
Acceptance of the Human Papillomavirus Vaccine among General Men and Men with a Same-Sex Orientation and Its Influencing Factors: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of Study Population and HPV Vaccine Acceptance Rate
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Literature Screening, Data Extraction, and Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Search Results
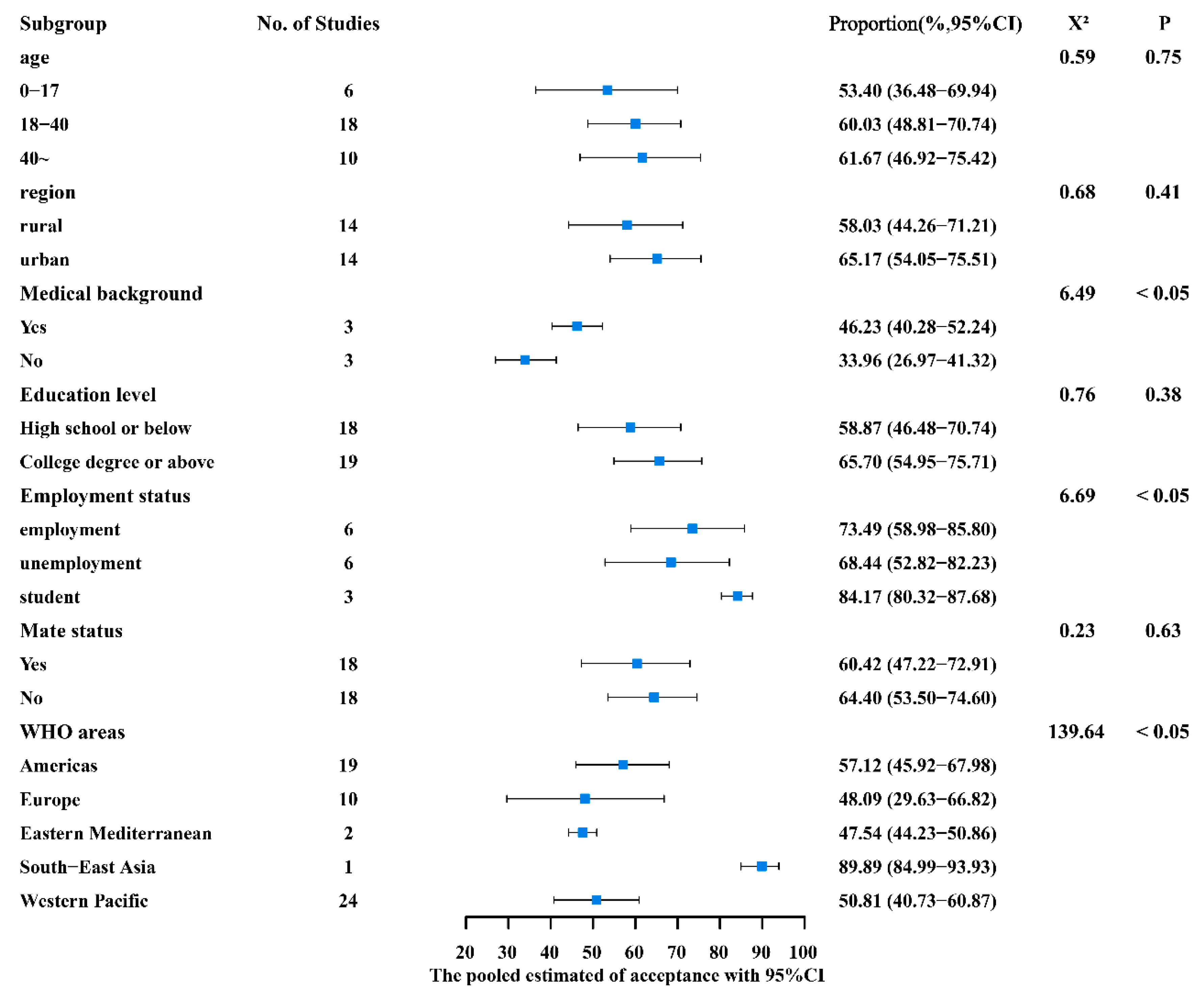
3.2. HPV Vaccine Acceptance and Results of Subgroup Analysis
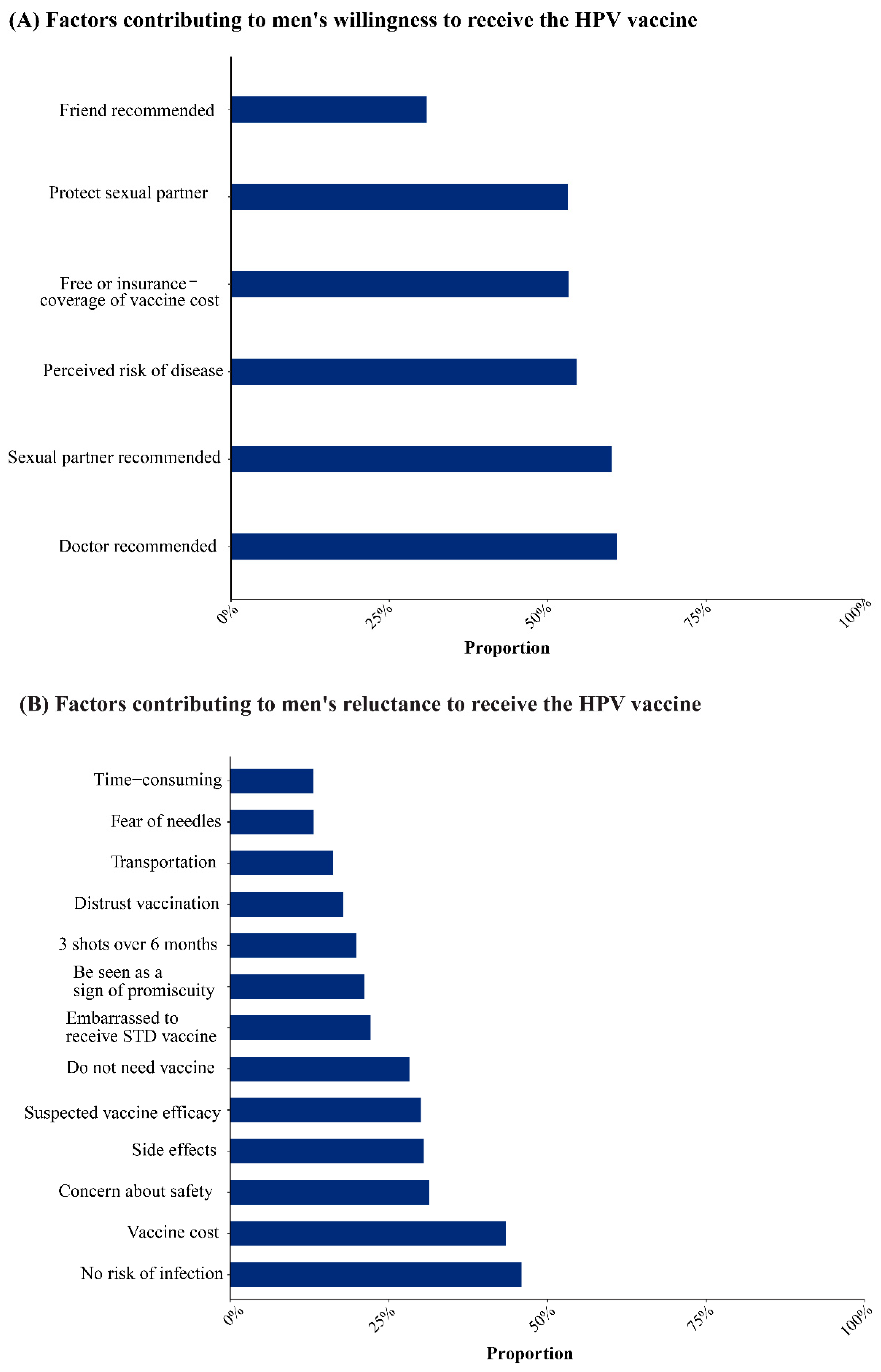
3.3. Analysis of Factors Influencing HPV Vaccination Intention
3.4. Publication Bias and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| WHO | World Health Organization |
| HPV | human papillomavirus |
| MSM | men having sex with men |
| MNSM | men not having sex with men |
| 95% CI | 95% confidence interval |
| STDs | sexually transmitted diseases |
References
- Schiffman, M.; Doorbar, J.; Wentzensen, N.; de Sanjosé, S.; Fakhry, C.; Monk, B.J.; Stanley, M.A.; Franceschi, S. Carcinogenic human papillomavirus infection. Nat. Rev. Dis. Primers 2016, 2, 16086. [Google Scholar] [CrossRef] [PubMed]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Han, B.; Wan, Y.; Liu, J.; Zhao, T.; Liu, H.; Cui, F. Do Male University Students Know Enough About Human Papillomavirus (HPV) to Make Informed Decisions About Vaccination? Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924840. [Google Scholar] [CrossRef] [PubMed]
- Dibble, K.E.; Maksut, J.L.; Siembida, E.J.; Hutchison, M.; Bellizzi, K.M. A Systematic Literature Review of HPV Vaccination Barriers Among Adolescent and Young Adult Males. J. Adolesc. Young Adult Oncol. 2019, 8, 495–511. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, L.E.; Schiller, J.T. Human Papillomavirus Vaccines. J. Infect. Dis. 2021, 224, S367–S378. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Zhao, C.; Zhang, G. Awareness of HPV and willingness to HPV vaccination among male university students in Tongzhou District. J. Prev. Med. 2022, 6, 571–576. (In Chinese) [Google Scholar]
- Osmani, V.; Klug, S.J. [HPV vaccination and the prevention of genital warts and precancerous lesions-current evidence and evaluation]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 590–599. [Google Scholar] [CrossRef]
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef]
- Barr, E.; Tamms, G. Quadrivalent human papillomavirus vaccine. Clin. Infect. Dis. 2007, 45, 609–617. [Google Scholar] [CrossRef]
- Liddon, N.; Hood, J.; Wynn, B.A.; Markowitz, L.E. Acceptability of human papillomavirus vaccine for males: A review of the literature. J. Adolesc. Health 2010, 46, 113–123. [Google Scholar] [CrossRef]
- Nadarzynski, T.; Smith, H.; Richardson, D.; Jones, C.J.; Llewellyn, C.D. Human papillomavirus and vaccine-related perceptions among men who have sex with men: A systematic review. Sex. Transm. Infect. 2014, 90, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Newman, P.A.; Logie, C.H.; Doukas, N.; Asakura, K. HPV vaccine acceptability among men: A systematic review and meta-analysis. Sex. Transm. Infect. 2013, 89, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Chen, Y.-P.; Liang, H.; Wang, Y. Acceptability of human papillomavirus vaccine among men: A Meta analysis. J. Prev. Med. 2018, 30, 897–901. (In Chinese) [Google Scholar]
