
Predictors of Willingness of the General Public to Receive a Second COVID-19 Booster Dose or a New COVID-19 Vaccine: A Cross-Sectional Study in Greece

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
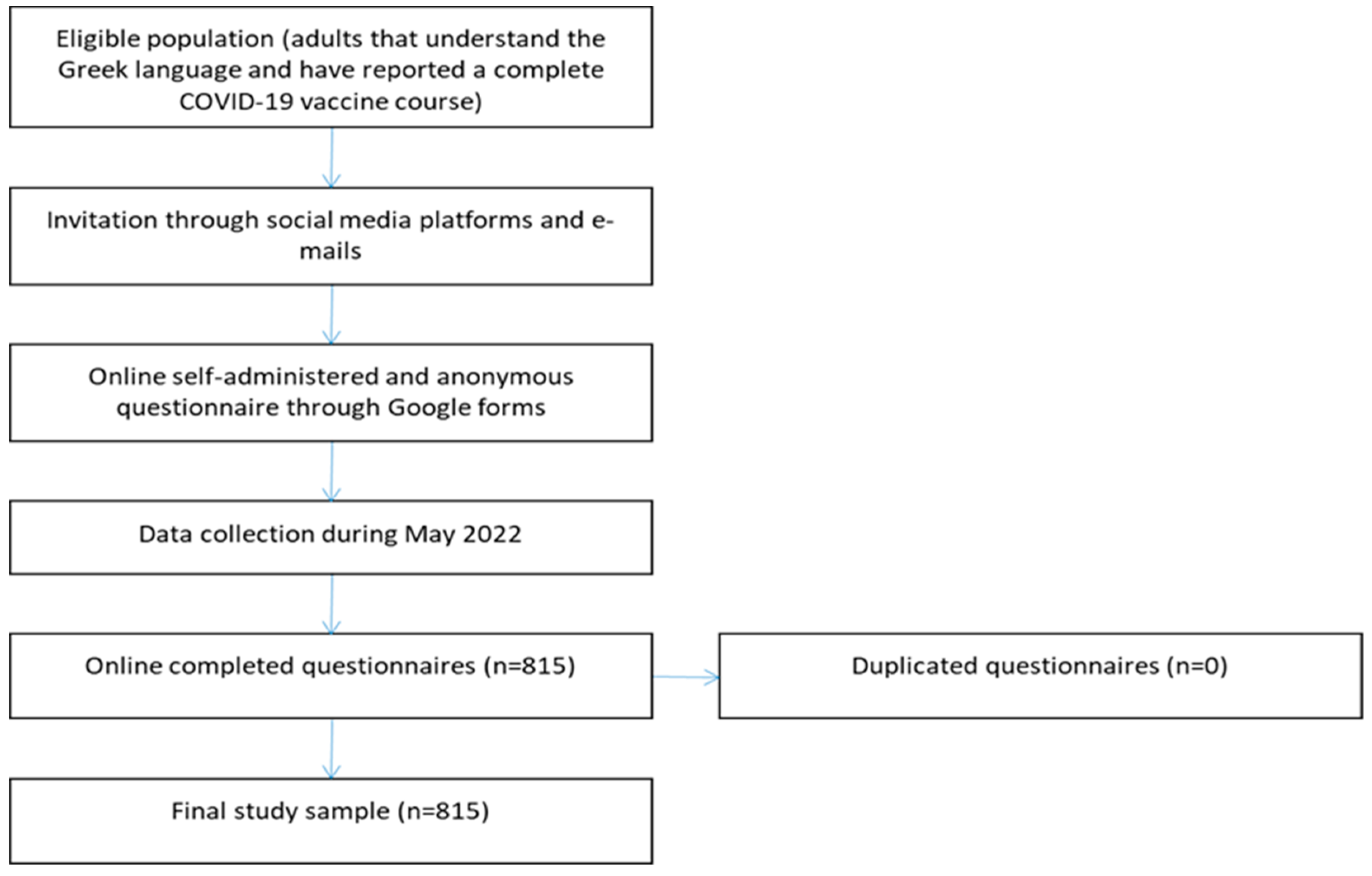
2.1. Study Design and Participants
2.2. Predictor Variables
2.3. Outcome Variable
2.4. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics
3.2. Willingness to Receive a Second Booster Dose or a New COVID-19 Vaccine
3.3. COVID-19 Related Variables and Attitudes toward COVID-19 Vaccination and Pandemic
3.4. Predictors of Willingness
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current Evidence on Efficacy of COVID-19 Booster Dose Vaccination against the Omicron Variant: A Systematic Review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Minka, S.O.; Minka, F.H. A Tabulated Summary of the Evidence on Humoral and Cellular Responses to the SARS-CoV-2 Omicron VOC, as Well as Vaccine Efficacy against This Variant. Immunol. Lett. 2022, 243, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Chen, L.; Shi, Y. Booster COVID-19 Vaccination against the SARS-CoV-2 Omicron Variant: A Systematic Review. Hum. Vaccines Immunother. 2022, 2, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning 2-Dose and 3-Dose Effectiveness of MRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations among Adults during Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 255–263. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Second Booster Dose of Two COVID-19 Vaccines for Older and Immunocompromised Individuals. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-second-booster-dose-two-covid-19-vaccines-older-and (accessed on 30 May 2022).
