
Humoral Immunogenicity of mRNA Booster Vaccination after Heterologous CoronaVac-ChAdOx1 nCoV-19 or Homologous ChAdOx1 nCoV-19 Vaccination in Patients with Autoimmune Rheumatic Diseases: A Preliminary Report

 ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
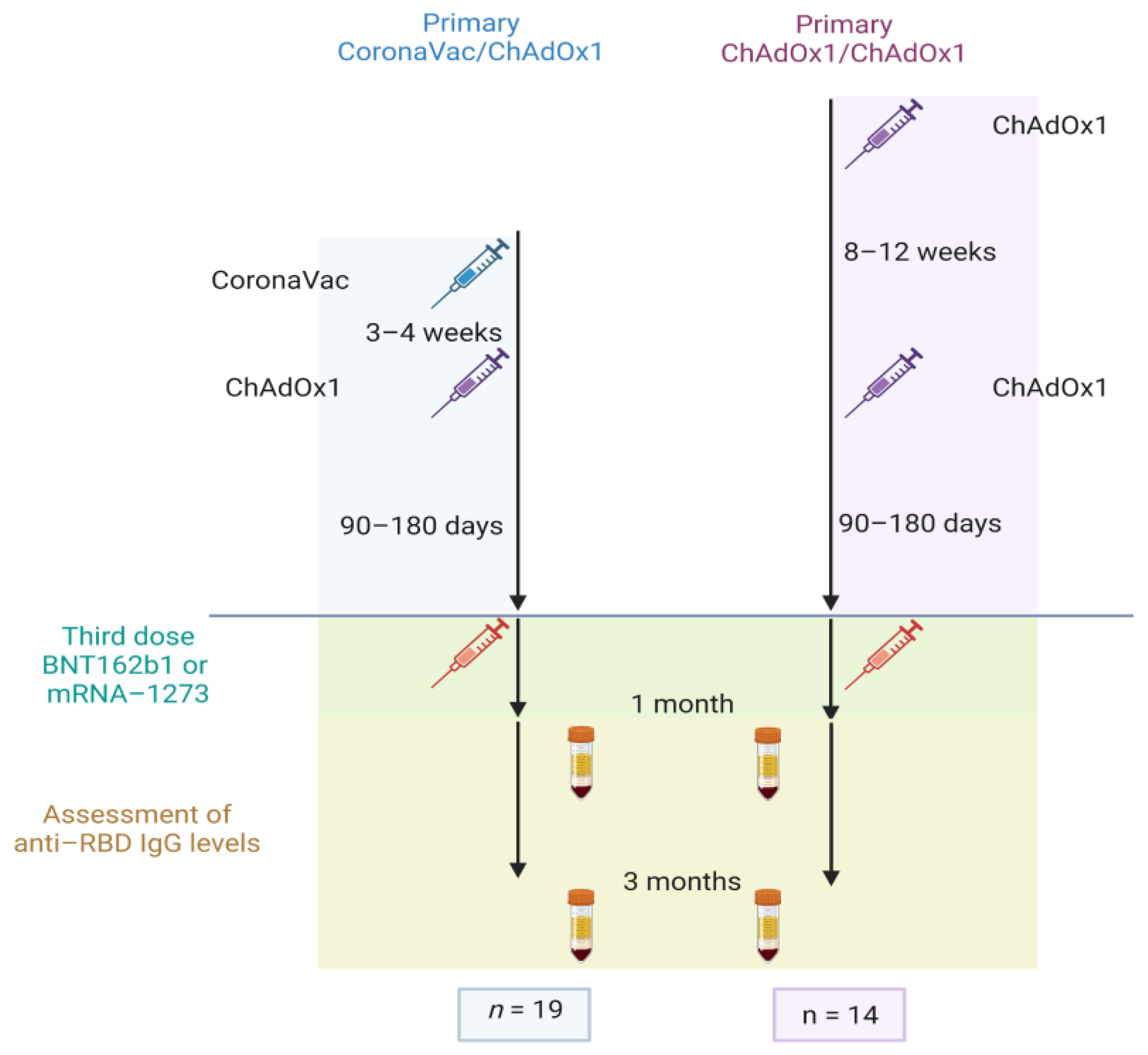
2.1. Study Design and Population
2.2. Vaccination Regimens
2.3. Vaccine Humoral Immunogenicity
2.4. AEFI and Disease Activity after Vaccination
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
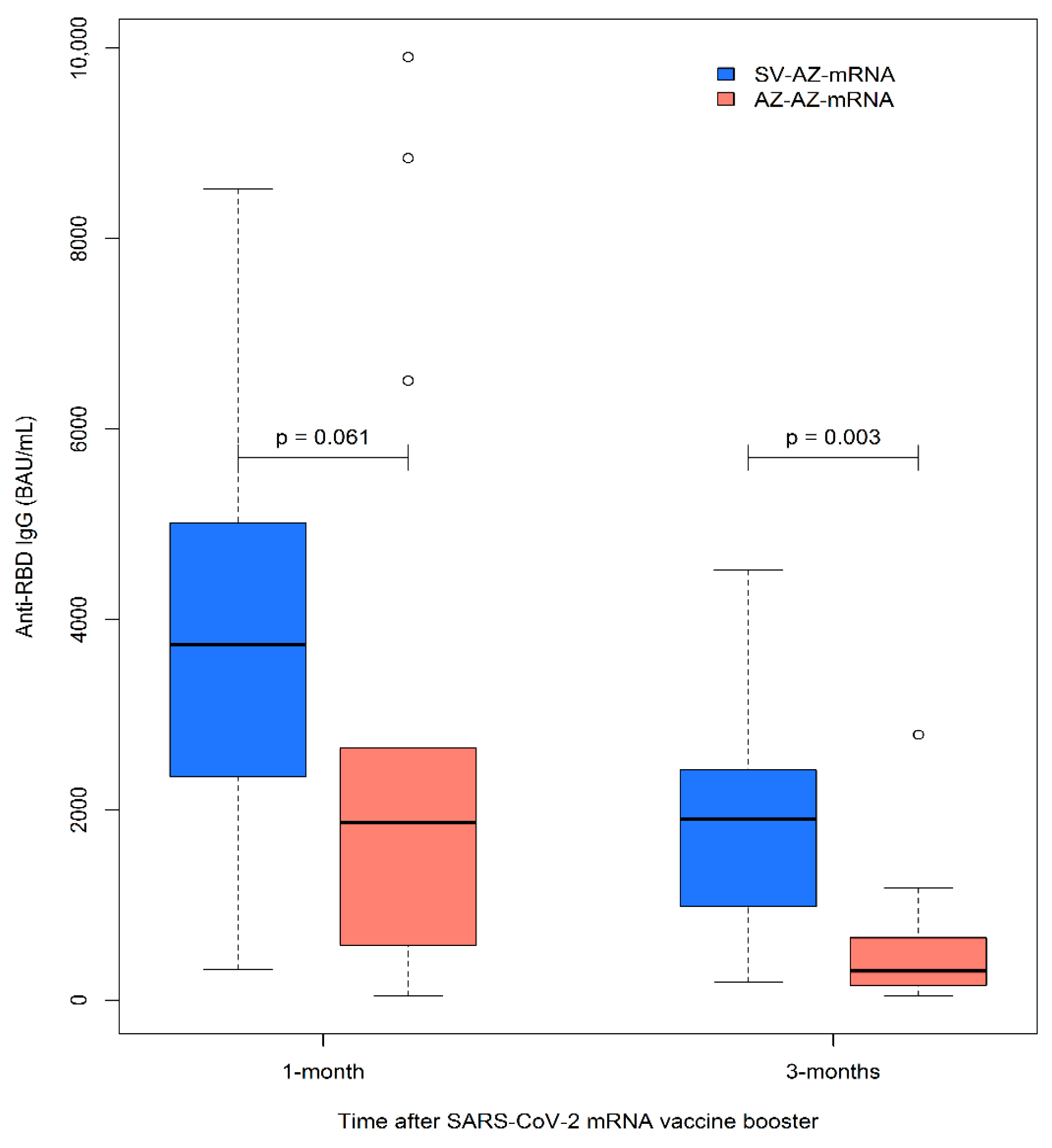
3.2. Humoral Immunogenicity of mRNA Vaccine Booster after CoronaVac/ChAdOx1 or ChAdOx1/ChAdOx1 Vaccination
3.3. Humoral Immunogenicity of the mRNA Vaccine Booster after CoronaVac/ChAdOx1 or ChAdOx1/ChAdOx1 Vaccination in Immunosuppressive Drug Subgroups
3.4. Humoral Immunogenicity of MRNA Vaccine Boosters after CoronaVac/ChAdOx1 or ChAdOx1/ChAdOx1 Vaccine Wanes 3 Months after Vaccination
3.5. Post-Booster Reaction and Disease Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, Y.Z.; Kuan, C.C. Vaccination to reduce severe COVID-19 and mortality in COVID-19 patients: A systematic review and meta-analysis. Eur. Rev. Med. Pharm. Sci. 2022, 26, 1770–1776. [Google Scholar] [CrossRef]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning of vaccine effectiveness against moderate and severe COVID-19 among adults in the US from the VISION network: Test negative, case-control study. BMJ 2022, 379, e072141. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef] [PubMed]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; Demissie, E.G.; El-Qunni, A.A.; Haile, A.; Huang, K.; Kinnett, B.; et al. Effect of Immunosuppression on the Immunogenicity of mRNA Vaccines to SARS-CoV-2: A Prospective Cohort Study. Ann. Intern. Med. 2021, 174, 1572–1585. [Google Scholar] [CrossRef]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330. [Google Scholar] [CrossRef]
- Prendecki, M.; Clarke, C.; Edwards, H.; McIntyre, S.; Mortimer, P.; Gleeson, S.; Martin, P.; Thomson, T.; Randell, P.; Shah, A.; et al. Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression. Ann. Rheum. Dis. 2021, 80, 1322. [Google Scholar] [CrossRef]
