
Mitigating Vaccine Hesitancy and Building Trust to Prevent Future Measles Outbreaks in England




Abstract
:1. Introduction
1.1. Epidemiology of Measles
1.2. History of Measles Vaccination Schedules in the UK
1.3. Measles Reporting and MMR Coverage Target for Measles Elimination in the UK
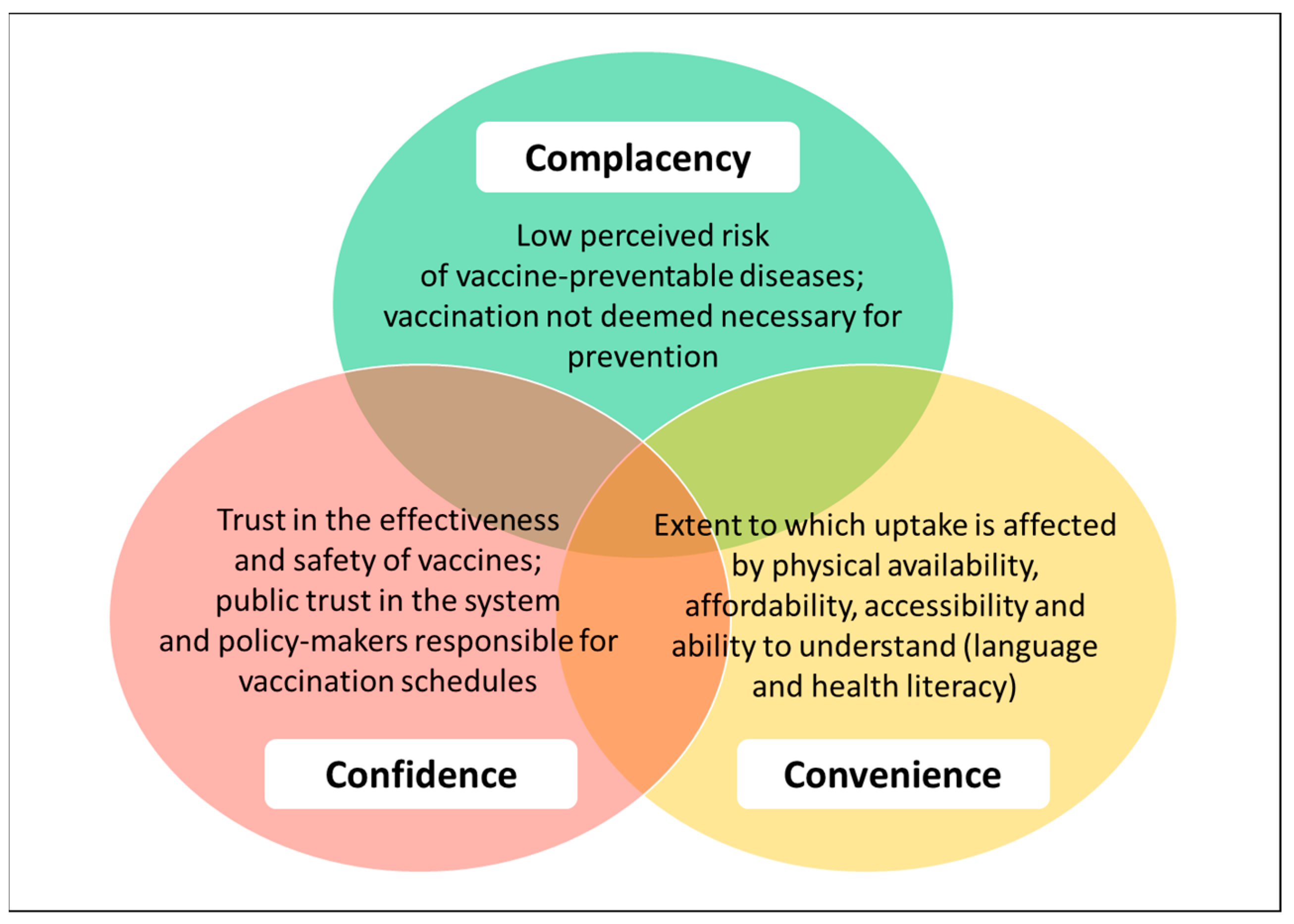
1.4. Vaccine Hesitancy
1.5. Aim of this Review
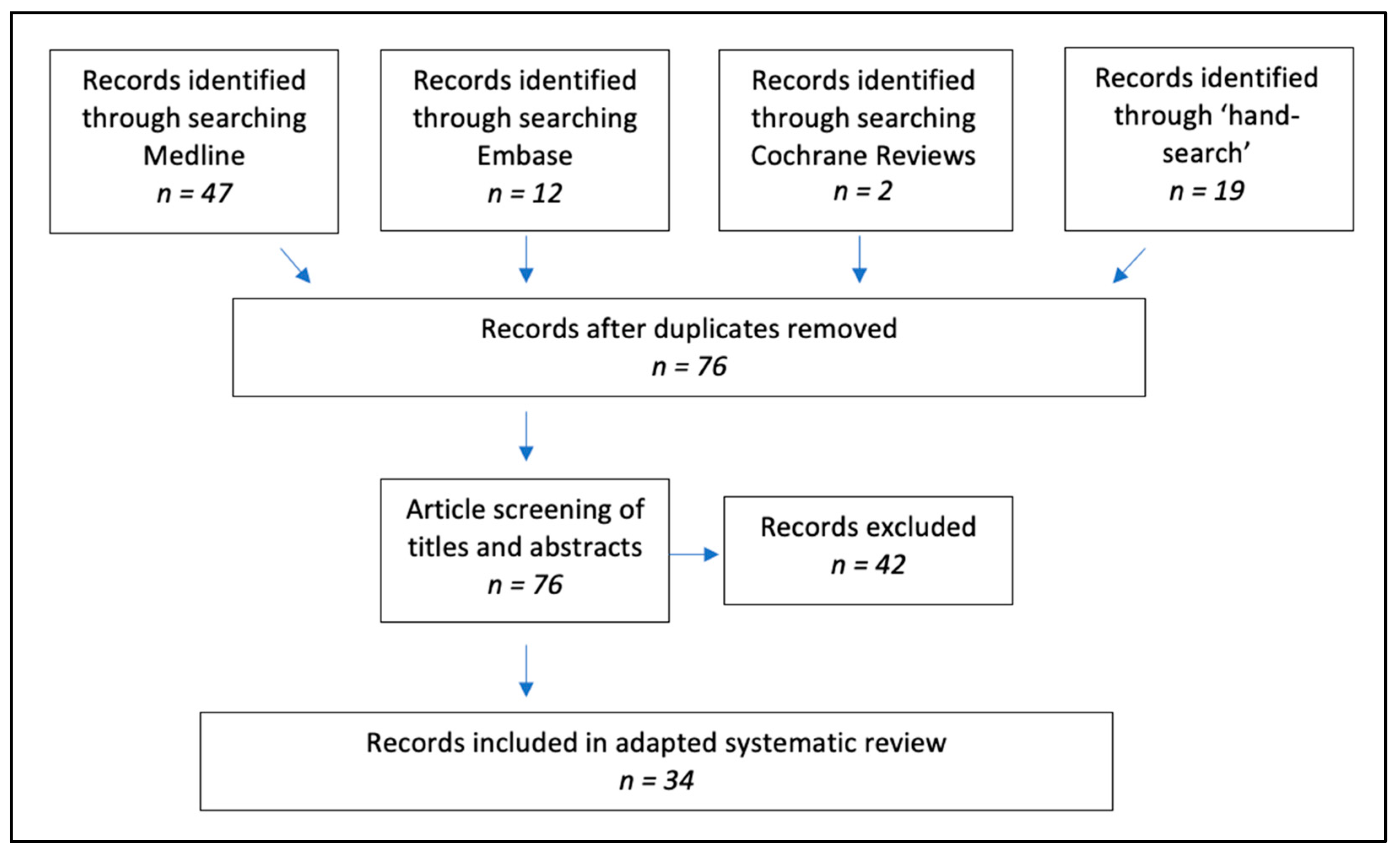
2. Materials and Methods
3. Results
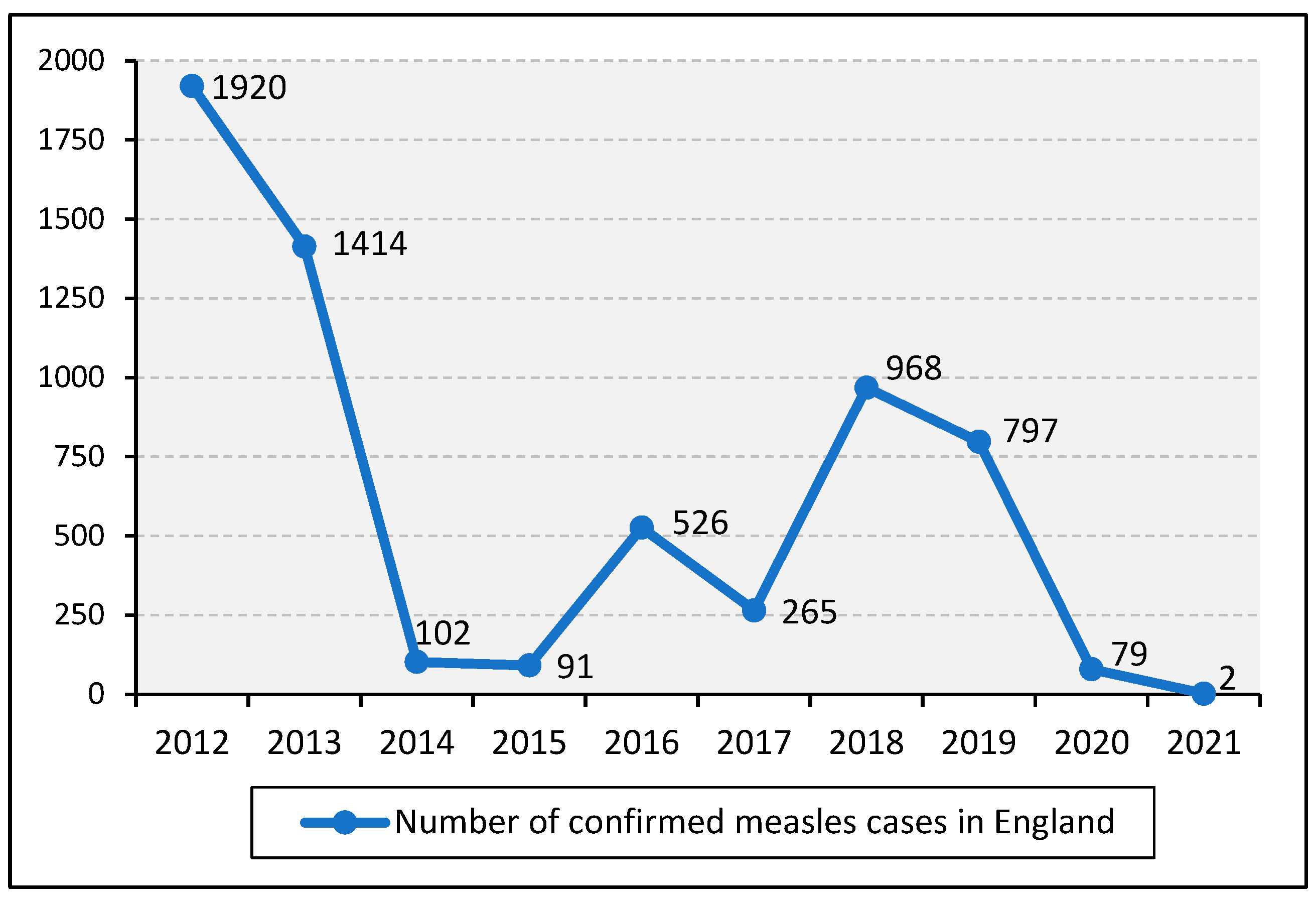
3.1. Measles Cases in England from 2012 to 2021
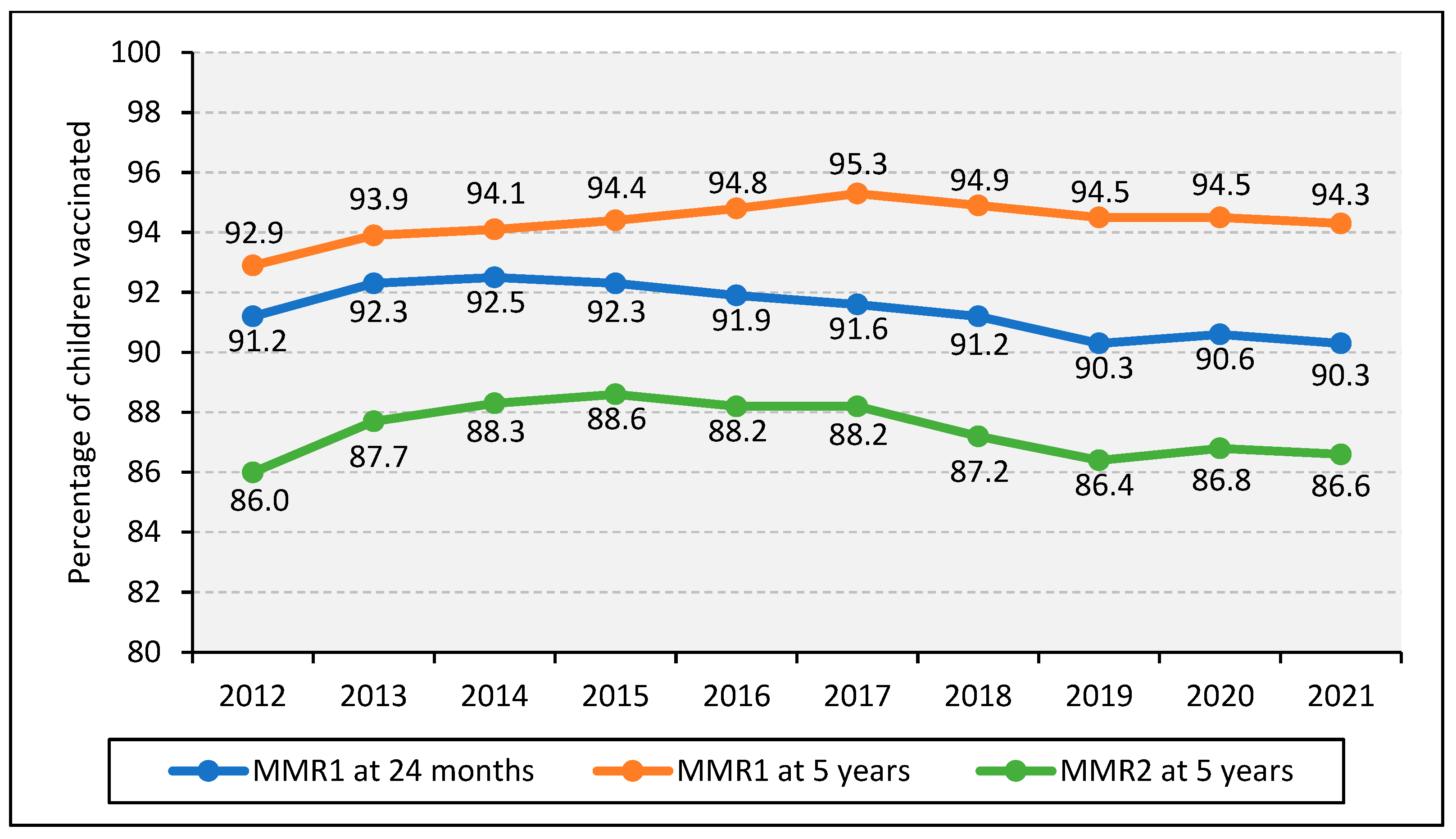
3.2. MMR Coverage in England from 2012 to 2021
3.2.1. National MMR Coverage
3.2.2. Regional MMR Coverage in England
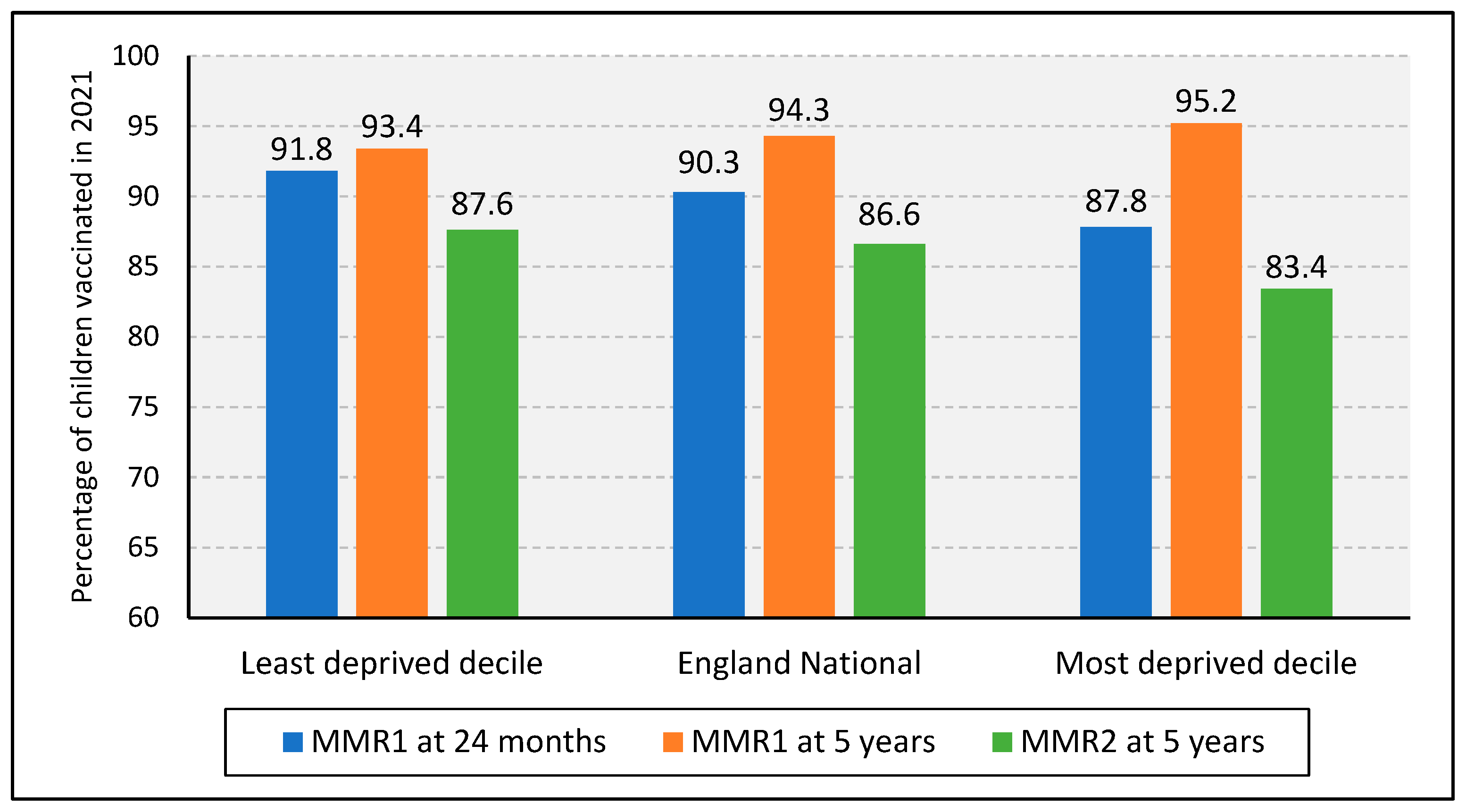
3.2.3. MMR Coverage in England by Socioeconomic Status
3.3. Literature Review: Potential Factors Associated with MMR Uptake
3.3.1. Convenience
Accessibility
Population Mobility
Information on Service Availability
Affordability and Funding
Inequalities and Sub-Populations
3.3.2. Confidence
Vaccine Safety and Effectiveness
Healthcare Professionals
Trusted Information
Mis- and Disinformation (Media and Autism)
Personal Experience
3.3.3. Complacency
Awareness of Severity of the Disease
Perceived Risk of Disease
3.4. Literature Review: Possible Interventions to Improve MMR Uptake

| Barriers | Recommendations |
|---|---|