- Arbel, R.; Sergienko, R.; Friger, M.; Peretz, A.; Beckenstein, T.; Yaron, S.; Netzer, D.; Hammerman, A. Effectiveness of a Second BNT162b2 Booster Vaccine against Hospitalization and Death from COVID-19 in Adults Aged over 60 Years. Nat. Med. 2022; Under publication. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by a Fourth Dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022, 386, 1712–1720. [Google Scholar] [CrossRef]
- Loubet, P.; Launay, O. What a Second Booster Dose of MRNA COVID-19 Vaccines Tells Us. Lancet Infect. Dis. 2022, 9, S1473–S3099. [Google Scholar] [CrossRef]
- Magen, O.; Waxman, J.G.; Makov-Assif, M.; Vered, R.; Dicker, D.; Hernán, M.A.; Lipsitch, M.; Reis, B.Y.; Balicer, R.D.; Dagan, N. Fourth Dose of BNT162b2 MRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2022, 386, 1603–1614. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of Covid-19 MRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-19 Vaccinations in the United States. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-onedose-pop-5yr (accessed on 30 May 2022).
- Al-Qerem, W.; Al Bawab, A.Q.; Hammad, A.; Ling, J.; Alasmari, F. Willingness of the Jordanian Population to Receive a COVID-19 Booster Dose: A Cross-Sectional Study. Vaccines 2022, 10, 410. [Google Scholar] [CrossRef]
- Chu, D.-T.; Vu Thi, H.; Nguyen Thi, Y.V.; Nguyen, M.-A.; Bui, N.-L.; Hoang, V.T.; Hoang Nam, D.; Do, D.-L.; Than, V.T.; Al-Tawfiq, J.A. Willingness to Receive COVID-19 Vaccine Booster Doses for Adults and Their Children in Vietnam. J. Hum. Behav. Soc. Environ. 2022, 1, 1–13. [Google Scholar] [CrossRef]
- Jørgensen, F.J.; Nielsen, L.H.; Petersen, M.B. Willingness to Take the Booster Vaccine in a Nationally Representative Sample of Danes. Vaccines 2022, 10, 425. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public Perceptions and Acceptance of COVID-19 Booster Vaccination in China: A Cross-Sectional Study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef] [PubMed]
- Lounis, M.; Bencherit, D.; Rais, M.A.; Riad, A. COVID-19 Vaccine Booster Hesitancy (VBH) and Its Drivers in Algeria: National Cross-Sectional Survey-Based Study. Vaccines 2022, 10, 621. [Google Scholar] [CrossRef] [PubMed]
- Miao, Y.; Li, Y.; Zhang, W.; Wu, J.; Gu, J.; Wang, M.; Wei, W.; Ye, B.; Miao, C.; Tarimo, C.S.; et al. The Psychological Experience of COVID-19 Vaccination and Its Impact on the Willingness to Receive Booster Vaccines among the Chinese Population: Evidence from a National Cross-Sectional Study. Int. J. Environ. Res. Public. Health 2022, 19, 5464. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Fancourt, D. Predictors of Uncertainty and Unwillingness to Receive the COVID-19 Booster Vaccine: An Observational Study of 22,139 Fully Vaccinated Adults in the UK. Lancet Reg. Health Eur. 2022, 14, 100317. [Google Scholar] [CrossRef] [PubMed]
- Rababa’h, A.M.; Abedalqader, N.N.; Ababneh, M. Jordanians’ Willingness to Receive Heterologous Prime-Boost COVID-19 Vaccination and Vaccine Boosters. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7516–7525. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Wang, X.; Liu, L.; Pei, M.; Li, X.; Li, N. Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing, China; Department of Infectious Diseases, Peking University Third Hospital, Beijing, China Willingness of the General Public to Receive A COVID-19 Vaccine Booster—China, April–May 2021. China CDC Wkly. 2022, 4, 66–70. [Google Scholar] [CrossRef]
- Wu, F.; Yuan, Y.; Deng, Z.; Yin, D.; Shen, Q.; Zeng, J.; Xie, Y.; Xu, M.; Yang, M.; Jiang, S.; et al. Acceptance of COVID-19 Booster Vaccination Based on the Protection Motivation Theory: A Cross-sectional Study in China. J. Med. Virol. 2022; Under publication. [Google Scholar] [CrossRef]
- Yadete, T.; Batra, K.; Netski, D.M.; Antonio, S.; Patros, M.J.; Bester, J.C. Assessing Acceptability of COVID-19 Vaccine Booster Dose among Adult Americans: A Cross-Sectional Study. Vaccines 2021, 9, 1424. [Google Scholar] [CrossRef]
