Eliminating Cervical Cancer in Mali and Senegal, Two Sub-Saharan Countries: Insights and Optimizing Solutions

Abstract
:1. Introduction
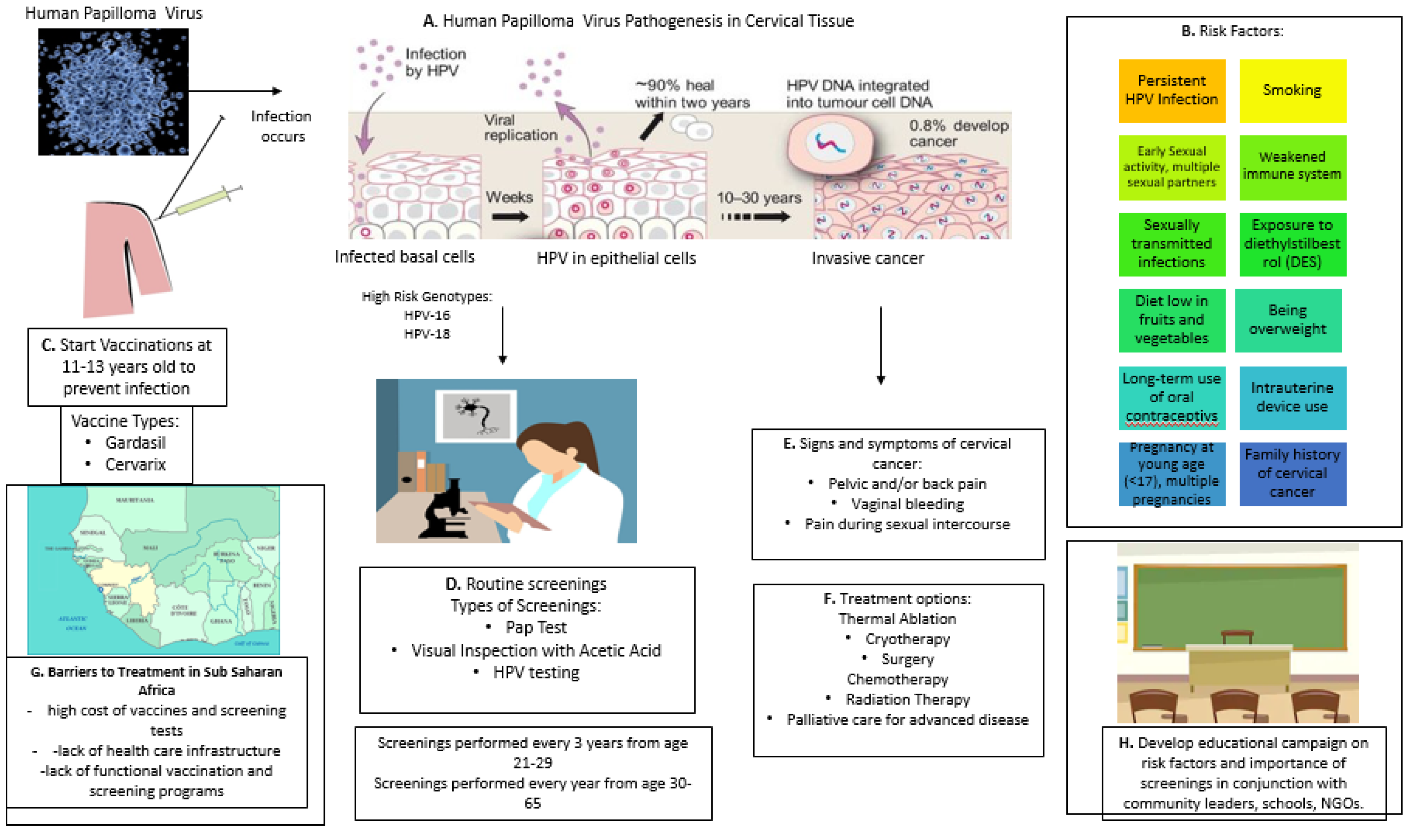
2. Pathogenesis of HPV in Cervical Cancer
3. HPV Vaccination
4. Screening
5. Cervical Cancer: The Sub-Saharan (Mali and Senegal) Africa Perspective
6. HPV Vaccination in Mali and Senegal
7. Cervical Cancer Screenings in Mali and Senegal
7.1. Mali
7.2. Senegal
8. Insights and Potential Measures to Eliminate Cervical Cancer in Mali and Senegal
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ramaswami, R.; Paulino, E.; Barrichello, A.; Nogueira-Rodrigues, A.; Bukowski, A.; Louis, J.S.; Goss, P.E. Disparities in Breast, Lung, and Cervical Cancer Trials Worldwide. J. Glob. Oncol. 2018, 4, 1–11. [Google Scholar] [CrossRef]
- Sahasrabuddhe, V.V.; Parham, G.P.; Mwanahamuntu, M.H.; Vermund, S.H. Cervical cancer prevention in low- and middle-income countries: Feasible, affordable, essential. Cancer Prev. Res. 2011, 5, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Vu, M.; Yu, J.; Awolude, O.A.; Chuang, L. Cervical cancer worldwide. Curr. Probl. Cancer 2018, 42, 457–465. [Google Scholar] [CrossRef]
- Shrestha, A.D.; Neupane, D.; Vedsted, P.; Kallestrup, P. Cervical Cancer Prevalence, Incidence and Mortality in Low and Middle Income Countries: A Systematic Review. Asian Pac. J. Cancer Prev. 2018, 19, 319–324. [Google Scholar]
- Cohen, P.A.; Jhingran, A.; Oaknin, A.; Denny, L. Cervical cancer. Lancet 2019, 393, 169–182. [Google Scholar] [CrossRef]
- Itarat, Y.; Kietpeerakool, C.; Jampathong, N.; Chumworathayi, B.; Kleebkaow, P.; Aue-Aungkul, A.; Nhokaew, W. Sexual behavior and infection with cervical human papillomavirus types 16 and 18. Int. J. Women’s Heal. 2019, 11, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Schiffman, M.; Doorbar, J.; Wentzensen, N.; De Sanjosé, S.; Fakhry, C.; Monk, B.J.; Stanley, M.A.; Franceschi, S. Carcinogenic human papillomavirus infection. Nat. Rev. Dis. Prim. 2016, 2, 16086. [Google Scholar] [CrossRef]
- Banister, C.E.; Liu, C.; Pirisi, L.; Creek, K.E.; Buckhaults, P.J. Identification and characterization of HPV-independent cervical cancers. Oncotarget 2017, 8, 13375–13386. [Google Scholar] [CrossRef] [Green Version]
