
Pneumococcal and Influenza Vaccination Rates and Pneumococcal Invasive Disease Rates Set Geographical and Ethnic Population Susceptibility to Serious COVID-19 Cases and Deaths


Abstract
:
1. Introduction
1.1. Coinfections in Severe COVID-19
1.2. Non-SARS-CoV-2 Vaccinations and COVID-19 Risk
1.3. Purpose of The Current Study
2. Methods
2.1. International Data
2.2. Italian Regional Data
2.3. U.S. Data
2.4. Statistics
3. Results
3.1. Data Sets
3.2. Correlations between National Vaccination Rates and COVID-19 Case and Death Rates
3.3. Do Combinations of Vaccines Protect against COVID-19?
3.4. Controlling for Possible Confounding of Vaccine Effects
3.5. Pneumococcal Invasive Disease and Lower Respiratory Infections as Possible Risks for COVID-19
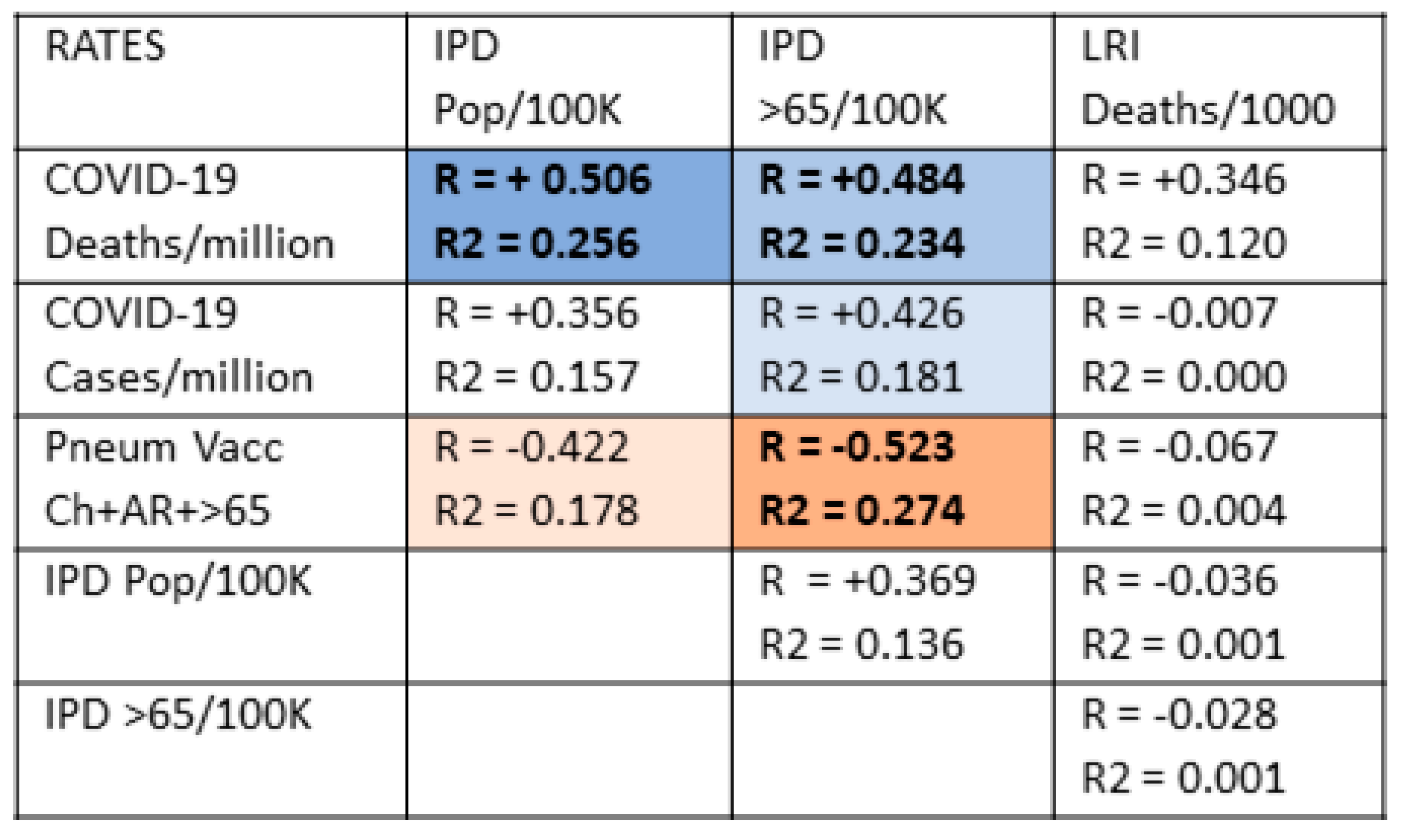
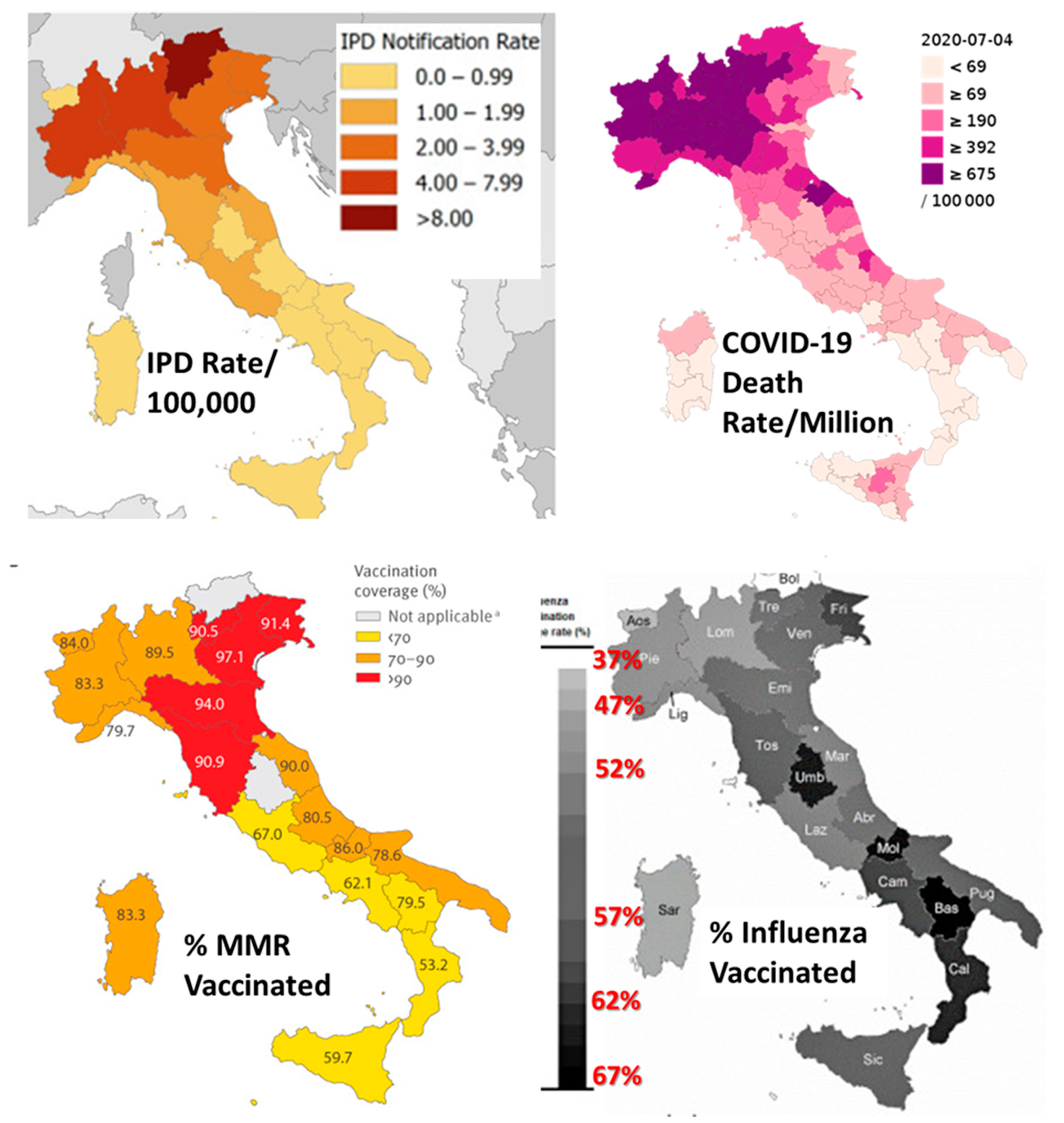
3.6. Testing the Hypothesis in the Regions of Italy
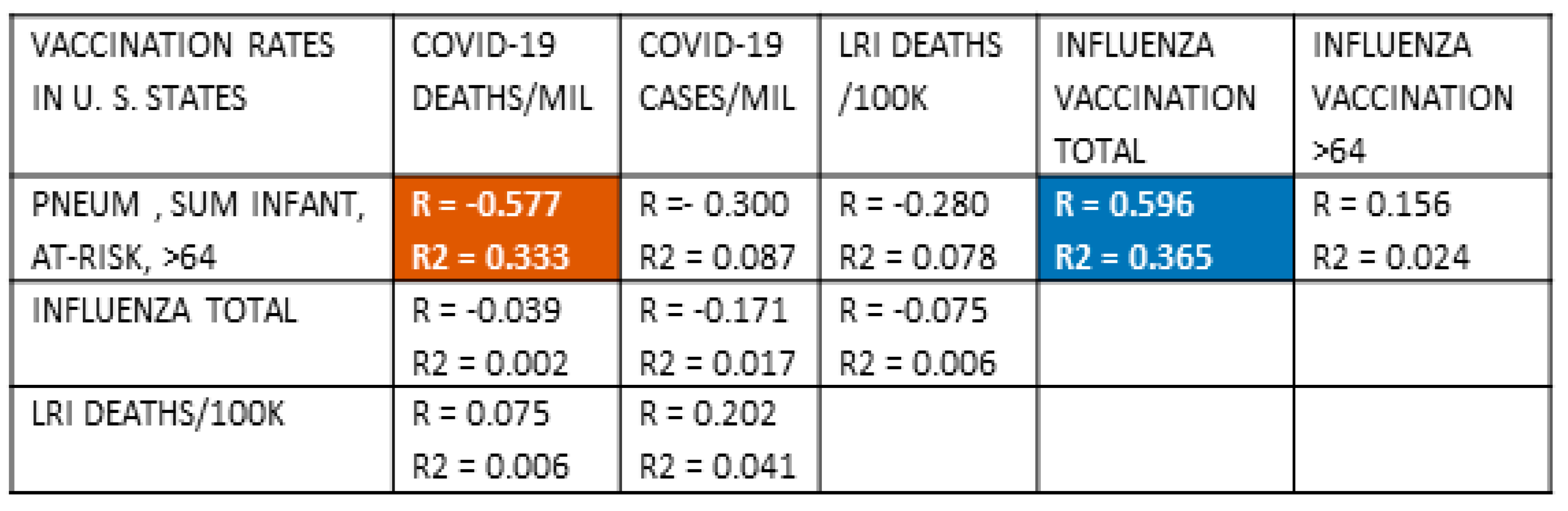
3.7. Testing the Hypothesis in the United States
4. Discussion
Limitations of This Study
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ng, O.T.; Marimuthu, K.; Koh, V.; Pang, J.; Linn, K.Z.; Sun, J.; Wang, L.D.; Chia, W.N.; Tiu, C.; Cham, M.; et al. SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: A retrospective cohort study. Lancet Infect. Dis. 2020, 21, 333–343. [Google Scholar] [CrossRef]
- King, J.A.; Whitten, T.A.; Bakal, J.A.; McAlister, F.A. Symptoms associated with a positive result for a swab for SARS-CoV-2 infection among children in Alberta. Can. Med Assoc. J. 2021, 193, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mudd, P.A.; Crawford, J.C.; Turner, J.S.; Souquette, A.; Reynolds, D.; Bender, D.; Bosanquet, J.P.; Anand, N.J.; Striker, D.A.; Martin, R.S.; et al. Distinct inflammatory profiles distinguish COVID-19 from influenza with limited contributions from cytokine storm. Sci. Adv. 2020, 6, eabe3024. [Google Scholar] [CrossRef]
- Worldometer. COVID-19. Available online: https://www.worldometers.info/coronavirus/coronavirus-cases/#daily-cases (accessed on 30 April 2021).
