Strategies to Improve Coverage of Typhoid Conjugate Vaccine (TCV) Immunization Campaign in Karachi, Pakistan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
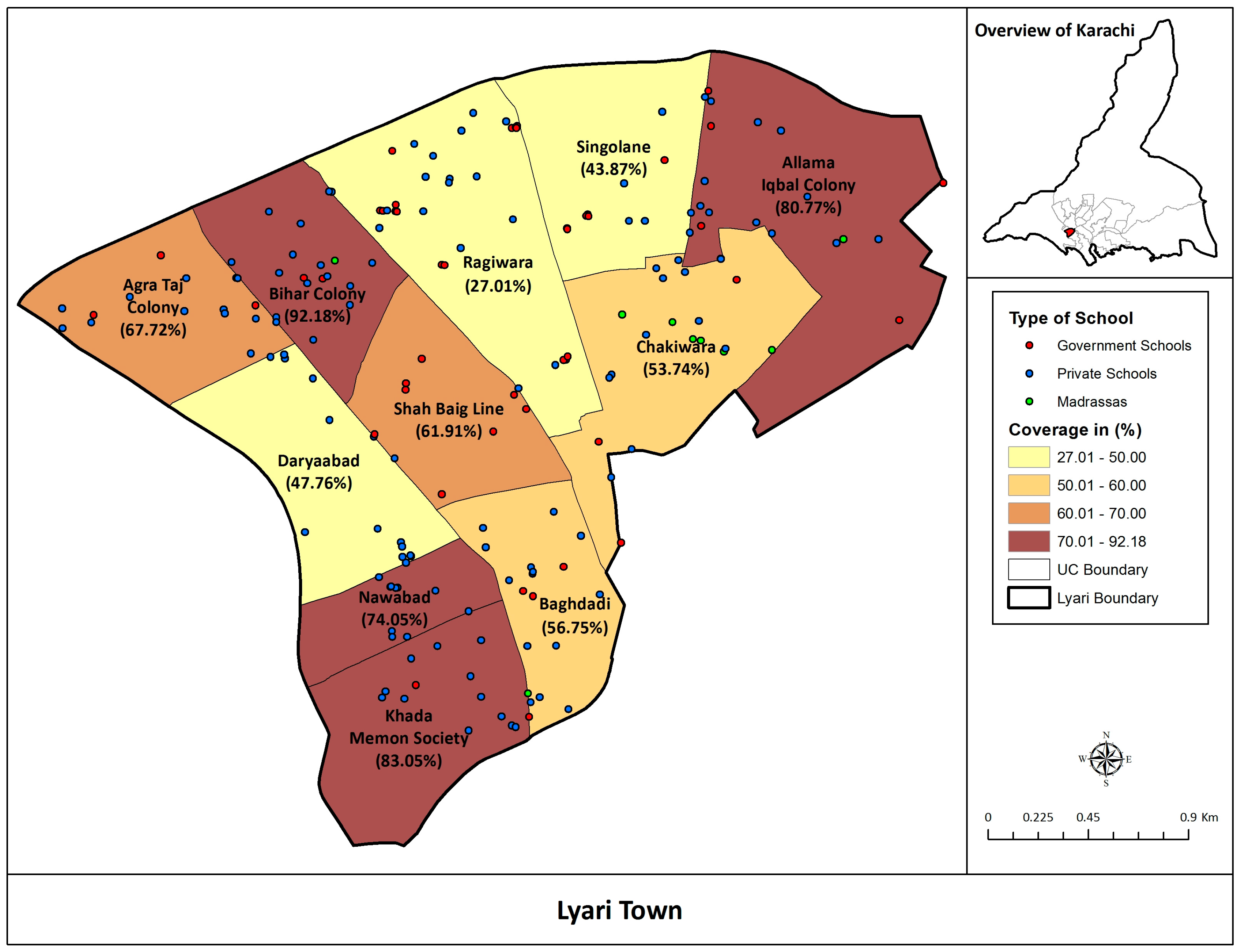
2.1. Setting
2.2. Planning of the Immunization Campaign
2.2.1. School-Based Campaign
2.2.2. Hospital-Based Campaign
2.2.3. Mobile Vaccination Campaign
3. Data Collection Methods
4. Ethical Approvals
5. Description of Strategies Found to be Effective in Improving Vaccination Coverage
5.1. Stakeholder Engagement
5.2. Vaccine Education Sessions in Schools and at Religious Institutions
5.3. Community Engagement and Social Media Campaign
5.4. Staff Trainings and Field Supervision
5.5. Healthcare Provider Education
6. Results
7. Discussion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harris, J.B.; Brooks, W.A. Typhoid and paratyphoid (enteric) fever. In Hunter’s Tropical Medicine and Emerging Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2020; pp. 608–616. [Google Scholar]
- Crump, J.A. Progress in typhoid fever epidemiology. Clin. Infect. Dis. 2019, 68, S4–S9. [Google Scholar] [CrossRef] [Green Version]
- Meiring, J.E.; Sambakunsi, R.; Moyo, E.; Misiri, T.; Mwakiseghile, F.; Patel, P.; Patel, P.; Ndaferankhande, J.; Laurens, M.B.; Gooding, K.; et al. Community Engagement before Initiation of Typhoid Conjugate Vaccine Trial in Schools in Two Urban Townships in Blantyre, Malawi: Experience and Lessons. Clin. Infect. Dis. 2019, 68, S146–S153. [Google Scholar] [CrossRef] [Green Version]