- De Martel, C.; Plummer, M.T.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Deivendran, S.; Marzook, K.H.; Pillai, M.R. The role of inflammation in cervical cancer. In Inflammation and Cancer; Springer: Berlin/Heidelberg, Germany, 2014; pp. 377–399. [Google Scholar]
- Dugué, P.-A.; Rebolj, M.; Garred, P.; Lynge, E. Immunosuppression and risk of cervical cancer. Expert Rev. Anticancer. Ther. 2013, 13, 29–42. [Google Scholar] [CrossRef]
- Ebrahimi, S.; Soltani, A.; Hashemy, S.I. Oxidative stress in cervical cancer pathogenesis and resistance to therapy. J. Cell. Biochem. 2018, 120, 6868–6877. [Google Scholar] [CrossRef]
- Simms, K.T.; Steinberg, J.; Caruana, M.; A Smith, M.; Lew, J.-B.; Soerjomataram, I.; E Castle, P.; Bray, F.; Canfell, K. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020–2099: A modelling study. Lancet Oncol. 2019, 20, 394–407. [Google Scholar] [CrossRef]
- Petrosky, E.; Bocchini, J.A.; Hariri, S.; Chesson, H.; Curtis, C.R.; Saraiya, M.; Unger, E.R.; Markowitz, L.E. Use of 9-Valent Human Papillomavirus (HPV) Vaccine: Updated HPV Vaccination Recommendations of the Advisory Committee on Immunization Practices. MMWR. Morb. Mortal. Wkly. Rep. 2015, 64, 300–304. [Google Scholar]
- Patel, C.; Brotherton, J.M.; Pillsbury, A.; Jayasinghe, S.; Donovan, B.; Macartney, K.; Marshall, H.S. The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: What additional disease burden will a nonavalent vaccine prevent? Eurosurveillance 2018, 23, 1700737. [Google Scholar] [CrossRef]
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M.; HPV Vaccination Impact Study Group; Ali, H.; Boily, M.-C.; Baldo, V.; Brassard, P.; Brotherton, J.M.L.; et al. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef] [Green Version]
- Bhatla, N.; Nene, B.M.; Joshi, S.; Esmy, P.O.; Joshi, G.; Poli, U.R.R.; Verma, Y.; Zomawia, E.; Pimple, S.; Prabhu, P.R.; et al. Are two doses of human papillomavirus vaccine sufficient for girls aged 15–18 years? Results from a cohort study in India. Papillomavirus Res. 2018, 5, 163–171. [Google Scholar] [CrossRef]
- Sonawane, K.; Nyitray, A.G.; Nemutlu, G.S.; Swartz, M.D.; Chhatwal, J.; A Deshmukh, A. Prevalence of Human Papillomavirus Infection by Number of Vaccine Doses Among US Women. JAMA Netw. Open 2019, 2, e1918571. [Google Scholar] [CrossRef]