| General vaccine hesitancy | |
| Lack of perceived trusted information [24,59,70]; concerns over combined vaccines [24,70,81]; concerns over side effects [44,65,82] |
|
| Lack of awareness of measles severity and availability of MMR vaccination programme [23,24,59] |
|
| Inequalities in service provision [22,65,73,74,75,76,77,103] |
|
| Community-specific needs are not addressed [23,24,71,78] |
|
| Inadequate immunisation training [9] |
|
| Lack of advanced information technology for surveillance [13,40] |
|
| Lack of funding [9] |
|
| Vaccine availability and affordability [20,110] |
3.4.1. Convenience
3.4.2. Confidence
3.4.3. Complacency
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| CASP | Critical Appraisal Skills Programme |
| CHIS | Child Health Information Systems |
| COVER | Cover of Vaccination Evaluated Rapidly |
| DHSC | Department of Health and Social Care |
| GP | General Practice |
| HBM | Health Belief Model |
| HPA | Health Protection Agency |
| IBIM | Immunisation Beliefs and Intentions Measure |
| ICS | Integrated Care System |
| IMD | Index of Multiple Deprivation |
| LA | Local Authority |
| LAC | Looked-After Children |
| MMR | Measles Mumps Rubella |
| MMR1 | 1st dose of Measles Mumps Rubella vaccine |
| MMR2 | 2nd dose of Measles Mumps Rubella vaccine |
| MMRV | Measles Mumps Rubella Varicella |
