
Comparison of SARS-CoV-2-Specific Antibodies in Human Milk after mRNA-Based COVID-19 Vaccination and Infection

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
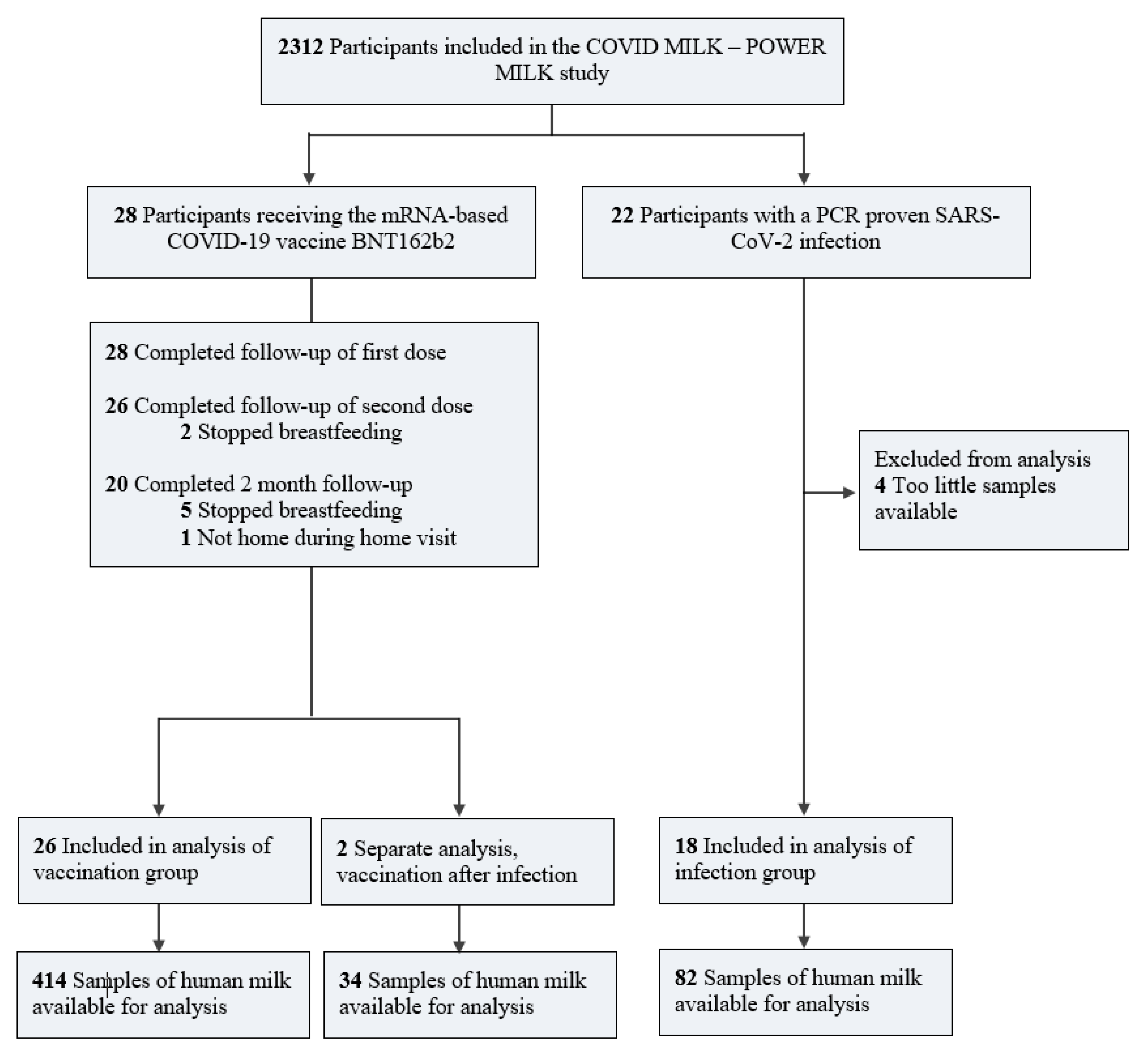
2.1. Study Design and Participants
2.2. Data Collection
2.3. Data Analysis
2.4. Statistical Methods
3. Results
3.1. Baseline Characteristics
3.2. Side Effects following Vaccination
3.3. COVID-19 Symptoms
3.4. Human Milk IgA Levels following Vaccination
3.5. Human Milk IgA Levels following SARS-CoV-2 Infection
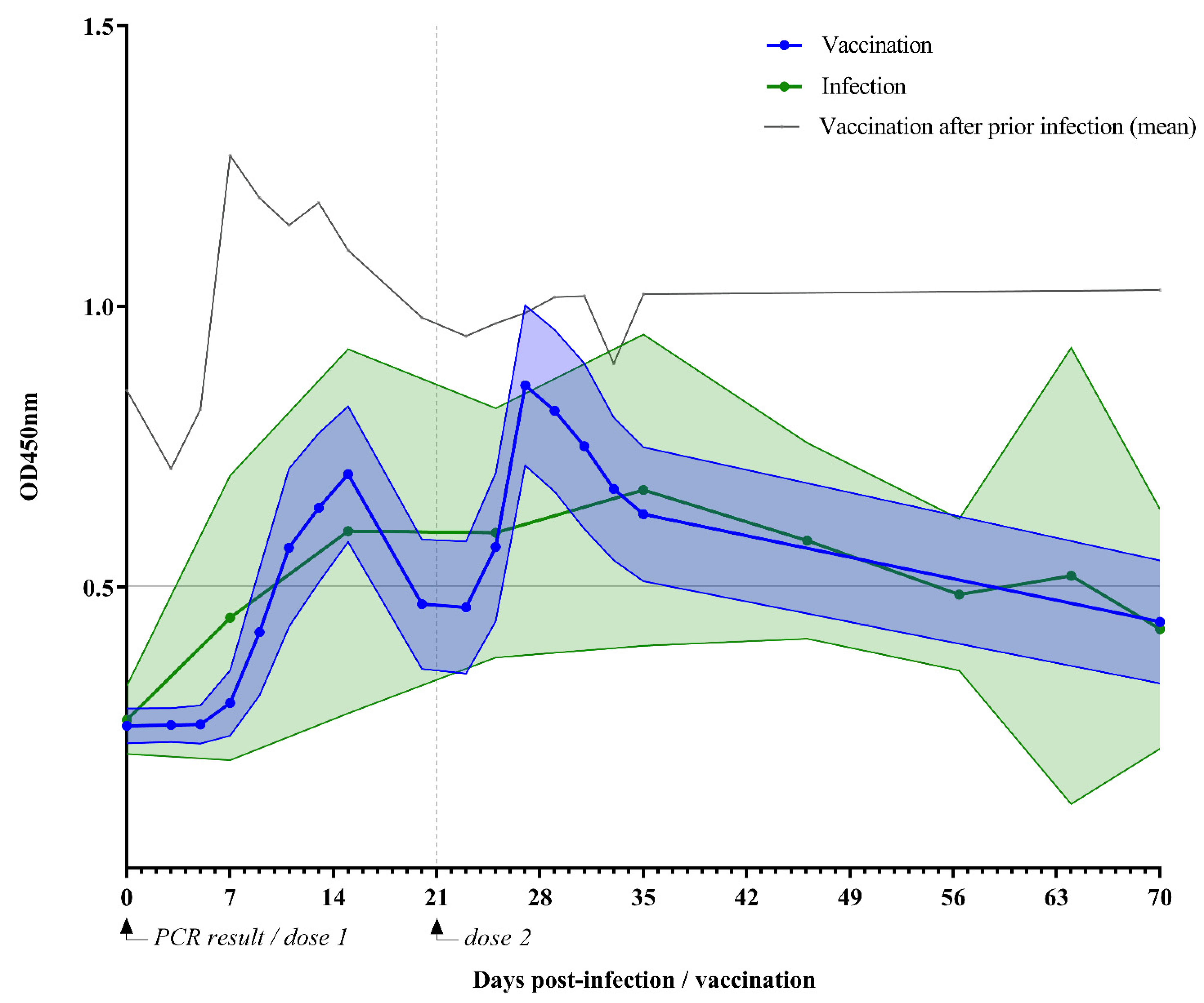
3.6. IgA Titers over Time: Vaccination Versus Infection
3.7. IgA Variability
3.8. Vaccination of Previously Infected Mothers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, X.; Tang, J.; Xie, R.; Li, W.; Chen, J.; Guo, Y.; Zhang, B.; Zhang, Y.; Wang, J.; Peng, C.; et al. Clinical and Epidemiological Features of 46 Children <1 Year Old With Coronavirus Disease 2019 in Wuhan, China: A Descriptive Study. J. Infect. Dis. 2020, 222, 1293–1297. [Google Scholar] [CrossRef] [PubMed]
- André, M.C.; Pätzug, K.; Bielicki, J.; Gualco, G.; Busi, I.; Hammer, J. Can SARS-CoV-2 cause life-threatening bronchiolitis in infants? Pediatric Pulmonol. 2020, 55, 2842–2843. [Google Scholar] [CrossRef] [PubMed]
- Grimaud, E.; Challiol, M.; Guilbaud, C.; Delestrain, C.; Madhi, F.; Ngo, J.; Epaud, R.; Nattes, E. Delayed acute bronchiolitis in infants hospitalized for COVID-19. Pediatric Pulmonol. 2020, 55, 2211–2212. [Google Scholar] [CrossRef] [PubMed]