- Stanaway, J.D.; Reiner, R.C.; Blacker, B.F.; Goldberg, E.M.; Khalil, I.A.; Troeger, C.E.; Andrews, J.R.; Bhutta, Z.A.; Crump, J.A.; Im, J.; et al. The global burden of typhoid and paratyphoid fevers: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Infect. Dis. 2019, 19, 369–381. [Google Scholar] [CrossRef] [Green Version]
- Browne, A.J.; Hamadani, B.H.K.; Kumaran, E.A.P.; Rao, P.; Longbottom, J.; Harriss, E.; Moore, C.E.; Dunachie, S.; Basnyat, B.; Baker, S.; et al. Drug-resistant enteric fever worldwide, 1990 to 2018: A systematic review and meta-analysis. BMC Med. 2020, 18, 1. [Google Scholar] [CrossRef] [Green Version]
- Qamar, F.N.; Yousafzai, M.T.; Sultana, S.; Baig, A.; Shakoor, S.; Hirani, F.; Wassay, A.; Khushboo, S.; Mehmood, J.; Freeman, A.; et al. A retrospective study of laboratory-based enteric fever surveillance, Pakistan, 2012–2014. J. Infect. Dis. 2018, 218, S201–S205. [Google Scholar] [CrossRef]
- Klemm, E.J.; Shakoor, S.; Page, A.J.; Qamar, F.N.; Judge, K.; Saeed, D.K.; Wong, V.K.; Dallman, T.J.; Nair, S.; Baker, S.; et al. Emergence of an extensively drug-resistant Salmonella enterica serovar Typhi clone harboring a promiscuous plasmid encoding resistance to fluoroquinolones and third-generation cephalosporins. MBio 2018, 9, e00105-18. [Google Scholar] [CrossRef] [Green Version]
- Islamabad. Available online: https://www.nih.org.pk/wp-content/uploads/2019/07/FELTP-Pakistan-Weekly-Epidemiological-Report-June-17-23-2019.pdf (accessed on 23 May 2020).