- Kjaer, S.K.; Nygård, M.; Dillner, J.; Marshall, J.B.; Radley, D.; Li, M.; Munk, C.; Hansen, B.T.; Sigurdardottir, L.G.; Hortlund, M.; et al. A 12-Year Follow-up on the Long-Term Effectiveness of the Quadrivalent Human Papillomavirus Vaccine in 4 Nordic Countries. Clin. Infect. Dis. 2017, 66, 339–345. [Google Scholar] [CrossRef]
- Patanwala, I.Y.; Bauer, H.M.; Miyamoto, J.; Park, I.U.; Huchko, M.J.; Smith-McCune, K.K. A systematic review of randomized trials assessing human papillomavirus testing in cervical cancer screening. Am. J. Obstet. Gynecol. 2012, 208, 343–353. [Google Scholar] [CrossRef] [Green Version]
- Clarke, M.A.; Gradissimo, A.; Schiffman, M.; Lam, J.; Sollecito, C.C.; Fetterman, B.; Lorey, T.; Poitras, N.E.; Raine-Bennett, T.; Castle, P.E.; et al. Human Papillomavirus DNA Methylation as a Biomarker for Cervical Precancer: Consistency across 12 Genotypes and Potential Impact on Management of HPV-Positive Women. Clin. Cancer Res. 2018, 24, 2194–2202. [Google Scholar] [CrossRef] [Green Version]
- Pardini, B.; De Maria, D.; Francavilla, A.; Di Gaetano, C.; Ronco, G.; Naccarati, A. MicroRNAs as markers of progression in cervical cancer: A systematic review. BMC Cancer 2018, 18, 696. [Google Scholar] [CrossRef] [PubMed]
- Sahasrabuddhe, V.V.; Gravitt, P.E.; Dunn, S.T.; Brown, D.; Allen, R.A.; Eby, Y.J.; Smith, K.; Zuna, R.E.; Zhang, R.R.; Gold, M.A.; et al. Comparison of Human Papillomavirus Detections in Urine, Vulvar, and Cervical Samples from Women Attending a Colposcopy Clinic. J. Clin. Microbiol. 2013, 52, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Guidelines for Screening and Treatment of Precancerous Lesions for Cervical Cancer Prevention; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Lekoane, K.M.B.; Kuupiel, D.; Mashamba-Thompson, T.P.; Ginindza, T.G. Evidence on the prevalence, incidence, mortality and trends of human papilloma virus-associated cancers in sub-Saharan Africa: Systematic scoping review. BMC Cancer 2019, 19, 563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GLOBOCAN. Senegal. Number of Cervical Cancer Cases. 2018. Available online: http://gco.iarc.fr/today/data/factsheets/populations/686-senegal-fact-sheets.pdf (accessed on 14 April 2020).