- Agüero, F.; Masuet-Aumatell, C.; Morchon, S.; Ramon-Torrell, J.M. Men who have sex with men: A group of travellers with special needs. Travel Med. Infect. Dis. 2019, 28, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Meyers, D. Introduction from the Agency for Healthcare Research and Quality. J. Am. Board Fam. Med. 2012, 25 (Suppl. S1), S1. [Google Scholar] [CrossRef] [PubMed]
- Hn, Z.; Ww, Y.; Hp, Y.; Cx, L.; Ry, J.; Hw, N. The prevalence of hyperuricemia in China: A meta-analysis. BMC Public Health 2011, 11, 832. [Google Scholar] [CrossRef]
- Ioannidis, J.P.; Patsopoulos, N.A.; Evangelou, E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ 2007, 335, 914–916. [Google Scholar] [CrossRef]
- Ferris, D.G.; Waller, J.L.; Miller, J.; Patel, P.; Jackson, L.; Price, G.A.; Wilson, C. Men’s attitudes toward receiving the human papillomavirus vaccine. J. Low Genit. Tract. Dis. 2008, 12, 276–281. [Google Scholar] [CrossRef]
- Ferris, D.G.; Waller, J.L.; Miller, J.; Patel, P.; Price, G.A.; Jackson, L.; Wilson, C. Variables associated with human papillomavirus (HPV) vaccine acceptance by men. J. Am. Board Fam. Med. 2009, 22, 34–42. [Google Scholar] [CrossRef]
- Gottvall, M.; Larsson, M.; Höglund, A.T.; Tydén, T. High HPV vaccine acceptance despite low awareness among Swedish upper secondary school students. Eur. J. Contracept. Reprod. Health Care 2009, 14, 399–405. [Google Scholar] [CrossRef]
- Daley, E.M.; Marhefka, S.L.; Buhi, E.R.; Vamos, C.A.; Hernandez, N.D.; Giuliano, A.R. Human papillomavirus vaccine intentions among men participating in a human papillomavirus natural history study versus a comparison sample. Sex. Transm. Dis. 2010, 37, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, B.Y.; Wilkens, L.R.; Thompson, P.J.; Shvetsov, Y.B.; Goodman, M.T.; Ning, L.; Kaopua, L. Acceptability of prophylactic human papillomavirus vaccination among adult men. Hum. Vaccines 2010, 6, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Brewer, N.T.; McRee, A.L.; Gilbert, P.; Smith, J.S. Acceptability of HPV vaccine among a national sample of gay and bisexual men. Sex. Transm. Dis. 2010, 37, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Brewer, N.T.; Smith, J.S. Human papillomavirus knowledge and vaccine acceptability among a national sample of heterosexual men. Sex. Transm. Infect. 2010, 86, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.K.; Lim, M.K.; Yun, E.H.; Lee, E.H.; Shin, H.R. Awareness of and attitude towards human papillomavirus infection and vaccination for cervical cancer prevention among adult males and females in Korea: A nationwide interview survey. Vaccine 2010, 28, 1854–1860. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.A.; Brewer, N.T.; Reiter, P.L. Association of human papillomavirus-related knowledge, attitudes, and beliefs with HIV status: A national study of gay men. J. Low. Genit. Tract Dis. 2011, 15, 83–88. [Google Scholar] [CrossRef]