- Tang, W.; Gartshteyn, Y.; Ricker, E.; Inzerillo, S.; Murray, S.; Khalili, L.; Askanase, A. The Use of COVID-19 Vaccines in Patients with SLE. Curr. Rheumatol. Rep. 2021, 23, 79. [Google Scholar] [CrossRef]
- Haberman, R.H.; Herati, R.S.; Simon, D.; Samanovic, M.; Blank, R.B.; Tuen, M.; Koralov, S.B.; Atreya, R.; Tascilar, K.; Allen, J.R.; et al. Methotrexate Hampers Immunogenicity to BNT162b2 mRNA COVID-19 Vaccine in Immune-Mediated Inflammatory Disease. medRxiv 2021. [CrossRef]
- Curtis, J.R.; Johnson, S.R.; Anthony, D.D.; Arasaratnam, R.J.; Baden, L.R.; Bass, A.R.; Calabrese, C.; Gravallese, E.M.; Harpaz, R.; Kroger, A.; et al. American College of Rheumatology Guidance for COVID-19 Vaccination in Patients with Rheumatic and Musculoskeletal Diseases: Version 4. Arthritis Rheumatol. 2022, 74, e21–e36. [Google Scholar] [CrossRef]
- Landewé, R.B.M.; Kroon, F.P.B.; Alunno, A.; Najm, A.; Bijlsma, J.W.; Burmester, G.R.; Caporali, R.; Combe, B.; Conway, R.; Curtis, J.R.; et al. EULAR recommendations for the management and vaccination of people with rheumatic and musculoskeletal diseases in the context of SARS-CoV-2: The November 2021 update. Ann. Rheum. Dis. 2022, 81, 1628–1639. [Google Scholar] [CrossRef]
- Gragnani, L.; Visentini, M.; Lorini, S.; La Gualana, F.; Santini, S.A.; Cacciapaglia, F.; Tavoni, A.; Cuomo, G.; Fallahi, P.; Iannone, F.; et al. COVID-19 vaccine immunogenicity in 16 patients with autoimmune systemic diseases. Lack of both humoral and cellular response to booster dose and ongoing disease modifying therapies. J. Transl. Autoimmun. 2022, 5, 100164. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.; Gragnani, L.; Raimondo, V.; Visentini, M.; Giuggioli, D.; Lorini, S.; Foti, R.; Cacciapaglia, F.; Caminiti, M.; Olivo, D.; et al. Absent or suboptimal response to booster dose of COVID-19 vaccine in patients with autoimmune systemic diseases. J. Autoimmun. 2022, 131, 102866. [Google Scholar] [CrossRef] [PubMed]
- Cardelli, C.; Caruso, T.; Tani, C.; Pratesi, F.; Talarico, R.; DI Cianni, F.; Italiano, N.; Laurino, E.; Moretti, M.; Cascarano, G.; et al. AB1152 COVID-19 mRNA vaccine booster in patients with systemic autoimmune diseases. Ann. Rheum. Dis. 2022, 81, 1693. [Google Scholar] [CrossRef]