- Mbaye, E.H.S.; Gheit, T.; Dem, A.; McKay-Chopin, S.; Toure-Kane, N.C.; Mboup, S.; Tommasino, M.; Sylla, B.S.; Boye, C.S.B. Human papillomavirus infection in women in four regions of Senegal. J. Med. Virol. 2013, 86, 248–256. [Google Scholar] [CrossRef]
- Muwonge, R.; for the IARC Multicentre Study Group on Cervical Cancer Early Detection; Mbus, L.N.; Ngoma, T.; Mbalawa, C.G.; Dolo, A.; Manuel, M.D.G.; Nouhou, H.; Nacoulma, M.; Mwaiselage, J.; et al. Socio-demographic and reproductive determinants of cervical neoplasia in seven sub-Sahara African countries. Cancer Causes Control. 2016, 27, 1437–1446. [Google Scholar] [CrossRef]
- Anorlu, R.I. Cervical cancer: The sub-Saharan African perspective. Reprod. Heal. Matters 2008, 16, 41–49. [Google Scholar] [CrossRef]
- De Abreu, A.L.; Malaguti, N.; Souza, R.P.; Uchimura, N.S.; Ferreira, É.C.; Pereira, M.W.; Carvalho, M.D.; Pelloso, S.M.; Bonini, M.G.; Gimenes, F.; et al. Association of human papillomavirus, Neisseria gonorrhoeae and Chlamydia trachomatis co-infections on the risk of high-grade squamous intraepithelial cervical lesion. Am. J. Cancer Res. 2016, 6, 1371–1383. [Google Scholar]
- Kharsany, A.B.M.; Karim, Q.A. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportunities. Open AIDS J. 2016, 10, 34–48. [Google Scholar] [CrossRef] [Green Version]
- Denslow, S.A.; Rositch, A.; Firnhaber, C.; Ting, J.; Smith, J.S. Incidence and progression of cervical lesions in women with HIV: A systematic global review. Int. J. STD AIDS 2013, 25, 163–177. [Google Scholar] [CrossRef]
- Hawes, S.E.; Critchlow, C.W.; Niang, M.A.F.; Diouf, M.B.; Diop, A.; Toure, P.; Kasse, A.A.; Dembele, B.; Sow, P.S.; Coll-Seck, A.M.; et al. Increased Risk of High-Grade Cervical Squamous Intraepithelial Lesions and Invasive Cervical Cancer among African Women with Human Immunodeficiency Virus Type 1 and 2 Infections. J. Infect. Dis. 2003, 188, 555–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Working Together for Health: The World Health Report 2006; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Teguete, I.; Dolo, A.; Sangare, K.; Sissoko, A.; Rochas, M.; Beseme, S.; Tounkara, K.; Yekta, S.; De Groot, A.S.; Koita, O.A. Prevalence of HPV 16 and 18 and attitudes toward HPV vaccination trials in patients with cervical cancer in Mali. PLoS ONE 2017, 12, e0172661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tracy, J.K.; Traore, C.B.; Bakarou, K.; Dembelé, R.; Sacko, R.C.D.F.; Sow, S.O. Risk Factors for High-risk Human Papilloma Virus Infection in Unscreened Malian Women. Trop. Med. Int. Heal. 2011, 16, 1432–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teguete, I.; Muwonge, R.; Traoré, C.; Dolo, A.; Bayo, S.; Sankaranarayanan, R. Can visual cervical screening be sustained in routine health services? Experience from Mali, Africa. BJOG Int. J. Obstet. Gynaecol. 2011, 119, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Barrionuevo-Rosas, L.; Albero, G.; Aldea, M.; Serrano, B.; Valencia, S.; Brotons, M.; Mena, M.; Cosano, R.; Muñoz, J.; et al. ICO information centre on HPV and cancer (HPV Information Centre). Human papillomavirus and related diseases in the world. Summ. Rep. 2015, 4, 20140822. [Google Scholar]
- Gabrielli, S.; Maggioni, E.; Fieschi, L. Cervical cancer prevention in Senegal: An International Cooperation Project Report. Acta Biomed 2018, 89, 29–34. [Google Scholar]
- Dykens, J.A.; Linn, A.M.; Irwin, T.; E Peters, K.; Pyra, M.; Traoré, F.; Diarra, M.T.; Hasnain, M.; Wallner, K.; Linn, P.; et al. Implementing visual cervical cancer screening in Senegal: A cross-sectional study of risk factors and prevalence highlighting service utilization barriers. Int. J. Women’s Heal. 2017, 9, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Fall, N.S.; Tamalet, C.; Diagne, N.; Fenollar, F.; Raoult, D.; Sokhna, C.; Lagier, J.-C. Feasibility, Acceptability, and Accuracy of Vaginal Self-Sampling for Screening Human Papillomavirus Types in Women from Rural Areas in Senegal. Am. J. Trop. Med. Hyg. 2019, 100, 1552–1555. [Google Scholar] [CrossRef]
