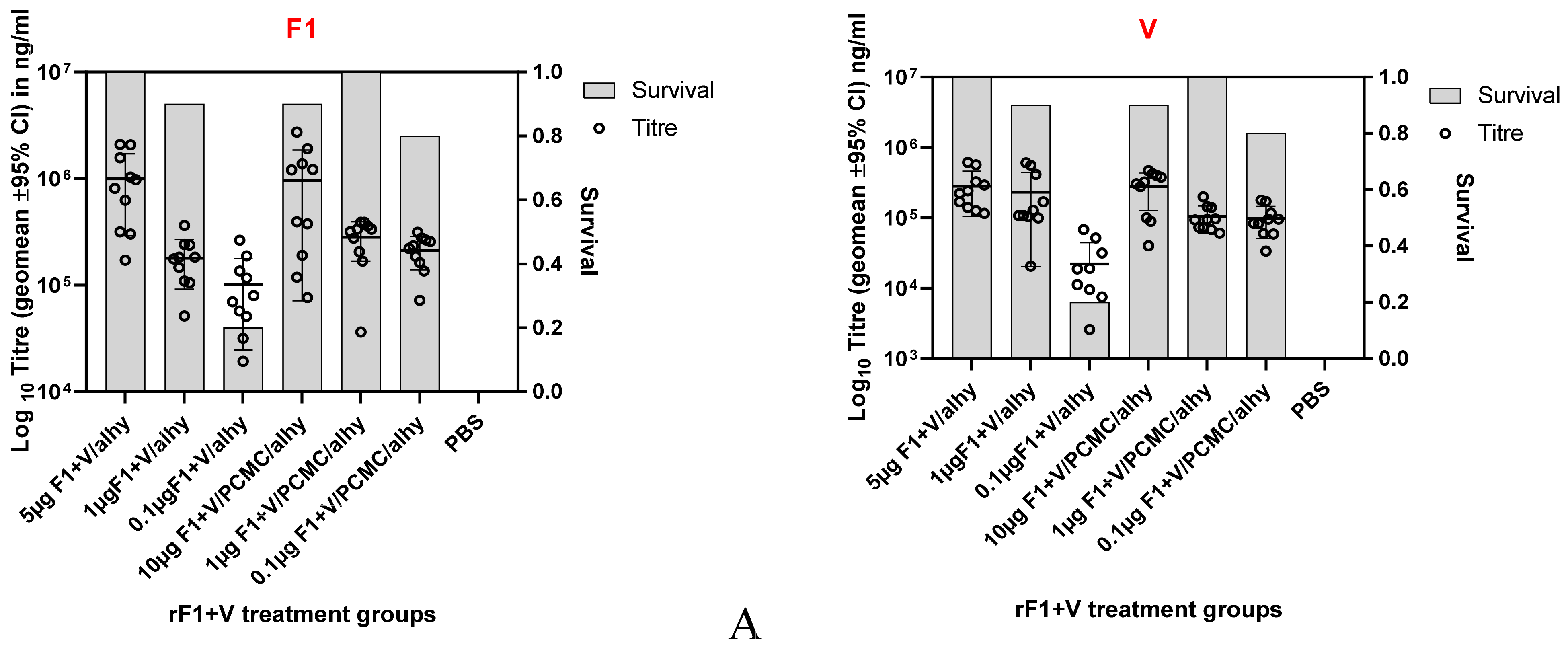
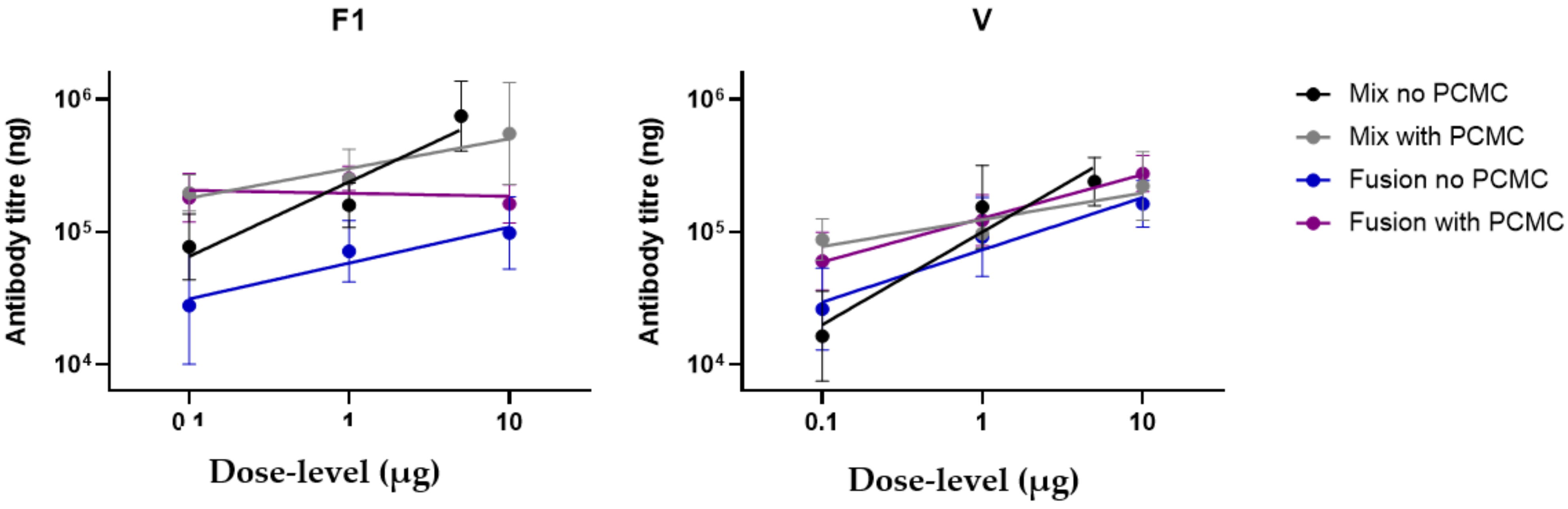
3.1. Induction of Dose-Related Immune Responses
3.2. Survival of Immunised Mice against Aerosol Challenge with Y. pestis
3.3. Factors That Influence Survival in Immunised Mice Challenged with Y. pestis
3.4. Factors That Influence the Antibody Response in Immunised Mice
3.5. Antibody Titres towards F1 and V Antigens Predict Survival with Challenge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Global Plague Statistics. Available online: https://www.who.int/health-topics/plague (accessed on 12 July 2021).
- Sagiyev, Z.; Berdibekov, A.; Bolger, T.; Merekenova, A.; Ashirova, S.; Nurgozhin, Z.; Dalibayev, Z. Human response to live plague vaccine EV, Almaty region, Kazakhstan, 2014–2015. PLoS ONE 2019, 14, e0218366. [Google Scholar] [CrossRef] [Green Version]
- Hawgood, B.J. Waldemar Mordecai Haffkine, CIE (1860–1930): Prophylactic vaccination against cholera and bubonic plague in British India. J. Med. Biogr. 2007, 15, 9–19. [Google Scholar] [CrossRef]