- Kim, W.-J.; Choi, S.-H.; Park, J.Y.; Song, J.S.; Chung, J.-W.; Choi, S.T. SARS-CoV-2 Omicron escapes mRNA vaccine booster-induced antibody neutralisation in patients with autoimmune rheumatic diseases: An observational cohort study. Ann. Rheum. Dis. 2022, 81, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Assawasaksakul, T.; Sathitratanacheewin, S.; Vichaiwattana, P.; Wanlapakorn, N.; Poovorawan, Y.; Avihingsanon, Y.; Assawasaksakul, N.; Kittanamongkolchai, W. Immunogenicity of the third and fourth BNT162b2 mRNA COVID-19 boosters and factors associated with immune response in patients with SLE and rheumatoid arthritis. Lupus Sci. Med. 2022, 9, e000726. [Google Scholar] [CrossRef] [PubMed]
- Intapiboon, P.; Uae-Areewongsa, P.; Ongarj, J.; Sophonmanee, R.; Seepathomnarong, P.; Seeyankem, B.; Surasombatpattana, S.; Pinpathomrat, N. Impaired neutralizing antibodies and preserved cellular immunogenicity against SARS-CoV-2 in systemic autoimmune rheumatic diseases. NPJ Vaccines 2022, 7, 149. [Google Scholar] [CrossRef]
- Lee, A.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef]
- Kontopoulou, K.; Nakas, C.T.; Belai, C.; Papazisis, G. Antibody titers after a third dose of the SARS-CoV-2 BNT162b2 vaccine in immunocompromised adults in Greece: Is a fourth dose necessary? J. Med. Virol. 2022, 94, 5056–5060. [Google Scholar] [CrossRef]
- Schmiedeberg, K.; Vuilleumier, N.; Pagano, S.; Albrich, W.C.; Ludewig, B.; Kempis, J.V.; Rubbert-Roth, A. Efficacy and tolerability of a third dose of an mRNA anti-SARS-CoV-2 vaccine in patients with rheumatoid arthritis with absent or minimal serological response to two previous doses. Lancet Rheumatol. 2022, 4, e11–e13. [Google Scholar] [CrossRef]
- Karbasi-Afshar, R.; Izadi, M.; Fazel, M.; Khedmat, H. Response of transplant recipients to influenza vaccination based on type of immunosuppression: A meta-analysis. Saudi J. Kidney Dis. Transplant. 2015, 26, 877–883. [Google Scholar] [CrossRef]
- De Santis, M.; Motta, F.; Isailovic, N.; Clementi, M.; Criscuolo, E.; Clementi, N.; Tonutti, A.; Rodolfi, S.; Barone, E.; Colapietro, F.; et al. Dose-Dependent Impairment of the Immune Response to the Moderna-1273 mRNA Vaccine by Mycophenolate Mofetil in Patients with Rheumatic and Autoimmune Liver Diseases. Vaccines 2022, 10, 801. [Google Scholar] [CrossRef] [PubMed]
