


Causes of Vaccine Hesitancy in Adults for the Influenza and COVID-19 Vaccines: A Systematic Literature Review

Abstract
:1. Introduction
2. Methodology
2.1. Search Strategy
2.2. Screening, Reliability Checks and Risk of Bias Assessment
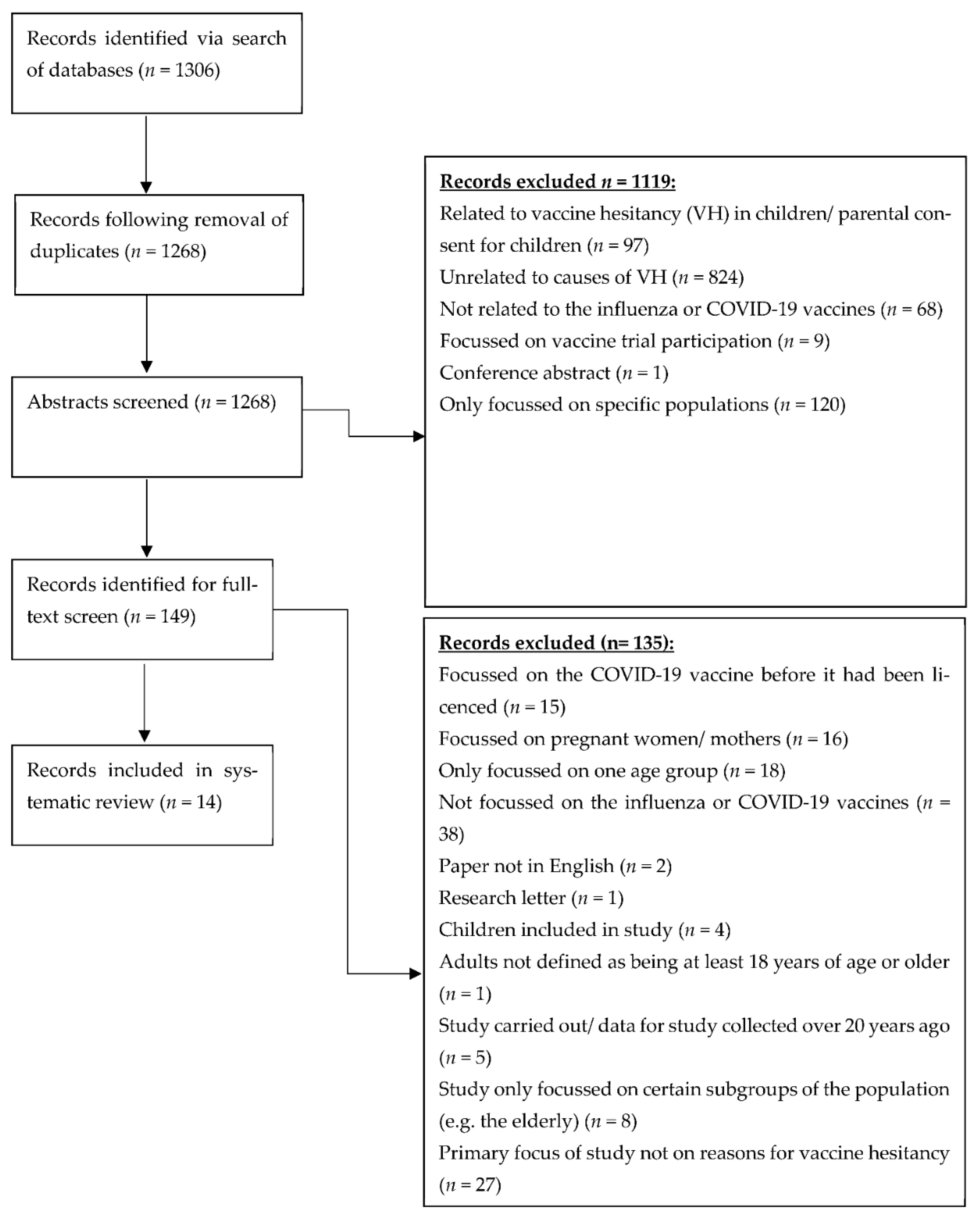
3. Results
3.1. Study Characteristics
3.2. Risk of Bias in the Included Studies
3.3. Causes of Vaccine Hesitancy
3.3.1. Concerns over Vaccine Safety
3.3.2. Lack of Trust
3.3.3. Lack of Need for Vaccination
3.3.4. Cultural Reasons
4. Discussion
4.1. Recommendations for Practice
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 29 July 2022).
- Vaccine Effectiveness: How Well Do Flu Vaccines Work? Available online: https://www.cdc.gov/flu/vaccines-work/vaccineeffect.htm#:~:text=Flu%20vaccination%20has%20been%20shown,to%20those%20who%20were%20unvaccinated (accessed on 26 June 2022).