- Khan, M.I.; Franco-Paredes, C.; Sahastrabuddhe, S.; Ochiai, R.L.; Mogasale, V.; Gessner, B.D. Barriers to typhoid fever vaccine access in endemic countries. Res. Rep. Trop. Med. 2017, 8, 37. [Google Scholar] [CrossRef] [Green Version]
- WHO. Weekly epidemiological record Relevé épidémiologique hebdomadaire; WHO: Geneva, Switzerland, 2008; Volume 83, pp. 373–384. [Google Scholar]
- Qamar, F.N.; Yousafzai, M.T.; Khaliq, A.; Karim, S.; Memon, H.; Junejo, A.; Baig, I.; Rahman, N.; Bhurgry, S.; Afroz, H.; et al. Adverse events following immunization with typhoid conjugate vaccine in an outbreak setting in Hyderabad, Pakistan. Vaccine 2020, 38, 3518–3523. [Google Scholar] [CrossRef]
- Shaikh, B.T.; Haq, Z.; Tran, N.; Hafeez, A. Health system barriers and levers in implementation of the Expanded Program on Immunization (EPI) in Pakistan: An evidence informed situation analysis. Public Health Rev. 2018, 39, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gurnani, V.; Haldar, P.; Aggarwal, M.K.; Das, M.K.; Chauhan, A.; Murray, J.; Arora, N.K.; Jhalani, M.; Sudan, P. Improving vaccination coverage in India: Lessons from Intensified Mission Indradhanush, a cross-sectoral systems strengthening strategy. BMJ 2018, 363, k4782. [Google Scholar] [CrossRef] [Green Version]
- Pugliese-Garcia, M.; Heyerdahl, L.W.; Mwamba, C.; Nkwemu, S.; Chilengi, R.; Demolis, R.; Guillermet, E.; Sharma, A. Factors influencing vaccine acceptance and hesitancy in three informal settlements in Lusaka, Zambia. Vaccine 2018, 36, 5617–5624. [Google Scholar] [CrossRef]
- Fournet, N.; Mollema, L.; Ruijs, W.L.; Harmsen, I.A.; Keck, F.; Durand, J.Y.; Cunha, M.P.; Wamsiedel, M.; Reis, R.; French, J.; et al. Under-vaccinated groups in Europe and their beliefs, attitudes and reasons for non-vaccination; two systematic reviews. BMC Public Health 2018, 18, 196. [Google Scholar] [CrossRef] [Green Version]
- Viqar, S. Constructing Lyari: Place, governance and identity in a Karachi neighbourhood. South Asian Hist. Cult. 2014, 5, 365–383. [Google Scholar] [CrossRef]
- Considered to be One of the Most Desperate Slum Areas in South Asia, Lyari Is also the Oldest Locality of Pakistan’s Sprawling, Unpredictable and Edgy Metropolis, Karachi. Available online: https://www.dawn.com/news/706128/the-good-the-bad-the-lyari (accessed on 28 March 2020).
- Baloch, N.; Rehman, M. Water Scarcity in Lyari Town-Real or Manmade: A Case Study. Available online: http://jisr.szabist.edu.pk/JISR-MSSE/Publication/2007/5/2/104/Article/070703Water.pdf (accessed on 16 June 2020).
- Mara, D.; Lane, J.; Scott, B.; Trouba, D. Sanitation and health. PLoS Med. 2010, 7, e1000363. [Google Scholar] [CrossRef] [Green Version]
- Ferdous, F.; Das, S.K.; Ahmed, S.; Farzana, F.D.; Malek, M.A.; Das, J.; Latham, J.R.; Faruque, A.S.G.; Chisti, M.J. Diarrhoea in slum children: Observation from a large diarrhoeal disease hospital in Dhaka, Bangladesh. Trop. Med. Int. Health 2014, 19, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- WHO. Safety of Mass Immunization Campaigns; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Berlier, M.; Barry, R.; Shadid, J.; Sirica, C.; Brunier, A.; Hasan, H.; Bouma, E. Communication challenges during the development and introduction of a new meningococcal vaccine in Africa. Clin. Infect. Dis. 2015, 61, S451–S458. [Google Scholar] [CrossRef] [Green Version]
- Jauregui, B.; Garcia, A.G.F.; Janusz, C.B.; Blau, J.; Munier, A.; Atherly, D.; Mvundura, M.; Hajjeh, R.; Lopman, B.; Clark, A.D.; et al. Evidence-based decision-making for vaccine introductions: Overview of the ProVac International Working Group’s experience. Vaccine 2015, 33, A28–A33. [Google Scholar] [CrossRef] [Green Version]
- Hardt, K.; Bonanni, P.; King, S.; Santospreciado, J.I.; El-Hodhod, M.; Zimet, G.D.; Preiss, S. Vaccine strategies: Optimising outcomes. Vaccine 2016, 34, 6691–6699. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.; Patel, P.; Meiring, J.E.; Misiri, T.; Mwakiseghile, F.; Gordon, M.A. On the Ground in Malawi-First Typhoid Conjugate Vaccine Study in Africa. Am. J. Trop. Med. Hyg. 2019, 100, 1299–1300. [Google Scholar] [CrossRef] [PubMed]
- Shikuku, D.N.; Muganda, M.; Amunga, S.O.; Obwanda, E.O.; Muga, A.; Matete, T.; Kisia, P. Door-to-door immunization strategy for improving access and utilization of immunization Services in Hard-to-Reach Areas: A case of Migori County, Kenya. BMC Public Health 2019, 19, 1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, E.; O’Reilly, M. A novel staff vaccination strategy. Infect. Control Hosp. Epidemiol. 2002, 23, 232–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccine Services. Available online: http://vaccineonwheels.com/hi_IN/ (accessed on 30 September 2020).