- Gilbert, P.; Brewer, N.T.; Reiter, P.L.; Ng, T.W.; Smith, J.S. HPV vaccine acceptability in heterosexual, gay, and bisexual men. Am. J. Men’s Health 2011, 5, 297–305. [Google Scholar] [CrossRef]
- Katz, M.L.; Krieger, J.L.; Roberto, A.J. Human papillomavirus (HPV): College male’s knowledge, perceived risk, sources of information, vaccine barriers and communication. J. Men’s Health 2011, 8, 175–184. [Google Scholar] [CrossRef]
- Wheldon, C.W.; Daley, E.M.; Buhi, E.R.; Nyitray, A.G.; Giuliano, A.R. Health beliefs and attitudes associated with HPV vaccine intention among young gay and bisexual men in the Southeastern United States. Vaccine 2011, 29, 8060–8065. [Google Scholar] [CrossRef]
- Thomas, E.A.; Goldstone, S.E. Should I or shouldn’t I: Decision making, knowledge and behavioral effects of quadrivalent HPV vaccination in men who have sex with men. Vaccine 2011, 29, 570–576. [Google Scholar] [CrossRef]
- Crosby, R.A.; DiClemente, R.J.; Salazar, L.F.; Nash, R.; Younge, S. Gardasil for guys: Correlates of intent to be vaccinated. J. Men’s Health 2011, 8, 119–125. [Google Scholar] [CrossRef]
- Colón-López, V.; Del Toro-Mejías, L.M.; Ortiz, A.P.; Tortolero-Luna, G.; Palefsky, J.M. HPV awareness and willingness to HPV vaccination among high-risk men attending an STI clinic in Puerto Rico. Puerto Rico Health Sci. J. 2012, 31, 227–231. [Google Scholar]
- Forster, A.S.; Marlow, L.A.; Wardle, J.; Stephenson, J.; Waller, J. Interest in having HPV vaccination among adolescent boys in England. Vaccine 2012, 30, 4505–4510. [Google Scholar] [CrossRef] [PubMed]
- Rank, C.; Gilbert, M.; Ogilvie, G.; Jayaraman, G.C.; Marchand, R.; Trussler, T.; Hogg, R.S.; Gustafson, R.; Wong, T. Acceptability of human papillomavirus vaccination and sexual experience prior to disclosure to health care providers among men who have sex with men in Vancouver, Canada: Implications for targeted vaccination programs. Vaccine 2012, 30, 5755–5760. [Google Scholar] [CrossRef] [PubMed]
- Bourke, L. Acceptance and Associated Factors of HPV Vaccination among Young Male Malaysians. J. Community Med. Health Educ. 2012, 1, 120. [Google Scholar] [CrossRef]
- Blödt, S.; Holmberg, C.; Müller-Nordhorn, J.; Rieckmann, N. Human Papillomavirus awareness, knowledge and vaccine acceptance: A survey among 18–25 year old male and female vocational school students in Berlin, Germany. Eur. J. Public Health 2012, 22, 808–813. [Google Scholar] [CrossRef]
- Ortashi, O.; Raheel, H.; Khamis, J. Acceptability of human papillomavirus vaccination among male university students in the United Arab Emirates. Vaccine 2013, 31, 5141–5144. [Google Scholar] [CrossRef]
- Lau, J.T.; Wang, Z.; Kim, J.H.; Lau, M.; Lai, C.H.; Mo, P.K. Acceptability of HPV vaccines and associations with perceptions related to HPV and HPV vaccines among men who have sex with men in Hong Kong. PLoS ONE 2013, 8, e57204. [Google Scholar] [CrossRef]