- Williamson, E.D.; Eley, S.M.; Griffin, K.F.; Green, M.; Russell, P.; Leary, S.E.C.; Oyston, P.C.F.; Easterbrook, T.; Reddin, K.M.; Robinson Titball, R.W. A new impoved sub-unit vaccine for plague: The basis of protection. FEMS Immunol. Med. Micro. 1995, 12, 223–230. [Google Scholar] [CrossRef]
- Williamson Eley, S.M.; Stagg, A.J.; Green, M.; Russell, P.; Titball, R.W. A sub-unit vaccine elicits IgG in serum, spleen cell cultures and bronchial washings and protects immunised animals against pneumonic plague. Vaccine 1997, 15, 1079–1084. [Google Scholar] [CrossRef]
- Russell, P.; Eley, S.; Hibbs, S.; Manchee, R.; Stagg, A.; Titball, R. A comparison of Plague vaccine, USP and EV76 vaccine induced protection against Yersinia pestis in a murine model. Vaccine 1995, 13, 1551–1556. [Google Scholar] [CrossRef]
- WHO R&D Blueprint: Plague Vaccines Workshop April 2018. Available online: https://www.who.int/blueprint/what/norms-standards/Plague_vaccines_workshop-23-april-2018/en/ (accessed on 12 July 2021).