- Liew, S.-Y.; Tree, T.; Smith, C.H.; Mahil, S.K. The Impact of Immune-Modifying Treatments for Skin Diseases on the Immune Response to COVID-19 Vaccines: A Narrative Review. Curr. Dermatol. Rep. 2022, 11, 263–288. [Google Scholar] [CrossRef] [PubMed]
- Skaria, T.G.; Sreeprakash, A.; Umesh, R.; Joseph, S.; Mohan, M.; Ahmed, S.; Mehta, P.; Oommen, S.E.; Benny, J.; Paulose, A.; et al. Withholding methotrexate after vaccination with ChAdOx1 nCov19 in patients with rheumatoid or psoriatic arthritis in India (MIVAC I and II): Results of two, parallel, assessor-masked, randomised controlled trials. Lancet Rheumatol. 2022, 4, e755–e764. [Google Scholar] [CrossRef] [PubMed]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Liu, Y.; Liu, Y. The Flare of Rheumatic Disease After SARS-CoV-2 Vaccination: A Review. Front. Immunol. 2022, 13, 919979. [Google Scholar] [CrossRef]
- Suntronwong, N.; Assawakosri, S.; Kanokudom, S.; Yorsaeng, R.; Auphimai, C.; Thongmee, T.; Vichaiwattana, P.; Duangchinda, T.; Chantima, W.; Pakchotanon, P.; et al. Strong Correlations between the Binding Antibodies against Wild-Type and Neutralizing Antibodies against Omicron BA.1 and BA.2 Variants of SARS-CoV-2 in Individuals Following Booster (Third-Dose) Vaccination. Diagnostics 2022, 12, 1781. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef]
- Sapkota, B.; Saud, B.; Shrestha, R.; Al-Fahad, D.; Sah, R.; Shrestha, S.; Rodriguez-Morales, A.J. Heterologous prime-boost strategies for COVID-19 vaccines. J. Travel Med. 2022, 29, taab191. [Google Scholar] [CrossRef]
- He, Q.; Mao, Q.; An, C.; Zhang, J.; Gao, F.; Bian, L.; Li, C.; Liang, Z.; Xu, M.; Wang, J. Heterologous prime-boost: Breaking the protective immune response bottleneck of COVID-19 vaccine candidates. Emerg. Microbes. Infect. 2021, 10, 629–637. [Google Scholar] [CrossRef]
- Mahasirimongkol, S.; Khunphon, A.; Kwangsukstid, O.; Sapsutthipas, S.; Wichaidit, M.; Rojanawiwat, A.; Wichuckchinda, N.; Puangtubtim, W.; Pimpapai, W.; Soonthorncharttrawat, S.; et al. The Pilot Study of Immunogenicity and Adverse Events of a COVID-19 Vaccine Regimen: Priming with Inactivated Whole SARS-CoV-2 Vaccine (CoronaVac) and Boosting with the Adenoviral Vector (ChAdOx1 nCoV-19) Vaccine. Vaccines 2022, 10, 536. [Google Scholar] [CrossRef]
