
COVID-19 Vaccine for Children: Vaccination Willingness of Parents and Its Associated Factors—A Network Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedure
2.2. Materials
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
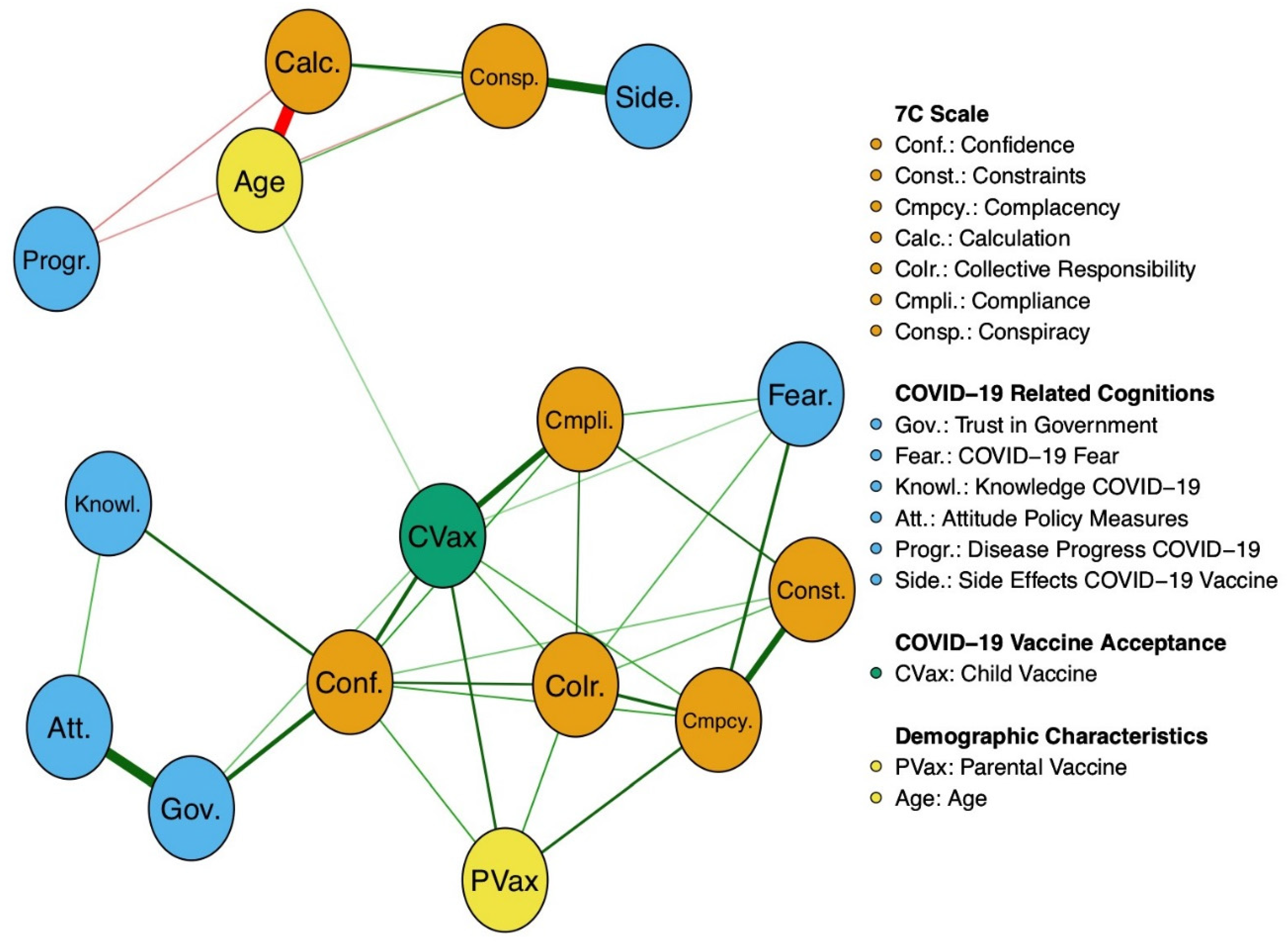
3.2. Network Estimation and Visualization