- Mark, E.G.; Golden, W.C.; Gilmore, M.M.; Sick-Samuels, A.; Curless, M.S.; Nogee, L.M.; Milstone, A.M.; Johnson, J. Community-Onset Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Young Infants: A Systematic Review. J. Pediatr. 2021, 228, 94–100.e103. [Google Scholar] [CrossRef] [PubMed]
- Simon, A.K.; Hollander, G.A.; McMichael, A. Evolution of the immune system in humans from infancy to old age. Proc. Biol. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef]
- Kim, L.; Whitaker, M.; O’Halloran, A.; Kambhampati, A.; Chai, S.J.; Reingold, A.; Armistead, I.; Kawasaki, B.; Meek, J.; Yousey-Hindes, K.; et al. Hospitalization Rates and Characteristics of Children Aged <18 Years Hospitalized with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 1–July 25, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1081–1088. [Google Scholar] [CrossRef]
- Mosca, F.; Gianni, M.L. Human milk: Composition and health benefits. Pediatr. Med. E Chir. 2017, 39, 155. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Breastfeeding and COVID-19: Scientific Brief. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Breastfeeding-2020.1 (accessed on 23 June 2020).
- Brandtzaeg, P. The mucosal immune system and its integration with the mammary glands. J. Pediatr 2010, 156, S8–S15. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Viant, C.; Gaebler, C.; Cipolla, M.; Hoffmann, H.