
Using a Dynamic Model to Estimate the Cost-Effectiveness of HPV Vaccination in Iran

Abstract
:1. Introduction
2. Material and Methods
2.1. Overview
2.2. Dynamic Transmission Model
2.3. Costs
2.4. Scenarios
3. Results
3.1. Initial Situation
3.2. Scenario Analysis
3.2.1. Health Outcomes
3.2.2. Budget Impact
3.2.3. Cost-Effectiveness Analysis
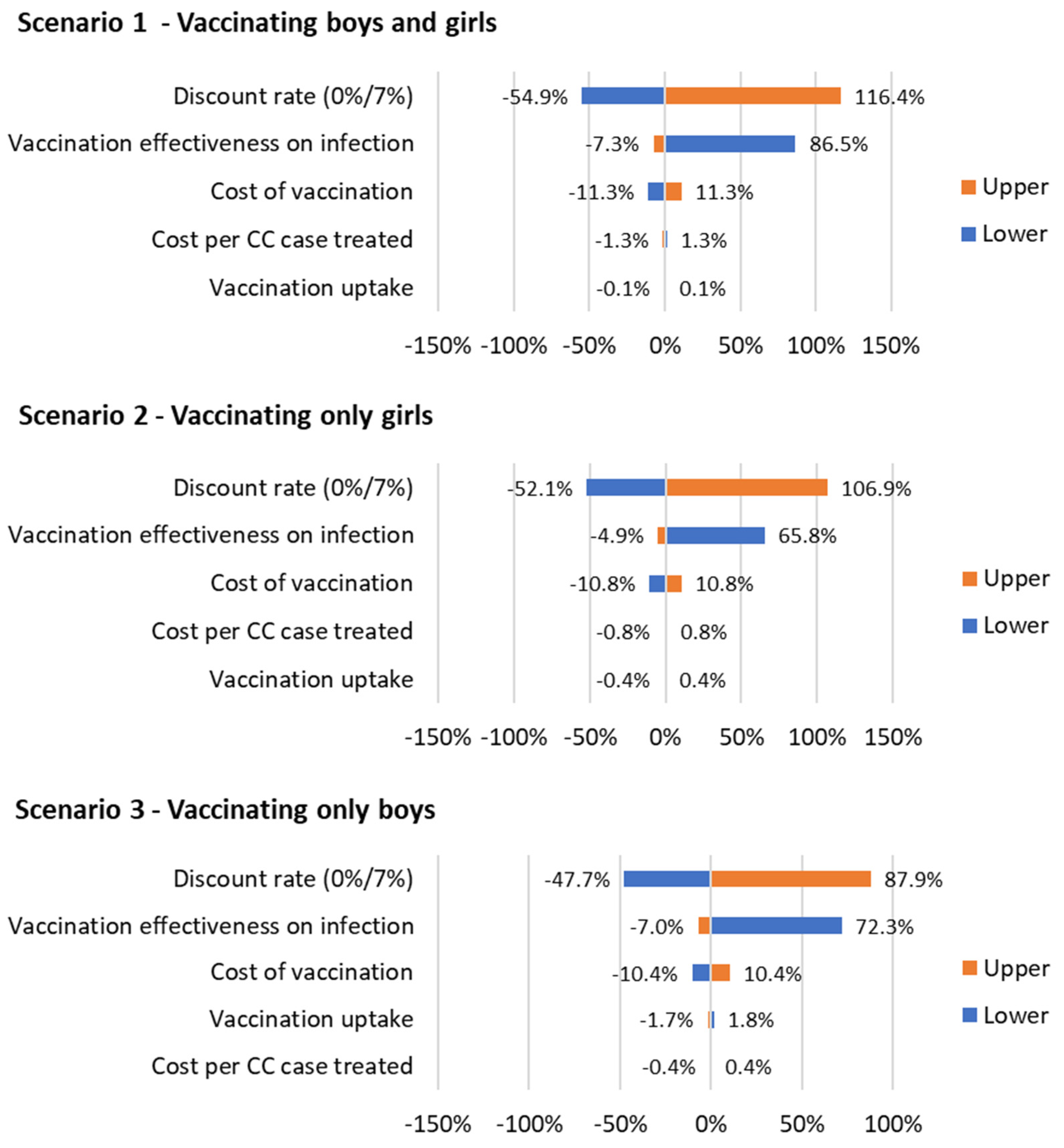
3.2.4. Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| CC | Cervical cancer |
| DALYs | Disability-adjusted life years |
| GDP | Gross domestic product |
| HPV | Human papillomavirus |
| ICER | Incremental cost-effectiveness ratio |
| LMICs | Low- and middle-income countries |
| QALYs | Quality-adjusted life years |
| USD | United States dollars |
| WTP | Willingness to pay |
References
- Meites, E.; Szilagyi, P.G.; Chesson, H.W.; Unger, E.R.; Romero, J.R.; Markowitz, L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 698–702. [Google Scholar] [CrossRef]
- World Health Organization. Sexually Transmitted Infections: Evidence Brief (WHO/RHR/19.22); World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/handle/10665/329888 (accessed on 20 June 2023).