- Root-Bernstein, R. Age and Location in Severity of COVID-19 Pathology: Do Lactoferrin and Pneumococcal Vaccination Explain Low Infant Mortality and Regional Differences? BioEssays 2020, 42. [Google Scholar] [CrossRef]
- Root-Bernstein, R. Possible Cross-Reactivity between SARS-CoV-2 Proteins, CRM197 and Proteins in Pneumococcal Vaccines May Protect Against Symptomatic SARS-CoV-2 Disease and Death. Vaccines 2020, 8, 559. [Google Scholar] [CrossRef] [PubMed]
- Herrera, A.L.; Huber, V.C.; Chaussee, M.S. The Association between Invasive Group A Streptococcal Diseases and Viral Respiratory Tract Infections. Front. Microbiol. 2016, 7, 342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Root-Bernstein, R.S.; Podufaly, A.; Aimone, F. Antigenic complementarity between influenza a virus and Haemophilus influenzae may drive lethal co-infection such as that seen in 1918-19. J. Virol. Antivir. Res. 2013, 2, 1. [Google Scholar] [CrossRef]
- Morens, D.M.; Taubenberger, J.K.; Fauci, A.S. Predominant role of bacterial pneumonia as a cause of death in pan-demic influenza: Implications for pandemic influenza preparedness. J. Infect. Dis. 2008, 198, 962. [Google Scholar] [CrossRef] [PubMed]
- Brundage, J.F. Interactions between influenza and bacterial respiratory pathogens: Implications for pandemic preparedness. Lancet 2006, 6, 303–312. [Google Scholar] [CrossRef]
- Brundage, J.F.; Shanks, D.G. Deaths from bacterial pneumonia in the 1918–1919 influenza pandemic. Emerg. Infect. Dis. 2008, 14, 1193–1199. [Google Scholar] [CrossRef]
- Chen, X.; Liao, B.; Cheng, L.; Peng, X.; Xu, X.; Li, Y.; Hu, T.; Li, J.; Zhou, X.; Ren, B. The microbial coinfection in COVID-19. Appl. Microbiol. Biotechnol. 2020, 104, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Miellet, W.R.; Van Veldhuizen, J.; Nicolaie, A.M.; Mariman, R.; Bootsma, H.J.; Bosch, T.; Rots, N.Y.; Sanders, E.A.M.; Van Beek, J.; Trzciński, K. Influenza-like Illness Exacerbates Pneumococcal Carriage in Older Adults. Clin. Infect. Dis. 2020, 30. [Google Scholar] [CrossRef]
- Intra, J.; Sarto, C.; Beck, E.; Tiberti, N.; Leoni, V.; Brambilla, P. Bacterial and fungal colonization of the respiratory tract in COVID-19 patients should not be neglected. Am. J. Infect. Control. 2020, 48, 1130–1131. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influ. Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; Wang, C.-Y.; Hsueh, P.-R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef]
- Lv, Z.; Cheng, S.; Le, J.; Huang, J.; Feng, L.; Zhang, B.; Li, Y. Clinical characteristics and co-infections of 354 hospitalized patients with COVID-19 in Wuhan, China: A retrospective cohort study. Microbes Infect. 2020, 22, 195–199. [Google Scholar] [CrossRef]
- Cucchiari, D.; Pericàs, J.M.; Riera, J.; Gumucio, R.; Coloma, E.; Nicolás, D. Pneumococcal superinfection in COVID-19 patients: A series of 5 cases. Med. Clínica 2020, 155, 502–505. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Flandre, P.L.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensiv. Care 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Zhu, F.; Zhu, B.; Cui, L. Co-infection with respiratory pathogens among COVID-2019 cases. Virus Res. 2020, 285, 198005. [Google Scholar] [CrossRef]
- Zhou, H.; Li, C.; Hu, T.; Liu, T.; Ni, N.; Chen, W.; Zhao, H.; Ruan, S.; Li, J.; Wu, H.; et al. Total infectomes of 162 SARS-CoV-2 cases using meta-transcriptomic sequencing. J. Infect. 2021, 82, e44–e48. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Hu, C.; Luo, L.; Fang, F.; Chen, Y.; Li, J.; Peng, Z.; Pan, H. Clinical features and short-term outcomes of 221 patients with COVID-19 in Wuhan, China. J. Clin. Virol. 2020, 127, 104364. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Ling, Y.; Bai, T.; Xie, Y.; Huang, J.; Li, J.; Xiong, W.; Yang, D.; Chen, R.; Lu, F.; et al. COVID-19 with Different Severities: A Multicenter Study of Clinical Features. Am. J. Respir. Crit. Care Med. 2020, 201, 1380–1388. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Townsend, L.; Hughes, G.; Kerr, C.; Kelly, M.; O’Connor, R.; Sweeney, E.; Doyle, C.; O’Riordan, R.; Martin-Loeches, I.; Bergin, C.; et al. Bacterial pneumonia coinfection and antimicrobial therapy duration in SARS-CoV-2 (COVID-19) infection. JAC Antimicrob. Resist. 2020, 2. [Google Scholar] [CrossRef] [PubMed]
- Rothe, K.; Feihl, S.; Schneider, J.; Wallnöfer, F.; Wurst, M.; Lukas, M.; Treiber, M.; Lahmer, T.; Heim, M.; Dommasch, M.; et al. Rates of bacterial co-infections and antimicrobial use in COVID-19 patients: A retrospective cohort study in light of antibiotic stewardship. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef]
- Ma, L.; Wang, W.; Le Grange, J.M.; Wang, X.; Du, S.; Li, C.; Wei, J.; Zhang, J.-N. Coinfection of SARS-CoV-2 and Other Respiratory Pathogens. Infect. Drug Resist. 2020, 13, 3045–3053. [Google Scholar] [CrossRef]
- Vaillancourt, M.; Jorth, P. The Unrecognized Threat of Secondary Bacterial Infections with COVID-19. mBio 2020, 11. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals With Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Bengoechea, J.A.; Bamford, C.G. SARS-CoV-2, bacterial co-infections, and AMR: The deadly trio in COVID-19? EMBO Mol. Med. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Huttner, B.; Catho, G.; Pano-Pardo, J.; Pulcini, C.; Schouten, J. COVID-19: Don’t neglect antimicrobial stewardship principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef] [PubMed]
- Ozaras, R.; Cirpin, R.; Duran, A.; Duman, H.; Arslan, O.; Bakcan, Y.; Kaya, M.; Mutlu, H.; Isayeva, L.; Kebanlı, F.; et al. Influenza and COVID-19 coinfection: Report of six cases and review of the literature. J. Med. Virol. 2020, 92, 2657–2665. [Google Scholar] [CrossRef]
- Ding, Q.; Lu, P.; Fan, Y.; Xia, Y.; Liu, M. The clinical characteristics of pneumonia patients coinfected with 2019 novel coronavirus and influenza virus in Wuhan, China. J. Med. Virol. 2020, 92, 1549–1555. [Google Scholar] [CrossRef]
- Hashemi, S.A.; Safamanesh, S.; Ghafouri, M.; Taghavi, M.R.; Heydari, M.S.M.Z.; Abad, H.N.A.; Zadeh-Moghaddam, H.G.; Azimian, A. Co-infection with COVID-19 and influenza A virus in two died patients with acute respiratory syndrome, Bojnurd, Iran. J. Med. Virol. 2020, 92. [Google Scholar] [CrossRef]
- Ma, S.; Lai, X.; Chen, Z.; Tu, S.; Qin, K. Clinical characteristics of critically ill patients co-infected with SARS-CoV-2 and the influenza virus in Wuhan. China. Int. J. Infect. Dis. 2020, 96, 683–687. [Google Scholar] [CrossRef]
- Cuadrado-Payán, E.; Montagud-Marrahi, E.; Torres-Elorza, M.; Bodro, M.; Blasco, M.; Poch, E.; Soriano, A.; Piñeiro, G.J. SARS-CoV-2 and influenza virus co-infection. Lancet 2020, 395, e84. [Google Scholar] [CrossRef]
- Thindwa, D.; Quesada, M.G.; Liu, Y.; Bennett, J.; Cohen, C.; Knoll, M.D.; von Gottberg, A.; Hayford, K.; Flasche, S. Use of seasonal influenza and pneumococcal polysaccharide vaccines in older adults to reduce COVID-19 mortality. Vaccine 2020, 38, 5398–5401. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.C.; Cutland, C.L.; Klugman, K.P.; Madhi, S.A. Pneumococcal Conjugate Vaccine Protection against Coronavirus-Associated Pneumonia Hospitalization in Children Living with and without HIV. mBio 2021, 12. [Google Scholar] [CrossRef]
- Jehi, L.; Ji, X.; Milinovich, A.; Erzurum, S.; Rubin, B.P.; Gordon, S.; Young, J.B.; Kattan, M.W. Individualizing Risk Prediction for Positive Coronavirus Disease 2019 Testing. Chest 2020, 158, 1364–1375. [Google Scholar] [CrossRef] [PubMed]
- Pawlowski, C.; Puranik, A.; Bandi, H.; Venkatakrishnan, A.J.; Agarwal, V.; Kennedy, R.; O’Horo, J.C.; Gores, G.J.; Williams, A.W.; Halamka, J.; et al. Exploratory analysis of immunization records highlights decreased SARS-CoV-2 rates in individuals with recent non-COVID-19 vaccinations. Sci. Rep. 2021, 11, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Noale, M.; Trevisan, C.; Maggi, S.; Incalzi, R.A.; Pedone, C.; Di Bari, M.; Adorni, F.; Jesuthasan, N.; Sojic, A.; Galli, M.; et al. The Association between Influenza and Pneumococcal Vaccinations and SARS-Cov-2 Infection: Data from the EPICOVID19 Web-Based Survey. Vaccines 2020, 8, 471. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, A.J.; Bruxvoort, K.J.; Fischer, H.; Hong, V.X.; Grant, L.R.; Jódar, L.; Gessner, B.D.; Tartof, S.Y. Prevention of COVID-19 among older adults receiving pneumococcal conjugate vaccine suggests interactions between Streptococcus pneumoniae and SARS-CoV-2 in the respiratory tract. J. Infect. Dis. 2021, 128. [Google Scholar] [CrossRef]
- Sumbul, B.; Sumbul, H.E.; Okyay, R.A.; Gülümsek, E.; Şahin, A.R.; Boral, B.; Koçyiğit, B.F.; Alfishawy, M.; Gold, J.; Tasdogan, A.M. Is there a link between pre-existing antibodies acquired due to childhood vaccinations or past infections and COVID-19? A case control study. PeerJ 2021, 9, e10910. [Google Scholar] [CrossRef]