- de la Statistique, A.N. de la Démographie (ANSD) Sénégal; Maryland: ANSD and Macro International, Inc.: Calverton, NY, USA, 2010. [Google Scholar]
- Kane, C.T.; Diawara, S.; Ndiaye, H.D.; Diallo, P.A.; Wade, A.S.; Diallo, A.G.; Belec, L.; Mboup, S. Concentrated and linked epidemics of both HSV-2 and HIV-1/HIV-2 infections in Senegal: Public health impacts of the spread of HIV. Int. J. STD AIDS 2009, 20, 793–796. [Google Scholar] [CrossRef]
- Diop-Ndiaye, H.; Beiter, K.; Gheit, T.; Ndoye, A.S.; Dramé, A.; McKay-Chopin, S.; Tommasino, M.; Boye, C.S.B.; Sylla, B.; Kane, C.T. Human Papillomavirus infection in senegalese female sex workers. Papillomavirus Res. 2019, 7, 97–101. [Google Scholar] [CrossRef]
- Hanisch, R.; Cherne, S.L.; Sow, P.S.; Winer, R.L.; Hughes, J.P.; Feng, Q.; Gottlieb, G.; Toure, M.; Dem, A.; Kiviat, N.B.; et al. Human papillomavirus type 16 viral load in relation to HIV infection, cervical neoplasia and cancer in Senegal. Cancer Epidemiol. 2014, 38, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Ntekim, A. Cervical Cancer in Sub Sahara Africa, Topics on Cervical Cancer with an Advocacy for Prevention; IntechOpen: London, UK, 2012. [Google Scholar]
- O’Donovan, J.; O’Donovan, C.; Nagraj, S. The role of community health workers in cervical cancer screening in low-income and middle-income countries: A systematic scoping review of the literature. BMJ Glob. Heal. 2019, 4, e001452. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, N.; Sunwoo, J.B.; Starmer, H.M. Implementation of a targeted HPV educational program in a population with HIV. World J. Otorhinolaryngol. Head Neck Surg. 2019, 5, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Sankaranarayanan, R. Screening for Cancer in Low- and Middle-Income Countries. Ann. Glob. Heal. 2014, 80, 412–417. [Google Scholar] [CrossRef]
- Untiet, S.; Vassilakos, P.; McCarey, C.; Tebeu, P.M.; Kengne-Fosso, G.; Menoud, P.-A.; Boulvain, M.; Navarria, I.; Petignat, P. HPV self-sampling as primary screening test in sub-Saharan Africa: Implication for a triaging strategy. Int. J. Cancer 2014, 135, 1911–1917. [Google Scholar] [CrossRef]
- Arbyn, M.; Verdoodt, F.; Snijders, P.J.F.; Verhoef, V.M.J.; Suonio, E.; Dillner, L.; Minozzi, S.; Bellisario, C.; Banzi, R.; Zhao, F.-H.; et al. Accuracy of human papillomavirus testing on self-collected versus clinician-collected samples: A meta-analysis. Lancet Oncol. 2014, 15, 172–183. [Google Scholar] [CrossRef]
- Logie, D.E.; Harding, R. An evaluation of a morphine public health programme for cancer and AIDS pain relief in Sub-Saharan Africa. BMC Public Heal. 2005, 5, 82. [Google Scholar] [CrossRef] [Green Version]
- Denny, L.; Anorlu, R. Cervical Cancer in Africa. Cancer Epidemiology Biomarkers Prev. 2012, 21, 1434–1438. [Google Scholar] [CrossRef] [Green Version]
- Denny, L.; Kuhn, L.; Hu, C.-C.; Tsai, W.-Y.; Wright, T.C. Human Papillomavirus–Based Cervical Cancer Prevention: Long-term Results of a Randomized Screening Trial. J. Natl. Cancer Inst. 2010, 102, 1557–1567. [Google Scholar] [CrossRef] [Green Version]
- Sankaranarayanan, R.; Nene, B.M.; Shastri, S.S.; Jayant, K.; Muwonge, R.; Budukh, A.M.; Hingmire, S.; Malvi, S.G.; Thorat, R.; Kothari, A.; et al. HPV Screening for Cervical Cancer in Rural India. N. Engl. J. Med. 2009, 360, 1385–1394. [Google Scholar] [CrossRef] [Green Version]
