
Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination
 , , , , ,
, , , , ,  , , , ,
, , , ,  , ,
, ,  , and add
Show full author list
, and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fenner, F. Global Eradication of Smallpox. Clin. Infect. Dis. 1982, 4, 916–930. [Google Scholar] [CrossRef]
- Hammarlund, E.; Lewis, M.W.; Carter, S.V.; Amanna, I.; Hansen, S.G.; Strelow, L.I.; Wong, S.W.; Yoshihara, P.; Hanifin, J.M.; Slifka, M.K. Multiple diagnostic techniques identify previously vaccinated individuals with protective immunity against monkeypox. Nat. Med. 2005, 11, 1005–1011. [Google Scholar] [CrossRef]
- Xu, R.; Johnson, A.J.; Liggitt, D.; Bevan, M.J. Cellular and Humoral Immunity against Vaccinia Virus Infection of Mice. J. Immunol. 2004, 172, 6265–6271. [Google Scholar] [CrossRef]
- Xiao, Y.; Isaacs, S.N. Therapeutic Vaccines and Antibodies for Treatment of Orthopoxvirus Infections. Viruses 2010, 2, 2381–2403. [Google Scholar] [CrossRef]
- Noble, J.; Mack, T.M.; Thomas, D.B. A Prospective Study of Serum Antibody and Protection Against Smallpox. Am. J. Trop. Med. Hyg. 1972, 21, 214–218. [Google Scholar]
- Moss, B. Smallpox vaccines: Targets of protective immunity. Immunol. Rev. 2011, 239, 8–26. [Google Scholar] [CrossRef] [PubMed]
- Golden, J.W.; Hooper, J.W. The strategic use of novel smallpox vaccines in the post-eradication world. Expert Rev. Vaccines 2011, 10, 1021–1035. [Google Scholar] [CrossRef]
- Ennis, F.A.; Cruz, J.; Demkowicz, W.E., Jr.; Rothman, A.L.; McClain, D.J. Primary Induction of Human CD8 + Cytotoxic T Lymphocytes and Interferon-γ–Producing T Cells after Smallpox Vaccination. J. Infect. Dis. 2002, 185, 1657–1659. [Google Scholar] [CrossRef]
- Redfield, R.R.; Wright, D.C.; James, W.D.; Jones, T.S.; Brown, C.; Burke, D.S. Disseminated Vaccinia in a Military Recruit with Human Immunodeficiency Virus (HIV) Disease. N. Engl. J. Med. 1987, 316, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Scientific American. I Was Vaccinated against Smallpox 40 Years Ago. Am I Still Protected? 2022. Available online: https://www.scientificamerican.com/article/i-was-vaccinated-against/ (accessed on 20 April 2023).
- Chan, C.E.Z.; Wong, S.K.K.; Yazid, N.B.M.; Ng, O.T.; Marimuthu, K.; Chan, M.; Howe, H.S.; Leo, Y.-S.; Leung, B.P.; Vasoo, S.S.; et al. Residual Humoral Immunity Sustained Over Decades in a Cohort of Vaccinia-Vaccinated Individuals. J. Infect. Dis. 2022, 227, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Combadiere, B.; Boissonnas, A.; Carcelain, G.; Lefranc, E.; Samri, A.; Bricaire, F.; Debre, P.; Autran, B. Distinct Time Effects of Vaccination on Long-Term Proliferative and IFN-γ–producing T Cell Memory to Smallpox in Humans. J. Exp. Med. 2004, 199, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Taub, D.D.; Ershler, W.B.; Janowski, M.; Artz, A.; Key, M.L.; McKelvey, J.; Muller, D.; Moss, B.; Ferrucci, L.; Duffey, P.L.; et al. Immunity from Smallpox Vaccine Persists for Decades: A Longitudinal Study. Am. J. Med. 2008, 121, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Costantino, V.; Trent, M.J.; Sullivan, J.S.; Kunasekaran, M.P.; Gray, R.; MacIntyre, R. Serological Immunity to Smallpox in New South Wales, Australia. Viruses 2020, 12, 554. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Figueiredo, P.; da Silva-Fernandes, A.T.; Mota, B.E.F.; Costa, G.B.; Borges, I.A.; Ferreira, P.C.P.; Abrahão, J.S.; Braga, E.M.; Kroon, E.G.; de Souza Trindade, G. Evaluating anti-Orthopoxvirus antibodies in individuals from Brazilian rural areas prior to the bovine vaccinia era. Mem. Inst. Oswaldo Cruz 2015, 110, 804–808. [Google Scholar] [CrossRef]
- Gushchin, V.A.; Ogarkova, D.A.; Dolzhikova, I.V.; Zubkova, O.V.; Grigoriev, I.V.; Pochtovyi, A.A.; Iliukhina, A.A.; Ozharovskaia, T.A.; Kuznetsova, N.A.; Kustova, D.D.; et al. Estimation of anti-orthopoxvirus immunity in Moscow residents and potential risks of spreading Monkeypox virus. Front. Immunol. 2022, 13, 1023164. [Google Scholar] [CrossRef]
- Hammarlund, E.; Lewis, M.W.; Hansen, S.G.; Strelow, L.I.; Nelson, J.A.; Sexton, G.J.; Hanifin, J.M.; Slifka, M.K. Duration of antiviral immunity after smallpox vaccination. Nat. Med. 2003, 9, 1131–1137. [Google Scholar] [CrossRef]
- Kim, S.-H.; Yeo, S.-G.; Park, K.-H.; Bang, J.-W.; Kim, H.-B.; Kim, N.-J.; Jee, Y.; Cho, H.; Oh, M.-D.; Choe, K.-W. The persistence of humoral and cellular immunities more than three decades after smallpox vaccination. Clin. Microbiol. Infect. 2007, 13, 91–93. [Google Scholar] [CrossRef]
- Poccia, F.; Gioia, C.; Montesano, C.; Martini, F.; Horejsh, D.; Castilletti, C.; Pucillo, L.P.; Capobianchi, M.R.; Ippolito, G. Flow Cytometry and T-Cell Response Monitoring after Smallpox Vaccination. Emerg. Infect. Dis. 2003, 9, 1468–1470. [Google Scholar] [CrossRef]
- Pütz, M.M.; Alberini, I.; Midgley, C.M.; Manini, I.; Montomoli, E.; Smith, G.L. Prevalence of antibodies to Vaccinia virus after smallpox vaccination in Italy. J. Gen. Virol. 2005, 86, 2955–2960. [Google Scholar] [CrossRef]
- Sammartino, J.C.; Cassaniti, I.; Ferrari, A.; Piralla, A.; Bergami, F.; Arena, F.A.; Paolucci, S.; Rovida, F.; Lilleri, D.; Percivalle, E.; et al. Characterization of immune response against monkeypox virus in cohorts of infected patients, historic and newly vaccinated subjects. J. Med. Virol. 2023, 95, e28778. [Google Scholar] [CrossRef]
- Edghill-Smith, Y.; Golding, H.; Manischewitz, J.; King, L.R.; Scott, D.; Bray, M.; Nalca, A.; Hooper, J.W.; Whitehouse, C.A.; Schmitz, J.E.; et al. Smallpox vaccine–induced antibodies are necessary and sufficient for protection against monkeypox virus. Nat. Med. 2005, 11, 740–747. [Google Scholar] [CrossRef]
- McCollum, A.M.; Damon, I.K. Human Monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar] [CrossRef]