- Baggio, S.; Gétaz, L. Current Gaps in Vaccination Coverage: A Need to Improve Prevention and Care; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Anderson, E.L. Recommended solutions to the barriers to immunization in children and adults. Mo. Med. 2014, 111, 344. [Google Scholar] [PubMed]
- Mahase, E. Vaccination Uptake: Access Is Still Biggest Barrier, Experts Warn; BMJ Publishing Group: London, UK, 2019. [Google Scholar]
- Paterson, P.F.; Meurice, L.R.; Stanberry, S.; Glismann, S.L. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smailhodzic, E.; Hooijsma, W.; Boonstra, A.; Langley, D.J. Social media use in healthcare: A systematic review of effects on patients and on their relationship with healthcare professionals. BMC Health Serv. Res. 2016, 16, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.T.L.; Nakamura, K.; Seino, K. Association between a wider availability of health information and health care utilization in Vietnam: Cross-sectional study. J. Med. Internet Res. 2017, 19, e405. [Google Scholar] [CrossRef]
- Kolff, C.A.; Scott, V.P.; Stockwell, M.S. The use of technology to promote vaccination: A social ecological model based framework. Hum. Vaccines Immunother. 2018, 14, 1636–1646. [Google Scholar] [CrossRef] [Green Version]
- Kazi, A.; Murtaza, A.; Khoja, S.; Zaidi, A.; Ali, S. Monitoring polio supplementary immunization activities using an automated short text messaging system in Karachi, Pakistan. Bull. World Health Organ. 2013, 92, 220–225. [Google Scholar] [CrossRef]
- Morris, J.; Wang, W.; Wang, L.; Peddecord, K.M.; Sawyer, M.H. Comparison of reminder methods in selected adolescents with records in an immunization registry. J. Adolesc. Health 2015, 56, S27–S32. [Google Scholar] [CrossRef]
- Brown, V.B.; Oluwatosin, O.A. Feasibility of implementing a cellphone-based reminder/recall strategy to improve childhood routine immunization in a low-resource setting: A descriptive report. BMC Health Serv. Res. 2017, 17, 703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaglani, M.; Riggs, M.; Kamenicky, C.; Glezen, W.P. A computerized reminder strategy is effective for annual influenza immunization of children with asthma or reactive airway disease. Pediatr. Infect. Dis. J. 2001, 20, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Pelucchi, C.; Tel, F.; Chiarelli, G.; Sabatini, C.; Semino, M.; Marseglia, G.L.; De Mattia, D.; Principi, N. Factors conditioning effectiveness of a reminder/recall system to improve influenza vaccination in asthmatic children. Vaccine 2009, 27, 633–635. [Google Scholar] [CrossRef]
- Hofstetter, A.M.; Durivage, N.; Vargas, C.Y.; Camargo, S.; Vawdrey, D.K.; Fisher, A.; Stockwell, M.S. Text message reminders for timely routine MMR vaccination: A randomized controlled trial. Vaccine 2015, 33, 5741–5746. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Union Council | Number of Children Vaccinated in Government Schools | Number of Children Vaccinated in Private Schools | Number of Children Vaccinated in Madrassas | Total; n (%) |
|---|---|---|---|---|
| Agra Taj Colony | 1344 | 5505 | 6849 (15.2%) | |
| Allama Iqbal Colony | 821 | 2025 | 2846 (6.3%) | |
| Baghdadi | 1351 | 5036 | 6387 (14.2%) | |
| Bihar Colony | 1695 | 4147 | 139 | 5981 (13.3%) |
| Chakiwara | 1070 | 2388 | 861 | 4319 (9.6%) |
| Daryaabad | 252 | 1608 | 1860 (4.1%) | |
| Khada Memon Society | 678 | 4709 | 5387 (12.0%) | |
| Nawabad | 1078 | 4090 | 5168 (11.5%) | |
| Ragiwara | 1449 | 1012 | 2461 (5.5%) | |
| Shah Baig Line | 1048 | 372 | 84 | 1504 (3.3%) |
| Singolane | 1315 | 687 | 229 | 2232 (5.5%) |
| Total number of children vaccinated | 12,101 (26.9%) | 31,578 (70.2%) | 1314 (2.9%) | 44,993 (100%) |
| Vaccination Strategy | n (%) |
|---|---|