- CDC. STD Facts—Human Papillomavirus (HPV). 20 December 2022. Available online: https://www.cdc.gov/std/hpv/stdfact-hpv.htm (accessed on 20 December 2022).
- Burger, E.A.; Lee, K.; Saraiya, M.; Thompson, T.D.; Chesson, H.W.; Markowitz, L.E.; Kim, J.J. Racial and ethnic disparities in human papillomavirus-associated cancer burden with first-generation and second-generation human papillomavirus vaccines: Racial/Ethnic Disparities in Cancer Burden. Cancer 2016, 122, 2057–2066. [Google Scholar] [CrossRef]
- WHO. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem. 2020. Available online: https://www.who.int/publications-detail-redirect/9789240014107 (accessed on 20 June 2023).
- Gallagher, K.E.; LaMontagne, D.S.; Watson-Jones, D. Status of HPV vaccine introduction and barriers to country uptake. Vaccine 2018, 36, 4761–4767. [Google Scholar] [CrossRef] [PubMed]
- WHO. Cervical Cancer. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 20 June 2023).
- Luvsan, M.-E.; Vodicka, E.; Jugder, U.; Tudev, U.; Clark, A.; Groman, D.; Otgonbayar, D.; Demberelsuren, S.; LaMongtagne, D.S.; Pecenka, C. The potential cost-effectiveness of HPV vaccination among girls in Mongolia. Vaccine X 2022, 11, 100161. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.; Pink, J.; Medley, G.F.; Petrou, S.; Staniszewska, S.; Underwood, M.; Sonnenberg, P.; Keeling, M.J. Assessing the cost-effectiveness of HPV vaccination strategies for adolescent girls and boys in the UK. BMC Infect. Dis. 2019, 19, 552. [Google Scholar] [CrossRef]
- Safaeian, F.; Ghaemimood, S.; El-Khatib, Z.; Enayati, S.; Mirkazemi, R.; Reeder, B. Burden of Cervical Cancer in the Eastern Mediterranean Region During the Years 2000 and 2017: Retrospective Data Analysis of the Global Burden of Disease Study. JMIR Public Health Surveill. 2021, 7, e22160. [Google Scholar] [CrossRef]
- Sargazi, N.; Daroudi, R.; Zendehdel, K.; Hashemi, F.A.; Tahmasebi, M.; Darrudi, A.; Nahvijou, A. Economic Burden of Gynecological Cancers in Iran. Value Health Reg. Issues 2022, 28, 1–6. [Google Scholar] [CrossRef]
- WHO. Life Tables: Life Tables by Country Iran (Islamic Republic of). 2023. Available online: https://apps.who.int/gho/data/view.searo.60760?lang=en (accessed on 30 June 2023).
- World Bank. World Bank Open Data; World Bank: Washington, DC, USA, 2023; Available online: https://data.worldbank.org (accessed on 20 June 2023).
- CDC. HPV Vaccine Safety and Effectiveness CDC. 6 May 2022. Available online: https://www.cdc.gov/vaccines/vpd/hpv/hcp/safety-effectiveness.html (accessed on 6 May 2022).
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S.; ICO/IARC Information Centre on HPV and Cancer. Human Papillomavirus and Related Diseases in Iran (Islamic Republic of); Summary Report 10 March 2023; ICO/IARC. 2023. Available online: https://hpvcentre.net/statistics/reports/IRN.pdf (accessed on 27 June 2023).