- Belani, H.K.; Sekar, P.; Guhaniyogi, R.; Abraham, A.; Bohjanen, P.R.; Bohjanen, K. Human papillomavirus vaccine acceptance among young men in Bangalore, India. Int. J. Dermatol. 2014, 53, e486–e491. [Google Scholar] [CrossRef]
- Gellenoncourt, A.; Patrizio, P.D. [Evaluation of the acceptability of the human papillomavirus vaccine among male high school students in Lorraine]. Sante Publique 2014, 26, 753–761. [Google Scholar] [CrossRef]
- Zou, H.; Grulich, A.E.; Cornall, A.M.; Tabrizi, S.N.; Garland, S.M.; Prestage, G.; Bradshaw, C.S.; Hocking, J.S.; Morrow, A.; Fairley, C.K.; et al. How very young men who have sex with men view vaccination against human papillomavirus. Vaccine 2014, 32, 3936–3941. [Google Scholar] [CrossRef]
- Khurana, S.; Sipsma, H.L.; Caskey, R.N. HPV vaccine acceptance among adolescent males and their parents in two suburban pediatric practices. Vaccine 2015, 33, 1620–1624. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, M.; Vescio, M.F.; Donà, M.G.; Latini, A.; Frasca, M.; Colafigli, M.; Farinella, M.; Rezza, G.; Cristaudo, A. Perceptions of Human Papillomavirus (HPV) infection and acceptability of HPV vaccine among men attending a sexual health clinic differ according to sexual orientation. Hum. Vaccines Immunother. 2016, 12, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Hunter, T.; Weinstein, M. Beliefs and knowledge about the human papillomavirus vaccine among undergraduate men. Health Educ. J. 2016, 75, 249–256. [Google Scholar] [CrossRef]
- Napolitano, F.; Napolitano, P.; Liguori, G.; Angelillo, I.F. Human papillomavirus infection and vaccination: Knowledge and attitudes among young males in Italy. Hum. Vaccines Immunother. 2016, 12, 1504–1510. [Google Scholar] [CrossRef]
- Zou, H.; Meng, X.; Jia, T.; Zhu, C.; Chen, X.; Li, X.; Xu, J.; Ma, W.; Zhang, X. Awareness and acceptance of human papillomavirus (HPV) vaccination among males attending a major sexual health clinic in Wuxi, China: A cross-sectional study. Hum. Vaccines Immunother. 2016, 12, 1551–1559. [Google Scholar] [CrossRef]
- Zhu, J.; Zhou, X.; Xi, S.; Huang, W.J.C.P.M. The cognitive study on human papillomavirus and human papillomavirus vaccine among MSM in Xiacheng district of Hangzhou. Chin. Prev. Med. 2016, 17, 212–216. (In Chinese) [Google Scholar]
- Sadlier, C.; Lynam, A.; O’Dea, S.; Delamere, S.; Quinlan, M.; Clarke, S.; Sheils, O.; Bergin, C. HPV vaccine acceptability in HIV-infected and HIV negative men who have sex with men (MSM) in Ireland. Hum. Vaccines Immunother. 2016, 12, 1536–1541. [Google Scholar] [CrossRef]
- Stephens, D.P.; Thomas, T.L.; Eaton, A. Identifying Health Beliefs Influencing Hispanic College Men’s Willingness to Vaccinate against HPV. Am. J. Sex. Educ. 2016, 11, 267–286. [Google Scholar] [CrossRef]
- Tian, T. Investigation of Human Papillomavirus Related Knowledge and Infection among MSM. Available online: https://kns.cnki.net/kcms2/article/abstract?v=PN9vNVFTqffG8kbbbm2NDtUfpiqYDbbmzxkSs701wszuaA__1ebNWNRFx-t6IAcriaWGfftAm_Bfyo6Yo0ukOB5uwrEbw_-rOvwTrqsoluSJWlJOzai7UWO-4V8NFAhPQmY3GAGGc_KFqJ1nFN13vA==&uniplatform=NZKPT&language=CHS (accessed on 16 December 2017). (In Chinese).