- Akter, F.; Hasan, T.B.; Alam, F.; Das, A.; Afrin, S.; Maisha, S.; Al Masud, A.; KM, S. Effect of prior immunisation with smallpox vaccine for protection against human Mpox: A systematic review. Rev. Med. Virol. 2023, 33, e2444. [Google Scholar] [CrossRef]
- Fink, D.L.; Callaby, H.; Luintel, A.; Beynon, W.; Bond, H.; Lim, E.Y.; Gkrania-Klotsas, E.; Heskin, J.; Bracchi, M.; Rathish, B.; et al. Clinical features and management of individuals admitted to hospital with monkeypox and associated complications across the UK: A retrospective cohort study. Lancet Infect. Dis. 2022, 23, 589–597. [Google Scholar] [CrossRef]
- Caria, J.; Pinto, R.; Leal, E.; Almeida, V.; Cristóvão, G.; Gonçalves, A.C.; Torres, M.; Santos, M.B.; Pinheiro, H.; Póvoas, D.; et al. Clinical and Epidemiological Features of Hospitalized and Ambulatory Patients with Human Monkeypox Infection: A Retrospective Observational Study in Portugal. Infect. Dis. Rep. 2022, 14, 810–823. [Google Scholar] [CrossRef] [PubMed]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: A prospective observational cohort study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Colavita, F.; Matusali, G.; Mazzotta, V.; Bettini, A.; Lapa, D.; Meschi, S.; Francalancia, M.; Pinnetti, C.; Bordi, L.; Mizzoni, K.; et al. Profiling the acute phase antibody response against mpox virus in patients infected during the 2022 outbreak. J. Med. Virol. 2023, 95, e28851. [Google Scholar] [CrossRef] [PubMed]
- Grifoni, A.; Zhang, Y.; Tarke, A.; Sidney, J.; Rubiro, P.; Reina-Campos, M.; Filaci, G.; Dan, J.M.; Scheuermann, R.H.; Sette, A. Defining antigen targets to dissect vaccinia virus and monkeypox virus-specific T cell responses in humans. Cell Host Microbe 2022, 30, 1662–1670.e4. [Google Scholar] [CrossRef]
- Adamo, S.; Gao, Y.; Sekine, T.; Mily, A.; Wu, J.; Storgärd, E.; Westergren, V.; Filén, F.; Treutiger, C.-J.; Sandberg, J.K.; et al. Memory profiles distinguish cross-reactive and virus-specific T cell immunity to mpox. Cell Host Microbe 2023, 31, 928–936.e4. [Google Scholar] [CrossRef] [PubMed]
- Cohn, H.; Bloom, N.; Cai, G.Y.; Clark, J.J.; Tarke, A.; Bermúdez-González, M.C.; Altman, D.R.; Lugo, L.A.; Lobo, F.P.; Marquez, S.; et al. Mpox vaccine and infection-driven human immune signatures: An immunological analysis of an observational study. Lancet Infect. Dis. 2023. [Google Scholar] [CrossRef]
- Rehan, S.T.; Ul Hussain, H.; Nihal, K.; Sukaina, M.; Khan, Z.; Nashwan, A.J. Global Monkeypox Virus Outbreak 2022: A Bibliometric Analysis. Cureus 2023, 15, e37107. [Google Scholar] [CrossRef]
- Criscuolo, E.; Giuliani, B.; Ferrarese, R.; Ferrari, D.; Locatelli, M.; Clementi, M.; Mancini, N.; Clementi, N. Smallpox vaccination-elicited antibodies cross-neutralize 2022-Monkeypox. J. Med. Virol. 2023, 95, e28643. [Google Scholar] [CrossRef]