- Clendinen, C.; Zhang, Y.; Warburton, R.N.; Light, D.W. Manufacturing costs of HPV vaccines for developing countries. Vaccine 2016, 34, 5984–5989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munira, S.L.; Hendriks, J.T.; Atmosukarto, I.I.; Friede, M.H.; Carter, L.M.; Butler, J.R.; Clements, A.C. A cost analysis of producing vaccines in developing countries. Vaccine 2019, 37, 1245–1251. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| A. Screening Tests | B. Requirements | C. Advantages | D. Disadvantages | E. Remarks |
|---|---|---|---|---|
| Pap Test |
|
|
|
|
| Visual Inspection with Acetic Acid (VIA) |
|
|
|
|
| HPV Testing Not recommendedfor women ages 21 to 29. In this groupHPV infection common |
|
|
|
|
| A. Awareness | B. Vaccination | C. Screening | D. Health Care Delivery |
|---|---|---|---|
| Knowledge of causes and potential remedies | Integration of anti-HPV vaccines into EPI by participation of local government and vaccine alliance (GAVI) | Integrate regular screenings into existing HIV or other reproductive health services if available | Training local health care personnel including midwives at the primary and tertiary level |
| Involve civil society and communities | Immunize with 2-dose vaccine, Gardasil 4, 9 (Merck) or Cervarix (GSK) Assess vaccine efficacity in individual country, monitor post-vaccination adverse side effects if any | Educate on timing and purpose of screenings to increase participation | Local health workers will lead educational campaigns |
| Community meetings and respect of local customs | Trusted source (CDC) recommends that preteens receive the vaccine at around age 11 or 12 years old | Strengthen local cervical cancer screening capacity | Establish community-participatory health services |
| Education of disease risk factors at primary school level | Catch-up vaccinations, Target sex workers and unvaccinated women | Negotiate affordably priced screening tests | Staging of cancer Access to Cryotherapy to destroy precancerous cells on cervix, a non-expensive procedure |
| Community leaders help end stigmas associated with STDs and promote vaccine acceptance | Negotiate vaccine pricing with the manufactures by local government and GAVI to increase access | Adapt screening tools based on cultural and practical considerations (acceptability, feasibility, cost, etc.) | Access to surgery to remove cancerous cells Access to Radiation therapy often offered in combination with chemotherapy. Above procedures hardly practiced in Sub-Saharan Africa because of cost and lack of qualified personnel |
| Leverage local newspapers, journals, television, social media, and mobile phones to promote educational materials | Set up regional vaccine production plants through cooperation of manufacturing pharmaceutical companies in conjunction with government and international aid organizations | Create local infrastructure to perform various screening tests | Make available Palliative care for advanced disease |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haque, A.; Kouriba, B.; Aïssatou, N.; Pant, A. Eliminating Cervical Cancer in Mali and Senegal, Two Sub-Saharan Countries: Insights and Optimizing Solutions. Vaccines 2020, 8, 181. https://doi.org/10.3390/vaccines8020181
Haque A, Kouriba B, Aïssatou N, Pant A. Eliminating Cervical Cancer in Mali and Senegal, Two Sub-Saharan Countries: Insights and Optimizing Solutions. Vaccines. 2020; 8(2):181. https://doi.org/10.3390/vaccines8020181
Chicago/Turabian StyleHaque, Azizul, Bourèma Kouriba, N’diaye Aïssatou, and Anudeep Pant. 2020. "Eliminating Cervical Cancer in Mali and Senegal, Two Sub-Saharan Countries: Insights and Optimizing Solutions" Vaccines 8, no. 2: 181. https://doi.org/10.3390/vaccines8020181
APA StyleHaque, A., Kouriba, B., Aïssatou, N., & Pant, A. (2020). Eliminating Cervical Cancer in Mali and Senegal, Two Sub-Saharan Countries: Insights and Optimizing Solutions. Vaccines, 8(2), 181. https://doi.org/10.3390/vaccines8020181