- Hoefer, L.; Tsikis, S.; Bethimoutis, G.; Nicolaidou, E.; Paparizos, V.; Antoniou, C.; Kanelleas, A.; Chardalias, L.; Stavropoulos, G.E.; Schneider, J.; et al. HPV vaccine acceptability in high-risk Greek men. Hum. Vaccines Immunother. 2018, 14, 134–139. [Google Scholar] [CrossRef]
- Cheung, T.; Lau, J.T.F.; Wang, J.Z.; Mo, P.K.H.; Ho, Y.S. Acceptability of HPV vaccines and associations with perceptions related to HPV and HPV vaccines among male baccalaureate students in Hong Kong. PLoS ONE 2018, 13, e0198615. [Google Scholar] [CrossRef] [PubMed]
- Stanley, C.; Secter, M.; Chauvin, S.; Selk, A. HPV vaccination in male physicians: A survey of gynecologists and otolaryngology surgeons’ attitudes towards vaccination in themselves and their patients. Papillomavirus Res. 2018, 5, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.L.; Zellner-Lawrence, T.; Mubasher, M.; Banerjee, A.; Hernandez, N.D. Examining HPV Awareness, Sexual Behavior, and Intent to Receive the HPV Vaccine Among Racial/Ethnic Male College Students 18–27 years. Am. J. Men’s Health 2018, 12, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Nadarzynski, T.; Smith, H.; Richardson, D.; Bremner, S.; Llewellyn, C. Men who have sex with men who do not access sexual health clinics nor disclose sexual orientation are unlikely to receive the HPV vaccine in the UK. Vaccine 2018, 36, 5065–5070. [Google Scholar] [CrossRef] [PubMed]
- Tian, T.; Wang, D.; Papamichael, C.; Yan, Z.; Guoyao, S.; Zhanlin, Z.; Mahan, Y.; Xiaoqing, T.; Zheng, G.; Jianghong, D. HPV vaccination acceptability among men who have sex with men in Urumqi, China. Hum. Vaccines Immunother. 2019, 15, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Yusoff, R.; Sam, I.C.; Zimet, G.D. Are Boys Ready for Human Papillomavirus Vaccine? A National Study of Boys in Malaysia. Sex. Transm. Dis. 2019, 46, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Jia, T.; Zhang, X.; Zhu, C.; Chen, X.; Zou, H. Analysis of willingness to receive human papillomavirus vaccine and related factors among men who have sex with men and male attendees at STD clinics. Diet. Health 2019, 6, 288–289. (In Chinese) [Google Scholar]
- Li, Y.; Ma, H.; Li, R.; Lin, H.; Xiao, W.; Huang, M.; Huang, S.; Wu, T.; Shu, Y. Awareness and willingness to receive the HPV vaccine and the related factors among male university students in Xiamen, China. Chin. J. Sch. Health 2019, 40, 1880–1883. (In Chinese) [Google Scholar]
- Ren, W.J.; Gao, J.; Hu, Q.Q. Influencing Factors Of The Willingness Of Male Nurses to HPV vaccination. Chin. J. Viral Dis. 2020, 10, 204–208. (In Chinese) [Google Scholar]
- Farsi, N.J.; Baharoon, A.H.; Jiffri, A.E.; Marzouki, H.Z.; Merdad, M.A.; Merdad, L.A. Human papillomavirus knowledge and vaccine acceptability among male medical students in Saudi Arabia. Hum. Vaccines Immunother. 2021, 17, 1968–1974. [Google Scholar] [CrossRef]
- Miaomiao, B. Study on Cognition Status of Human Papillomavirus and Vaccination Willingness of Male College Students Based on Health Belief Mode. Available online: https://kns.cnki.net/kcms2/article/abstract?v=PN9vNVFTqffcthkjLdWbpTXwsCjSKkKLJD1KcFMzc45YQxjwOvsQpV_I_K1qHSAekjlaijVElzcJpu6E0XZFjIzTc74PPr-549-jrZtwbaA-Hf1dnOpxGRzJTQSeRYLw9VZHFkdzbTwePqRi65oDlQ==&uniplatform=NZKPT&language=CHS (accessed on 16 August 2021). (In Chinese).