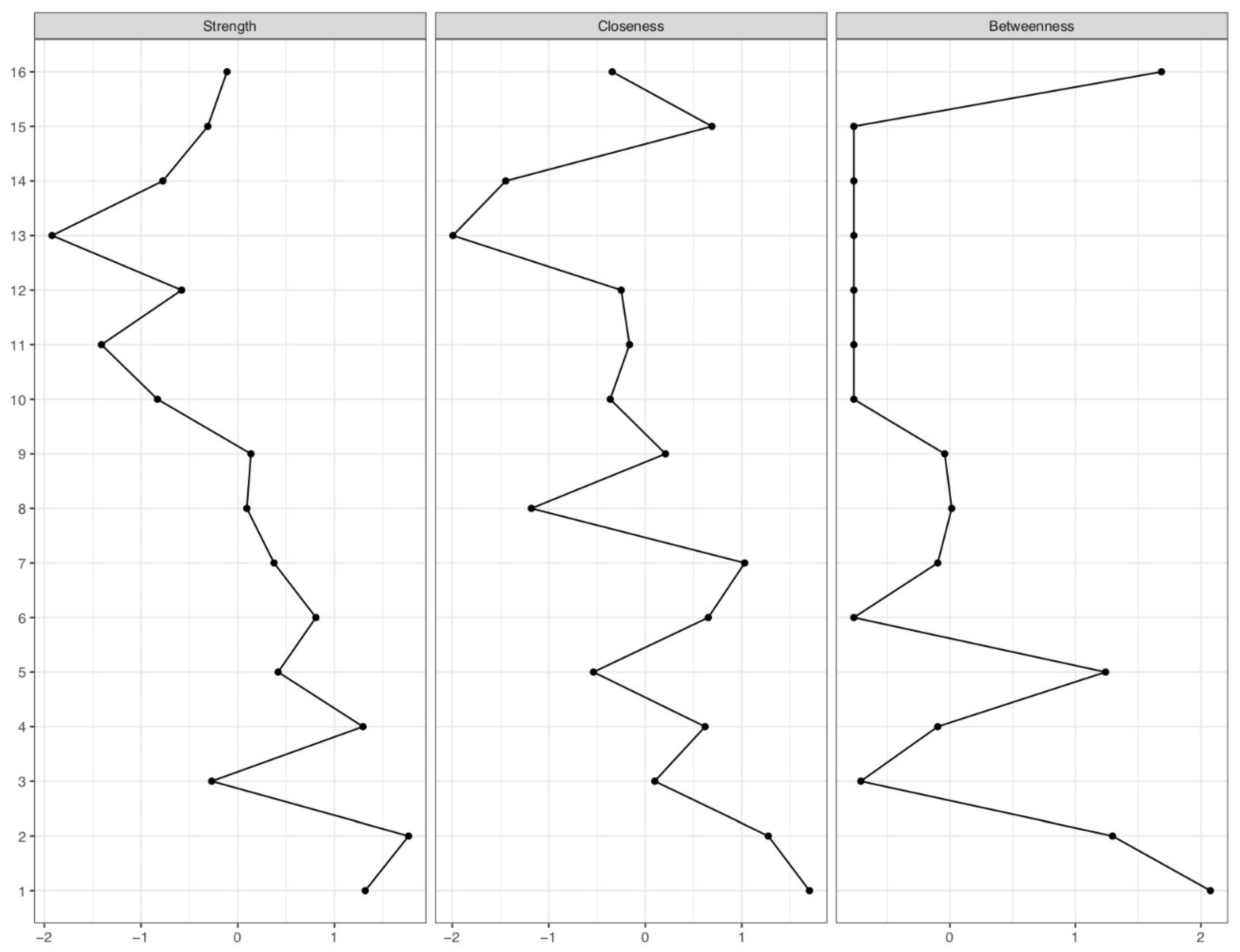
3.3. Centrality Indices
3.4. Bootstrapping Procedures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deutsche Welle. Available online: https://www.dw.com/en/coronavirus-where-the-vaccine-has-been-rolled-out/a-56073292 (accessed on 13 March 2022).