| NHS | National Health Service |
| NHSE | National Health Service England |
| ONS | Office for National Statistics |
| PHE | Public Health England |
| R0 | Reproductive number |
| SDH | Social Determinants of Health |
| UK | United Kingdom |
| UK HAS | United Kingdom Health Security Agency |
| WHO | World Health Organization |
Appendix A
| # | Search Term | MeSH/ Free Text | Search Field Limits | MEDLINE (26 May 2022) | EMBASE (26 May 2022) | Cochrane (26 May 2022) |
|---|---|---|---|---|---|---|
| 1 | Measles-Mumps-Rubella Vaccine | MeSH | All fields | 3034 | 8053 | 173 |
| 2 | Measles | MeSH | All fields | 14,556 | 19,682 | 296 |
| 3 | MeaslesVaccine | MeSH | All fields | 7174 | 9836 | 383 |
| 4 | Measles virus | MeSH | All fields | 6607 | 8861 | 81 |
| 5 | 1 OR 2 OR 3 OR 4 | 21,941 | 33,166 | 512 | ||
| 6 | England | MeSH | All fields | 92,384 | 32,558 | 2671 |
| 7 | 5 AND 6 | 295 | 57 | 5 | ||
| 8 | Vaccin * | Free text | Title or abstract or key word | 442,491 | 549,644 | 29,204 |
| 9 | 7 AND 8 | 237 | 47 | 5 | ||
| 10 | Uptake | Free text | Title or abstract or key word | 428,025 | 569,433 | 22,472 |
| 11 | Vaccination Coverage | MeSH | All fields | 2125 | 4281 | 31 |
| 12 | 10 OR 11 | 429,775 | 573171 | 22,493 | ||
| 13 | 9 AND 12 | 47 | 12 | 2 |
References
- Measles: The Green Book. In The Green Book; Public Health England: London, UK, 2019.