- He, W.; Pan, H.; Lin, B.; Zhong, X. Analysis of HPV Vaccination Willingness amongst HIV-Negative Men Who Have Sex with Men in China. Vaccines 2021, 9, 1069. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.H.; Liu, Z.Z.; Cui, S.T.; Chu, Z.X.; Jiang, Y.J.; Xu, J.J.; Hu, Q.H.; Shang, H. High Human Papillomavirus Vaccine Acceptability and Cost-Effectiveness of the Chinese 2-Valent Vaccine Among Men Who Have Sex With Men: A Cross-Sectional Study in Shenyang, China. Front. Med. 2021, 8, 763564. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zhou, T.; Zhong, X. Factors Related to HPV Vaccination Intention among MSM in China: A Bayesian Network Model. Int. J. Environ. Res. Public Health 2022, 19, 15532. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; He, W.; Lin, B.; Zhong, X. Factors influencing HPV vaccination willingness among men who have sex with men in China: A structural equation modeling analysis. Hum. Vaccines Immunother. 2022, 18, 2038504. [Google Scholar] [CrossRef] [PubMed]
- Pham, D.; Shukla, A.; Welch, K.; Villa, A. Assessing knowledge of human papillomavirus among men who have sex with men (MSM) using targeted dating applications. Vaccine 2022, 40, 5376–5383. [Google Scholar] [CrossRef] [PubMed]
- Ran, H.; Chen, Y.; Gao, J.; Guo, H.; Peng, S. Low awareness of HPV infection and willingness of HPV vaccination among Chinese male college students in the east of China. Front. Public Health 2022, 10, 971707. [Google Scholar] [CrossRef]
- Zhang, H.; Tang, M.-y.; Tian, X.-f. Investigation of HPV vaccine awareness and vaccination willingness among male students in private college based on model of TAM-TPB. Occup. Health 2022, 38, 2260–2265. (In Chinese) [Google Scholar]
- Zhang, J.; Lin, H.; Shen, W.; Gao, M.; Ding, Y.; He, N.; Chen, X.; Liu, X. The willingness of HPV vaccination and related factors among HIV-positive males in Taizhou city. Chin. J. AIDS STD 2022, 28, 1064–1069. (In Chinese) [Google Scholar]
- Gürsoy, M.Y.; Sağtaş, F. Human Papillomavirus Vaccination in Male University Students in Turkey: Coverage Rate, Barriers, and Associated Factors. J. Prev. 2023, 44, 181–191. [Google Scholar] [CrossRef]
- Lv, H.; Liu, L.; Lu, H. Knowledge levels and vaccination willingness of HPV among HIV-infected men. Chin. J. AIDS STD 2023, 29, 596–600. (In Chinese) [Google Scholar]
- Woestenberg, P.J.; van Benthem, B.H.B.; Bogaards, J.A.; King, A.J.; van der Klis, F.R.M.; Pasmans, H.; Leussink, S.; van der Sande, M.A.B.; Hoebe, C. HPV infections among young MSM visiting sexual health centers in the Netherlands: Opportunities for targeted HPV vaccination. Vaccine 2020, 38, 3321–3329. [Google Scholar] [CrossRef] [PubMed]
- Fairley, C.K.; Zou, H.; Zhang, L.; Chow, E.P.F. Human papillomavirus vaccination in men who have sex with men—What will be required by 2020 for the same dramatic changes seen in heterosexuals. Sex Health 2017, 14, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Dursun, P.; Altuntas, B.; Kuscu, E.; Ayhan, A. Women’s knowledge about human papillomavirus and their acceptance of HPV vaccine. Aust. N. Z. J. Obstet. Gynaecol. 2009, 49, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Gerend, M.A.; Shepherd, M.A.; Lustria, M.L.; Shepherd, J.E. Predictors of provider recommendation for HPV vaccine among young adult men and women: Findings from a cross-sectional survey. Sex. Transm. Infect. 2016, 92, 104–107. [Google Scholar] [CrossRef]
- Daley, E.M.; Vamos, C.A.; Thompson, E.L.; Zimet, G.D.; Rosberger, Z.; Merrell, L.; Kline, N.S. The feminization of HPV: How science, politics, economics and gender norms shaped U.S. HPV vaccine implementation. Papillomavirus Res. 2017, 3, 142–148. [Google Scholar] [CrossRef]
- Rani, U.; Darabaner, E.; Seserman, M.; Bednarczyk, R.A.; Shaw, J. Public Education Interventions and Uptake of Human Papillomavirus Vaccine: A Systematic Review. J. Public Health Manag. Pract. 2022, 28, E307–E315. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Age | Survey Time | Country | Sample Size | Sexual Orientation/Behavior | Research Methods | Acceptance Rate (%) | Quality Assessment * |
|---|---|---|---|---|---|---|---|---|---|
| Ferris, D., et al. † [18,19] | 2008 | 18–45 | — | the U. S | 571 | heterosexual/ homosexual/bisexual | cross-sectional study | 32.92 | High |