- Zaeck, L.M.; Lamers, M.M.; Verstrepen, B.E.; Bestebroer, T.M.; van Royen, M.E.; Götz, H.; Shamier, M.C.; van Leeuwen, L.P.M.; Schmitz, K.S.; Alblas, K.; et al. Low levels of monkeypox virus-neutralizing antibodies after MVA-BN vaccination in healthy individuals. Nat. Med. 2022, 29, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Dalton, A.F.; Diallo, A.O.; Chard, A.N.; Moulia, D.L.; Deputy, N.P.; Fothergill, A.; Kracalik, I.; Wegner, C.W.; Markus, T.M.; Pathela, P.; et al. Estimated Effectiveness of JYNNEOS Vaccine in Preventing Mpox: A Multijurisdictional Case-Control Study—United States, August 19, 2022–March 31, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Hazra, A.; Zucker, J.; Bell, E.; Flores, J.; Gordon, L.; Mitjà, O.; Suñer, C.; Lemaignen, A.; Jamard, S.; Nozza, S.; et al. Mpox in people with past infection or a complete vaccination course: A global case series. Lancet Infect. Dis. 2023. [Google Scholar] [CrossRef]
- Karem, K.L.; Reynolds, M.; Hughes, C.; Braden, Z.; Nigam, P.; Crotty, S.; Glidewell, J.; Ahmed, R.; Amara, R.; Damon, I.K. Monkeypox-Induced Immunity and Failure of Childhood Smallpox Vaccination to Provide Complete Protection. Clin. Vaccine Immunol. 2007, 14, 1318–1327. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
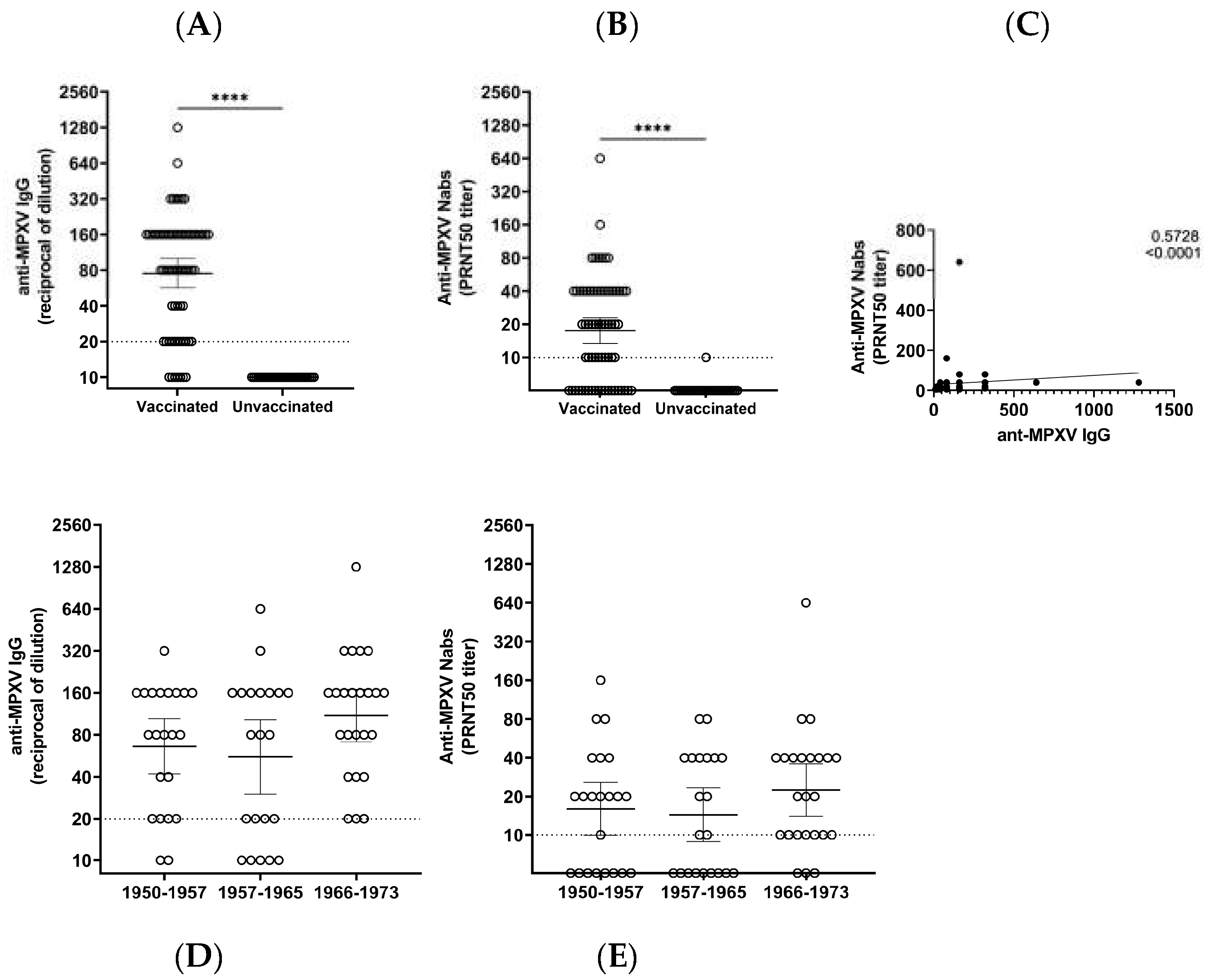
| Born between (Years) | |||
|---|---|---|---|
| 1950–1957 | 1958–1965 | 1966–1973 | |
| N. | 22 | 21 | 24 |
| IgG GMT (95%CI) | 66.2 (41.9–104) | 55.6 (30.2–102.6) | 109.9 (71.4–169.2) |
| IgG % reactive (N) | 90.1 (20) | 76.2 (16) | 100 (24) |
| Nabs GMT (95%CI) | 16.0 (10.0–25.9) | 14.4 (8.9–23.4) | 22.5 (14.0–35.9) |
| NAbs % reactive (N) | 63.6 (14) | 57.1 (12) | 87.5 (21) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matusali, G.; Petruccioli, E.; Cimini, E.; Colavita, F.; Bettini, A.; Tartaglia, E.; Sbarra, S.; Meschi, S.; Lapa, D.; Francalancia, M.; et al. Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination. Vaccines 2023, 11, 1541. https://doi.org/10.3390/vaccines11101541
Matusali G, Petruccioli E, Cimini E, Colavita F, Bettini A, Tartaglia E, Sbarra S, Meschi S, Lapa D, Francalancia M, et al. Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination. Vaccines. 2023; 11(10):1541. https://doi.org/10.3390/vaccines11101541
Chicago/Turabian StyleMatusali, Giulia, Elisa Petruccioli, Eleonora Cimini, Francesca Colavita, Aurora Bettini, Eleonora Tartaglia, Settimia Sbarra, Silvia Meschi, Daniele Lapa, Massimo Francalancia, and et al. 2023. "Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination" Vaccines 11, no. 10: 1541. https://doi.org/10.3390/vaccines11101541
APA StyleMatusali, G., Petruccioli, E., Cimini, E., Colavita, F., Bettini, A., Tartaglia, E., Sbarra, S., Meschi, S., Lapa, D., Francalancia, M., Bordi, L., Mazzotta, V., Coen, S., Mizzoni, K., Beccacece, A., Nicastri, E., Pierelli, L., Antinori, A., Girardi, E., ... Maggi, F. (2023). Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination. Vaccines, 11(10), 1541. https://doi.org/10.3390/vaccines11101541