- Moss, W.J. Measles. Lancet 2017, 390, 2490–2502. [Google Scholar] [CrossRef] [PubMed]
- Hübschen, J.; Gouandjika-Vasilache, I.; Dina, J. Measles. Lancet 2022, 399, 678–690. [Google Scholar] [CrossRef]
- World Health Organization Measles vaccines: WHO position paper, April 2017–Recommendations. Vaccine 2019, 37, 219–222. [CrossRef]
- Durrheim, D.N. Measles eradication—Retreating is not an option. Lancet Infect. Dis. 2020, 20, e138–e141. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A.; Orenstein, W.A.; Offit, P.A. Vaccines, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2017; ISBN 9780323393010. [Google Scholar]
- UK Health Security Agency. Measles Notifications and Deaths in England and Wales: 1940 to 2020. 2022. Available online: https://www.gov.uk/government/publications/measles-deaths-by-age-group-from-1980-to-2013-ons-data/measles-notifications-and-deaths-in-england-and-wales-1940-to-2013 (accessed on 23 April 2022).
- Di Pietrantonj, C.; Rivetti, A.; Marchione, P.; Debalini, M.G.; Demicheli, V. Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Public Health England. National Measles Guidelines; Public Health England: London, UK, 2019.
- Department of Health UK. NHS Public Health Functions Agreement 2015–2016: Service Specification No.10. Measles, Mumps and Rubella [MMR] Immunisation Programme [Internet]. 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/383184/1516_No10_Measles_Mumps_and_Rubella__MMR__Immunisation_Programme_FINAL.pdf (accessed on 21 March 2022).
- Williams, J.R.; Manfredi, P.; Butler, A.R.; Ciofi Degli Atti, M.; Salmaso, S. Heterogeneity in regional notification patterns and its impact on aggregate national case notification data: The example of measles in Italy. BMC Public Health 2003, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.E.; Rota, P.A.; Goodson, J.L.; Williams, D.; Abernathy, E.; Takeda, M.; Mulders, M.N. Genetic Characterization of Measles and Rubella Viruses Detected Through Global Measles and Rubella Elimination Surveillance, 2016–2018. MMWR. Morb. Mortal. Wkly. Rep. 2019, 68, 587–591. [Google Scholar] [CrossRef] [Green Version]
- Mette, A.; Reuss, A.M.; Feig, M.; Kappelmayer, L.; Siedler, A.; Eckmanns, T.; Poggensee, G. Under-Reporting of Measles. Dtsch Arztebl Int. 2011, 108, 191–196. [Google Scholar] [CrossRef]
- Richard, J.-L.; Vidondo, B.; Mäusezahl, M. A 5-year comparison of performance of sentinel and mandatory notification surveillance systems for measles in Switzerland. Eur. J. Epidemiology 2007, 23, 55–65. [Google Scholar] [CrossRef]
- Public Health England. Measles and rubella elimination UK strategy. In PHE Publications; Public Health England: London, UK, 2019. [Google Scholar]
- UK Health Security Agency. UK Measles and Rubella Elimination Indicators and Status; UK Health Security Agency: London, UK, 2022.
- De Serres, G.; Gay, N.J.; Farrington, C.P. Epidemiology of transmissible diseases after elimination. Am. J. Epidemiol. 2000, 151, 11. [Google Scholar] [CrossRef]
- World Health Organization. Global Measles and Rubella: Strategic Plan 2012–2020; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. Measles Mortality Reduction and Regional Elimination Strategic Plan 2001–2005; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy. Sage Report. 2014. Available online: https://www.asset-scienceinsociety.eu/sites/default/files/sage_working_group_revised_report_vaccine_hesitancy.pdf (accessed on 19 December 2022).
- Aranda, S. Ten Threats to Global Health in 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Public Health England. National Immunisation Programme: Health Equity Audit; Public Health England: London, UK, 2021.
- Wilder-Smith, A.B.; Qureshi, K. Resurgence of Measles in Europe: A Systematic Review on Parental Attitudes and Beliefs of Measles Vaccine. J. Epidemiology Glob. Health 2019, 10, 46–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHALE, P.; Keenan, A.; Ghebrehewet, S. Reasons for measles cases not being vaccinated with MMR: Investigation into parents’ and carers’ views following a large measles outbreak. Epidemiology Infect. 2015, 144, 870–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulos, T.; Vynnycky, E. Estimates of the basic reproduction number for rubella using seroprevalence data and indicator-based approaches. PLOS Comput. Biol. 2022, 18, e1008858. [Google Scholar] [CrossRef] [PubMed]
- Department of Health & Social Care. Transforming the Public Health System: Reforming the Public Health System for the Challenges of Our Times. 2021. Available online: https://www.gov.uk/government/publications/transforming-the-public-health-system/transforming-the-public-health-system-reforming-the-public-health-system-for-the-challenges-of-our-times (accessed on 23 April 2022).
- Public Health England, NHS Digital. Childhood Vaccination Coverage Statistics, England-2020–2021. NHS Digital. 2021. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-immunisation-statistics/england---2020-21 (accessed on 17 December 2022).
- Health Protection Agency. UK Government Web Archive for http://www.hpa.org.uk/ [Internet]. 2022. Available online: https://webarchive.nationalarchives.gov.uk/ukgwa/*/http://www.hpa.org.uk/ (accessed on 14 May 2022).
- UK Health Security Agency. Confirmed Cases of Measles, Mumps and Rubella in England and Wales: 1996 to 2021; UK Health Security Agency: London, UK, 2022.
- UK Health Security Agency. Quarterly vaccination coverage statistics for children aged up to 5 years in the UK [COVER] programme: July to September 2021. Health Prot. Rep. 2021, 6, 7–13. [Google Scholar]
- Critical Appraisal Skills Programme. CASP (Qualitative) Checklist. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 9 January 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderberg, D.; Chevalier, A.; Wadsworth, J. Anatomy of a health scare: Education, income and the MMR controversy in the UK. J. Health Econ. 2011, 30, 515–530. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, A.; Murch, S.; Anthony, A.; Linnell, J.; Casson, D.; Malik, M.; Berelowitz, M.; Dhillon, A.; Thomson, M.; Harvey, P.; et al. RETRACTED: Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. Lancet 1998, 351, 637–641. [Google Scholar] [CrossRef]
- Laksono, B.M.; de Vries, R.D.; Verburgh, R.J.; Visser, E.G.; de Jong, A.; Fraaij, P.L.A.; Ruijs, W.L.M.; Nieuwenhuijse, D.F.; Ham, H.-J.V.D.; Koopmans, M.P.G.; et al. Studies into the mechanism of measles-associated immune suppression during a measles outbreak in the Netherlands. Nat. Commun. 2018, 9, 4944. [Google Scholar] [CrossRef] [Green Version]
- UK Health Security Agency. Laboratory confirmed cases of measles, rubella and mumps, England: July to September 2021. Health Prot. Rep. 2021, 6. Available online: https://www.gov.uk/government/publications/measles-mumps-and-rubella-lab-confirmed-cases-in-england-2021 (accessed on 19 January 2023).