- Fink, G.; Orlova-Fink, N.; Schindler, T.; Grisi, S.; Ferrer, A.P.S.; Daubenberger, C.; Brentani, A. Inactivated trivalent influenza vaccination is associated with lower mortality among patients with COVID-19 in Brazil. BMJ Evid. Based Med. 2020. [Google Scholar] [CrossRef]
- Amato, M.; Werba, J.P.; Frigerio, B.; Coggi, D.; Sansaro, D.; Ravani, A.; Ferrante, P.; Veglia, F.; Tremoli, E.; Baldassarre, D. Relationship between Influenza Vaccination Coverage Rate and COVID-19 Outbreak: An Italian Ecological Study. Vaccines 2020, 8, 535. [Google Scholar] [CrossRef]
- Cocco, P.; Meloni, F.; Coratza, A.; Schirru, D.; Campagna, M.; De Matteis, S. Vaccination against seasonal influenza and socio-economic and environmental factors as determinants of the geographic variation of COVID-19 incidence and mortality in the Italian elderly. Prev. Med. 2021, 143, 106351. [Google Scholar] [CrossRef]
- Arokiaraj, M.C. Considering Interim Interventions to Control COVID-19 Associated Morbidity and Mortality—Perspectives. Front. Public Health 2020, 8. [Google Scholar] [CrossRef]
- Zanettini, C.; Omar, M.; Dinalankara, W.; Imada, E.L.; Colantuoni, E.; Parmigiani, G.; Marchionni, L. Influenza vac-cination and COVID19 mortality in the USA. medRxiv 2020. [Google Scholar] [CrossRef]
- Del Riccio, M.; Lorini, C.; Bonaccorsi, G.; Paget, J.; Caini, S. The Association between Influenza Vaccination and the Risk of SARS-CoV-2 Infection, Severe Illness, and Death: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2020, 17, 7870. [Google Scholar] [CrossRef]
- Marín-Hernández, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID-19 deaths in Italy. J. Med Virol. 2021, 93, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.E.; Baumgartl, W.H.; Okyay, R.A.; Licht, W.E.; Fidel, P.L.; Noverr, M.C.; Tilley, L.P.; Hurley, D.J.; Rada, B.; Ashford, J.W. Analysis of Measles-Mumps-Rubella (MMR) Titers of Recovered COVID-19 Patients. mBio 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Ashford, J.W.; Gold, J.E.; Huenergardt, M.A.; Katz, R.B.; Strand, S.E.; Bolanos, J.; Wheeler, C.J.; Perry, G.; Smith, C.J.; Steinman, L.; et al. MMR Vaccination: A Potential Strategy to Reduce Severity and Mortality of COVID-19 Illness. Am. J. Med. 2021, 134, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Fidel, P.L.; Noverr, M.C. Could an Unrelated Live Attenuated Vaccine Serve as a Preventive Measure To Dampen Septic Inflammation Associated with COVID-19 Infection? mBio 2020, 11. [Google Scholar] [CrossRef]
- Ogimi, C.; Qu, P.; Boeckh, M.; Ignacio, R.A.B.; Zangeneh, S.Z. Association between live childhood vaccines and COVID-19 outcomes: A national-level analysis. Epidemiol. Infect. 2021, 149, 1–15. [Google Scholar] [CrossRef]
- Klinger, D.; Blass, I.; Rappoport, N.; Linial, M. Significantly Improved COVID-19 Outcomes in Countries with Higher BCG Vaccination Coverage: A Multivariable Analysis. Vaccines 2020, 8, 378. [Google Scholar] [CrossRef]
- Martínez-Baz, I.; Trobajo-Sanmartín, C.; Arregui, I.; Navascués, A.; Adelantado, M.; Indurain, J.; Fresán, U.; Ezpeleta, C.; Castilla, J. Influenza Vaccination and Risk of SARS-CoV-2 Infection in a Cohort of Health Workers. Vaccines 2020, 8, 611. [Google Scholar] [CrossRef]
- Belingheri, M.; Paladino, E.M.; Latocca, R.; De Vito, G.; Riva, A.M. Association between seasonal flu vaccination and COVID-19 among healthcare workers. Occup. Med. 2020, 70, 665–671. [Google Scholar] [CrossRef]
- Ragni, P.; Marino, M.; Formisano, D.; Bisaccia, E.; Scaltriti, S.; Bedeschi, E.; Grilli, R. Association between Exposure to Influenza Vaccination and COVID-19 Diagnosis and Outcomes. Vaccines 2020, 8, 675. [Google Scholar] [CrossRef]
- Massoudi, N.; Mohit, B. A Case–Control Study of the 2019 Influenza Vaccine and Incidence of COVID-19 Among Healthcare Workers. J. Clin. Immunol. 2021, 41, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Gopalaswamy, R.; Ganesan, N.; Velmurugan, K.; Aravindhan, V.; Subbian, S. The Strange Case of BCG and COVID-19: The Verdict Is Still up in the Air. Vaccines 2020, 8, 612. [Google Scholar] [CrossRef] [PubMed]
- Allam, M.F.; Amin, G.E.-D. BCG Vaccine does not Protect Against COVID-19. Open Respir. Med. J. 2020, 14, 45–46. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Gualerzi, G.; Ranzieri, S.; Bragazzi, N.L. Stop playing with data: There is no sound evidence that Bacille Calmette-Guérin may avoid SARS-CoV-2 infection (for now). Acta Biomed. 2020, 91, 207–213. [Google Scholar] [CrossRef]
- Chimoyi, L.; Velen, K.; Churchyard, G.J.; Wallis, R.; Lewis, J.J.; Charalambous, S. An ecological study to evaluate the association of Bacillus Calmette-Guerin (BCG) vaccination on cases of SARS-CoV2 infection and mortality from COVID-19. PLoS ONE 2020, 15, e0243707. [Google Scholar] [CrossRef] [PubMed]
- Hamiel, U.; Kozer, E.; Youngster, I. SARS-CoV-2 Rates in BCG-Vaccinated and Unvaccinated Young Adults. JAMA 2020, 323, 2340–2341. [Google Scholar] [CrossRef]
- Bluhm, R.; Pinkovskiy, M. The Spread of COVID-19 and the BCG Vaccine: A Natural Experiment in Reunified Germany. SSRN Electron. J. 2020, 19, 87–114. [Google Scholar] [CrossRef]
- De Chaisemartin, C.; De Chaisemartin, L. Bacille Calmette-Guérin Vaccination in Infancy Does Not Protect Against Coronavirus Disease 2019 (COVID-19): Evidence from a Natural Experiment in Sweden. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Rivas, M.N.; Ebinger, J.E.; Wu, M.; Sun, N.; Braun, J.; Sobhani, K.; Van Eyk, J.E.; Cheng, S.; Arditi, M. BCG vaccination history associates with decreased SARS-CoV-2 seroprevalence across a diverse cohort of health care workers. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Moorlag, S.J.; Van Deuren, R.C.; Van Werkhoven, C.H.; Jaeger, M.; Debisarun, P.; Taks, E.; Mourits, V.P.; Koeken, V.A.; De Bree, L.C.J.; Doesschate, T.T.; et al. Safety and COVID-19 Symptoms in Individuals Recently Vaccinated with BCG: A Retrospective Cohort Study. Cell Rep. Med. 2020, 1, 100073. [Google Scholar] [CrossRef]
- Alkholy, U.M.; Salama, M.E.; Mahmoud, H.; Taher, A.; Elsayes, K.M. Could Bordetella pertussis vaccine protect against coronavirus COVID-19? J. Glob. Antimicrob. Resist. 2020, 22, 803–805. [Google Scholar] [CrossRef]
- Ietto, G. SARS—CoV-2: Reasons of epidemiology of severe ill disease cases and therapeutic approach using trivalent vaccine (tetanus, diphtheria and Bordetella pertussis). Med. Hypotheses 2020, 141, 109779. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.B.; Al Omari, S.; Rafei, R.; Dabboussi, F.; Hamze, M. COVID-19 in children: Could pertussis vaccine play the protective role? Med. Hypotheses 2020, 145, 110305. [Google Scholar] [CrossRef]
- Reche, P.A. Potential Cross-Reactive Immunity to SARS-CoV-2 From Common Human Pathogens and Vaccines. Front. Immunol. 2020, 11, 586984. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Giamarellos-Bourboulis, E.J.; Domínguez-Andrés, J.; Curtis, N.; Van Crevel, R.; Van De Veerdonk, F.L.; Bonten, M. Trained Immunity: A Tool for Reducing Susceptibility to and the Severity of SARS-CoV-2 Infection. Cell 2020, 181, 969–977. [Google Scholar] [CrossRef] [PubMed]
- He, F.; Xia, X.; Nie, D.; Yang, H.; Jiang, Y.; Huo, X.; Guo, F.; Fang, B.; Hu, B.; Jiang, H.; et al. Respiratory bacterial pathogen spectrum among COVID-19 infected and non–COVID-19 virus infected pneumonia patients. Diagn. Microbiol. Infect. Dis. 2020, 98, 115199. [Google Scholar] [CrossRef]
- Renzi, S.; Clementi, M.; Racca, S.; Mucci, M.; Beccaria, P.; Borghi, G.; Landoni, G.; Zangrillo, A. Is Bordetella pertussis co-infecting SARS-CoV-2 patients? Braz. J. Anesthesiol. 2021, 71, 92–93. [Google Scholar] [CrossRef]
- Troeger, C.; Blacker, B.; Khalil, A.I.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Torres, A.; Cillóniz, C.; Blasi, F.; Chalmers, J.D.; Gaillat, J.; Dartois, N.; Schmitt, H.-J.; Welte, T. Burden of pneumococcal community-acquired pneumonia in adults across Europe: A literature review. Respir. Med. 2018, 137, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaacman, D.J.; McIntosh, E.D.; Reinert, R.R. Burden of invasive pneumococcal disease and serotype distribution among Streptococcus pneumoniae isolates in young children in Europe: Impact of the 7-valent pneumococcal conjugate vaccine and considerations for future conjugate vaccines. Int. J. Infect. Dis. 2010, 14, e197–e209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control. Invasive Pneumococcal Disease Surveillance and Disease Data Disease Data from ECDC Surveillance Atlas. 2020. Available online: https://www.ecdc.europa.eu/en/pneumococcal-disease/surveillance-and-disease-data/atlas (accessed on 8 February 2021).