- Sun, W.; Singh, A.K. Plague vaccines: Recent progress and prospects. NPJ Vaccines 2019, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- Williamson, E.D. Oyston PFC. In Plotkin’s Vaccines, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Demeure, C.; Dussurget, O.; Fiol, G.M.; Le Guern, A.-S.; Savin, C.; Pizarro-Cerdá, J. Yersinia pestis and plague: An updated view on evolution, virulence determinants, immune subversion, vaccination and diagnostics. Microbes Infect. 2019, 21, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Dentovskaya, S.V.; Kopylov, P.K.; Ivanov, S.A.; Ageev, S.A.; Anisimov, A.P. Molecular bases of vaccine-prevention of plague. Mol. Genet. Microbiol. Virol. 2013, 28, 87–98. [Google Scholar] [CrossRef]
- Andersson, J.A.; Sha, J.; Erova, T.E.; Fitts, E.C.; Ponnusamy, D.; Kozlova, E.V.; Kirtley, M.L.; Chopra, A.K. Identification of New Virulence Factors and Vaccine Candidates for Yersinia pestis. Front. Cell. Infect. Microbiol. 2017, 7, 448. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhang, X.; Zhou, D.; Yang, R. Live-attenuatedYersinia pestisvaccines. Expert Rev. Vaccines 2013, 12, 677–686. [Google Scholar] [CrossRef] [PubMed]
- WHO. Plague Outbreak in Madagascar: External Situation Report 14, 4 December 2017. Available online: Afro.who.int/health-topics/plague/plague-outbreak-situation-reports (accessed on 12 July 2021).
- Smiley, S.T. Immune defense against pneumonic plague. Immunol. Rev. 2008, 225, 256–271. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Thompson, K.; Francis, M.S. Environmental Regulation of Yersinia Pathophysiology. Front. Cell. Infect. Microbiol. 2016, 6, 25. [Google Scholar] [CrossRef] [Green Version]
- Plano, G.V.; Schesser, K. The Yersinia pestis type III secretion system: Expression, assembly and role in the evasion of host defenses. Immunol. Res. 2013, 57, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, G.R. The type III injectisome. Nat. Rev. Microbiol. 2006, 4, 811–825. [Google Scholar] [CrossRef]
- Feodorova, V.A.; Motin, V.L. Current developments and future prospects. Emerg. Microbes Infect. 2012, 1, 1–5. [Google Scholar] [CrossRef]
- Williamson, E.D.; Flick Smith, H.C.; Waters, E.L.; Miller, J.; Hodgson, I.; Smith, S.; LeButt, C.S.; Hill, J. Immunogenicity of the rF1+rV vaccine with the identification of potential immune correlates of protection. Microb. Pathogen. 2007, 42, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Heath, D.G.; Anderson, G.W.; Mauro, J.; Welkos, S.; Andrews, G.P.; Adamovicz, J.; Friedlander, A.M. Protection against experimental bubonic and pneumonic plague by a recombinant capsular F1-V antigen fusion protein vaccine. Vaccine 1998, 16, 1131–1137. [Google Scholar] [CrossRef]
- Williamson, E.D.; Packer, P.J.; Waters, E.L.; Simpson, A.J.; Dyer, D.; Hartings, J.; Twenhafel, N.; Pitt, M.L.M. Recombinant (F1 + V) vaccine protects cynomolgus macaques against pneumonic plague. Vaccine 2011, 29, 4771–4777. [Google Scholar] [CrossRef] [PubMed]