- Yoshida, M.; Kobashi, Y.; Kawamura, T.; Shimazu, Y.; Nishikawa, Y.; Omata, F.; Zhao, T.; Yamamoto, C.; Kaneko, Y.; Nakayama, A.; et al. Factors Associated with COVID-19 Vaccine Booster Hesitancy: A Retrospective Cohort Study, Fukushima Vaccination Community Survey. Vaccines 2022, 10, 515. [Google Scholar] [CrossRef]
- Greek Ministry of Health. Second COVID-19 Booster Dose. Available online: https://emvolio.gov.gr/sites/default/files/attachments/odigies_gia_2i_anamnistiki_dosi_.pdf (accessed on 30 May 2022).
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Moisoglou, I.; Kaitelidou, D. Development and Validation of a Questionnaire to Measure Attitudes toward COVID-19 Vaccination and Pandemic. Int. J. Caring Sci. 2022, 15, 1–10. [Google Scholar]
- Nohynek, H.; Wilder-Smith, A. Does the World Still Need New Covid-19 Vaccines? N. Engl. J. Med. 2022, 386, 2140–2142. [Google Scholar] [CrossRef] [PubMed]
- SteelFisher, G.K.; Blendon, R.J.; Caporello, H. An Uncertain Public—Encouraging Acceptance of Covid-19 Vaccines. N. Engl. J. Med. 2021, 384, 1483–1487. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A Systematic Review and Meta-Analysis of Acceptability and Its Predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Uptake of COVID-19 Vaccines among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 766. [Google Scholar] [CrossRef]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Intention of Healthcare Workers to Accept COVID-19 Vaccination and Related Factors: A Systematic Review and Meta-Analysis. Asian Pac. J. Trop. Med. 2021, 14, 543. [Google Scholar] [CrossRef]
- Dhanda, S.; Osborne, V.; Lynn, E.; Shakir, S. Postmarketing Studies: Can They Provide a Safety Net for COVID-19 Vaccines in the UK? BMJ Evid.-Based Med. 2022, 27, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.M.; Romero, J.R.; Bell, B.P. Postapproval Vaccine Safety Surveillance for COVID-19 Vaccines in the US. JAMA 2020, 324, 1937. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Hu, T.; Li, L.; Lin, C.; Yang, Z.; Chow, C.; Lu, Z.; You, C. An Analysis of the Willingness to the COVID-19 Vaccine Booster Shots among Urban Employees: Evidence from a Megacity H in Eastern China. Int. J. Environ. Res. Public. Health 2022, 19, 2300. [Google Scholar] [CrossRef] [PubMed]
- Al Janabi, T.; Pino, M. Predictors for Actual COVID-19 Vaccine Uptake and Intended Booster Dosage among Medical Students of an Osteopathic Medical School in New York. Epidemiologia 2021, 2, 38. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The Use of the Health Belief Model to Assess Predictors of Intent to Receive the COVID-19 Vaccine and Willingness to Pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public Preference for COVID-19 Vaccines in China: A Discrete Choice Experiment. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Predictors of COVID-19 Vaccination Uptake and Reasons for Decline of Vaccination: A Systematic Review. MedRxiv 2021. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Willingness, Refusal and Influential Factors of Parents to Vaccinate Their Children against the COVID-19: A Systematic Review and Meta-Analysis. Prev. Med. 2022, 157, 106994. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Ohayon, M.M.; Griffiths, M.D.; Lin, C.-Y.; Pakpour, A.H. Fear of COVID-19 and Its Association with Mental Health-Related Factors: Systematic Review and Meta-Analysis. BJPsych Open 2022, 8, e73. [Google Scholar] [CrossRef]
- Luo, F.; Ghanei Gheshlagh, R.; Dalvand, S.; Saedmoucheshi, S.; Li, Q. Systematic Review and Meta-Analysis of Fear of COVID-19. Front. Psychol. 2021, 12, 661078. [Google Scholar] [CrossRef]
- Stead, M.; Jessop, C.; Angus, K.; Bedford, H.; Ussher, M.; Ford, A.; Eadie, D.; MacGregor, A.; Hunt, K.; MacKintosh, A.M. National Survey of Attitudes towards and Intentions to Vaccinate against COVID-19: Implications for Communications. BMJ Open 2021, 11, e055085. [Google Scholar] [CrossRef] [PubMed]
- UK Office for National Statistics. Coronavirus (COVID-19) Infection Survey Technical Article: Analysis of Characteristics Associated with Vaccination Uptake; UK Office for National Statistics: London, UK, 2021.