- Yılmaz, M.; Sahin, M.K. Parents’ willingness and attitudes concerning the COVID-19 vaccine: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e14364. [Google Scholar] [CrossRef] [PubMed]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2021, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2021, 114, 252–260. [Google Scholar] [CrossRef]
- Araf, Y.; Akter, F.; Tang, Y.; Fatemi, R.; Alam Parvez, S.; Zheng, C.; Hossain, G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef]
- Schoch-Spana, M.; Brunson, E.K.; Long, R.; Ruth, A.; Ravi, S.J.; Trotochaud, M.; Borio, L.; Brewer, J.; Buccina, J.; Connell, N.; et al. The public’s role in COVID-19 vaccination: Human-centered recommendations to enhance pandemic vaccine awareness, access, and acceptance in the United States. Vaccine 2021, 39, 6004–6012. [Google Scholar] [CrossRef]
- Geoghegan, S.; O’Callaghan, K.P.; Offit, P.A. Vaccine Safety: Myths and Misinformation. Front. Microbiol. 2020, 11, 372. [Google Scholar] [CrossRef] [Green Version]
- Luo, C.; Chen, A.; Cui, B.; Liao, W. Exploring public perceptions of the COVID-19 vaccine online from a cultural perspective: Semantic network analysis of two social media platforms in the United States and China. Telemat. Inform. 2021, 65, 101712. [Google Scholar] [CrossRef]
- Bronstein, M.V.; Kummerfeld, E.; MacDonald, A.; Vinogradov, S. Willingness to vaccinate against SARS-CoV-2: The role of reasoning biases and conspiracist ideation. Vaccine 2021, 40, 213–222. [Google Scholar] [CrossRef]
- Hettich, N.; Krakau, L.; Rückert, K.; Brähler, E.; Zahn, D.; Yilmaz, S.; Münzel, T.; Gianicolo, E.; Schmidtmann, I.; Schulz, A.; et al. Willingness to be vaccinated against SARS-CoV-2 in the German population during the second wave of the pandemic. Dtsch. Arztebl. Int. 2021, 118, 720–721. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: A Country-level Analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Umakanthan, S.; Lawrence, S. Predictors of COVID-19 vaccine hesitancy in Germany: A cross-sectional, population-based study. Postgrad. Med. J. 2022. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Schernhammer, E.; Weitzer, J.; Laubichler, M.D.; Birmann, B.M.; Bertau, M.; Zenk, L.; Caniglia, G.; Jäger, C.C.; Steiner, G. Correlates of COVID-19 vaccine hesitancy in Austria: Trust and the government. J. Public Health 2021, 44, e106–e116. [Google Scholar] [CrossRef] [PubMed]
- Altenbuchner, A.; Haug, S.; Schnell, R.; Scharf, A.; Weber, K. Impfbereitschaft von Eltern mit einem COVID-19-Vakzin: Die Rolle von Elternschaft und Geschlecht [Parents’ Willingness to Vaccinate with a COVID-19 Vaccine]. Padiatr. Padol. 2021, 56, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Luxi, N.; Giovanazzi, A.; Capuano, A.; Crisafulli, S.; Cutroneo, P.M.; Fantini, M.P.; Ferrajolo, C.; Moretti, U.; Poluzzi, E.; Raschi, E.; et al. COVID-19 Vaccination in Pregnancy, Paediatrics, Immunocompromised Patients, and Persons with History of Allergy or Prior SARS-CoV-2 Infection: Overview of Current Recommendations and Pre- and Post-Marketing Evidence for Vaccine Efficacy and Safety. Drug Saf. 2021, 44, 1247–1269. [Google Scholar] [CrossRef]