| Gottvall, M., et al. [20] | 2009 | 15–16 | 2008 Autumn | Sweden | 261 | — | cross-sectional study | 74.33 | High |
| Daley, E., et al. [21] | 2010 | 18–70 | March 2007 | the U. S | 494 | — | cross-sectional study | 80.57 | High |
| Hernandez, B. Y., et al. [22] | 2010 | 18–79 | 2004–2007 | the U. S | 445 | MSM/heterosexual | cross-sectional study | 69.21 | Moderate |
| Reiter, P., et al. [23] | 2010 | 18–59 | January 2009 | the U. S | 306 | homosexual/bisexual | cross-sectional study | 73.53 | High |
| Reiter, P. L., et al. [24] | 2010 | 18–59 | January 2009 | the U. S | 297 | heterosexual | cross-sectional study | 36.70 | High |
| Oh, J. K., et al. [25] | 2010 | ≥20 | November 2007 | Korea | 496 | — | cross-sectional study | 55.44 | High |
| Gilbert, P., et al. [26] | 2011 | — | January 2009 | the U. S | 247 | homosexual | cross-sectional study | 74.90 | High |
| Gilbert, P., et al. [27] | 2011 | 18–59 | January 2009 | the U. S | 608 | heterosexual/bisexual/homosexual | cross-sectional study | 55.59 | High |
| Katz, M. L., et al. [28] | 2011 | 16–26 | 2009 | the U. S | 165 | — | cross-sectional study | 79.39 | Moderate |
| Wheldon, C. W., et al. [29] | 2011 | 18–29 | September 2010–December 2010 | the U. S | 179 | homosexual/bisexual | cross-sectional study | 35.75 | High |
| Thomas, Emily A., et al. [30] | 2011 | 36.57 ‡ | June 2009–September 2009 | the U. S | 191 | MSM | cross-sectional study | 64.40 | Moderate |
| Richard A., et al. [31] | 2011 | 18–24 | — | the U. S | 148 | — | cross-sectional study | 45.27 | Moderate |
| Colon-Lopez, V., et al. [32] | 2012 | 18–26 | 2009–2010 | the U. S | 46 | MSM/heterosexual | cross-sectional study | 76.92 § | Moderate |
| Forster, A. S., et al. [33] | 2012 | 16–18 | March2009 and September 2009 | the U. K | 528 | — | cross-sectional study | 41.10 | High |
| Rank, C., et al. [34] | 2012 | 19–83 | July 2008–February 2009 | Canada | 1041 | homosexual/bisexual/ other | cross-sectional study | 66.95 | High |
| Bourke, L. [35] | 2012 | 18–27 | November 2011–March 2012 | Malaysia | 350 | heterosexual/ homosexual/none | cross-sectional study | 55.43 | Moderate |
| Blodt, S., et al. [36] | 2012 | 18–25 | July 2010 | Germany | 245 | — | cross-sectional study | 8.19 § | Moderate |
| Ortashi, O., et al. [37] | 2013 | 21 ‡ | June 2012–August2012 | U.A. E | 356 | — | cross-sectional study | 46.07 | Moderate |
| Gray, Clive M., et al. [38] | 2013 | 18–60 | September 2010–January 2011 | China | 542 | homosexual/bisexual/ heterosexual | cross-sectional study | 19.93 | High |
| Belani, H. K., et al. [39] | 2014 | 18–45 | November 2010 and February 2011 | India | 178 | — | cross-sectional study | 89.89 | Moderate |
| Gellenoncourt, A. and P. Di Patrizio [40] | 2014 | 16–18 | May 2013–June 2013 | France | 328 | — | cross-sectional study | 34.45 | High |
| Zou, H. C., et al. [41] | 2014 | 16–20 | September 2010–August 2012 | Australia | 200 | MSM | cross-sectional study | 30.00 | Moderate |
| Khurana, S., et al. [42] | 2015 | 11–21 | April 2011–February 2012 | the U. S | 154 | — | cross-sectional study | 15.54 § | High |
| Giuliani, M., et al. [43] | 2016 | 33 ‡ | April 2013–June 2013 | Italy | 423 | MSM/MNSM | cross-sectional study | 34.28 | High |
| Hunter, T. and M. Weinstein [44] | 2016 | 18–26 | — | the U. S | 116 | — | cross-sectional study | 19.83 | Moderate |
| Napolitano, F., et al. [45] | 2016 | 14–24 | January 2015–April 2015 | Italy | 956 | — | cross-sectional study | 58.16 | High |
| Zou, H. C., et al. [46] | 2016 | ≥18 | April 2014–July 2014 | China | 368 | MSM/MNSM | cross-sectional study | 36.68 | Moderate |
| Zhu, J, H., et al. [47] | 2016 | 16–72 | March 2014–September 2014 | China | 422 | MSM | cross-sectional study | 73.46 | Moderate |
| Sadlier, C., et al. [48] | 2016 | ≥18 | January 2014–April 2014 | Ireland | 302 | MSM | cross-sectional study | 30.96 § | Moderate |
| Stephens, Dionne P., et al. [49] | 2016 | 18–24 | — | the U. S | 51 | — | cross-sectional study | 90.20 | Moderate |
| Tian, T. [50] | 2017 | 18–65 | April 2016–October 2016 | China | 500 | homosexual/bisexual | cross-sectional study | 82.00 | High |
| Hoefer, Lea, et al. [51] | 2017 | 18–55 | July 2015.7–October 2015 | Greece | 298 | — | cross-sectional study | 76.85 | Moderate |