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards Vaccines and Intention to Vaccinate against COVID-19: Implications for Public Health Communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef] [PubMed]
- McLean, C.P.; Anderson, E.R. Brave Men and Timid Women? A Review of the Gender Differences in Fear and Anxiety. Clin. Psychol. Rev. 2009, 29, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef]
- Worldometer. Greece Population. Available online: https://www.worldometers.info/world-population/greece-population/ (accessed on 30 May 2022).


{kind=link}
| Characteristics | N | % |
|---|---|---|
| Gender | ||
| Male | 195 | 23.9 |
| Female | 620 | 76.1 |
| Age (years) a | 37.0 | 13.3 |
| Marital status | ||
| Single | 440 | 54.0 |
| Married or in a relationship without marriage | 290 | 35.6 |
| Divorced | 75 | 9.2 |
| Widowed | 10 | 1.2 |
| Educational level | ||
| Elementary school | 0 | 0.0 |
| High school | 225 | 27.6 |
| University degree | 590 | 72.4 |
| Chronic disease | ||
| No | 625 | 76.7 |
| Yes | 190 | 23.3 |
| Self-perceived physical health | ||
| Very poor | 0 | 0.0 |
| Poor | 5 | 0.6 |
| Moderate | 90 | 11.0 |
| Good | 400 | 49.1 |
| Very good | 320 | 39.3 |
| Influenza vaccination during 2021 | ||
| No | 545 | 66.9 |
| Yes | 270 | 33.1 |
| N | % | |
|---|---|---|
| Previous COVID-19 diagnosis | ||
| No | 400 | 49.1 |
| Yes | 415 | 50.9 |
| Hospitalization due to COVID-19 (n = 415) | ||
| No | 400 | 96.4 |
| Yes | 15 | 3.6 |
| COVID-19-related death in family members/friends | ||
| No | 560 | 68.7 |
| Yes | 255 | 31.3 |
| If a second booster dose or a new COVID-19 vaccine is recommended as a supplement to the current vaccination schedule, would you accept it? | ||
| Definitely no | 60 | 7.4 |
| Probably no | 40 | 4.9 |
| Unsure | 210 | 25.7 |
| Probably yes | 320 | 39.3 |
| Definitely yes | 185 | 22.7 |
| Which of the following concerns best describe why you might refuse to accept a second COVID-19 booster dose or a new COVID-19 vaccine? (n = 310) | ||
| I have doubts about the COVID-19 vaccine safety | 40 | 12.9 |
| I have doubts about the COVID-19 vaccine effectiveness | 95 | 30.7 |
| I worry about the short-term side effects | 90 | 29.0 |
| I have a low risk of infection | 0 | 0.0 |
| I am healthy and I am at low risk of COVID-19-related complications | 70 | 22.6 |
| I am not convinced that another dose will be necessary | 125 | 40.3 |
| I do not need it because I believe I have immunity against the SARS-CoV-2 | 60 | 19.4 |
| I have already been diagnosed with COVID-19, so I think another booster dose would not be beneficial | 65 | 21.0 |
| I am tired of the vaccination process | 85 | 27.4 |
| I worry about the long-term side effects | 145 | 46.8 |
| Adverse reactions and discomfort experienced after previous COVID-19 vaccine doses | 2.8 | 2.3 |
| Fear of the COVID-19 a | 5.6 | 2.0 |
| Information regarding the COVID-19 pandemic and vaccination a | 8.1 | 1.5 |
| Compliance with hygiene measures a | 9.0 | 1.1 |
| Trust in COVID-19 vaccination a | 7.0 | 1.6 |
| Fear of a second booster dose or a new COVID-19 vaccine a | 3.6 | 3.3 |
| Concerns about the long-term side effects of a second booster dose or a new COVID-19 vaccine a | 4.0 | 3.1 |
| Self-perceived protection by the previous COVID-19 vaccine doses a | 7.0 | 2.3 |