-H.; Oliveira, T.Y.; Oren, D.A.; et al. Enhanced SARS-CoV-2 neutralization by dimeric IgA. Sci. Transl. Med. 2021, 13, eabf1555. [Google Scholar] [CrossRef]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Medina Baez, A.; Shook, L.L.; Cvrk, D.; James, K.; et al. COVID-19 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, P303.e1–P303.e17. [Google Scholar] [CrossRef]
- Juncker, H.G.; Romijn, M.; Loth, V.N.; Ruhe, E.J.M.; Bakker, S.; Kleinendorst, S.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; et al. Antibodies Against SARS-CoV-2 in Human Milk: Milk Conversion Rates in the Netherlands. J. Hum. Lact. 2021, 37, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Sterlin, D.; Mathian, A.; Miyara, M.; Mohr, A.; Anna, F.; Claër, L.; Quentric, P.; Fadlallah, J.; Devilliers, H.; Ghillani, P.; et al. IgA dominates the early neutralizing antibody response to SARS-CoV-2. Sci. Transl. Med. 2021, 13. [Google Scholar] [CrossRef]
- Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. The Levels of SARS-CoV-2 Specific Antibodies in Human Milk Following Vaccination. J. Hum. Lact. 2021, 37, 477–484. [Google Scholar] [CrossRef]
- Lebrão, C.W.; Cruz, M.N.; Silva, M.H.d.; Dutra, L.V.; Cristiani, C.; Affonso Fonseca, F.L.; Suano-Souza, F.I. Early Identification of IgA Anti-SARSCoV-2 in Milk of Mother With COVID-19 Infection. J. Hum. Lact. 2020, 36, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Graphpad Software. Area under Dose-Response Data. Available online: https://www.graphpad.com/support/faqid/2031/ (accessed on 18 June 2021).