- Olivera, M.D.; Hogan, A.; Watson, O.; Charles, G.; Hauck, K.; Ghani, A.; Windskill, P. Modelling the impact of vaccine hesitancy in prolonging the need for Non-Pharmaceutical Interventions to control the COVID-19 pandemic. Commun. Med. 2022, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Truong, J.; Bakshi, S.; Wasim, A.; Ahmad, M.; Majid, U. What factors promote vaccine hesitancy or acceptance during pandemics? A systematic review and thematic analysis. Health Promot. Int. 2021, 2, 37. [Google Scholar] [CrossRef] [PubMed]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 6, 75. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.A.M.; Colebunders, R.; Gele, A.A.; Farah, A.; Osman, S.; Guled, I.; Absullahi, A.; Hussein, A.; Ali, A.; Fodjo, J. COVID-19 Vaccine Acceptability and Adherence to Preventive Measures in Somalia: Results of an Online Survey. Vaccines 2021, 6, 543. [Google Scholar] [CrossRef]
- Ahmed, T.F.; Ahmed, A.; Ahmed, S.; Ahmed, H. Understanding COVID-19 vaccine acceptance in Pakistan: An echo of previous immunizations or prospect of change? Expert Rev. Vaccines 2021, 20, 1185–1193. [Google Scholar] [CrossRef]
- Dorman, C.; Perera, A.; Condon, C.; Chau, C.; Qian, J.; Kalk, K.; DiazDeleon, D. Factors Associated with Willingness to be Vaccinated Against COVID-19 in a Large Convenience Sample. J. Community Health 2021, 46, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef] [PubMed]
- Galistiani, G.F.; Matuz, M.; Matuszka, N.; Dorό, P.; Schváb, K.; Engi, Z.; Benkő, R. Determinants of influenza vaccine uptake and willingness to be vaccinated by pharmacists among the active adult population in Hungary: A cross-sectional exploratory study. BMC Public Health 2021, 21, 521. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Goldfarb, J.; Brownstein, J.; Kriner, D. The Relationship between US Adults’ Misconceptions about COVID-19 Vaccines and Vaccination Preferences. Vaccines 2021, 9, 901. [Google Scholar] [CrossRef] [PubMed]
- Kumari, A.; Ranjan, P.; Chopra, S.; Kaur, D.; Kaur, T.; Kalanidhi, K.; Goel, A.; Singh, A.; Baitha, U.; Prakash, B.; et al. What Indians Think of the COVID-19 vaccine: A qualitative study comprising focus group discussions and thematic analysis. Diabetes Metab Syndr. 2021, 15, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Montalti, M.; Valerio, Z.; Rallo, F.; Squillance, L.; Costantino, C.; Tomasello, F.; Mauro, G.L.; Stillo, M.; Perrone, P.; Resi, D.; et al. Attitudes toward the SARS-CoV-2 and Influenza Vaccination in the Metropolitan Cities of Bologna and Palermo, Italy. Vaccines 2021, 9, 1200. [Google Scholar] [CrossRef] [PubMed]
- Quinn, S.C.; Jamison, A.; Freimuth, V.S.; An, J.; Hancock, G.; Musa, D. Exploring racial influences on flu vaccine attitudes and behavior: Results of a national survey of White and African American adults. Vaccine 2017, 35, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Qunaibi, E.A.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy in a large-scale survey on Arabs. Elife 2021, 10, e68038. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.; Sherrard, L.; Dubé, È.; Gilbert, N. Determinants of non-vaccination against seasonal influenza. Health Rep. 2018, 10, 29. [Google Scholar]
- Subramaniam, N.; Patil, S.; Umakanthan, S.; Sharma, R. COVID-19 Vaccine Hesitancy and Resistance in India Explored through a Population-Based Longitudinal Survey. Vaccines 2021, 9, 1064. [Google Scholar] [CrossRef] [PubMed]
- Syed Alwi, S.A.R.; Rafidah, E.; Zurraini, A.; Juslina, O.; Brohi, I.B.; Lukas, S. A survey on COVID-19 vaccine acceptance and concern among Malaysians. BMC Public Health 2021, 21, 1129. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.; Cohen, A.; Norris, S.; Martinson, N.; von Mollendorf, C.; Tempia, S.; Walaza, S.; Madhi, S.; McMorrow, M.; Variava, E.; et al. Knowledge, attitudes, and practices about influenza illness and vaccination: A cross-sectional survey in two South African communities. Influenza 2016, 10, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Amlôt, R.; Weinman, J.; Yiend, J.; Rubin, G. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; He, Y.; Shi, Y. Parents’ and Guardians’ Willingness to Vaccinate Their Children against COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 179. [Google Scholar] [CrossRef] [PubMed]
- Shehata, A.A.; Parvin, R.; Nagy, A.; Wang, A.; Azhar, T.M.; Attia, Y.A.; Azhar, E.I.; Paul, A.E.; Rahmatullah, M. An overview of the ongoing challenges in SARS-CoV-2 global control. Ger. J. Microbiol. 2021, 1, 1–18. [Google Scholar] [CrossRef]