- World Health Organization. Eliminating Measles and Rubella: Framework for the Verification Process in the WHO European Region; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Nicolay, N.; Mirinaviciute, G.; Mollet, T.; Celentano, L.P.; Bacci, S. Epidemiology of measles during the COVID-19 pandemic, a description of the surveillance data, 29 EU/EEA countries and the United Kingdom, January to May 2020. Eurosurveillance 2020, 25, 2001390. [Google Scholar] [CrossRef]
- World Health Organization. Global Progress against Measles Threatened Amidst COVID-19 Pandemic. 2021. Available online: https://www.who.int/news/item/10-11-2021-global-progress-against-measles-threatened-amidst-covid-19-pandemic (accessed on 1 December 2022).
- UK Health Security Agency. Measles Notifications and Confirmed Cases by Oral Fluid Testing 2013 to 2021 by Quarter. 2022 [cited ]. Available online: https://www.gov.uk/government/publications/measles-confirmed-cases (accessed on 19 January 2023).
- UK Health Security Agency. Confirmed Cases of Measles in England and Wales by Region and Age: 2012 to 2021. 2022. Available online: https://www.gov.uk/government/publications/measles-confirmed-cases/confirmed-cases-of-measles-in-england-and-wales-by-region-and-age-2012-to-2021 (accessed on 19 January 2023).
- Office for National Statistics. Estimates of the Population for the UK, England and Wales, Scotland and Northern Ireland. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland (accessed on 5 March 2020).
- Public Health England. Evaluation of Vaccine Uptake during the 2013 MMR Catch-up Campaign in England; Public Health England: London, UK, 2014.
- Sturgis, P.; Brunton-Smith, I.; Jackson, J. Trust in science, social consensus and vaccine confidence. Nat. Hum. Behav. 2021, 5, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- Office for Health Improvement & Disparities. Population Vaccination Coverage–MMR. 2021. Available online: https://fingertips.phe.org.uk/profile/health-protection/data#page/1 (accessed on 12 May 2022).
- MHCLG. The English Indices of Deprivation 2019; Minist Housing, Communities Local Government: London, UK, 2019. [Google Scholar]
- Pareek, M.; Pattison, H.M. The two-dose measles, mumps, and rubella [MMR] immunisation schedule: Factors affecting maternal intention to vaccinate. Br. J. Gen. Pract. 2000, 50, 969–971. [Google Scholar] [PubMed]
- Baugh, V.; Bosanquet, J. A measles outbreak within an Orthodox Jewish community in London, United Kingdom. Descriptive epidemiology, lessons learnt and recommendations. Eur. J. Public Health 2013, 23. [Google Scholar] [CrossRef] [Green Version]
- British Medical Association. Action to Improve Immunisation Coverage Rates Across the UK; British Medical Association: London, UK, 2020. [Google Scholar]
- Office for National Statistics. Coronavirus [COVID-19] latest Insights: Vaccines. 2022. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19latestinsights/vaccines (accessed on 23 June 2022).
- Lindholt, M.F.; Jørgensen, F.; Bor, A.; Petersen, M.B. Public acceptance of COVID-19 vaccines: Cross-national evidence on levels and individual-level predictors using observational data. BMJ Open 2021, 11, e048172. [Google Scholar] [CrossRef]
- Kadambari, S.; Goldacre, R.; Morris, E.; Goldacre, M.J.; Pollard, A.J. Indirect effects of the covid-19 pandemic on childhood infection in England: Population based observational study. BMJ 2022, 376, e067519. [Google Scholar] [CrossRef]
- Torjesen, I. Measles outbreaks likely as covid pandemic leaves millions of world’s children unvaccinated, WHO warns. BMJ 2021, 375, n2755. [Google Scholar] [CrossRef]
- McQuaid, F.; Mulholland, R.; Rai, Y.S.; Agrawal, U.; Bedford, H.; Cameron, J.C.; Gibbons, C.; Roy, P.; Sheikh, A.; Shi, T.; et al. Uptake of infant and preschool immunisations in Scotland and England during the COVID-19 pandemic: An observational study of routinely collected data. PLOS Med. 2022, 19, e1003916. [Google Scholar] [CrossRef]
- Wilkinson, E. Is anti-vaccine sentiment affecting routine childhood immunisations? BMJ 2022, 376. Available online: https://www.bmj.com/content/bmj/376/bmj.o360.full.pdf (accessed on 19 January 2023). [CrossRef]
- MacDonald, M. Commentary: Parents’ decisions on MMR vaccination for their children were based on personal experience rather than scientific evidence. Evid. Based Nurs. 2005, 8, 60. [Google Scholar] [CrossRef]
- Ferson, M.J.; Fitzsimmons, G.; Christie, D.; Woollett, H. School health nurse interventions to increase immunisation uptake in school entrants. Public Health 1995, 109, 25–29. [Google Scholar] [CrossRef]
- Public Health England. Maintaining Routine Immunisation Programmes during COVID-19; London, UK (updated June 2021). Available online: https://www.nice.org.uk/media/default/about/covid-19/specialty-guides/maintaining-immunisation-programmes.pdf (accessed on 19 January 2023).
- Freud’s Health & Behaviour Change. MMR Childhood Vaccinations: Survey Topline Results. 2022. Available online: https://khub.net/documents/135939561/174090192/2022+MMR+campaign+attitudinal+survey+results.pdf/8652d3a8-33fa-b7d6-6b12-81452d07394b (accessed on 19 December 2022).
- Robertson, R. Public Satisfaction with GP Services Drops to Lowest Level in 35 Years. The King’s Fund. 2018. Available online: https://www.kingsfund.org.uk/blog/2018/02/public-satisfaction-gp-services (accessed on 6 June 2022).
- Marchand, C.; Peckham, S. Addressing the crisis of GP recruitment and retention: A systematic review. Br. J. Gen. Pract. 2017, 67, e227–e237. [Google Scholar] [CrossRef] [Green Version]
- Fisher, R.; Allen, L.; Malhotra, A.; Alderwick, H. Tackling the inverse care law: Analysis of policies to improve general practice in deprived areas since 1990. Health Found. 2022. [Google Scholar] [CrossRef]
- Healthcare Transformers. Healthcare Hotspots in the UK. 2022. Available online: https://healthcaretransformers.com/healthcare-business/uk-healthcare-hotspots/ (accessed on 26 May 2022).
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav. Immun. 2021, 94, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Emerson, E.; Robertson, J.; Baines, S.; Hatton, C. Vaccine Coverage among Children with and without Intellectual Disabilities in the UK: Cross Sectional Study. BMC Public Health 2019, 19, 748. [Google Scholar] [CrossRef] [PubMed]
- Tuffrey, C.; Finlay, F. Immunisation status amongst children attending special schools. Ambul. Child Health 2001, 7, 213–217. [Google Scholar] [CrossRef]
- Pan American Health Organization; World Health Organization. Social Determinants of Health. 2017. Available online: https://www.paho.org/en/topics/social-determinants-health (accessed on 12 January 2023).