- Lv, M.; Luo, X.; Shen, Q.; Lei, R.; Liu, X.; Liu, E.; Li, Q.; Chen, Y. Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Children and Adolescents: A Systematic Review. Vaccines 2021, 9, 1102. [Google Scholar] [CrossRef]
- Eberhardt, C.S.; Siegrist, C. Is there a role for childhood vaccination against COVID-19? Pediatr. Allergy Immunol. 2020, 32, 9–16. [Google Scholar] [CrossRef]
- Babicki, M.; Pokorna-Kałwak, D.; Doniec, Z.; Mastalerz-Migas, A. Attitudes of Parents with Regard to Vaccination of Children against COVID-19 in Poland. A Nationwide Online Survey. Vaccines 2021, 9, 1192. [Google Scholar] [CrossRef]
- Ruggiero, K.M.; Wong, J.; Sweeney, C.F.; Avola, A.; Auger, A.; Macaluso, M.; Reidy, P. Parents’ Intentions to Vaccinate Their Children Against COVID-19. J. Pediatr. Health Care 2021, 35, 509–517. [Google Scholar] [CrossRef]
- Goldman, R.D.; Yan, T.D.; Seiler, M.; Cotanda, C.P.; Brown, J.C.; Klein, E.J.; Hoeffe, J.; Gelernter, R.; Hall, J.E.; Davis, A.L.; et al. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine 2020, 38, 7668–7673. [Google Scholar] [CrossRef] [PubMed]
- Robert-Koch-Institut. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Impfquotenmonitoring.html (accessed on 20 April 2022).
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.; Costa, D.; Costa, D.; Keating, J.; Arantes, J. Predicting COVID-19 Vaccination Intention: The Determinants of Vaccine Hesitancy. Vaccines 2021, 9, 1161. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Fedele, F.; Aria, M.; Esposito, V.; Micillo, M.; Cecere, G.; Spano, M.; De Marco, G. COVID-19 vaccine hesitancy: A survey in a population highly compliant to common vaccinations. Hum. Vaccines Immunother. 2021, 17, 3348–3354. [Google Scholar] [CrossRef]
- Bianco, A.; Della Polla, G.; Angelillo, S.; Pelullo, C.P.; Licata, F.; Angelillo, I.F. Parental COVID-19 vaccine hesitancy: A cross-sectional survey in Italy. Expert Rev. Vaccines 2022, 21, 541–547. [Google Scholar] [CrossRef]
- Russo, L.; Croci, I.; Campagna, I.; Pandolfi, E.; Villani, A.; Reale, A.; Barbieri, M.A.; Raponi, M.; Gesualdo, F.; Tozzi, A.E. Intention of Parents to Immunize Children against SARS-CoV-2 in Italy. Vaccines 2021, 9, 1469. [Google Scholar] [CrossRef]
- Brandstetter, S.; Böhmer, M.M.; Pawellek, M.; Seelbach-Göbel, B.; Melter, M.; Kabesch, M.; Apfelbacher, C.; Ambrosch, A.; Arndt, P.; Baessler, A.; et al. Parents’ intention to get vaccinated and to have their child vaccinated against COVID-19: Cross-sectional analyses using data from the KUNO-Kids health study. Eur. J. Pediatr. 2021, 180, 3405–3410. [Google Scholar] [CrossRef]
- Universität Erfurt. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/topic/impfung/30-kinderimpfung/ (accessed on 14 March 2022).