| Variable | Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) a | p-Value |
|---|---|---|---|---|
| Gender (male vs. female) | 2.48 (1.72–3.60) | <0.001 | 2.40 (1.34–4.29) | 0.003 |
| Age (years) | 1.03 (1.02–1.04) | <0.001 | 0.97 (0.95–0.99) | 0.02 |
| Marital status (married vs. single/widowed/divorced) | 2.05 (1.50–2.79) | <0.001 | 1.29 (0.75–2.24) | 0.36 |
| Educational level (university degree vs. high school) | 1.28 (0.93–1.74) | 0.13 | 1.00 (0.54–1.85) | 0.99 |
| Chronic disease (yes vs. no) | 0.92 (0.66–1.29) | 0.64 | 1.26 (0.74–2.14) | 0.40 |
| Self-perceived physical health (good/very good vs. very poor/poor/moderate) | 2.51 (1.62–3.87) | <0.001 | 3.63 (1.78–7.42) | <0.001 |
| Influenza vaccination during 2021 (yes vs. no) | 2.58 (1.86–3.57) | <0.001 | 1.59 (0.95–2.66) | 0.08 |
| Previous COVID-19 diagnosis (no vs. yes) | 3.07 (2.28–4.14) | <0.001 | 2.96 (1.84–4.75) | <0.001 |
| COVID-19-related death in family members/friends (yes vs. no) | 1.19 (0.87–1.61) | 0.28 | 1.37 (0.82–2.29) | 0.24 |
| Adverse reactions and discomfort experienced after previous COVID-19 vaccine doses | 0.86 (0.81–0.92) | <0.001 | 1.13 (0.99–1.28) | 0.05 |
| Fear of the COVID-19 | 1.65 (1.50–1.80) | <0.001 | 1.73 (1.47–2.03) | <0.001 |
| Information regarding the COVID-19 pandemic and vaccination | 1.48 (1.33–1.64) | <0.001 | 0.98 (0.82–1.17) | 0.85 |
| Compliance with hygiene measures | 1.25 (1.10–1.42) | 0.001 | 0.95 (0.75–1.22) | 0.69 |
| Trust in COVID-19 vaccination | 2.11 (1.87–2.38) | <0.001 | 2.11 (1.69–2.63) | <0.001 |
| Fear of a second booster dose or a new COVID-19 vaccine | 0.63 (0.59–0.67) | <0.001 | 0.66 (0.59–0.75) | <0.001 |
| Concerns about the long-term side effects of a second booster dose or a new COVID-19 vaccine | 0.71 (0.68–0.75) | <0.001 | 0.91 (0.81–1.04) | 0.16 |
| Self-perceived protection by the previous COVID-19 vaccine doses | 1.29 (1.21–1.38) | <0.001 | 1.04 (0.92–1.18) | 0.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. Predictors of Willingness of the General Public to Receive a Second COVID-19 Booster Dose or a New COVID-19 Vaccine: A Cross-Sectional Study in Greece. Vaccines 2022, 10, 1061. https://doi.org/10.3390/vaccines10071061
Galanis P, Vraka I, Katsiroumpa A, Siskou O, Konstantakopoulou O, Katsoulas T, Mariolis-Sapsakos T, Kaitelidou D. Predictors of Willingness of the General Public to Receive a Second COVID-19 Booster Dose or a New COVID-19 Vaccine: A Cross-Sectional Study in Greece. Vaccines. 2022; 10(7):1061. https://doi.org/10.3390/vaccines10071061
Chicago/Turabian StyleGalanis, Petros, Irene Vraka, Aglaia Katsiroumpa, Olga Siskou, Olympia Konstantakopoulou, Theodoros Katsoulas, Theodoros Mariolis-Sapsakos, and Daphne Kaitelidou. 2022. "Predictors of Willingness of the General Public to Receive a Second COVID-19 Booster Dose or a New COVID-19 Vaccine: A Cross-Sectional Study in Greece" Vaccines 10, no. 7: 1061. https://doi.org/10.3390/vaccines10071061
APA StyleGalanis, P., Vraka, I., Katsiroumpa, A., Siskou, O., Konstantakopoulou, O., Katsoulas, T., Mariolis-Sapsakos, T., & Kaitelidou, D. (2022). Predictors of Willingness of the General Public to Receive a Second COVID-19 Booster Dose or a New COVID-19 Vaccine: A Cross-Sectional Study in Greece. Vaccines, 10(7), 1061. https://doi.org/10.3390/vaccines10071061