- Hanquet, G.; Krizova, P.; Valentiner-Branth, P.; Ladhani, S.N.; Nuorti, J.P.; Lepoutre, A.; Mereckiene, J.; Knol, M.; Winje, A.B.; Ciruela, P.; et al. Effect of childhood pneumococcal conjugate vaccination on invasive disease in older adults of 10 European countries: Implications for adult vaccination. Thorax 2018, 74, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Ceyhan, M.; Dagan, R.; Sayiner, A.; Chernyshova, L.; Dinleyici, E.Ç.; Hryniewicz, W.; Kulcsár, A.; Mad’Arová, L.; Pazdiora, P.; Sidorenko, S.; et al. Surveillance of pneumococcal diseases in Central and Eastern Europe. Hum. Vaccines Immunother. 2016, 12, 2124–2134. [Google Scholar] [CrossRef] [Green Version]
- Van Aalst, M.; Lötsch, F.; Spijker, R.; van der Meer, J.T.; Langendam, M.W.; Goorhuis, A.; Grobusch, M.P.; de Bree, G.J. Incidence of invasive pneumococcal disease in immunocompromised patients: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2018, 24, 89–100. [Google Scholar] [CrossRef]
- Quattrone, F.; Donzelli, G.; D’Arienzo, S.; Fornili, M.; Innocenti, F.; Forni, S.; Baglietto, L.; Tavoschi, L.; Lopalco, P.L. Invasive Pneumococcal Disease in Tuscany Region, Italy, 2016–2017: Integrating Multiple Data Sources to Investigate Underreporting. Int. J. Environ. Res. Public Health 2020, 17, 7581. [Google Scholar] [CrossRef] [PubMed]
- Monali, R.; De Vita, E.; Mariottini, F.; Privitera, G.; Lopalco, P.L.; Tavoschi, L. Impact of vaccination on invasive pneumococcal disease in Italy 2007–2017: Surveillance challenges and epidemiological changes. Epidemiol. Infect. 2020, 148, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Radaelli, G.; Riva, E.; Giovannini, M. Characteristics of Invasive Pneumococcal Disease in Young Children before the Introduction of PCV13 in Lombardy, Italy. World J. Vaccines 2012, 2, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Regev-Yochay, G.; Rahav, G.; Strahilevitz, J.; Bishara, J.; Katzir, M.; Chowers, M.; Finkelstein, R.; Chazan, B.; Zimhony, O.; Dagan, R. A nationwide surveillance of invasive pneumococcal disease in adults in Israel before an expected effect of PCV7. Vaccine 2013, 31, 2387–2394. [Google Scholar] [CrossRef]
- Draz, I.H.; Halawa, E.F.; Wahby, G.; Ismail, D.K.; Meligy, B.S. Pneumococcal infection among hospitalized Egyptian children. J. Egypt. Public Health Assoc. 2015, 90, 52–57. [Google Scholar] [CrossRef]
- Özdemir, H.; Yıldız, C.; Ötgün, S.N.; Erkol, H.; Karbuz, A.; Kocabaş, B.A.; Kara, T.T.; Gözalan, A.; Durmaz, R.; Çiftçi, E.; et al. The effects of pneumococcal conjugate vaccine (PCV7 and PCV13) on Turkish children with invasive pneumococcal disease: A single center experience. Arch. Argent. de Pediatr. 2017, 115, 316–322. [Google Scholar] [CrossRef]
- Chun, B.C.; Noh, H.-O. Changes of Invasive Pneumococcal Disease Burden in Korea, 2005–2014: Analysis of the National Health Insurance Database. Open Forum Infect. Dis. 2016, 3. [Google Scholar] [CrossRef] [Green Version]
- Anonymous. Pneumococcal Infections in 2017, Japan. IASR 2018, 39, 107–108. [Google Scholar]
- Pennington, K.; The Enhanced Invasive Pneumococcal Disease Surveillance Working Group, for the Communicable Diseases Network Australia. Invasive Pneumococcal Disease Surveillance, 1 July–30 September 2019. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/15C3D92378263DBDCA257C9700814898/$File/IPD-jul-sept-2019-Qrt.pdf (accessed on 1 May 2021).
- Lopez, L.; Heffernan, H.; Gilkison, C.; Sherwood, J. For the Ministry of Health, New Zealand. Invasive Pneumococcal Disease in New Zealand, 2016. CLIENT REPORT No: FW190193. 2019. Available online: https://surv.esr.cri.nz/PDF_surveillance/IPD/2016/2016IPDAnnualReport.pdf (accessed on 15 March 2021).
- Houseman, C.; Hughes, G.J.; Chapman, K.E.; Wilson, D.; Gorton, R. Increased Invasive Pneumococcal Disease, North East England, UK. Emerg. Infect. Dis. 2017, 23, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control. Surveillance and Reporting. Pneumococcal Disease. Available online: https://www.cdc.gov/pneumococcal/surveillance.html (accessed on 30 April 2021).
- Morrill, H.J.; Caffrey, A.R.; Noh, E.; Laplante, K.L. Epidemiology of pneumococcal disease in a national cohort of older adults. Infect. Dis. Ther. 2014, 3, 19–33. [Google Scholar] [CrossRef] [Green Version]
- Augustovski, F.A.; Martí, S.G.; Pichon-Riviere, A.; Debbag, R. Childhood pneumococcal disease burden in Argentina. Rev. Panam. Salud Pública 2009, 25, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Afonso, E.T.; Minamisava, R.; Bierrenbach, A.L.; Escalante, J.J.C.; Alencar, A.P.; Domingues, C.M.; Morais-Neto, O.L.; Toscano, C.M.; Andrade, A.L. Effect of 10-Valent Pneumococcal Vaccine on Pneumonia among Children, Brazil. Emerg. Infect. Dis. 2013, 19, 589–597. [Google Scholar] [CrossRef]
- Vadlamudi, N.K.; Patrick, D.M.; Hoang, L.; Sadarangani, M.; Marra, F. Incidence of invasive pneumococcal disease after introduction of the 13-valent conjugate pneumococcal vaccine in British Columbia: A retrospective cohort study. PLoS ONE 2020, 15, e0239848. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, M.; Palacios, M.G.; Grajales, A.G.; Báez-Revueltas, F.B.; Wilson, M.; McDade, C.; Farkouh, R. Modeling the sustained use of the 13-valent pneumococcal conjugate vaccine compared to switching to the 10-valent vaccine in Mexico. Hum. Vaccines Immunother. 2018, 15, 560–569. [Google Scholar] [CrossRef] [Green Version]
- Knoll, M.D.; Bennett, J.; Quesada, M.G.; Kagucia, E.; Peterson, M.; Feikin, D.; Cohen, A.; Hetrich, M.; Yang, Y.; Sinkevitch, J.; et al. Global Landscape Review of Serotype-Specific Invasive Pneumococcal Disease Surveillance among Countries Using PCV10/13: The Pneumococcal Serotype Replacement and Distribution Estimation (PSERENADE) Project. Microorganisms 2021, 9, 742. [Google Scholar] [CrossRef]
- Lagos, R.; Muñoz, A.; Valenzuela, M.T.; Heitmann, I.; Levine, M.M. Population-based surveillance for hospitalized and ambulatory pediatric invasive pneumococcal disease in Santiago, Chile. Pediatr. Infect. Dis. J. 2002, 21, 1115–1123. [Google Scholar] [CrossRef]
- Tempia, S.; Wolter, N.; Cohen, C.; Walaza, S.; Von Mollendorf, C.; Cohen, A.L.; Moyes, J.; De Gouveia, L.; Nzenze, S.; Treurnicht, F.; et al. Assessing the impact of pneumococcal conjugate vaccines on invasive pneumococcal disease using polymerase chain reaction-based surveillance: An experience from South Africa. BMC Infect. Dis. 2015, 15, 450. [Google Scholar] [CrossRef] [Green Version]
- Anonymous. Human Papillomavirus and Related Diseases Report. ANDORRA. 17 June 2019. Section 9. Indicators Related to Immunisation Practices Other Than HPV Vaccines. 2019. Available online: https://hpvcentre.net/statistics/reports/AND.pdf (accessed on 23 February 2021).