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental Acceptability of COVID-19 Vaccination for Children Under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef]
- Wang, Z.; Xiao, J.; Jiang, F.; Li, J.; Yi, Y.; Min, W.; Tan, A.; Liang, R.; Liu, S.; Chen, L.; et al. The willingness of Chinese adults to receive the COVID-19 vaccine and its associated factors at the early stage of the vaccination programme: A network analysis. J. Affect. Disord. 2021, 297, 301–308. [Google Scholar] [CrossRef]
- Bagateli, L.E.; Saeki, E.Y.; Fadda, M.; Agostoni, C.; Marchisio, P.; Milani, G.P. COVID-19 Vaccine Hesitancy among Parents of Children and Adolescents Living in Brazil. Vaccines 2021, 9, 1115. [Google Scholar] [CrossRef] [PubMed]
- Yoda, T.; Katsuyama, H. Parents’ hesitation about getting their children vaccinated against COVID-19 in Japan. Hum. Vaccines Immunother. 2021, 17, 4993–4998. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Klas, A.; Mikocka-Walus, A.; German, B.; Rogers, G.; Ling, M.; Fernando, J.; Kothe, E.; Westrupp, E. “Poison” or “protection”? A mixed methods exploration of Australian parents’ COVID-19 vaccination intentions. Psychosomatics 2021, 150, 110626. [Google Scholar] [CrossRef]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Methods Prim. 2021, 1, 1–18. [Google Scholar] [CrossRef]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Krakowczyk, J.B.; Planert, J.; Skoda, E.-M.; Dinse, H.; Kaup, T.; Teufel, M.; Bäuerle, A. Pandemic fatigue, psychopathological risk factors, and vaccination attitudes during the COVID-19 pandemic in 2021—A network analysis. J. Affect. Disord. Rep. 2022, 8, 100345. [Google Scholar] [CrossRef]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 COVID-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef]
- Ali, K.; Berman, G.; Zhou, H.; Deng, W.; Faughnan, V.; Coronado-Voges, M.; Ding, B.; Dooley, J.; Girard, B.; Hillebrand, W.; et al. Evaluation of mRNA-1273 SARS-CoV-2 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 2241–2251. [Google Scholar] [CrossRef]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of Vaccination Readiness. Eur. J. Psychol. Assess. 2021, 0, 1–9. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Skoda, E.-M.; Spura, A.; De Bock, F.; Schweda, A.; Dörrie, N.; Fink, M.; Musche, V.; Weismüller, B.; Benecke, A.; Kohler, H.; et al. Veränderung der psychischen Belastung in der COVID-19-Pandemie in Deutschland: Ängste, individuelles Verhalten und die Relevanz von Information sowie Vertrauen in Behörden. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2021, 64, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Bäuerle, A.; Teufel, M.; Musche, V.; Weismüller, B.; Kohler, H.; Hetkamp, M.; Dörrie, N.; Schweda, A.; Skoda, E.-M. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Kaup, T.; Schweda, A.; Krakowczyk, J.; Dinse, H.; Skoda, E.-M.; Teufel, M.; Bäuerle, A. Levels, Predictors, and Distribution of Interpersonal Solidarity during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 2041. [Google Scholar] [CrossRef] [PubMed]
- Reips, U.-D.; Funke, F. Interval-level measurement with visual analogue scales in Internet-based research: VAS Generator. Behav. Res. Methods 2008, 40, 699–704. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 1 April 2022).
- Constantin, M.A.; Schuurman, N.K.; Vermunt, J. A General Monte Carlo Method for Sample Size Analysis in the Context of Network Models. PsyArXiv 2021. [Google Scholar] [CrossRef]
- Haslbeck, J.M.B.; Waldorp, L.J. Structure Estimation for Mixed Graphical Models in High Dimensional Data. arXiv 2015, arXiv:1510.05677. [Google Scholar]
- Chen, J.; Chen, Z. Extended Bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics 2007, 9, 432–441. [Google Scholar] [CrossRef] [Green Version]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef] [Green Version]
- Isvoranu, A.-M.; Abdin, E.; Chong, S.A.; Vaingankar, J.; Borsboom, D.; Subramaniam, M. Extended network analysis: From psychopathology to chronic illness. BMC Psychiatry 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A.; Bendezu-Quispe, G. Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean. Vaccines 2021, 9, 1303. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Ahmed, S.; Bonna, A.S.; Sarkar, A.-S.; Islam, A.; Urmi, T.A.; Proma, T.S. Parental coronavirus disease vaccine hesitancy for children in Bangladesh: A cross-sectional study. F1000Research 2022, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- RKI. Pressemitteilung der STIKO zur COVID-19-Auffrischimpfung bei Kindern und Jugendlichen im Alter von 12-17 Jahren sowie zur Optimierung der 1-Maligen Impfung mit der COVID-19 Vaccine Janssen. Available online: https://www.rki.de/DE/Content/Kommissionen/STIKO/Empfehlungen/PM_2022-01-13.html#:~:text=Die%20STIKO%20empfiehlt%20daher%20die,zur%20vorangegangenen%20Impfung%20verabreicht%20werden (accessed on 20 April 2022).