- Pillai, S. SARS-CoV-2 vaccination washes away original antigenic sin. Trends Immunol. 2022, 43, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Röltgen, K.; Nielsen, S.C.A.; Silva, O.; Younes, S.F.; Zaslavsky, M.; Costales, C.; Yang, F.; Wirz, O.F.; Solis, D.; Hoh, R.A.; et al. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell 2022, 185, 1025–1040.e1014. [Google Scholar] [CrossRef] [PubMed]
- Rijkers, G.T.; van Overveld, F.J. The “original antigenic sin” and its relevance for SARS-CoV-2 (COVID-19) vaccination. Clin. Immunol. Commun. 2021, 1, 13–16. [Google Scholar] [CrossRef]
- Roncati, L.; Palmieri, B. What about the original antigenic sin of the humans versus SARS-CoV-2? Med. Hypotheses 2020, 142, 109824. [Google Scholar] [CrossRef] [PubMed]
- Fazekas de St, G.; Webster, R.G. Disquisitions of Original Antigenic Sin. I. Evidence in man. J. Exp. Med. 1966, 124, 331–345. [Google Scholar] [CrossRef]
- Shachor-Meyouhas, Y.; Dabaja-Younis, H.; Magid, A.; Leiba, R.; Szwarcwort-Cohen, M.; Almog, R.; Mekel, M.; Weissman, A.; Hyams, G.; Gepstein, V.; et al. Immunogenicity and SARS-CoV-2 Infection following the Fourth BNT162b2 Booster Dose among Health Care Workers. Vaccines 2023, 11, 283. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of COVID-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Total n = 33 (%) | CoronaVac/ ChAdOx1 n = 19 (%) | ChAdOx1/ChAdOx1 n = 14 (%) | p-Value |
|---|---|---|---|---|
| Female sex | 26 (78.8) | 15 (78.9) | 11 (78.6) | 1 |
| Mean age, years (SD) | 42.9 (10.6) | 42.9 (11) | 43 (10.4) | 0.978 |
| Mean duration (SD), day | 117.9 (18.5) | 117.5 (18.2) | 118.4 (19.5) | 0.886 |
| ARDs | 0.167 | |||
| SLE | 18 (54.5) | 8 (42.1) | 10 (71.4) | |
| RA | 5 (15.2) | 3 (15.8) | 2 (14.3) | |
| SpA/PsA | 5 (15.2) | 4 (21.1) | 1 (7.1) | |
| IIM | 4 (12.1) | 4 (21.1) | 0 (0) | |
| IgG4-Related Disease | 1 (3) | 0 (0) | 1 (7.1) | |
| GC use | 25 (75.8) | 13 (68.4) | 12 (85.7) | 0.416 |
| GC dose, mg (IQR) | 7.5 (5, 7.5) | 7.5 (5, 7.5) | 6.2 (5, 8.1) | 0.885 |
| Immunosuppressants | ||||