- Luna, C.M.; Pulido, L.; Niederman, M.S.; Casey, A.; Burgos, D.; Agüero, S.D.L.; Grosso, A.; Membriani, E.; Entrocassi, A.C.; Fermepin, M.R.; et al. Decreased relative risk of pneumococcal pneumonia during the last decade, a nested case-control study. Pneumonia 2018, 10, 9. [Google Scholar] [CrossRef]
- Katz, N.; Stecher, D.; Urueña, A.; Juárez, M.D.V.; Aquino, A.; Laspiur, S.; Goldberg, L.; Odonnell, V.; Galante, M.; Vizzotti, C. Adults’ Vaccination in Argentina: First-Ever Assessment of Compliance Through A Nationwide Survey. Open Forum Infect. Dis. 2016, 3, 739. [Google Scholar] [CrossRef] [Green Version]
- Boey, L.; Bosmans, E.; Ferreira, L.B.; Heyvaert, N.; Nelen, M.; Smans, L.; Tuerlinckx, H.; Roelants, M.; Claes, K.; Derdelinckx, I.; et al. Vaccination coverage of recommended vaccines and determinants of vaccination in at-risk groups. Hum. Vaccines Immunother. 2020, 16, 2136–2143. [Google Scholar] [CrossRef]
- Goren, A.; Roberts, C.; Victor, T.W. Comorbid risk, respondent characteristics and likelihood of pneumococcal vaccination versus no vaccination among older adults in Brazil. Expert Rev. Vaccines 2013, 13, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Sevilla, J.P.; Stawasz, A.; Burnes, D.; Agarwal, A.; Hacibedel, B.; Helvacioglu, K.; Sato, R.; Bloom, D.E. Indirect costs of adult pneumococcal disease and the productivity-based rate of return to the 13-valent pneumococcal conjugate vaccine for adults in Turkey. Hum. Vaccin. Immunother. 2020, 16, 1923–1936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, M.; Lindegaard, H.; Hendricks, O.; Friis-Møller, N. Factors associated with influenza and pneumococcal vaccine uptake among rheumatoid arthritis patients in Denmark invited to participate in a pneumococcal vaccine trial (Immunovax_RA). Scand. J. Rheumatol. 2017, 46, 446–453. [Google Scholar] [CrossRef]
- Ejstrud, P.; Hansen, J.B.; Andreasen, D.A. Prophylaxis against pneumococcal infection after splenectomy: A chal-lenge for hospitals and primary care. Eur. J. Surg. 1997, 163, 733–738. [Google Scholar] [PubMed]
- Bonnave, C.; Mertens, D.; Peetermans, W.; Cobbaert, K.; Ghesquiere, B.; Deschodt, M.; Flamaing, J. Adult vaccination for pneumococcal disease: A comparison of the national guidelines in Europe. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 785–791. [Google Scholar] [CrossRef] [Green Version]
- Poscia, A.; Collamati, A.; Carfì, A.; Topinkova, E.; Richter, T.; Denkinger, M.; Pastorino, R.; Landi, F.; Ricciardi, W.; Bernabei, R.; et al. Influenza and pneumococcal vaccination in older adults living in nursing home: A survival analysis on the shelter study. Eur. J. Public Health 2017, 27, 1016–1020. [Google Scholar] [CrossRef] [PubMed]
- Savulescu, C.; Krizova, P.; Lepoutre, A.; Mereckiene, J.; Vestrheim, D.F.; Ciruela, P.; Ordobas, M.; Guevara, M.; McDonald, E.; Morfeldt, E.; et al. Effect of high-valency pneumococcal conjugate vaccines on invasive pneumococcal disease in children in SpIDnet countries: An observational multicentre study. Lancet Respir. Med. 2017, 5, 648–656. [Google Scholar] [CrossRef] [Green Version]
- Jacques, M.; Letaief, H.; Philippe, G.; Xavier, M.; Bernard, C.; Lukas, C. Low Influenza, Pneumococcal and Diphtheria–Tetanus–Poliomyelitis Vaccine Coverage in Patients with Primary Sjögren’s Syndrome: A Cross-Sectional Study. Vaccines 2019, 8, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hmamouchi, I.; Winthrop, K.; Launay, O.; Dougados, M. Low rate of influenza and pneumococcal vaccine coverage in rheumatoid arthritis: Data from the international COMORA cohort. Vaccine 2015, 33, 1446–1452. [Google Scholar] [CrossRef]
- Theidel, U.; Kuhlmann, A.; Braem, A. Pneumococcal Vaccination Rates in Adults in Germany. Dtsch. Aerzteblatt Online 2013, 110, 743–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alqahtani, A.S.; Bondagji, D.M.; Alshehari, A.A.; Basyouni, M.H.; Alhawassi, T.M.; BinDhim, N.F.; Rashid, H. Vaccinations against respiratory infections in Arabian Gulf countries: Barriers and motivators. World J. Clin. Cases 2017, 5, 212–221. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Memish, Z.A. Prevention of pneumococcal infections during mass gathering. Hum. Vaccines Immunother. 2015, 12, 326–330. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Fang, Y.; Dong, W.; Lau, M.; Mo, P.K. Illness representations on pneumonia and pneumococcal vaccination uptake among community-living Chinese people with high-risk conditions aged ≥65 years—A population-based study. Hum. Vaccines Immunother. 2021, 17, 1455–1462. [Google Scholar] [CrossRef]
- Vajer, P.; Tamás, F.; Urbán, R.; Torzsa, P.; Kalabay, L. Pneumococcal vaccination in general practice. Orvosi Hetil. 2015, 156, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Einarsdóttir, H.; Erlendsdóttir, H.; Kristinsson, K.; Gottfredsson, M. Nationwide study of recurrent invasive pneumococcal infections in a population with a low prevalence of human immunodeficiency virus infection. Clin. Microbiol. Infect. 2005, 11, 744–749. [Google Scholar] [CrossRef] [Green Version]
- Giese, C.; Mereckiene, J.; Danis, K.; O’Donnell, J.; O’Flanagan, D.; Cotter, S. Low vaccination coverage for seasonal influenza and pneumococcal disease among adults at-risk and health care workers in Ireland, 2013: The key role of GPs in recommending vaccination. Vaccine 2016, 34, 3657–3662. [Google Scholar] [CrossRef] [PubMed]
- Regev-Yochay, G.; Reisenberg, K.; Katzir, M.; Wiener-Well, Y.; Rahav, G.; Strahilevitz, J.; Istomin, V.; Tsyba, E.; Peretz, A.; Khakshoor, S.; et al. Pneumococcal Meningitis in Adults after Introduction of PCV7 and PCV13, Israel, July 2009–June 20151. Emerg. Infect. Dis. 2018, 24, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, L.H.; Trumbo, S.P.; Matus, C.R.; Sanwogou, N.J.; Toscano, C.M. Pneumococcal conjugate vaccine introduction in Latin America and the Caribbean: Progress and lessons learned. Expert Rev. Vaccines 2016, 15, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Hervert, L.P.; Ferreira-Guerrero, E.; Díaz-Ortega, J.L.; Trejo-Valdivia, B.; Téllez-Rojo, M.M.; Mongua-Rodríguez, N.; Enf, L.; Hernández-Serrato, M.I.; Montoya-Rodríguez, A.A.; García-García, L. Cobertura de vacunación en adultos y adultos mayores en México [Vaccination coverage in young, middle age and elderly adults in Mexico]. Salud Publica Mex. 2013, 55, 300–306. [Google Scholar] [CrossRef]
- Cepeda-Perez, A.S.; Winniczuk, N.T.; Diaz-Borjon, A. Adherencia a las recomendaciones actuales de inmunización en pacientes con artritis reumatoide en México. Reumatol. Clin. 2021, 17, 155–159. [Google Scholar] [CrossRef]
- Mitchell, S.; Nakhid-Schuster, L.; Neeff, M. Adult cochlear implant recipients and meningitis in New Zealand: Are patients receiving the recommended immunisations? N. Z. Med. J. 2020, 133, 14–20. [Google Scholar] [PubMed]
- Gorska-Ciebiada, M.; Saryusz-Wolska, M.; Ciebiada, M.; Loba, J. Pneumococcal and seasonal influenza vaccination among elderly patients with diabetes. Postepy Hig. Med. Dosw 2015, 69, 1182–1189. [Google Scholar] [CrossRef]
- Tawfik, H.; Bashwar, Z.; Al-Ali, A.; Salem, A.M.; Abdelbagi, I. Improving physician’s adherence to completing vaccination schedules for patients with type 2 diabetes attending non-communicable diseases clinics in West Bay Health Center, Qatar. BMJ Qual. Improv. Rep. 2015, 4. [Google Scholar] [CrossRef] [Green Version]
- Della Salute, M. Piano Nazionale Prevenzione Vaccinale 2017–2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 5 November 2020).
- Setia, S.; Eng, P.; Lim, L.H.; Loo, C.M.; Low, J.A.; Tan, C.; Tan, E.K.; Wong, S.Y. Role of pneumococcal vaccination in prevention of pneumococcal disease among adults in Singapore. Int. J. Gen. Med. 2014, 7, 179–191. [Google Scholar] [CrossRef] [Green Version]
- Kolšek-šušteršič, M.; Krasnič, A.B.; Mioč, V.; Paragi, M.; Rifel, J. Nasopharyngeal carriage of Streptococcus pneumoniae and serotypes indentified among nursing home residents in comparison to the elderly and patients younger than 65 years living in domestic environment. Slov. J. Public Health 2017, 56, 172–178. [Google Scholar] [CrossRef]
- Feldman, C.; Dlamini, S.K.; Madhi, S.A.; Meiring, S.; Von Gottberg, A.; De Beer, J.C.; De Necker, M.; Stander, M.P. The cost-effectiveness of using pneumococcal conjugate vaccine (PCV13) versus pneumococcal polysaccharide vaccine (PPSV23), in South African adults. PLoS ONE 2020, 15, e0227945. [Google Scholar] [CrossRef]
- Christenson, B.; Pauksen, K.; Sylvan, S.P. Effect of influenza and pneumococcal vaccines in elderly persons in years of low influenza activity. Virol. J. 2008, 5, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omlin, A.G.; Mühlemann, K.; Fey, M.F.; Pabst, T. Pneumococcal vaccination in splenectomised cancer patients. Eur. J. Cancer 2005, 41, 1731–1734. [Google Scholar] [CrossRef]
- Fischer, L.; Gerstel, P.F.; Poncet, A.; Siegrist, C.-A.; Laffitte, E.; Gabay, C.; Seebach, J.D.; Ribi, C. Pneumococcal polysaccharide vaccination in adults undergoing immunosuppressive treatment for inflammatory diseases—A longitudinal study. Arthritis Res. Ther. 2015, 17, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Tandjung, R.; Badertscher, N.; Morell, S.; Rosemann, T. General practitioners’ experiences, attitudes, and opinions regarding the pneumococcal vaccination for adults: A qualitative study. Int. J. Gen. Med. 2012, 5, 967–974. [Google Scholar] [CrossRef] [Green Version]
- Chiou, W.-Y.; Hung, S.-K.; Lin, H.-Y.; Chen, L.-C.; Hsu, F.-C.; Tsai, S.-J.; Yu, B.-H.; Lee, M.-S.; Li, C.-Y. Effectiveness of 23-valent pneumococcal polysaccharide vaccine on elderly patients with colorectal cancer. Medicine 2019, 98, e18380. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.-H.; Wu, M.-S.; Wu, I.-C. Vaccination coverage and associated factors for receipt of the 23-valent pneumococcal polysaccharide vaccine in Taiwan. Medicine 2018, 97, e9773. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-Y.; Chiang, C.-S.; Chiu, C.-H.; Wang, E.-T.; Chen, Y.-Y.; Yao, S.-M.; Chang, L.-Y.; Huang, L.-M.; Lin, T.-Y.; Chou, J.-H. Successful Control of Streptococcus pneumoniae 19A Replacement with a Catch-up Primary Vaccination Program in Taiwan. Clin. Infect. Dis. 2019, 69, 1581–1587. [Google Scholar] [CrossRef]
- Satman, I.; Akalin, S.; Cakir, B.; Altinel, S.; The diaVAX Study Group. The effect of physicians’ awareness on influenza and pneumococcal vaccination rates and correlates of vaccination in patients with diabetes in Turkey: An epidemiological Study “diaVAX”. Hum. Vaccines Immunother. 2013, 9, 2618–2626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamidi, A.A.; Taş, B.G.; Gündüz, A.; Çelebi, S.N.; Esen, E.S.; Toprak, D.; Dökmetaş, I. Immunization rates of pneumococcal, influenza and tetanus vaccines and knowledge and attitudes of adult patients who receive inpatient treatment at hospital: Point prevalence study. Hum. Vaccines Immunother. 2018, 14, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Akın, L.; Macabéo, B.; Caliskan, Z.; Altinel, S.; Satman, I. Cost-Effectiveness of Increasing Influenza Vaccination Coverage in Adults with Type 2 Diabetes in Turkey. PLoS ONE 2016, 11, e0157657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, R.; Winthrop, K.L.; Pye, S.R.; Brown, B.; Dixon, W.G. Influenza and Pneumococcal Vaccination Uptake in Patients with Rheumatoid Arthritis Treated with Immunosuppressive Therapy in the UK: A Retrospective Cohort Study Using Data from the Clinical Practice Research Datalink. PLoS ONE 2016, 11, e0153848. [Google Scholar] [CrossRef] [PubMed]
- Filia, A.; Tavilla, A.; Bella, A.; Magurano, F.; Ansaldi, F.; Chironna, M.; Nicoletti, L.; Palù, G.; Iannazzo, S.; Declich, S.; et al. Measles in Italy, July 2009 to September 2010. Eurosurveillance 2011, 16, 19925. [Google Scholar] [CrossRef]
- Boccalini, S.; Varone, O.; Chellini, M.; Pieri, L.; Sala, A.; Berardi, C.; Bonanni, P.; Bechini, A. Hospitalizations for pneumonia, invasive diseases and otitis in Tuscany (Italy), 2002–2014: Which was the impact of universal pneumococcal pediatric vaccination? Hum. Vaccines Immunother. 2017, 13, 428–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cases of COVID-19 per 100K in Italy as of 4 July 2020. Available online: https://upload.wikimedia.org/wikipedia/commons/thumb/e/e6/COVID-19_outbreak_Italy_per_capita_cases_map.svg/460px-COVID-19_outbreak_Italy_per_capita_cases_map.svg.png (accessed on 4 July 2020).