- Van den Bos, G.R.; American Psychological Association. APA Dictionary of Psychology, 2nd ed.; American Psychological Association: Washington, DC, USA, 2015. [Google Scholar]
- Feng, H.; Zhu, H.; Zhang, H.; Cao, L.; Li, L.; Wang, J.; Huang, Y.; Lai, X.; Lyu, Y.; Jing, R.; et al. Caregivers’ intentions to COVID-19 vaccination for their children in China: A cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 4799–4805. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Willingness, refusal and influential factors of parents to vaccinate their children against the COVID-19: A systematic review and meta-analysis. Prev. Med. 2022, 157, 106994. [Google Scholar] [CrossRef] [PubMed]
- Biswas, R.; Alzubaidi, M.S.; Shah, U.; Abd-Alrazaq, A.A.; Shah, Z. A Scoping Review to Find Out Worldwide COVID-19 Vaccine Hesitancy and Its Underlying Determinants. Vaccines 2021, 9, 1243. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.-X.; Lin, X.-Q.; Chen, Y.; Tung, T.-H.; Zhu, J.-S. Determinants of parental hesitancy to vaccinate their children against COVID-19 in China. Expert Rev. Vaccines 2021, 20, 1339–1349. [Google Scholar] [CrossRef]
- Delgado-Gallegos, J.L.; Padilla-Rivas, G.R.; Gastelum-Arias, L.J.; Zuñiga-Violante, E.; Avilés-Rodríguez, G.; Arellanos-Soto, D.; Franco-Villareal, H.; Garza-Treviño, E.N.; Cosío-León, M.D.L.; Romo-Cardenas, G.S.; et al. Parent’s Perspective towards Child COVID-19 Vaccination: An Online Cross-Sectional Study in Mexico. Int. J. Environ. Res. Public Health 2021, 19, 290. [Google Scholar] [CrossRef]
- Wroe, A.L.; Turner, N.; Salkovskis, P.M. Understanding and Predicting Parental Decisions About Early Childhood Immunizations. Health Psychol. 2004, 23, 33–41. [Google Scholar] [CrossRef]
- Wagner, A.; Liberatore, F.; Schmelzer, S.; Dratva, J. Confident and altruistic–parents’ motives to vaccinate their children against COVID-19: A cross-sectional online survey in a Swiss vaccination centre. Swiss Med. Wkly. 2022, 152, w30156. [Google Scholar] [CrossRef]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet Infect. Dis. 2022, 22, 183–195. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Soares, P.; Rocha, J.; Moniz, M.; Gama, A.; Laires, P.; Pedro, A.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Tao, L.; Liu, J. The Association Between Risk Perception and COVID-19 Vaccine Hesitancy for Children Among Reproductive Women in China: An Online Survey. Front. Med. 2021, 8, 741298. [Google Scholar] [CrossRef]
- Chinawa, A.T.; Chinawa, J.M.; Ossai, E.N.; Obinna, N.; Onukwuli, V.; Aronu, A.E.; Manyike, C.P. Maternal level of awareness and predictors of willingness to vaccinate children against COVID-19; A multi-center study. Hum. Vaccines Immunother. 2021, 17, 3982–3988. [Google Scholar] [CrossRef]
- Chen, F.; He, Y.; Shi, Y. Parents’ and Guardians’ Willingness to Vaccinate Their Children against COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 179. [Google Scholar] [CrossRef] [PubMed]