- Fellows, P.; Price, J.; Martin, S.; Metcalfe, K.; Krile, R.; Barnewall, R.; Hart, M.K.; Lockman, H. Characterization of a Cynomolgus Macaque Model of Pneumonic Plague for Evaluation of Vaccine Efficacy. Clin. Vaccine Immunol. 2015, 22, 1070–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fellows, P.; Adamovicz, J.; Hartings, J.; Sherwood, R.; Mega, W.; Brasel, T.; Barr, E.; Holland, L.; Lin, W.; Rom, A.; et al. Protection in mice passively immunized with serum from cynomolgus macaques and humans vaccinated with recombinant plague vaccine (rF1V). Vaccine 2010, 28, 7748–7756. [Google Scholar] [CrossRef] [PubMed]
- Quenee, L.E.; Ciletti, N.A.; Elli, D.; Hermanas, T.M.; Schneewind, O. Prevention of pneumonic plague in mice, rats, guinea pigs and non-human primates with clinical grade rV10, rV10-2 or F1-V vaccines. Vaccine 2011, 29, 6572–6583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, E.D.; Flick-Smith, H.C.; LeButt, C.; Rowland, C.A.; Jones, S.M.; Waters, E.L.; Gwyther, R.J.; Miller, J.; Packer, P.J.; Irving, M. Human Immune Response to a Plague Vaccine Comprising Recombinant F1 and V Antigens. Infect. Immun. 2005, 73, 3598–3608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, S.R. Development of a recombinant vaccine against aerosolised plague. Vaccine 2007, 25, 3115–3117. [Google Scholar] [CrossRef]
- Hart, M.K.; Saviolakis, G.A.; Welkos, S.L.; House, R.V. Advanced Development of the rF1V and rBV A/B Vaccines: Progress and Challenges. Adv. Prev. Med. 2011, 2012, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, K.B.; Mehta, S. The clinical development process for a novel preventive vaccine: An overview. J. Postgrad. Med. 2016, 62, 4–11. [Google Scholar] [CrossRef]
- Moore, B.D.; New, R.R.C.; Butcher, W.; Mahood, R.; Steward, J.; Bayliss, M.; Macleod, C.; Bogus, M.; Williamson, E.D. Dual route vaccination for plague with emergency use applications. Vaccine 2018, 36, 5210–5217. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Asokanathan, C.; Kmiec, D.; Irvine, J.; Fleck, R.; Xing, D.; Moore, B.; Parton, R.; Coote, J. Protein coated microcrystals formulated with model antigens and modified with calcium phosphate exhibit enhanced phagocytosis and immunogenicity. Vaccine 2014, 32, 4234–4242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Drug Administration, HHS. 21CFR 601.90-Evidence needed to demonstrate effectiveness of new drugs when human efficacy studies are not ethical or feasible. Fed. Regist. 2002, 67, 37988–37998. [Google Scholar]
- Fellows, P.; Lin, W.; Detrisac, C.; Hu, S.-C.; Rajendran, N.; Gingras, B.; Holland, L.; Price, J.; Bolanowski, M.; House, R.V. Establishment of a Swiss Webster Mouse Model of Pneumonic Plague to Meet Essential Data Elements under the Animal Rule. Clin. Vaccine Immunol. 2012, 19, 468–476. [Google Scholar] [CrossRef]
- Nolan, T.; Bernstein, H.; Blatter, M.M.; Bromberg, K.; Guerra, F.; Kennedy, W.; Pichichero, M.; Senders, S.D.; Trofa, A.; Collard, A.; et al. Immunogenicity and safety of an inactivated hepatitis A vaccine administered concomitantly with diphtheria–tetanus–acellular pertussis and haemophilus influenzae type B vaccines to children less than 2 years of age. Pediatrics 2006, 118, 602–609. [Google Scholar] [CrossRef]