- Twenge, J.M.; Sherman, R.A.; Wells, B.E. Declines in Sexual Frequency among American Adults, 1989–2014. Arch. Sex. Behav. 2017, 46, 2389–2401. [Google Scholar] [CrossRef]
- Darroch, J.E.; Landry, D.J.; Oslak, S. Age differences between sexual partners in the United States. Fam. Plan. Perspect. 1999, 31, 160–167. [Google Scholar] [CrossRef]
- Emrani, Z.; Akbari Sari, A.; Zeraati, H.; Olyaeemanesh, A.; Daroudi, R. Health-related quality of life measured using the EQ-5D–5 L: Population norms for the capital of Iran. Health Qual. Life Outcomes 2020, 18, 108. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Disability Weights GHDx [Dataset]. 2018. Available online: https://ghdx.healthdata.org/record/ihme-data/gbd-2017-disability-weights (accessed on 6 June 2023).
- Emmerson, J.; Kim, D.D. DALY Calculator; Center for the Evaluation of Value and Risk in Health, Tufts Medical Center: Boston, MA, USA, 2018. [Google Scholar]
- NICE. Guide to the Methods of Technology Appraisal; NICE: Ra’anana, Israel, 2004. [Google Scholar]
- Sargazi, N.; Takian, A.; Daroudi, R.; Nahvijou, A.; Yaseri, M.; Ghanbari Motlagh, A.; Zendehdel, K. Cost-Benefit Analysis of Human Papillomavirus Vaccine in Iran. J. Prev. 2022, 43, 841–857. [Google Scholar] [CrossRef]
- Cordova-Pozo, K.; Rouwette, E.A.J.A. Types of scenario planning and their effectiveness: A review of reviews. Futures 2023, 149, 103153. [Google Scholar] [CrossRef]
- Hagens, A.; İnkaya, A.Ç.; Yildirak, K.; Sancar, M.; van der Schans, J.; Acar Sancar, A.; Ünal, S.; Postma, M.; Yeğenoğlu, S. COVID-19 Vaccination Scenarios: A Cost-Effectiveness Analysis for Turkey. Vaccines 2021, 9, 399. [Google Scholar] [CrossRef]
- World Health Organization; Baltussen, R.M.P.M.; Adam, T.; Tan-Torres Edejer, T.; Hutubessy, R.C.W.; Acharya, A.; Evans, D.B.; Murray, C.J.L. Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis; World Health Organization: Geneva, Switzerland, 2003; Available online: https://apps.who.int/iris/handle/10665/42699 (accessed on 20 June 2023).
- Walker, D.G.; Hutubessy, R.; Beutels, P. WHO Guide for standardisation of economic evaluations of immunization programmes. Vaccine 2010, 28, 2356–2359. [Google Scholar] [CrossRef] [PubMed]
- Rosettie, K.L.; Joffe, J.N.; Sparks, G.W.; Aravkin, A.; Chen, S.; Compton, K.; Ewald, S.B.; Mathew, E.B.; Michael, D.; Pedroza Velandia, P.; et al. Cost-Effectiveness of HPV Vaccination in 195 Countries: A Meta-Regression Analysis. PLoS ONE 2021, 16, e0260808. [Google Scholar] [CrossRef] [PubMed]
- Drolet, M.; Laprise, J.-F.; Martin, D.; Jit, M.; Bénard, É.; Gingras, G.; Boily, M.-C.; Alary, M.; Baussano, I.; Hutubessy, R.; et al. Optimal human papillomavirus vaccination strategies to prevent cervical cancer in low-income and middle-income countries in the context of limited resources: A mathematical modelling analysis. Lancet Infect. Dis. 2021, 21, 1598–1610. [Google Scholar] [CrossRef] [PubMed]
- Kosen, S.; Andrijono, A.; Ocviyanti, D.; Indriatmi, W. The Cost-Effectiveness of Quadrivalent Human Papillomavirus Vaccination in Indonesia. Asian Pac. J. Cancer Prev. APJCP 2017, 18, 2011–2017. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.P.; Ortiz-Ortiz, K.J.; Ríos, M.; Laborde, J.; Kulkarni, A.; Pillsbury, M.; Lauschke, A.; Monsanto, H.A.; Marques-Goyco, C. Modelling the effects of quadrivalent Human Papillomavirus (HPV) vaccination in Puerto Rico. PLoS ONE 2017, 12, e0184540. [Google Scholar] [CrossRef] [PubMed]
- Cheung, T.H.; Cheng, S.S.Y.; Hsu, D.C.; Wong, Q.W.-L.; Pavelyev, A.; Walia, A.; Saxena, K.; Prabhu, V.S. The impact and cost-effectiveness of 9-valent human papillomavirus vaccine in adolescent females in Hong Kong. Cost Eff. Resour. Alloc. 2021, 19, 75. [Google Scholar] [CrossRef]