- Centers for Disease Control. 2017 Childhood Pneumococcal Conjugate Vaccine (PCV) Coverage Report. 2017. Available online: https://www.cdc.gov/vaccines/imz-managers/coverage/childvaxview/data-reports/pcv/reports/2017.html (accessed on 9 November 2020).
- Centers for Disease Control. Pneumococcal Vaccination Coverage Among Adults 18–64 Years at Increased Risk and ≥65 Years, Td and Tdap Vaccination Coverage Among Adults ≥18 Years, and Shingles Vaccination Coverage Among Adults ≥60 Years by Selected Local Area, State, HHS Region, and the United States, BRFSS, 2008 through 2017. Available online: https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/data-reports/general-population/trend/index.html (accessed on 9 November 2020).
- Centers for Disease Control and Prevention. Influenza and pneumococcal vaccination coverage among persons aged > or = 65 years—United States, 2004–2005. MMWR Morb. Mortal. Wkly. Rep. 2006, 55, 1065–1068. [Google Scholar]
- Curtin, F.; Schulz, P. Multiple correlations and bonferroni’s correction. Biol. Psychiatry 1998, 44, 775–777. [Google Scholar] [CrossRef]
- Benin, A.L.; O’Brien, K.L.; Watt, J.P.; Reid, R.; Zell, E.R.; Katz, S.; Donaldson, C.; Parkinson, A.; Schuchat, A.; Santosham, M.; et al. Effectiveness of the 23-Valent Polysaccharide Vaccine against Invasive Pneumococcal Disease in Navajo Adults. J. Infect. Dis. 2003, 188, 81–89. [Google Scholar] [CrossRef]
- Lu, P.-J.; O’Halloran, A.; Williams, W.W.; Lindley, M.C.; Farrall, S.; Bridges, C.B. Racial and ethnic disparities in vaccination coverage among adult populations in the U.S. Vaccine 2015, 33, 83–91. [Google Scholar] [CrossRef]
- Happe, M.; Samuvel, D.J.; Ohtola, J.A.; Korte, J.E.; Westerink, M.J. Race-related differences in functional antibody response to pneumococcal vaccination in HIV-infected individuals. Vaccine 2019, 37, 1622–1629. [Google Scholar] [CrossRef]
- Centers for Disease Control. Vaccination Coverage among Adults in the United States, National Health Interview Survey. 2016. Available online: https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/pubs-resources/NHIS-2016.html#pneumo (accessed on 13 December 2020).
- Centers for Disease Control. Risk for COVID-19 Infection, Hospitalization, and Death by Race/Ethnicity. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 17 March 2021).
- Said, M.A.; O’Brien, K.L.; Nuorti, J.P.; Singleton, R.; Whitney, C.G.; Hennessy, T.W. The epidemiologic evidence underly-ing recommendations for use of pneumococcal polysaccharide vaccine among American Indian and Alaska Native populations. Vaccine 2011, 29, 5355–5362. [Google Scholar] [CrossRef]
- de St Maurice, A.; Grijalva, C.G.; Fonnesbeck, C.; Schaffner, W.; Halasa, N.B. Racial and regional differences in rates of invasive pneumococcal disease. Pediatrics 2015, 136, e1186–e1194. [Google Scholar] [CrossRef]
- Hsu, K.; Pelton, S.; Karumuri, S.; Heisey-Grove, D.; Klein, J.; Massachusetts Department of Public Health Epidemiologists. Population-based surveillance for childhood invasive pneumococcal disease in the era of conjugate vaccine. Pediatr. Infect. Dis. J. 2005, 24, 17–23. [Google Scholar] [CrossRef]
- Soto, K.; Petit, S.; Hadler, J.L. Changing disparities in invasive pneumococcal disease by socioeconomic status and race/ ethnicity in Connecticut, 1998–2008. Public Health Rep. 2011, 126 (Suppl. 3), 81–88. [Google Scholar] [CrossRef] [Green Version]
- Intra, J.; Besana, S.; Savarino, C.; Brambilla, P. Serotype Distribution and Antimicrobial Resistance of Streptococcus pneumoniae Invasive Isolates Collected at the Italian Hospital of Desio, Lombardy, from 2008 to 2016. Front. Public Health 2017, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin-Chowdhury, Z.; Aiano, F.; Mensah, A.; Sheppard, C.L.; Litt, D.; Fry, N.K.; Andrews, N.; Ramsay, E.M.; Ladhani, S.N. Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on Invasive Pneumococcal Disease and Risk of Pneumococcal Coinfection with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Prospective National Cohort Study, England. Clin. Infect. Dis. 2021, 72, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Boccalini, S.; Bechini, A.; Levi, M.; Tiscione, E.; Gasparini, R.; Bonanni, P. Cost-effectiveness of new adult pneumococcal vaccination strategies in Italy. Hum. Vaccines Immunother. 2013, 9, 699–706. [Google Scholar] [CrossRef] [Green Version]
- Orsi, A.; Ansaldi, F.; Trucchi, C.; Rosselli, R.; Icardi, G. Pneumococcus and the Elderly in Italy: A Summary of Available Evidence Regarding Carriage, Clinical Burden of Lower Respiratory Tract Infections and On-Field Effectiveness of PCV13 Vaccination. Int. J. Mol. Sci. 2016, 17, 1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuffrida, S. Calabria: A successful experience implementing Herpes Zoster vaccination strategies. Aging Clin. Exp. Res. 2019, 31, 421–423. [Google Scholar] [CrossRef]
- Baldo, V.; Cocchio, S.; Gallo, T.; Furlan, P.; Romor, P.; Bertoncello, C.; Buja, A.; Baldovin, T. Pneumococcal Conjugated Vaccine Reduces the High Mortality for Community-Acquired Pneumonia in the Elderly: An Italian Regional Experience. PLoS ONE 2016, 11, e0166637. [Google Scholar] [CrossRef]
- Bellino, S.; Piovesan, C.; Bella, A.; Rizzo, C.; Pezzotti, P.; Ramigni, M. Determinants of vaccination uptake, and influenza vaccine effectiveness in preventing deaths and hospital admissions in the elderly population; Treviso, Italy, 2014/2015-2016/2017 seasons. Hum. Vaccines Immunother. 2020, 16, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, D.; Tafuri, S.; Caputi, G.; Fortunato, F.; Reggio, P.; Germinario, C.; Prato, R. Eight years of active proposal of pneumococcal 23-valent polysaccharide vaccine: Survey on coverage rate among elderly and chronic patients. Am. J. Infect. Control. 2010, 38, e8–e15. [Google Scholar] [CrossRef] [PubMed]
- Choe, Y.J.; Blatt, D.B.; Lee, H.J.; Choi, E.H. Associations between geographic region and immune response variations to pneumococcal conjugate vaccines in clinical trials: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 92, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, G.G. Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017–2018 influenza season. Vaccine 2020, 38, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Mateus, J.; Grifoni, A.; Tarke, A.; Sidney, J.; Ramirez, S.I.; Dan, J.M.; Burger, Z.C.; Rawlings, S.A.; Smith, D.M.; Phillips, E.; et al. Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans. Science 2020, 370, 89–94. [Google Scholar] [CrossRef]