- Wang, Z.; Schmidt, F.; Weisblum, Y.; Muecksch, F.; Barnes, C.O.; Finkin, S.; Schaefer-Babajew, D.; Cipolla, M.; Gaebler, C.; Lieberman, J.A.; et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nature 2021, 592, 616–622. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2–Specific Antibodies in Breast Milk After COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.; Marino, J.; Amanat, F.; Krammer, F.; Hahn-Holbrook, J.; Zolla-Pazner, S.; Powell, R.L. Evidence of a significant secretory-IgA-dominant SARS-CoV-2 immune response in human milk following recovery from COVID-19. iScience 2020, 23, 101735. [Google Scholar] [CrossRef]
- Van Keulen, B.J.; Romijn, M.; Bondt, A.; Dingess, K.A.; Kontopodi, E.; van der Straten, K.; den Boer, M.A.; Burger, J.A.; Poniman, M.; Bosch, B.J.; et al. Human Milk from Previously COVID-19-Infected Mothers: The Effect of Pasteurization on Specific Antibodies and Neutralization Capacity. Nutrients 2021, 13, 1645. [Google Scholar] [CrossRef]
- Collier, A.-r.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Apraku Bondzie, E.; Sellers, D.; et al. Immunogenicity of COVID-19 mRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370–2380. [Google Scholar] [CrossRef]
- Low, J.M.; Gu, Y.; Ng, M.S.F.; Amin, Z.; Lee, L.Y.; Ng, Y.P.M.; Shunmuganathan, B.D.O.; Niu, Y.; Gupta, R.; Tambyah, P.A.; et al. Codominant IgG and IgA expression with minimal vaccine mRNA in milk of BNT162b2 vaccinees. npj Vaccines 2021, 6, 105. [Google Scholar] [CrossRef] [PubMed]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, Á.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021, 397, 1057–1058. [Google Scholar] [CrossRef]
- Van Gils, M.J.; van Willigen, H.D.; Wynberg, E.; Han, A.X.; van der Straten, K.; Verveen, A.; Lebbink, R.; Dijkstra, M.; Burger, J.A.; Oomen, M.; et al. Single-Dose SARS-Cov-2 Vaccine in A Prospective Cohort Of COVID-19 Patients. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.05.25.21257797v1.full-text (accessed on 1 November 2021).