- Damm, O.; Horn, J.; Mikolajczyk, R.T.; Kretzschmar, M.E.E.; Kaufmann, A.M.; Deleré, Y.; Ultsch, B.; Wichmann, O.; Krämer, A.; Greiner, W. Cost-effectiveness of human papillomavirus vaccination in Germany. Cost Eff. Resour. Alloc. 2017, 15, 18. [Google Scholar] [CrossRef]
- Laprise, J.-F.; Drolet, M.; Boily, M.-C.; Jit, M.; Sauvageau, C.; Franco, E.L.; Lemieux-Mellouki, P.; Malagón, T.; Brisson, M. Comparing the cost-effectiveness of two- and three-dose schedules of human papillomavirus vaccination: A transmission-dynamic modelling study. Vaccine 2014, 32, 5845–5853. [Google Scholar] [CrossRef] [PubMed]
- Majed, L.; Bresse, X.; El Mouaddin, N.; Schmidt, A.; Daniels, V.J.; Pavelyev, A.; Levy-Bachelot, L.; Elbasha, E. Public health impact and cost-effectiveness of a nine-valent gender-neutral HPV vaccination program in France. Vaccine 2021, 39, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Uusküla, A.; Müürsepp, A.; Kawai, K.; Raag, M.; Jürisson, M.; Pillsbury, M. The epidemiological and economic impact of a quadrivalent human papillomavirus (hpv) vaccine in Estonia. BMC Infect. Dis. 2013, 13, 304. [Google Scholar] [CrossRef]
- Population Pyramid. Population Pyramids of Iran from 1950 to 2100. Available online: https://www.populationpyramid.net/world/2023/ (accessed on 30 June 2023).
- Macrotrends. Iran Birth Rate 1950–2023. Available online: https://www.macrotrends.net/countries/IRN/iran/birth-rate (accessed on 30 June 2023).
- Macrotrends. Iran Death Rate 1950–2023. 2023. Available online: https://www.macrotrends.net/countries/IRN/iran/death-rate (accessed on 30 June 2023).
- Trottier, H.; Mahmud, S.; Prado, J.C.M.; Sobrinho, J.S.; Costa, M.C.; Rohan, T.E.; Villa, L.L.; Franco, E.L. Type-Specific Duration of Human Papillomavirus Infection: Implications for Human Papillomavirus Screening and Vaccination. J. Infect. Dis. 2008, 197, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- NCI. HPV and Cancer. 2019. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer (accessed on 30 June 2023).
- American Cancer Society. Cancer Facts & Figures 2023. 2023. Available online: https://www.cancer.org/cancer/types/cervical-cancer/detection-diagnosis-staging/survival.html (accessed on 30 June 2023).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scenario | Costs (USD) | QALYs | Deaths | Incremental | ICER | ||
|---|---|---|---|---|---|---|---|
| Costs (USD) | QALYs | Deaths | |||||
| Baseline (no vac) | 867,751,387 | 2,158,770,017 | 112,796 | ||||
| 1. Vaccinating boys and girls | 2,557,840,626 | 2,158,983,533 | 87,301 | 1,690,089,239 | 213,516 | −25,496 | 7916 |
| 2. Vaccinating only girls | 1,712,938,252 | 2,158,940,799 | 92,269 | 845,186,865 | 170,782 | −20,527 | 4949 |
| 3. Vaccinating only boys | 1,613,029,477 | 2,158,818,009 | 107,728 | 745,278,090 | 47,992 | −5068 | 15,529 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagens, A.; Sloof, A.C.; Janghorban, R. Using a Dynamic Model to Estimate the Cost-Effectiveness of HPV Vaccination in Iran. Vaccines 2024, 12, 438. https://doi.org/10.3390/vaccines12040438
Hagens A, Sloof AC, Janghorban R. Using a Dynamic Model to Estimate the Cost-Effectiveness of HPV Vaccination in Iran. Vaccines. 2024; 12(4):438. https://doi.org/10.3390/vaccines12040438
Chicago/Turabian StyleHagens, Arnold, Albertus Constantijn Sloof, and Roksana Janghorban. 2024. "Using a Dynamic Model to Estimate the Cost-Effectiveness of HPV Vaccination in Iran" Vaccines 12, no. 4: 438. https://doi.org/10.3390/vaccines12040438
APA StyleHagens, A., Sloof, A. C., & Janghorban, R. (2024). Using a Dynamic Model to Estimate the Cost-Effectiveness of HPV Vaccination in Iran. Vaccines, 12(4), 438. https://doi.org/10.3390/vaccines12040438