| Children vaccinated in school-based vaccination campaign | 39,939 (45.39%) |
| Children vaccinated in mop-up activity | 5054 (5.74%) |
| Children vaccinated in hospital-based vaccination campaigns | 16,042 (18.23%) |
| Children vaccinated in community based-vaccination campaigns | 26,958 (30.64%) |
| Total number of children vaccinated | 87,993 |
| Age Groups, Years | School-Based Vaccination Campaign; n (%) | Hospital-Based Vaccination Campaign; n (%) | Community Based-Vaccination Campaign; n (%) | Total; n (%) |
|---|---|---|---|---|
| <3 | 222 (0.5) | 3728 (23.2) | 4083 (15.1) | 8033 (9.1) |
| 3–6 | 5873 (13.1) | 4212 (26.3) | 6186 (22.9) | 16,271 (18.5) |
| 6–9 | 11,356 (25.2) | 3520 (21.9) | 6284 (23.3) | 21,160 (24.0) |
| 9–12 | 12,784 (28.4) | 2634 (16.4) | 5789 (21.5) | 21,207 (24.1) |
| 12–15 | 14,758 (32.8) | 1948 (12.1) | 4616 (17.1) | 21,322 (24.2) |
| Total | 44,993 | 16,042 | 26,958 | 87,993 |
| 1. Before implementation of any mass immunization program evaluate the strategies best suited for the local context. |
| 2. In the case of urban slum areas, pamphlets, handbills, banners and announcements alone are not enough, opportunities for open, direct communication with parents and children is important. |
| 3. Multiple permanent, temporary, and mobile vaccination posts enable widespread reach throughout the population. |
| 4. Continuous data analysis and periodical calculation of coverage in targeted areas and neighborhoods helps to identify pockets of low-coverage and prioritize further activities in targeted populations in a timely manner. |
| 5. The use of technology may assist not only in sharing messages for vaccination, but for real time data collection for timely action. |
| 6. Bringing all community stakeholders on board may help implement field operations in high-refusal areas. |
| 7. Microplanning should include social mapping of local influencers in the community. |
| 8. A strong AEFI management and referral plan should be in place as even a single SAE in a politically unstable setting can be disastrous for the entire campaign. |
| 9. Effective use of technology is the cheapest way to promote vaccination and enhance awareness. |
| 10. Community members should be asked for their assistance, suggestions, and feedback. |
| 11. Safety and security of field staff in the community should be assured. |
| 12. Discussions and engagement of physicians is mandatory to impart the correct messages to the community. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qamar, F.N.; Batool, R.; Qureshi, S.; Ali, M.; Sadaf, T.; Mehmood, J.; Iqbal, K.; Sultan, A.; Duff, N.; Yousafzai, M.T. Strategies to Improve Coverage of Typhoid Conjugate Vaccine (TCV) Immunization Campaign in Karachi, Pakistan. Vaccines 2020, 8, 697. https://doi.org/10.3390/vaccines8040697
Qamar FN, Batool R, Qureshi S, Ali M, Sadaf T, Mehmood J, Iqbal K, Sultan A, Duff N, Yousafzai MT. Strategies to Improve Coverage of Typhoid Conjugate Vaccine (TCV) Immunization Campaign in Karachi, Pakistan. Vaccines. 2020; 8(4):697. https://doi.org/10.3390/vaccines8040697
Chicago/Turabian StyleQamar, Farah Naz, Rabab Batool, Sonia Qureshi, Miqdad Ali, Tahira Sadaf, Junaid Mehmood, Khalid Iqbal, Akram Sultan, Noah Duff, and Mohammad Tahir Yousafzai. 2020. "Strategies to Improve Coverage of Typhoid Conjugate Vaccine (TCV) Immunization Campaign in Karachi, Pakistan" Vaccines 8, no. 4: 697. https://doi.org/10.3390/vaccines8040697
APA StyleQamar, F. N., Batool, R., Qureshi, S., Ali, M., Sadaf, T., Mehmood, J., Iqbal, K., Sultan, A., Duff, N., & Yousafzai, M. T. (2020). Strategies to Improve Coverage of Typhoid Conjugate Vaccine (TCV) Immunization Campaign in Karachi, Pakistan. Vaccines, 8(4), 697. https://doi.org/10.3390/vaccines8040697