- Jones, S.M.; Day, F.; Stagg, A.J.; Williamson, E.D. Protection conferred by a fully recombinant sub-unit vaccine against Yer-sinia pestis in male and female mice of four inbred strains. Vaccine 2001, 19, 358–366. [Google Scholar] [CrossRef]
- Mandrekar, J.N. ROC curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, E.D.; Westlake, G.E. Vaccines for emerging pathogens: Prospects for licensure. Review series on Vaccines for emerging pathogens: From research to the clinic Part 1. Clin. Exp. Immunol. 2019, 198, 170–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, N.J.; Martin, J.E.; Graham, B.S.; Nabel, G.J. Correlates of protective immunity for Ebola vaccines: Implications for regulatory approval by the animal rule. Nat. Rev. Genet. 2009, 7, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Burns, D.L. Licensure of vaccines using the Animal Rule. Curr. Opin. Virol. 2012, 2, 353–356. [Google Scholar] [CrossRef]
- Beasley, D.W.C.; Brasel, T.L.; Comer, E.J. First vaccine approval under the FDA Animal Rule. NPJ Vaccines 2016, 1, 16013. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group ID | Number of Mice | Vaccine Type and Formulation | Vaccine Concentration: Dose Level of Each Protein Antigen (F1 and V) or of the Fusion Protein in µg/Mouse | Prime | Boost | Died | % Survival | Culturable Y. pestis in Spleens Post Mortem |
|---|---|---|---|---|---|---|---|---|
| (Day 0) | (Day 21) | |||||||
| A | 10 | rF1 + rV/alhydrogel | 5 * | SC | SC | 0 | 100 | 0 |
| B | 10 | 1 | 1 | 90 | 1 | |||
| C | 10 | 0.1 | 8 | 20 | 8 | |||
| D | 10 | rF1 + rV (PCMC/alhydrogel) | 10 | SC | SC | 1 | 90 | 1 |
| E | 10 | 1 | 0 | 100 | 0 | |||
| F | 10 | 0.1 | 2 | 80 | 2 | |||
| G | 10 | rF1V fusion/alhydrogel | 10 | SC | SC | 1 | 90 | 2 |
| H | 10 | 1 | 4 | 60 | 4 | |||
| I | 10 | 0.1 | 10 | 0 | 9 | |||
| J | 10 | rF1V fusion (PCMC/alhydrogel) | 10 | SC | SC | 0 | 100 | 0 |
| K | 10 | 1 | 0 | 100 | 0 | |||
| L | 10 | 0.1 | 1 | 90 | 1 | |||
| M | 15 | PBS | NA | SC | SC | 15 | 0 | 15 |
| Group | No. Dead/No. in Group | Kaplan–Meier Median Time to Death in Hours (95% Confidence Interval) | Overall Log-Rank Test p-Value | Pairwise Log-Rank Test p-Value | Bonferroni–Holm Adjusted Log-Rank Test p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| B | C | M | B | C | M | ||||
| A | 0/10 | NA | <0.0001 * | 0.3173 | 0.0002 * | <0.0001 * | 1.0000 | 0.0143 * | <0.0001 * |
| B | 1/10 | --- (120.35, ---) | - | 0.0012 * | <0.0001 * | - | 0.0661 | <0.0001 * | |
| C | 8/10 | 109.07 (91.18, 235.78) | - | <0.0001 * | - | - | 0.0004 * | ||
| M (control) | 15/15 | 61.85 (60.60, 66.67) | - | - | - | - | - | - | |
| E | F | M | E | F | M | ||||
| D | 1/10 | --- (96.47, ---) | <0.0001 * | 0.3173 | 0.5842 | <0.0001 * | 1.0000 | 1.0000 | <0.0001 * |
| E | 0/10 | NA | - | 0.1464 | <0.0001 * | - | 1.0000 | <0.0001 * | |
| F | 2/10 | --- (107.78, ---) | - | - | <0.0001 * | - | - | <0.0001 * | |
| M (control) | 15/15 | 61.85 (60.60, 66.67) | - | - | - | - | - | - | |