| Azathioprine | 15 (45.5) | 8 (42.1) | 7 (50) | 0.923 |
| Methotrexate | 13 (39.4) | 9 (47.4) | 4 (28.6) | 0.464 |
| Mycophenolate mofetil | 7 (21.2) | 4 (21.1) | 3 (21.4) | 1 |
| Leflunomide | 3 (9.1) | 3 (21.4) | 0 (0) | 0.244 |
| Multiple DMARDs | 5 (15.2) | 5 (26.3) | 0 (0) | 0.057 |
| Immunogenicity | Total n = 33 (%) | CoronaVac/ ChAdOx1 n = 19 (%) | ChAdOx1/ ChAdOx1 n = 14 (%) | p-Value |
|---|---|---|---|---|
| Mean (SD) time to booster; day | 117.9 (18.5) | 117.5 (18.2) | 118.4 (19.5) | 0.886 |
| Seropositivity rate | 32 (97.0) | 19 (100.0) | 13 (92.9) | 0.424 |
| 1-month median (IQR) anti-RBD IgG (BAU/mL) | 2729 (1190.4, 4864) | 3735.8 (2347.9, 5014.0) | 1867.8 (591.6, 2548.6) | 0.061 |
| 3-month mean (SD) anti-RBD IgG (BAU/mL) (n = 28) | 1122.6 (926.5) | 1609.9 (828.4) | 597.8 (735.5) | 0.003 * |
| Median (IQR) anti-RBD IgG ratio 1 | 3 (1.9, 3.7) | 2.5 (1.8, 3.3) | 3.6 (2.9, 4.7) | 0.032 * |
| Immunosuppressive Drugs | 1-Month Anti-RBD IgG (BAU/mL) | p-Value | 3-Month Anti-RBD IgG (BAU/mL) | p-Value |
|---|---|---|---|---|
| Glucocorticoids | 0.389 | 0.297 | ||
| yes (n = 25) | 2648.7 (774, 4864) | 732.2 (186.8, 1353.6) | ||
| no (n = 8) | 3417.7 (2066.3, 5204.9) | 1558 (387.8, 2015.2) | ||
| Mycophenolate mofetil | 0.561 | 1 | ||
| yes (n = 7) | 2895.8 (2449.7) | 675.4 (233.4, 2335.3) | ||
| no (n = 26) | 3590.2 (2847.2) | 859.3 (291.6, 1868) | ||
| Methotrexate | 0.126 | 0.162 | ||
| yes (n = 13) | 4355.5 (2835.6) | 1404 (906.6) | ||
| no (n = 20) | 2849.8 (2585.1) | 897.5 (908.9) | ||
| Azathioprine | 0.556 | 0.228 | ||
| yes (n = 15) | 3128.1 (2776.1) | 878.7 (771.1) | ||
| no (n = 13) | 3705.3 (2772.9) | 1317.7 (1017.4) | ||
| Comparing immunosuppressiveness | ||||
| Mycophenolate mofetil vs. Methotrexate | 2895.8 (2449.7) vs. 4355.5 (2835.6) | 0.266 | 1197.5 (1283.6) vs. 1404 (906.6) | 0.696 |
| Mycophenolate mofetil vs. Azathioprine | 2963.8 (2790.5) vs. 3128.1 (2776.1) | 0.899 | 281.1 (186.4, 1811.3) vs. 732.2 (193.4, 1216.6) | 0.815 |
| Methotrexate vs. Azathioprine | 4220.4 (2952.9) vs. 2825 (2753) | 0.244 | 1262.3 (928.8) vs. 631.9 (559.1) | 0.083 |
| Adverse Events | Total n = 33 (%) | CoronaVac/ChAdOx1 n = 19 (%) | ChAdOx1/ChAdOx1 n = 14 (%) | p-Value |
|---|---|---|---|---|