- Appelman, B.; van der Straten, K.; Lavell, A.H.A.; Schinkel, M.; Slim, M.A.; Poniman, M.; Burger, J.A.; Oomen, M.; Tejjani, K.; Vlaar, A.P.J.; et al. Time since SARS-CoV-2 infection and humoral immune response following BNT162b2 mRNA vaccination. EBioMedicine 2021, 72, 103589. [Google Scholar] [CrossRef] [PubMed]
- Sui, Z.; Dai, X.; Lu, Q.; Zhang, Y.; Huang, M.; Li, S.; Peng, T.; Xie, J.; Zhang, Y.; Wu, C.; et al. Viral dynamics and antibody responses in people with asymptomatic SARS-CoV-2 infection. Signal. Transduct. Target. Ther. 2021, 6, 181. [Google Scholar] [CrossRef]
- Lou, B.; Li, T.-D.; Zheng, S.-F.; Su, Y.-Y.; Li, Z.-Y.; Liu, W.; Yu, F.; Ge, S.-X.; Zou, Q.-D.; Yuan, Q.; et al. Serology characteristics of SARS-CoV-2 infection after exposure and post-symptom onset. Eur. Respir. J. 2020, 56, 2000763. [Google Scholar] [CrossRef]
- Schlaudecker, E.P.; Steinhoff, M.C.; Omer, S.B.; McNeal, M.M.; Roy, E.; Arifeen, S.E.; Dodd, C.N.; Raqib, R.; Breiman, R.F.; Zaman, K. IgA and Neutralizing Antibodies to Influenza A Virus in Human Milk: A Randomized Trial of Antenatal Influenza Immunization. PLoS ONE 2013, 8, e70867. [Google Scholar] [CrossRef]
- Lamberti, L.M.; Zakarija-Grković, I.; Fischer Walker, C.L.; Theodoratou, E.; Nair, H.; Campbell, H.; Black, R.E. Breastfeeding for reducing the risk of pneumonia morbidity and mortality in children under two: A systematic literature review and meta-analysis. BMC Public Health 2013, 13, 1786–1792. [Google Scholar] [CrossRef] [Green Version]
- Chambers, C.; Krogstad, P.; Bertrand, K.; Contreras, D.; Tobin, N.H.; Bode, L.; Aldrovandi, G. Evaluation for SARS-CoV-2 in Breast Milk From 18 Infected Women. JAMA 2020, 324, 1347–1348. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| BNT162b2 Vaccination | SARS-CoV-2 Infection | ||
|---|---|---|---|
| No Milk Conversion (n = 26) | Milk Conversion (n = 2) 1 | (n = 18) | |
| Maternal features | |||
| Age, median (IQR), y | 33.5 (30.8–35) | 35.5 | 31 (28.5–36.5) |
| BMI, median (IQR), kg/m2 | 24.0 (21.0–26.6) | 25.8 | 25.8 (21.6–25.2) |
| Chronic disease, No. (%) | 3 (11.5) 2 | 0 (0) | 0 (0) |
| Parity primiparous, No. (%) | 12 (46.2) | 1 (50) | 9 (50) |
| Age postpartum, median (IQR), months | 7.0 (4.8–9.0) | 9 | 6.0 (4.5–8.5) |
| Delivery mode (vaginal), No. (%) | 19 (73.1) | 1 (50) | 12 (66.7) |
| Lactational stage, No. (%) | |||
| <6 months | 8 (30.8) | 1 (50) | 5 (27.8) |
| 6–12 months | 16 (61.5) | - | 11 (61.1) |
| >12 months | 2 (7.7) | 1 (50) | 2 (11.1) |
| Vaccination history, No. (%) | |||
| Child-immunization 3 | 26 (100) | 2 (100) | 16 (88.9) |
| Whooping cough vaccine during pregnancy | 25 (96.2) | 2 (100) | 15 (83.3) |
| Other | 14 (53.8) 4 | 1 (50) | 12 (66.7) 4 |
| Race/ethnicity, No. (%) | |||
| Europe | 25 (96.2) | 2 (100) | 14 (77.8) |
| Oceania | 1 (3.8) | - | 2 (11.1) |
| Africa | - | - | 1 (5.6) |
| South America | - | - | 1 (5.6) |
| Infant features | |||