| Cheung, T., et al. [52] | 2018 | 16–29 | June 2015–September 2015 | China | 1004 | — | cross-sectional study | 23.30 | High |
| Stanley, C., et al. [53] | 2018 | — | January 2016–May 2016 | Canada | 63 | — | cross-sectional study | 80.39 § | High |
| Cooper, Dexter L., et al. [54] | 2018 | 18–27 | — | the U. S | 190 | heterosexual/ sexual minority | cross-sectional study | 21.05 | Moderate |
| Nadarzynski, T., et al. [55] | 2018 | 14–63 | July 2015–September 2015 | the U. K | 1508 | MSM | cross-sectional study | 83.02 | Moderate |
| Tian, T., et al. [56] | 2019 | — | — | China | 458 | MSM | cross-sectional study | 84.28 | Moderate |
| Wong, L. P., et al. [57] | 2019 | 13–14 | February 2013–April 2013 | Malaysia | 2823 | — | cross-sectional study | 48.39 | High |
| Kuang, J, Y., et al. [58] | 2019 | ≥18 | March 2018–March 2019 | China | 580 | MSM/MNSM | cross-sectional study | 36.90 | low |
| Li, Y, F., et al. [59] | 2019 | 21 ‡ | March 2018–June 2018 | China | 1209 | homosexual/bisexual/ heterosexual | cross-sectional study | 38.46 | High |
| Wang, S., et al. [3] | 2020 | 16–26 | September 2018–December 2018 | China | 1274 | — | cross-sectional study | 38.70 | High |
| Ren, W, J., et al. [60] | 2020 | 22–35 | — | China | 102 | — | cross-sectional study | 9.80 | Moderate |
| Farsi, N. J., et al. [61] | 2021 | 21 ‡ | 2017–2018 | Saudi Arabia | 517 | — | cross-sectional study | 48.55 | High |
| Bai, M, M [62] | 2021 | 18–26 | August 2019–December 2019 | China | 1196 | heterosexual/bisexual/homosexual | cross-sectional study | 54.60 | High |
| Wei He, et al. [63] | 2021 | ≥18 | — | China | 406 | MSM | cross-sectional study | 86.21 | High |
| Ye, Ze-Hao, et al. [64] | 2021 | ≥18 | July 2020–December 2020 | China | 234 | MSM | cross-sectional study | 57.69 | Moderate |
| Chen, Q., et al. [65] | 2022 | 14–55 | — | China | 969 | MSM | cross-sectional study | 82.77 | Moderate |
| Pan, H., et al. [66] | 2022 | 16–45 | June 2021 | China | 889 | MSM | cross-sectional study | 82.79 | High |
| Pham, D., et al. [67] | 2022 | 44 ‡ | — | the U. S | 3342 | homosexual/bisexual/ heterosexual/other | cross-sectional study | 63.26 | Moderate |
| Ran, H., et al. [68] | 2022 | ≥18 | February 2021–May 2021 | China | 912 | heterosexual/ homosexual/bisexual | cross-sectional study | 34.54 | High |
| Shi, J., et al. [6] | 2022 | 16–26 | September 2019–November 2019 | China | 935 | — | cross-sectional study | 38.50 | Moderate |
| Zhang, H, et al. [69] | 2022 | 19.38 ‡ | April 2021 | China | 421 | — | cross-sectional study | 23.52 | High |
| Zhang, J., et al. [70] | 2022 | 18–72 | August 2016–June 2019 | China | 711 | heterosexual/ homosexual/bisexual | cross-sectional study | 42.33 | Moderate |
| Gursoy, M. Y. and F. Sagtas [71] | 2023 | 18–38 | February 2022–April 2022 | Turkey | 1723 | heterosexual/ homosexual/bisexual | cross-sectional study | 10.45 § | Moderate |
| Lv, H, W., et al. [72] | 2023 | ≥18 | July 2022–August 2022 | China | 407 | heterosexual/ homosexual/bisexual | cross-sectional study | 88.53 § | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, F.; Du, Y.; Cao, K.; Chen, C.; Yang, M.; Yan, R.; Yang, S. Acceptance of the Human Papillomavirus Vaccine among General Men and Men with a Same-Sex Orientation and Its Influencing Factors: A Systematic Review and Meta-Analysis. Vaccines 2024, 12, 16. https://doi.org/10.3390/vaccines12010016
Shen F, Du Y, Cao K, Chen C, Yang M, Yan R, Yang S. Acceptance of the Human Papillomavirus Vaccine among General Men and Men with a Same-Sex Orientation and Its Influencing Factors: A Systematic Review and Meta-Analysis. Vaccines. 2024; 12(1):16. https://doi.org/10.3390/vaccines12010016
Chicago/Turabian StyleShen, Fang, Yuxia Du, Kexin Cao, Can Chen, Mengya Yang, Rui Yan, and Shigui Yang. 2024. "Acceptance of the Human Papillomavirus Vaccine among General Men and Men with a Same-Sex Orientation and Its Influencing Factors: A Systematic Review and Meta-Analysis" Vaccines 12, no. 1: 16. https://doi.org/10.3390/vaccines12010016
APA StyleShen, F., Du, Y., Cao, K., Chen, C., Yang, M., Yan, R., & Yang, S. (2024). Acceptance of the Human Papillomavirus Vaccine among General Men and Men with a Same-Sex Orientation and Its Influencing Factors: A Systematic Review and Meta-Analysis. Vaccines, 12(1), 16. https://doi.org/10.3390/vaccines12010016