- Braun, J.; Loyal, L.; Frentsch, M.; Wendisch, D.; Georg, P.; Kurth, F.; Hippenstiel, S.; Dingeldey, M.; Kruse, B.; Fauchere, F.; et al. SARS-CoV-2-reactive T cells in healthy donors and patients with COVID-19. Nature 2020, 587, 270–274. [Google Scholar] [CrossRef]
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501. [Google Scholar] [CrossRef]
- Stervbo, U.; Rahmann, S.; Roch, T.; Westhoff, T.H.; Babel, N. Epitope similarity cannot explain the pre-formed T cell immunity towards structural SARS-CoV-2 proteins. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Woldemeskel, B.A.; Kwaa, A.K.; Garliss, C.C.; Laeyendecker, O.; Ray, S.C.; Blankson, J.N. Healthy donor T cell responses to common cold coronaviruses and SARS-CoV-2. J. Clin. Investig. 2020, 130, 6631–6638. [Google Scholar] [CrossRef]
- Bacher, P.; Rosati, E.; Esser, D.; Martini, G.R.; Saggau, C.; Schiminsky, E.; Dargvainiene, J.; Schröder, I.; Wieters, I.; Khodamoradi, Y.; et al. Low-Avidity CD4+ T Cell Responses to SARS-CoV-2 in Unexposed Individuals and Humans with Severe COVID-19. Immunity 2020, 53, 1258–1271. [Google Scholar] [CrossRef]
- Troeger, E.C.; Khalil, A.I.; Blacker, B.F.; Biehl, M.H.; Albertson, S.B.; Zimsen, S.R.M.; Rao, P.C.; Abate, D.; Admasie, A.; Ahmadi, A.; et al. Quantifying risks and interventions that have affected the burden of lower respiratory infections among children younger than 5 years: An analysis for the Global Burden of Disease Study 2017. Lancet Infect. Dis. 2020, 20, 60–79. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nation | COVID Cases / mil | COVID Deaths /mil | LRI Deaths /1000 | IPD/ 100K | Ch Pn | Ad Pn | AR Pn | Ch+ Ad Pn | All Pn | Hib | Ad Inf | DTP | M C V | O P V | BCG |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Andorra | 82,144 | 983 | 47.7 | 96 | 0 | 0 | 96 | 96 | 98 | 99 | 99 | 99 | 0 | ||
| Argentina | 26,842 | 723 | 62.8 | 36 | 80 | 18.5 | 37 | 99 | 136 | 83 | 83 | 86 | 83 | 93 | |
| Australia | 1080 | 35 | 18.4 | 8 | 95 | 80 | 36 | 175 | 211 | 94 | 80.5 | 95 | 93 | 95 | 0 |
| Austria | 15,400 | 148 | 8.8 | 6.9 | 62 | 50 | 10 | 112 | 122 | 85 | 75 | 85 | 94 | 85 | 0 |
| Bahrain | 48,091 | 191 | 6.3 | 97 | 0 | 31 | 97 | 128 | 99 | 18 | 20 | 99 | 99 | 97 | |
| Belgium | 41,297 | 1079 | 45.4 | 13.2 | [96]48 | 29 | 20 | 77 | 97 | 97 | 63 | 98 | 85 | 98 | 0 |
| Bolivia | 12,125 | 748 | 60.3 | 75 | 0 | 75 | 75 | 85 | 79 | 75 | 85 | ||||
| Brazil | 26,427 | 760 | 33 | 45 | [84]64 | 10 | 10 | 74 | 84 | 83 | 78 | 87 | 76 | 85 | 98 |
| Canada | 6702 | 275 | 25.1 | 20 | 81 | 37 | 17 | 118 | 135 | 91 | 64 | 91 | 87 | 91 | 0 |
| Chile | 27,037 | 754 | 27.4 | 33.9 | [93]71 | 5 | 76 | 95 | 41 | 95 | 93 | 96 | 96 | ||
| Croatia | 15,210 | 175 | 16 | 0.2 | 83 | 77 | 160 | 94 | 94 | 93 | 94 | 98 | |||
| Czech Rep | 36,576 | 404 | 27.2 | 5 | 71 | 37 | 108 | 97 | 97 | 92 | 97 | 99 | |||
| Denmark | 9170 | 127 | 40.5 | 13.8 | 97 | 65 | 6 | 162 | 168 | 97 | 52 | 97 | 90 | 97 | 0 |
| France | 25,440 | 610 | 31.8 | 8 | 81 | 18 | 26 | 99 | 128 | 95 | 63 | 96 | 83 | 70 | 22 |
| Germany | 7646 | 135 | 27.3 | 10 | 86 | 50.9 | 16 | 137 | 153 | 92 | 45.5 | 96 | 93 | 93 | 0 |
| Greece | 5022 | 69 | 24.6 | 0.4 | 96 | 34 | 30 | 130 | 160 | 99 | 70 | 99 | 83 | 99 | 45.5 |
| Hong Kong | 713 | 14 | 99 | 40 | 139 | 47 | 99 | 99.8 | 0 | 99.8 | |||||
| Hungary | 10,322 | 233 | 9.8 | 3.4 | 99 | 36 | 4 | 135 | 139 | 93 | 99 | 99 | 99 | 99 | |
| Iceland | 14,733 | 53 | 28.8 | 9.7 | 92 | 50 | 26 | 142 | 168 | 93 | 93 | 93 | 93 | 0 | |
| Ireland | 13,020 | 391 | 28.9 | 11.8 | 86 | 36 | 16 | 122 | 138 | 94 | 62 | 94 | 89 | 94 | 43 |
| Israel | 34,618 | 287 | 20.8 | 9.6 | 95 | 70 | 165 | 98 | 59 | 98 | 96 | 98 | 0 | ||
| Italy | 14,276 | 672 | 15.2 | 12.1 | 49 | 26 | 12 | 75 | 87 | 94 | 60 | 95 | 89 | 96 | 0 |
| Japan | 829 | 14 | 76.6 | 2.5 | 99 | 74 | 13 | 173 | 186 | 99 | 27 | 99 | 93 | 98 | 99 |
| Kuwait | 30,394 | 187 | 8.7 | 97 | 25 | 79 | 122 | 201 | 99 | 17 | 34 | 98 | 99 | 96 | |
| Mexico | 7335 | 725 | 14.5 | 7 | 86 | 45 | 30 | 131 | 161 | 88 | 63 | 88 | 99 | 82 | 96 |
| Netherlands | 23,194 | 460 | 42.6 | 16 | 94 | 2 | 97 | 93 | 79 | 93 | 83 | 94 | 0 | ||
| New Zeal. | 395 | 5 | 16.3 | 10.2 | 96 | 50 | 15 | 146 | 161 | 91 | 62 | 92 | 99 | 92 | 10 |
| Nicaragua | 841 | 24 | 13.5 | 99 | 0 | 99 | 99 | 99 | 99 | 99 | 99 | ||||
| Norway | 4341 | 52 | 33.6 | 11 | 94 | 15 | 114 | 99 | 99 | 99 | 97 | 44 | |||
| Oman | 22,747 | 250 | 10.1 | 99 | 10 | 17 | 109 | 126 | 99 | 17 | 75 | 99 | 99 | 99 | |
| Peru | 27,610 | 1048 | 54.5 | 19.8 | (84)42 | 5 | 47 | 84 | 69 | 84 | 66 | 87 | 90 | ||
| Poland | 13,052 | 193 | 26.5 | 3.6 | 60 | 69 | 9 | 129 | 138 | 95 | 95 | 93 | 87 | 92 | |
| Portugal | 16,385 | 274 | 60.4 | 3.9 | (98)49 | 5 | 59 | 99 | 68 | 99 | 96 | 99 | 21 | ||
| Qatar | 47,657 | 83 | 2.5 | 98 | 20 | 48 | 118 | 165 | 98 | 24 | 29 | 99 | 99 | 99 | |
| San Marino | 42,049 | 1296 | 58 | 2 | 4 | 60 | 64 | 86 | 21 | 88 | 86 | 88 | 0 | ||
| Saudi Arab. | 9995 | 157 | 14.6 | 17.4 | 96 | 7 | 74 | 103 | 177 | 96 | 15 | 7 | 96 | 97 | 98 |
| Singapore | 9895 | 5 | 58.8 | 82 | 60 | 41 | 142 | 183 | 96 | 96 | 98 | 96 | 98 | ||
| Slovakia | 13,018 | 58 | 32 | 1.8 | 97 | 17.6 | 114.6 | 97 | 68 | 97 | 97 | 97 | 90 | ||
| Slovenia | 20,518 | 239 | 30.3 | 12.2 | 97 | 6 | 0 | 103 | 103 | 96 | 95 | 94 | 95 | 96 | |
| South Africa | 12,956 | 354 | 58.3 | 50 | 86 | 3 | 13 | 89 | 102 | 85 | 85 | 83 | 98 | 84 | |
| South Korea | 530 | 9 | 21.9 | 0.79 | 97 | 60 | 30 | 157 | 187 | 98 | 74 | 98 | 97 | 85 | 99 |
| Spain | 29,692 | 830 | 23.5 | 56.2 | (61)31 | 33 | 11 | 64 | 80 | 94 | 60 | 93 | 94 | 96 | 0 |
| Sweden | 14,471 | 595 | 31.1 | 13.9 | 97 | 28 | 125 | 97 | 44 | 97 | 95 | 98 | 26 | ||
| Switzerland | 24,423 | 312 | 21.5 | 7.6 | 84 | 2 | 59 | 86 | 144 | 95 | 39 | 96 | 89 | 96 | 0 |
| Taiwan | 26 | 0.3 | 37.5 | 7.2 | 100 | 41 | 21 | 141 | 162 | 99 | 0 | ||||
| Turkey | 4569 | 126 | 8 | 2.4 | 97 | 24 | 20 | 121 | 141 | 98 | 6 | 98 | 87 | 99 | 96 |
| UAE | 14,085 | 51 | 4.7 | 13.6 | 99 | 21 | 43 | 120 | 163 | 99 | 22 | 17 | 99 | 95 | 94 |
| U.K. | 16,857 | 713 | 61.2 | 11.4 | 92 | 44 | 15 | 136 | 151 | 94 | 83.5 | 94 | 88 | 93 | 0 |
| Uruguay | 1287 | 20 | 46.5 | 95 | 0 | 46 | 95 | 141 | 94 | 94 | 90 | 93 | 99 | ||
| USA | 30,206 | 729 | 29.7 | 23 | 88 | 62 | 23 | 150 | 173 | 92 | 65.2 | 94 | 97 | 93 | 0 |
| Venezuela | 3486 | 30 | 15.2 | 0 | 0 | 12 | 0 | 12 | 64 | 0 | 64 | 93 | 62 | 91 |
| USA State | COVID-19 Cases/ Million pop | COVID-19 Deaths/ Million pop | Pneumonia Deaths/ 100,000 (2019) | PNEUM CHILD (%) (2017) | PNEUM 18–64 AT RISK (%) (2017) | PNEUM >65 (%) (2016) | TOTAL PNEUM RATE | INF VACC RATE >64 (2019) | INF VACC RATE TOTAL (2019) |