| Birthweight, median (range), grams | 3388 (3126–3710) | 3495 | 3475 (3278–3848) |
| Gestational age, mean (SD), weeks | 39.1 (1.7) | 41 | 39.9 (1.5) |
| Sex of infant (female), No. (%) | 16 (61.5) | 1 (50) | 7 (38.9) |
| Exclusive breastfeeding, No. (%) | 12 (46.2) | 1 (50) | 7 (38.9) |
| Side Effects 1 | No. (%) |
|---|---|
| After first dose | |
| Local pain/swelling | 6 (28.6) |
| Muscle aches | 5 (23.8) |
| Headache | 4 (19) |
| Fever | 1 (4.8) |
| Fatigue | 2 (9.5) |
| Other | 2 (9.5) 2 |
| After second dose | |
| Fatigue | 7 (33.3) |
| Local pain/swelling | 6 (28.6) |
| Fever | 5 (23.8) |
| Headache | 5 (23.8) |
| Muscle aches | 4 (19) |
| Other | 9 (42.9) 3 |
| No side effects at both doses | 1 (3.6) |
| Symptoms | No. (%) 1 |
|---|---|
| Headache | 12 (75) |
| Fatigue | 12 (75) |
| Sudden loss of smell and/or taste | 10 (62.5) |
| Cold symptoms | 9 (56.3) |
| Sore throat | 8 (50) |
| Fever | 6 (37.5) |
| Dry cough | 6 (37.5) |
| Photophobic | 2 (12.5) |
| Abdominal pain | 1 (6.3) |
| Nausea/vomiting | 1 (6.3) |
| Loss of appetite | 1 (6.3) |
| Hospital admission 2 | 1 (6.3) |
| Asymptomatic | 1 (6.3) |
| 70 Days | Vaccination, Uninfected | Vaccination, Previously Infected | SARS-CoV-2 Infection, Unvaccinated |
|---|---|---|---|
| df | 397 | 17 | 73 |
| AUCG | 37.6 ± 6.4 a | 71.1 ± 8.3 b | 38.2 ± 5.6 a |
| AUCcutoff | 7.5 ± 3.8 a | 36 ± 8.3 b | 5.7 ± 4.9 a |
| AUCI | 19.8 ± 6.4 a | 12.3 ± 8.3 a | 19.7 ± 5.6 a |
| One month | |||
| df | 380 | 16 | 44 |
| AUCG | 18.9 ± 1.8 a | 35.2 ± 1.1 b | 19 ± 4.3 a |
| AUCcutoff | 5.6 ± 1.6 a | 17.7 ± 1.1 b | 3.7 ± 4 a |
| AUCI | 10 ± 1.8 a | 6.2 ± 1 a | 9.8 ± 4.3 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; Bijl, T.P.L.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. Comparison of SARS-CoV-2-Specific Antibodies in Human Milk after mRNA-Based COVID-19 Vaccination and Infection. Vaccines 2021, 9, 1475. https://doi.org/10.3390/vaccines9121475
Juncker HG, Mulleners SJ, van Gils MJ, Bijl TPL, de Groot CJM, Pajkrt D, Korosi A, van Goudoever JB, van Keulen BJ. Comparison of SARS-CoV-2-Specific Antibodies in Human Milk after mRNA-Based COVID-19 Vaccination and Infection. Vaccines. 2021; 9(12):1475. https://doi.org/10.3390/vaccines9121475
Chicago/Turabian StyleJuncker, Hannah G., Sien J. Mulleners, Marit J. van Gils, Tom P. L. Bijl, Christianne J. M. de Groot, Dasja Pajkrt, Aniko Korosi, Johannes B. van Goudoever, and Britt J. van Keulen. 2021. "Comparison of SARS-CoV-2-Specific Antibodies in Human Milk after mRNA-Based COVID-19 Vaccination and Infection" Vaccines 9, no. 12: 1475. https://doi.org/10.3390/vaccines9121475
APA StyleJuncker, H. G., Mulleners, S. J., van Gils, M. J., Bijl, T. P. L., de Groot, C. J. M., Pajkrt, D., Korosi, A., van Goudoever, J. B., & van Keulen, B. J. (2021). Comparison of SARS-CoV-2-Specific Antibodies in Human Milk after mRNA-Based COVID-19 Vaccination and Infection. Vaccines, 9(12), 1475. https://doi.org/10.3390/vaccines9121475