| AEFI | 24 (72.7) | 14 (73.7) | 10 (71.4) | 1 |
| Systemic reactions | 8 (24.2) | 4 (21.1) | 4 (28.6) | 0.695 |
| Fever | 7 (21.2) | 4 (21.1) | 3 (21.4) | 1 |
| Chill | 3 (9.1) | 1 (5.3) | 2 (14.3) | 0.561 |
| Fatigue | 4 (12.1) | 1 (5.3) | 3 (21.4) | 0.288 |
| Myalgia | 5 (15.2) | 2 (10.5) | 3 (21.4) | 0.628 |
| Headache | 3 (9.1) | 1 (5.3) | 2 (14.3) | 0.561 |
| Local reactions | 23 (69.7) | 14 (77.7) | 9 (64.2) | 1 |
| Pain | 22 (66.7) | 13 (68.4) | 9 (64.3) | 1 |
| Swelling | 3 (9.1) | 3 (15.8) | 0 (0) | 0.244 |
| Disease flares | 6 (18.2) | 4 (21.1) | 2 (14.3) | 1 |
| COVID-19 infection | 5 (26.3) | 5 (26.3) | 0 (0) | 0.057 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Intapiboon, P.; Pinpathomrat, N.; Juthong, S.; Uea-Areewongsa, P.; Ongarj, J.; Siripaitoon, B. Humoral Immunogenicity of mRNA Booster Vaccination after Heterologous CoronaVac-ChAdOx1 nCoV-19 or Homologous ChAdOx1 nCoV-19 Vaccination in Patients with Autoimmune Rheumatic Diseases: A Preliminary Report. Vaccines 2023, 11, 537. https://doi.org/10.3390/vaccines11030537
Intapiboon P, Pinpathomrat N, Juthong S, Uea-Areewongsa P, Ongarj J, Siripaitoon B. Humoral Immunogenicity of mRNA Booster Vaccination after Heterologous CoronaVac-ChAdOx1 nCoV-19 or Homologous ChAdOx1 nCoV-19 Vaccination in Patients with Autoimmune Rheumatic Diseases: A Preliminary Report. Vaccines. 2023; 11(3):537. https://doi.org/10.3390/vaccines11030537
Chicago/Turabian StyleIntapiboon, Porntip, Nawamin Pinpathomrat, Siriporn Juthong, Parichat Uea-Areewongsa, Jomkwan Ongarj, and Boonjing Siripaitoon. 2023. "Humoral Immunogenicity of mRNA Booster Vaccination after Heterologous CoronaVac-ChAdOx1 nCoV-19 or Homologous ChAdOx1 nCoV-19 Vaccination in Patients with Autoimmune Rheumatic Diseases: A Preliminary Report" Vaccines 11, no. 3: 537. https://doi.org/10.3390/vaccines11030537
APA StyleIntapiboon, P., Pinpathomrat, N., Juthong, S., Uea-Areewongsa, P., Ongarj, J., & Siripaitoon, B. (2023). Humoral Immunogenicity of mRNA Booster Vaccination after Heterologous CoronaVac-ChAdOx1 nCoV-19 or Homologous ChAdOx1 nCoV-19 Vaccination in Patients with Autoimmune Rheumatic Diseases: A Preliminary Report. Vaccines, 11(3), 537. https://doi.org/10.3390/vaccines11030537