{kind=link}
| Study | Methods | Participants | Causes of Vaccine Hesitancy |
|---|---|---|---|
| Ahmed et al. [6] | Cross-sectional survey | >18 years, residing in Somalia (n = 4543) | Cultural reasons, not needed (6.22% of respondents felt it was ineffective) and it being dangerous (9.33% of respondents were scared of side effects) |
| Ahmed et al. [7] | Cross-sectional survey | >18 years, residing in Pakistan. (n = 655) | Not needed (belief that a Muslim’s trust in God is enough protection was significantly associated with vaccine hesitancy (AOR 2.45; 95% CI 1.34–4.48), vaccination is dangerous, lack of trust and cultural reasons |
| Dorman, et al. [8] | Cross-sectional survey | >18 years, residing in Orange County, USA, (n = 26,324) | Not needed, vaccination is dangerous (confidence in vaccination safety was a key determinant of willingness to be vaccinated (r = 0.723, p < 0.001)) |
| El-Elimat et al. [9] | Cross-sectional survey | >18 years, residing in Jordan (n = 3100) | Lack of trust, vaccination is dangerous (<60% respondents believed that pharmaceutical companies would be able to make a safe and effective vaccination; 49.6% reported that they would not have the vaccine due to side effects) |
| Galistianiet et al. [10] | Cross-sectional survey | Aged 20–59 years, residing in Hungary (n = 1631) | Not needed (55.4% of unvaccinated participants did not believe that influenza vaccination was the best way to prevent influenza); vaccination is dangerous |
| Kreps et al. [11] | Cross-sectional survey | >18 years and above. (n = 1027) | Not needed; vaccination is dangerous (63.9% of the hesitant respondents thought the side effects would be severe) |
| Kumari et al. [12] | Thematic analysis of focus group discussions | >18 years, residing in India (n = 39). | Not needed, dangerous, lack of trust (the study findings suggested that trust in the safety of vaccines was a driver for a positive attitude towards vaccine acceptance) |
| Montalti, et al. [13] | Cross-sectional survey | >18 years old from Bologna and Palermo (n = 443) | Not needed, dangerous, lack of trust (24.4% of respondents in one city cited they were aware of cases where people had become “damaged” as a result of vaccination) |
| Quinn et al. [14] | Cross-sectional survey | 819 African American 838 White respondents, all >18 years | Not needed (African Americans had a statistically significant higher dependency on naturalism as an alternative to vaccination), dangerous, lack of trust |
| Qunaibi et al. [15] | Cross-sectional survey | Adults of Arab ethnicity from 145 countries (n = 36,220) | Not needed, dangerous (55.7% of respondents had concerns about the safety of the vaccine), lack of trust |
| Roy et al. [16] | Cross-sectional study | >18 years in US (n = 108,700) | Not needed (66–74% respondents felt it was not necessary), dangerous, lack of trust |
| Subramaniam et al. [17] | Population-based longitudinal survey | >18 years and over residing in India (n = 3000) | Not needed (8.1% of vaccine resistant respondents), dangerous, lack of trust |
| Syed et al. [18] | Cross-sectional study | >18 years, residing in Malaysia (n = 1411) | Not needed, dangerous (including fear of side-effects (95.8%, RII = 0.98)), lack of trust, cultural reasons |
| Wong et al. [19] | Cross-sectional survey | >18 years from 973 households in Soweto and 1442 households in Klerksdorp | Not needed (some participants believed that the influenza vaccine would not prevent influenza (Soweto: 23, 19%; Klerksdorp: 17, 19%; p = 0.9)), dangerous, lack of trust and cultural reasons |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, S.; Shah, Z.; Garfield, S. Causes of Vaccine Hesitancy in Adults for the Influenza and COVID-19 Vaccines: A Systematic Literature Review. Vaccines 2022, 10, 1518. https://doi.org/10.3390/vaccines10091518
Kumar S, Shah Z, Garfield S. Causes of Vaccine Hesitancy in Adults for the Influenza and COVID-19 Vaccines: A Systematic Literature Review. Vaccines. 2022; 10(9):1518. https://doi.org/10.3390/vaccines10091518
Chicago/Turabian StyleKumar, Simran, Zayna Shah, and Sara Garfield. 2022. "Causes of Vaccine Hesitancy in Adults for the Influenza and COVID-19 Vaccines: A Systematic Literature Review" Vaccines 10, no. 9: 1518. https://doi.org/10.3390/vaccines10091518
APA StyleKumar, S., Shah, Z., & Garfield, S. (2022). Causes of Vaccine Hesitancy in Adults for the Influenza and COVID-19 Vaccines: A Systematic Literature Review. Vaccines, 10(9), 1518. https://doi.org/10.3390/vaccines10091518