- U.S. Department of Health & Human Services. Healthy People 2030: Social Determinants of Health. 2022. Available online: https://health.gov/healthypeople/priority-areas/social-determinants-health (accessed on 12 January 2023).
- World Health Organization. A Conceptual Framework for Action on the Social Determinants of Health. 2010. Available online: https://apps.who.int/iris/handle/10665/44489 (accessed on 12 January 2023).
- Evans, M.; Stoddart, H.; Condon, L.; Freeman, E.; Grizzell, M.; Mullen, R. Parents’ perspectives on the MMR immunisation: A focus group study. Br. J. Gen. Pract. 2001, 51, 904–910. [Google Scholar]
- Wombwell, E.; Fangman, M.T.; Yoder, A.K.; Spero, D.L. Religious Barriers to Measles Vaccination. J. Commun. Health 2015, 40, 597–604. [Google Scholar] [CrossRef]
- Public Health England. Guide to the Use of Human and Animal Products in Vaccines. Guidance. 2021. Available online: https://www.gov.uk/government/publications/use-of-human-and-animal-products-in-vaccines/guide-to-the-use-of-human-and-animal-products-in-vaccines (accessed on 6 June 2022).
- Marmot, M. Health Equity in England: The Marmot Review 10 Years on. BMJ 2020, 368, m693. [Google Scholar] [CrossRef]
- Crocker-Buque, T.; Edelstein, M.; Mounier-Jack, S. Interventions to reduce inequalities in vaccine uptake in children and adolescents aged <19 years: A systematic review. J. Epidemiol. Community Health 2016, 71, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Kc, A.; Chen, C.; Huang, Y.; Wang, Y.; Zou, S.; Zhou, H. Inequality in measles vaccination coverage in the “big six” countries of the WHO South-East Asia region. Hum. Vaccines Immunother. 2020, 16, 1485–1497. [Google Scholar] [CrossRef]
- Hungerford, D.; Macpherson, P.; Farmer, S.; Ghebrehewet, S.; Seddon, D.; Vivancos, R.; Keenan, A. Effect of socioeconomic deprivation on uptake of measles, mumps and rubella vaccination in Liverpool, UK over 16 years: A longitudinal ecological study. Epidemiology Infect. 2015, 144, 1201–1211. [Google Scholar] [CrossRef]
- Torracinta, L.; Tanner, R.; Vanderslott, S. MMR Vaccine Attitude and Uptake Research in the United Kingdom: A Critical Review. Vaccines 2021, 9, 402. [Google Scholar] [CrossRef]
- Ellis, N.; Walker-Todd, E.; Heffernan, C. Influences on childhood immunisation decision-making in London’s Gypsy and Traveller communities. Br. J. Nurs. 2020, 29, 822–826. [Google Scholar] [CrossRef] [PubMed]
- UK Government. Regional ethnic diversity. Ethnicity Facts and Figures 22 December 2022. Available online: https://www.ethnicity-facts-figures.service.gov.uk/uk-population-by-ethnicity/national-and-regional-populations/regional-ethnic-diversity/latest (accessed on 19 January 2023).
- Murray, C.; Smart, S. Regionalising Migration: The North East as a Case Study. Manchester Institute for Public Policy Research (IPPR) 2017. Available online: https://www.ippr.org/files/publications/pdf/regionalising-migration-NE-as-case-study_Jan2017.pdf (accessed on 19 January 2023).
- Casiday, R.; Cresswell, T.; Wilson, D.; Panter-Brick, C. A survey of UK parental attitudes to the MMR vaccine and trust in medical authority. Vaccine 2006, 24, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Motta, M.; Stecula, D. Quantifying the effect of Wakefield et al. [1998] on skepticism about MMR vaccine safety in the U.S. PLoS ONE 2021, 16, e0256395. [Google Scholar] [CrossRef]
- Allan, N.; Harden, J. Parental decision-making in uptake of the MMR vaccination: A systematic review of qualitative literature. J. Public Health 2015, 37, 678–687. [Google Scholar] [CrossRef] [Green Version]
- Hilton, S.; Petticrew, M.; Hunt, K. Parents’ champions vs. vested interests: Who do parents believe about MMR? A qualitative study. BMC Public Health 2007, 7, 42. [Google Scholar] [CrossRef] [Green Version]
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Impicciatore, P.; Bosetti, C.; Schiavio, S.; Pandolfini, C.; Bonati, M. Mothers as Active Partners in the Prevention of Childhood Diseases: Maternal Factors Related to Immunization Status of Preschool Children in Italy. Prev. Med. 2000, 31, 49–55. [Google Scholar] [CrossRef]
- Robert Koch Institute. The 20 Most Frequent Objections to Vaccinations. Robert Koch Institute. 2016. Available online: https://www.rki.de/EN/Content/Institute/DepartmentsUnits/InfDiseaseEpidem/Div33/Objections_and_Responses.html;jsessionid=F8CFD5291B76B2A4BFC209E5850E47D3.internet072#doc8185752bodyText8 (accessed on 6 June 2022).
- Oyedele, O.O.; Odemuyiwa, S.O.; Ammerlaan, W.; Muller, C.P.; Adu, F.D. Passive Immunity to Measles in the Breastmilk and Cord Blood of Some Nigerian Subjects. J. Trop. Pediatr. 2005, 51, 45–48. [Google Scholar] [CrossRef] [Green Version]
- Rao, T.S.; Andrade, C. The MMR vaccine and autism: Sensation, refutation, retraction, and fraud. Indian J. Psychiatry 2011, 53, 95–96. [Google Scholar] [CrossRef]
- McCartney, M. MMR, measles, and the South Wales Evening Post. BMJ 2013, 346, f2598. [Google Scholar] [CrossRef] [PubMed]
- Deer, B. How the vaccine crisis was meant to make money. BMJ 2011, 342, c5258. [Google Scholar] [CrossRef] [PubMed]
- Burki, T. Vaccine misinformation and social media. Lancet Digit. Health 2019, 1, e258–e259. [Google Scholar] [CrossRef] [Green Version]
- Stecula, D.A.; Kuru, O.; Jamieson, K.H. How Trust in Experts and Media Use Affect Acceptance of Common Anti-Vaccination Claims. Harv. Kennedy Sch. Misinformation Rev. 2020. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- Wawrzuta, D.; Jaworski, M.; Gotlib, J.; Panczyk, M. Social Media Sharing of Articles About Measles in a European Context: Text Analysis Study. J. Med. Internet Res. 2021, 23, e30150. [Google Scholar] [CrossRef]
- Brown, K.; Fraser, G.; Ramsay, M.; Shanley, R.; Cowley, N.; Van Wijgerden, J.; Toff, P.; Falconer, M.; Hudson, M.; Green, J.; et al. Attitudinal and Demographic Predictors of Measles-Mumps-Rubella Vaccine (MMR) Uptake during the UK Catch-Up Campaign 2008–09: Cross-Sectional Survey. PLoS ONE 2011, 6, e19381. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Le Menach, A.; Boxall, N.; Amirthalingam, G.; Maddock, L.; Balasegaram, S.; Mindlin, M. Increased measles–mumps–rubella (MMR) vaccine uptake in the context of a targeted immunisation campaign during a measles outbreak in a vaccine-reluctant community in England. Vaccine 2014, 32, 1147–1152. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: UK has highest vaccine confidence and Japan and South Korea the lowest, survey finds. BMJ 2021, 373, n1439. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease [COVID-19]. World Health Organization [WHO]. 2022. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 14 June 2022).