| H | I | M | H | I | M | ||||
| G | 1/10 | --- (96.50, ---) | <0.0001 * | 0.1469 | <0.0001 * | <0.0001 * | 1.0000 | 0.0017 * | <0.0001 * |
| H | 4/10 | --- (91.53, ---) | - | 0.0005 * | <0.0001 * | - | 0.0308 * | 0.0001 * | |
| I | 10/10 | 96.34 (60.82, 108.27) | - | - | 0.0001 * | - | - | 0.0087 * | |
| M (control) | 15/15 | 61.85 (60.60, 66.67) | - | - | - | - | - | - | |
| K | L | M | K | L | M | ||||
| J | 0/10 | NA | <0.0001 * | 1.0000 | 0.3173 | <0.0001 * | 1.0000 | 1.0000 | <0.0001 * |
| K | 0/10 | NA | - | 0.3173 | <0.0001 * | - | 1.0000 | <0.0001 * | |
| L | 1/10 | --- (308.87, ---) | - | - | <0.0001 * | - | - | <0.0001 * | |
| M (control) | 15/15 | 61.85 (60.60, 66.67) | - | - | - | - | - | - | |
| (A) Factors Significantly Influencing Survival Determined by Binary Logistic Regression | ||
|---|---|---|
| F1 or V | Factors | Significance |
| F1 | Higher titres | p < 0.001 |
| PCMC and dose level | Significant interaction p = 0.02 | |
| Vaccine type (F1 and V versus F1-V) | Not significant | |
| V | Higher titres | p = 0.001 |
| PCMC/alhydrogel | p < 0.001 | |
| Higher dose level | p = 0.005 | |
| Titre dose level | Significant interaction p = 0.004 | |
| Vaccine type | Not significant | |
| (B) Factors significantly Influencing Survival Determined by ANCOVA | ||
| F1 or V | Interacting Variables | Significance |
| F1 | Effect of vaccine type altered by formulation (PCMC/alhydrogel) | p < 0.001 |
| Effect of vaccine type altered by dose level | p = 0.001 | |
| Effect of formulation (with PCMC and without) altered by dose level | p < 0.001 | |
| V | Effect of dose level on titre | p < 0.001 |
| Effect of PCMC/alhydrogel on titre | p = 0.007 | |
| Dose level and formulation in PCMC/alhydrogel | p < 0.001 | |
| Titre and dose level and formulation in PCMC/alhydrogel | Significant interaction p = 0.006 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moore, B.D.; Macleod, C.; Henning, L.; Krile, R.; Chou, Y.-L.; Laws, T.R.; Butcher, W.A.; Moore, K.M.; Walker, N.J.; Williamson, E.D.; et al. Predictors of Survival after Vaccination in a Pneumonic Plague Model. Vaccines 2022, 10, 145. https://doi.org/10.3390/vaccines10020145
Moore BD, Macleod C, Henning L, Krile R, Chou Y-L, Laws TR, Butcher WA, Moore KM, Walker NJ, Williamson ED, et al. Predictors of Survival after Vaccination in a Pneumonic Plague Model. Vaccines. 2022; 10(2):145. https://doi.org/10.3390/vaccines10020145
Chicago/Turabian StyleMoore, Barry D., Clair Macleod, Lisa Henning, Robert Krile, Ying-Liang Chou, Thomas R. Laws, Wendy A. Butcher, Kristoffer M. Moore, Nicola J. Walker, Ethel Diane Williamson, and et al. 2022. "Predictors of Survival after Vaccination in a Pneumonic Plague Model" Vaccines 10, no. 2: 145. https://doi.org/10.3390/vaccines10020145
APA StyleMoore, B. D., Macleod, C., Henning, L., Krile, R., Chou, Y. -L., Laws, T. R., Butcher, W. A., Moore, K. M., Walker, N. J., Williamson, E. D., & Galloway, D. R. (2022). Predictors of Survival after Vaccination in a Pneumonic Plague Model. Vaccines, 10(2), 145. https://doi.org/10.3390/vaccines10020145