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; Perrone, P.; Squillace, L.; Dallolio, L.; Pandolfi, P.; et al. Would Parents Get Their Children Vaccinated Against SARS-CoV-2? Rate and Predictors of Vaccine Hesitancy According to a Survey over 5000 Families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of U.S. adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y. Multilevel determinants of COVID-19 vaccination hesitancy in the United States: A rapid systematic review. Prev. Med. Rep. 2021, 25, 101673. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Gender | |||
| Female | 2252 | 93.6 | |
| Male | 148 | 6.2 | |
| Diverse | 5 | 0.2 | |
| Level of education | |||
| University degree | 1371 | 57 | |
| High school degree | 315 | 13.1 | |
| Higher middle school degree | 105 | 4.4 | |
| Lower middle school degree | 597 | 24.8 | |
| Other form of schooling | 4 | 0.1 | |
| Residence area | |||
| Urban area (population size > 20,000) | 853 | 35.5 | |
| Rural area (population size < 20,000) | 1552 | 64.5 | |
| Marital status | |||
| Single | 73 | 3.0 | |
| Married | 2009 | 83.5 | |
| In a relationship | 225 | 9.4 | |
| Separated/divorced | 93 | 3.9 | |
| Widowed | 3 | 0.1 | |
| Other | 2 | 0.1 | |
| COVID-19 vaccine | |||
| Yes | 2088 | 86.8 | |
| No | 317 | 13.2 | |
| Health status | |||
| Physical illness | 486 | 20.2 | |
| Mental illness | 212 | 8.8 | |
| Number of children < 18 | |||
| 1 | 1553 | 64.4 | |
| 2 | 734 | 30.5 | |
| 3 | 97 | 4.0 | |
| More than 3 | 21 | 0.9 | |
| Age of children | |||
| 5 | 766 | 31.9 | |
| 6 | 539 | 22.4 | |
| 7 | 480 | 20.0 | |
| 8 | 414 | 17.2 | |
| 9 | 359 | 14.9 | |
| 10 | 302 | 12.6 | |
| 11 | 306 | 12.7 | |
| >12 | 508 | 21.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krakowczyk, J.B.; Bäuerle, A.; Pape, L.; Kaup, T.; Nulle, L.; Teufel, M.; Skoda, E.-M. COVID-19 Vaccine for Children: Vaccination Willingness of Parents and Its Associated Factors—A Network Analysis. Vaccines 2022, 10, 1155. https://doi.org/10.3390/vaccines10071155
Krakowczyk JB, Bäuerle A, Pape L, Kaup T, Nulle L, Teufel M, Skoda E-M. COVID-19 Vaccine for Children: Vaccination Willingness of Parents and Its Associated Factors—A Network Analysis. Vaccines. 2022; 10(7):1155. https://doi.org/10.3390/vaccines10071155
Chicago/Turabian StyleKrakowczyk, Julia Barbara, Alexander Bäuerle, Lars Pape, Theodor Kaup, Laura Nulle, Martin Teufel, and Eva-Maria Skoda. 2022. "COVID-19 Vaccine for Children: Vaccination Willingness of Parents and Its Associated Factors—A Network Analysis" Vaccines 10, no. 7: 1155. https://doi.org/10.3390/vaccines10071155
APA StyleKrakowczyk, J. B., Bäuerle, A., Pape, L., Kaup, T., Nulle, L., Teufel, M., & Skoda, E. -M. (2022). COVID-19 Vaccine for Children: Vaccination Willingness of Parents and Its Associated Factors—A Network Analysis. Vaccines, 10(7), 1155. https://doi.org/10.3390/vaccines10071155