- World Health Organization. Periodic Intensification of Routine Immunization; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Hambidge, S.J.; Phibbs, S.L.; Chandramouli, V.; Fairclough, D.; Steiner, J.F. A Stepped Intervention Increases Well-Child Care and Immunization Rates in a Disadvantaged Population. Pediatrics 2009, 124, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.; Dyson, L.; Bedford, H.; Cheater, F.M.; Condon, L.; Crocker, A.; Emslie, C.; Ireland, L.; Kemsley, P.; Kerr, S.; et al. Understanding uptake of Immunisations in TravellIng aNd Gypsy communities (UNITING): A qualitative interview study. Health Technol. Assess. 2016, 20, 72. [Google Scholar] [CrossRef]
- Cockman, P.; Dawson, L.; Mathur, R.; Hull, S. Improving MMR vaccination rates: Herd immunity is a realistic goal. BMJ 2011, 343, d5703. [Google Scholar] [CrossRef] [PubMed]
- Crocker-Buque, T.; Mounier-Jack, S. Vaccination in England: A review of why business as usual is not enough to maintain coverage. BMC Public Health 2018, 18, 1351. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Delivering Quality Health Services: A Global Imperative for Universal Health Coverage; World Health Organization, World Bank Group, OECD: Geneva, Switzerland, 2018. [Google Scholar]
- Armitage, C.J.; Conner, M.; Prestwich, A.; De Bruin, M.; Johnston, M.; Sniehotta, F.; Epton, T. Investigating which behaviour change techniques work for whom in which contexts delivered by what means: Proposal for an international collaboratory of Centres for Understanding Behaviour Change (CUBiC). Br. J. Health Psychol. 2020, 26, 1–14. [Google Scholar] [CrossRef]
- Kok, G.; Gottlieb, N.H.; Peters, G.-J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.; Fernández, M.E.; Markham, C.; Bartholomew, L.K. A taxonomy of behaviour change methods: An Intervention Mapping approach. Health Psychol. Rev. 2015, 10, 297–312. [Google Scholar] [CrossRef] [Green Version]
- Buck, J. Further improving MMR immunisation uptake. Br. J. Gen. Pract. 2020. Available online: https://bjgp.org/content/further-improving-mmr-immunisation-uptake (accessed on 19 January 2023).
- Altinoluk-Davis, F.; Gray, S.; Bray, I. Measuring the effectiveness of catch-up MMR delivered by school nurses compared to signposting to general practice on improving MMR coverage. J. Public Health 2020, 42, 416–422. [Google Scholar] [CrossRef]
- Filia, A.; Rota, M.C.; Grossi, A.; Martinelli, D.; Prato, R.; Rezza, G. Are vaccine shortages a relevant public health issue in Europe? Results from a survey conducted in the framework of the EU Joint Action on Vaccination. Vaccine 2022, 40, 1987–1995. [Google Scholar] [CrossRef]
- Durrheim, D.N.; Andrus, J.K.; Tabassum, S.; Bashour, H.; Githanga, D.; Pfaff, G. A dangerous measles future looms beyond the COVID-19 pandemic. Nat. Med. 2021, 27, 360–361. [Google Scholar] [CrossRef]
- Coles, E.; Anderson, J.; Maxwell, M.; Harris, F.M.; Gray, N.M.; Milner, G.; MacGillivray, S. The influence of contextual factors on healthcare quality improvement initiatives: A realist review. Syst. Rev. 2020, 9, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolton-Maggs, D.; Conrad, D.; Keenan, A.; Lamden, K.; Ghebrehewet, S.; Vivancos, R. Perceptions of mumps and MMR vaccination among university students in England: An online survey. Vaccine 2012, 30, 5081–5085. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, P. Ensuring excellence in immunization services. Hum. Vaccines Immunother. 2015, 12, 252–254. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Vaccine Uptake in the General Population. 2022. Available online: www.nice.org.uk/guidance/ng218 (accessed on 15 July 2022).
- Ghebrehewet, S.; Thorrington, D.; Farmer, S.; Kearney, J.; Blissett, D.; McLeod, H.; Keenan, A. The economic cost of measles: Healthcare, public health and societal costs of the 2012-13 outbreak in Merseyside, UK. Vaccine 2016, 34, 1823–1831. [Google Scholar] [CrossRef]
- Department of Health & Social Care. Prevention is Better Than Cure: Our Vision to Help You Live Well for Longer; Department of Health & Social Care: London, UK, 2018; Volume 258.
- Office for National Statistics. COVID-19 Vaccine Refusal, UK: February to March 2021. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellhealt/bulletins/covid19vaccinerefusaluk/februarytomarch2021#main-themes-for-concern-about-or-unwillingness-to-receive-a-covid-19-vaccine (accessed on 13 July 2022).
- Harapan, H.; Shields, N.; Kachoria, A.G.; Shotwell, A.; Wagner, A.L. Religion and Measles Vaccination in Indonesia, 1991–2017. Am. J. Prev. Med. 2021, 60, S44–S52. [Google Scholar] [CrossRef]
- Bedford, H.; Donovan, H. We need to increase MMR vaccine uptake urgently. BMJ 2022, 376, o818. [Google Scholar] [CrossRef]
- Xue, H.; Gong, X.; Stevens, H. COVID-19 Vaccine Fact-Checking Posts on Facebook: Observational Study. J. Med. Internet Res. 2022, 24, e38423. [Google Scholar] [CrossRef]
- Wolfe, R.M.; Sharp, L.K. Anti-vaccinationists past and present. Br. Med. J. 2002, 325, 430. [Google Scholar] [CrossRef] [Green Version]
- Fraser, S.M. Leicester and smallpox: The Leicester method. Med. Hist. 1980, 24, 315–332. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Tailoring Immunization Programmes (TIP). Copenhagen: WHO Regional Office for Europe; 2019. Available online: https://www.who.int/europe/publications/i/item/9789289054492 (accessed on 19 January 2023).
- Chaudhuri, K.; Chakrabarti, A.; Chandan, J.S.; Bandyopadhyay, S. COVID-19 vaccine hesitancy in the UK: A longitudinal household cross-sectional study. BMC Public Health 2022, 22, 1–13. [Google Scholar] [CrossRef]
- Veli, N.; Martin, C.A.; Woolf, K.; Nazareth, J.; Pan, D.; Al-Oraibi, A.; Baggaley, B.F.; Bryant, F.; Nellums, L.B.; Pareek, M. Hesitancy for receiving regular SARS-CoV-2 vaccination in UK healthcare workers: A cross-sectional analysis from the UK-REACH study. BMC Med. 2022, 20, 386. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ukraine: Immediate Steps Needed to Prevent a Measles Outbreak Due to the Ongoing War and Low Vaccination Rates, Warns WHO. 2022. Available online: https://www.who.int/europe/news/item/27-04-2022-ukraine--immediate-steps-needed-to-prevent-a-measles-outbreak-due-to-the-ongoing-war-and-low-vaccination-rates--warns-who (accessed on 12 January 2023).
- Public Health England Campaign Resource Centre. Childhood Vaccination 2022. Public Health England. 2021. Available online: https://campaignresources.phe.gov.uk/resources/about-us (accessed on 13 July 2022).
- Jackson, C.; Cheater, F.M.; Peacock, R.; Leask, J.; Trevena, L. Evaluating a web-based MMR decision aid to support informed decision-making by UK parents: A before-and-after feasibility study. Health Educ. J. 2010, 69, 74–83. [Google Scholar] [CrossRef]
- World Health Organization. Tactics to Apply to Make Your Communications Understandable. 2022. Available online: https://www.who.int/about/communications/understandable/visuals (accessed on 15 July 2022).
- Jackson, C.; Cheater, F.M.; Harrison, W.; Peacock, R.; Bekker, H.; West, R.; Leese, B. Randomised cluster trial to support informed parental decision-making for the MMR vaccine. BMC Public Health 2011, 11, 475. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guide to Help Countries Expand Access to Essential Medicines. 2022. Available online: Ghttps://www.who.int/news/item/30-03-2020-new-who-guide-to-help-countries-expand-access-to-essential-medicines (accessed on 19 January 2023).
- World Health Organization. Global Patient Safety Action Plan 2021–2030; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/teams/integrated-health-services/patient-safety/policy/global-patient-safety-action-plan (accessed on 19 January 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Confirmed Cases of Measles | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Region | North East | North West | Yorkshire and the Humber | East Midlands | West Midlands | East of England | London | South East | South West |
| 2012 | 50 | 881 | 152 | 51 | 122 | 49 | 135 | 383 | 97 |
| 2013 | 379 | 381 | 88 | 49 | 64 | 76 | 189 | 26 | 162 |
| 2014 | 6 | 7 | 2 | 4 | 7 | 10 | 51 | 12 | 3 |
| 2015 | 2 | 2 | 2 | 0 | 2 | 1 | 65 | 4 | 13 |
| 2016 | 1 | 3 | 12 | 4 | 8 | 24 | 318 | 60 | 96 |
| 2017 | 2 | 42 | 40 | 1 | 38 | 14 | 68 | 23 | 37 |
| 2018 | 14 | 33 | 84 | 13 | 81 | 33 | 389 | 181 | 140 |
| 2019 | 3 | 51 | 28 | 48 | 14 | 102 | 461 | 68 | 22 |
| 2020 | 0 | 9 | 0 | 4 | 0 | 5 | 39 | 19 | 2 |
| Rate of Measles Infection per 100,000 Population | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Region | North East | North West | Yorkshire and the Humber | East Midlands | West Midlands | East of England | London | South East | South West |
| 2012 | 1.92 | 12.44 | 2.86 | 1.12 | 2.16 | 0.83 | 1.62 | 4.39 | 1.82 |
| 2013 | 14.52 | 5.36 | 1.65 | 1.07 | 1.13 | 1.28 | 2.25 | 0.30 | 3.01 |
| 2014 | 0.23 | 0.10 | 0.04 | 0.09 | 0.12 | 0.17 | 0.60 | 0.14 | 0.06 |
| 2015 | 0.08 | 0.03 | 0.04 | 0.00 | 0.03 | 0.02 | 0.75 | 0.04 | 0.24 |
| 2016 | 0.04 | 0.04 | 0.22 | 0.08 | 0.14 | 0.39 | 3.63 | 0.66 | 1.74 |
| 2017 | 0.08 | 0.58 | 0.73 | 0.02 | 0.65 | 0.23 | 0.77 | 0.25 | 0.67 |
| 2018 | 0.53 | 0.45 | 1.53 | 0.27 | 1.37 | 0.53 | 4.37 | 1.98 | 2.50 |
| 2019 | 0.11 | 0.69 | 0.51 | 0.99 | 0.24 | 1.64 | 5.14 | 0.74 | 0.39 |
| 2020 | 0.00 | 0.12 | 0.00 | 0.08 | 0.00 | 0.08 | 0.43 | 0.21 | 0.04 |
| Percentage of Children Vaccinated with MMR by Their Second Birthday | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Region | North East | North West | Yorkshire and the Humber | East Midlands | West Midlands | East of England | London | South East | South West |
| 2012 | 93.0 | 93.4 | 93.1 | 92.9 | 92.0 | 91.8 | 86.1 | 92.1 | 91.7 |
| 2013 | 94.1 | 94.9 | 94.2 | 94.0 | 92.7 | 92.8 | 87.1 | 92.6 | 93.5 |
| 2014 | 95.5 | 94.8 | 94.7 | 94.9 | 93.6 | 93.7 | 87.5 | 91.8 | 94.2 |
| 2015 | 95.2 | 94.0 | 94.3 | 94.3 | 93.5 | 93.9 | 87.3 | 91.1 | 93.7 |
| 2016 | 95.0 | 92.9 | 94.0 | 94.1 | 93.1 | 93.5 | 86.4 | 91.9 | 92.9 |
| 2017 | 94.9 | 93.6 | 94.0 | 93.6 | 93.2 | 93.8 | 85.1 | 90.8 | 93.1 |
| 2018 | 94.5 | 92.9 | 93.3 | 93.1 | 91.2 | 92.4 | 85.1 | 91.5 | 93.3 |
| 2019 | 94.5 | 92.4 | 92.8 | 92.0 | 90.6 | 91.3 | 83.0 | 91.4 | 93.0 |
| 2020 | 95.1 | 91.9 | 92.6 | 92.3 | 90.3 | 91.7 | 83.6 | 92.7 | 93.3 |
| 2021 | 95.3 | 91.0 | 92.3 | 92.4 | 90.2 | 92.6 | 82.4 | 92.3 | 93.3 |
| Percentage of Children Vaccinated with MMR by Their Fifth Birthday | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Region | North East | North West | Yorkshire and the Humber | East Midlands | West Midlands | East of England | London | South East | South West |
| MMR1 | 97.0 | 95.2 | 95.8 | 95.7 | 94.4 | 95.5 | 88.8 | 95.3 | 96.0 |
| MMR2 | 92.5 | 87.4 | 90.0 | 89.0 | 85.6 | 90.4 | 75.1 | 89.5 | 91.2 |
| Factors | Complacency | Confidence | Convenience |
|---|---|---|---|
| Accessibility | X | ||
| Awareness of disease severity | X | ||
| Affordability and funding | X | ||
| Healthcare professionals | X | ||
| Inequalities and sub-populations | X | ||
| Information on service availability | X | ||
| Trusted information | X | ||
| Mis- and disinformation (autism) | X | ||
| Perceived risk of disease | X | ||
| Personal experience | X | ||
| Population mobility | X | ||
| Vaccine safety and effectiveness | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thompson, S.; Meyer, J.C.; Burnett, R.J.; Campbell, S.M. Mitigating Vaccine Hesitancy and Building Trust to Prevent Future Measles Outbreaks in England. Vaccines 2023, 11, 288. https://doi.org/10.3390/vaccines11020288
Thompson S, Meyer JC, Burnett RJ, Campbell SM. Mitigating Vaccine Hesitancy and Building Trust to Prevent Future Measles Outbreaks in England. Vaccines. 2023; 11(2):288. https://doi.org/10.3390/vaccines11020288
Chicago/Turabian StyleThompson, Sarah, Johanna C. Meyer, Rosemary J. Burnett, and Stephen M. Campbell. 2023. "Mitigating Vaccine Hesitancy and Building Trust to Prevent Future Measles Outbreaks in England" Vaccines 11, no. 2: 288. https://doi.org/10.3390/vaccines11020288
APA StyleThompson, S., Meyer, J. C., Burnett, R. J., & Campbell, S. M. (2023). Mitigating Vaccine Hesitancy and Building Trust to Prevent Future Measles Outbreaks in England. Vaccines, 11(2), 288. https://doi.org/10.3390/vaccines11020288