|---|---|---|---|---|---|---|---|---|---|
| Alabama | 41,780 | 629 | 21.4 | 87.4 | 29.4 | 71.7 | 188.5 | 58.0 | 45.8 |
| Alaska | 25,584 | 115 | 12.1 | 83.9 | 24.3 | 64.2 | 172.4 | 49.0 | 42.1 |
| Arizona | 35,619 | 847 | 12.4 | 84.4 | 30.5 | 74 | 188.9 | 50.6 | 43.2 |
| Arkansas | 40,382 | 691 | 18 | 77.5 | 32.2 | 75 | 184.7 | 47.6 | 51.7 |
| California | 24,694 | 455 | 15.6 | 84.9 | 29 | 69.9 | 183.8 | 54.9 | 47.5 |
| Colorado | 22,745 | 416 | 9.7 | 84.4 | 37.3 | 78.8 | 200.5 | 55.9 | 51.4 |
| Connecticut | 21,913 | 1,310 | 14.8 | 89 | 28.8 | 72.4 | 190.2 | 55.3 | 56.3 |
| Cook County, IL (Chicago) | 19,503 | 501 | 87.7 | 30.1 | 60.9 | 178.7 | |||
| Delaware | 27,320 | 737 | 13.1 | 88.8 | 39.6 | 69.3 | 197.7 | 58.3 | 51.6 |
| District of Columbia | 25,628 | 928 | 88.5 | 30.2 | 54.9 | 173.6 | 59.8 | 49.3 | |
| Florida | 39,292 | 797 | 9.6 | 84.1 | 25.9 | 73.3 | 183.3 | 52.8 | 41.8 |
| Georgia | 38,245 | 815 | 14.5 | 83.2 | 27.7 | 71.2 | 182.1 | 52.6 | 43.0 |
| Hawaii | 11,263 | 156 | 24.5 | 82.1 | 25.2 | 65.3 | 172.6 | 52.7 | 46.8 |
| Idaho | 40,827 | 384 | 11.9 | 87.5 | 28.3 | 70.5 | 186.3 | 53.0 | 41.4 |
| Illinois | 38,510 | 832 | 16.3 | 88.7 | 28.3 | 68.6 | 185.6 | 55.4 | 49.8 |
| Indiana | 31,249 | 688 | 14 | 78.9 | 31.6 | 72.5 | 183 | 46.9 | 48.0 |
| Iowa | 49,703 | 585 | 15.7 | 88.8 | 33.9 | 74.1 | 196.8 | 59.7 | 53.8 |
| Kansas | 34,082 | 400 | 17.1 | 83.9 | 30.3 | 76.2 | 190.4 | 56.3 | 50.0 |
| Kentucky | 27,047 | 350 | 18.3 | 92.4 | 38 | 64.3 | 194.7 | 59.4 | 48.4 |
| Louisiana | 40,432 | 1298 | 15.6 | 79.1 | 30.2 | 68.6 | 177.9 | 45.7 | 44.0 |
| Maine | 5723 | 113 | 15.3 | 82.2 | 43.1 | 77.2 | 202.5 | 48.5 | 53.0 |
| Maryland | 25,700 | 698 | 13.6 | 87.6 | 33.9 | 74.7 | 196.2 | 56.5 | 53.1 |
| Massachusetts | 24,867 | 1472 | 15.8 | 91.5 | 32 | 73.4 | 196.9 | 54.5 | 56.8 |
| Michigan | 22,930 | 796 | 14.5 | 82.9 | 36.8 | 72.4 | 192.1 | 51.9 | 48.3 |
| Minnesota | 32,070 | 481 | 10 | 79.6 | 30.5 | 72.7 | 182.8 | 59.1 | 53.4 |
| Mississippi | 42,741 | 1157 | 26.1 | 92.3 | 25.2 | 68.7 | 186.2 | 60.0 | 44.1 |
| Missouri | 35,562 | 542 | 18.7 | 83.2 | 33.1 | 74.4 | 190.7 | 61.2 | 47.5 |
| Montana | 37,126 | 427 | 10.7 | 87.3 | 33.6 | 73.3 | 194.2 | 57.4 | 47.7 |
| Nebraska | 42,594 | 363 | 16.1 | 89.5 | 31.5 | 75.8 | 196.8 | 57.9 | 55.3 |
| Nevada | 35,720 | 601 | 16 | 83.9 | 28.8 | 68.5 | 181.2 | 59.5 | 42.3 |
| New Hampshire | 9184 | 360 | 14.3 | 90 | 35.3 | 78.6 | 203.9 | 50.7 | 54.2 |
| New Jersey | 29,281 | 1865 | 12.6 | 80.1 | 25.9 | 68.1 | 174.1 | 63.7 | 45.2 |
| New Mexico | 26,173 | 533 | 14.2 | 86.3 | 32.5 | 71.3 | 190.1 | 53.2 | 48.8 |
| New York | 29,080 | 1739 | 18.4 | 79.6 | 26.2 | 64 | 169.8 | 44.8 | 48.6 |
| New York City | 30,953 | 2738 | 74.2 | 34 | 65.9 | 174.1 | |||
| North Carolina | 27,969 | 439 | 16.9 | 87.9 | 34.2 | 76.7 | 198.8 | 65.6 | 53.5 |
| North Dakota | 71,261 | 839 | 15.6 | 85.3 | 32.1 | 75.2 | 192.6 | 56.5 | 52.9 |
| Ohio | 21,410 | 476 | 15.7 | 81.6 | 32 | 74.3 | 187.9 | 55.8 | 48.6 |
| Oklahoma | 34,435 | 363 | 17.8 | 78.1 | 35.1 | 75.1 | 188.3 | 64.5 | 52.3 |
| Oregon | 11,961 | 173 | 10.2 | 83.3 | 42.5 | 77.3 | 203.1 | 49.2 | 48.2 |
| Pennsylvania | 18,369 | 711 | 15.5 | 82 | 32.3 | 75.3 | 189.6 | 59.7 | 53.0 |
| Philadelphia, PA | 30,000 | 1192 | 83.2 | 30.1 | 67.2 | 180.5 | |||
| Rhode Island | 34,341 | 1155 | 13.3 | 88.5 | 34.4 | 73 | 195.9 | 51.1 | 56.8 |
| South Carolina | 36,065 | 784 | 14.5 | 80.2 | 27.8 | 73.6 | 181.6 | 58.4 | 47.7 |
| South Dakota | 62,625 | 606 | 20.7 | 82.5 | 26.5 | 76.9 | 185.9 | 58.4 | 55.1 |
| Tennessee | 41,272 | 526 | 20.7 | 84.2 | 30.8 | 74.5 | 189.5 | 51.1 | 45.1 |
| Texas | 35,177 | 665 | 12.9 | 85.5 | 26.7 | 71.3 | 183.5 | 48.1 | 42.2 |
| Utah | 41,367 | 206 | 13.4 | 83.8 | 32.5 | 73.7 | 190 | 45.2 | 48.7 |
| Vermont | 3830 | 95 | 9.8 | 86.5 | 43.7 | 74.8 | 205 | 52.0 | 54.5 |
| Virginia | 22,667 | 435 | 13.1 | 90.2 | 38.5 | 73 | 201.7 | 54.4 | 55.7 |
| Washington | 15,856 | 322 | 10.9 | 84.7 | 41.6 | 78.1 | 204.4 | 58.9 | 53.4 |
| West Virginia | 15,849 | 280 | 21.2 | 86.7 | 34.7 | 73 | 194.4 | 58.4 | 50.9 |
| Wisconsin | 45,928 | 397 | 14.1 | 87.9 | 31.2 | 74.3 | 193.4 | 63.5 | 56.6 |
| Wyoming | 29,909 | 197 | 18.9 | 85.8 | 27.9 | 70.1 | 183.8 | 45.4 | 43.8 |
| ITALIAN REGION | COVID-19 DEATHS/ 100K | IPD/ 100K | PCV13 % (INFANT2016) | MMR % (Infant) | MMR % (Age 16) | INF % (Total Pop.) |
|---|---|---|---|---|---|---|
| ABRUZZO | 400 | 1.0 | 89.3 | 92.2 | 80.5 | 56 |
| AOSTA VALLEY | 800 | 2.0 | 87.4 | 87.8 | 84.0 | 45 |
| BASILICATA | 70 | 0.2 | 97.0 | 90.2 | 79.5 | 67 |
| BOLZANO | 500 | 9.0 | 80.5 | 70.8 | 91.0 | 37 |
| CALABRIA | 35 | 0.2 | 90.0 | 85.4 | 53.2 | 64 |
| CAMPANIA | 70 | 0.2 | 82.1 | 86.9 | 62.1 | 62 |
| EMILIA ROMAGNA | 400 | 3.0 | 90.6 | 93.9 | 94.0 | 56 |
| FRIULI V. G. | 50 | 2.0 | 81.4 | 91.4 | 90.4 | 60 |
| LAZIO | 130 | 1.5 | 93.8 | 89.6 | 67.0 | 53 |
| LIGURIA | 500 | 1.5 | 91.8 | 87.9 | 79.7 | 51 |
| LOMBARDY | 1000 | 8.0 | 85.7 | 94.8 | 84.4 | 49 |
| MARCHE | 600 | 2.5 | 89.4 | 92.4 | 90.0 | 53 |
| MOISE | 130 | 0.5 | 91.5 | 88.8 | 67.0 | 66 |
| PIEDMONT | 700 | 7.1 | 91.8 | 93.1 | 83.3 | 50 |
| PUGLIA | 70 | 0.2 | 91.4 | 92.3 | 78.6 | 58 |
| SARDINIA | 70 | 0.2 | 94.2 | 95.5 | 83.3 | 47 |
| SICILY | 150 | 0.5 | 91.7 | 86.8 | 59.7 | 56 |
| TOSCANY | 250 | 6.2 | 89.0 | 92.7 | 90.9 | 58 |
| TRENTO | 700 | 8.7 | 87.3 | 88.5 | 90.5 | 55 |
| UMBRIA | 130 | 0.5 | 94.3 | 95.2 | 89.0 | 65 |
| VENETO | 300 | 4.0 | 86.6 | 93.0 | 97.1 | 56 |
| Race/Ethnicity | % Adult >64 Pneumococcal Vaccination (2015–2016) | IPD Rate in >64 Adults/100,000 Population | IPD Rate in >64 Adults Compared with Whites | COVID-19 Case Rate Compared with Whites | COVID-19 Hospitalization Rate Compared with Whites | COVID-19 Deaths Compared with Whites |
|---|---|---|---|---|---|---|
| White | 68.2–71.0 | 4.9–16.7 | 1.0 | 1.0 | 1.0 | 1.0 |
| Asians | 49.0–52.6 | 5.9 | 1.0 | 0.7 | 1.0 | 1.0 |
| African American/Black | 50.2–55.5 | 11.3–29.4 | 1.8–2.3 | 1.1 | 2.9 | 1.9 |
| Hispanic/Latino | 41.7–48.6 | 9.2–22.2 | 1.9–2.5 | 1.3 | 3.1 | 2.3 |
| Native Americans | 60.3–64.2 (*) | 80–120 | 3.0–5.0 | 1.7 | 3.7 | 2.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Root-Bernstein, R. Pneumococcal and Influenza Vaccination Rates and Pneumococcal Invasive Disease Rates Set Geographical and Ethnic Population Susceptibility to Serious COVID-19 Cases and Deaths. Vaccines 2021, 9, 474. https://doi.org/10.3390/vaccines9050474
Root-Bernstein R. Pneumococcal and Influenza Vaccination Rates and Pneumococcal Invasive Disease Rates Set Geographical and Ethnic Population Susceptibility to Serious COVID-19 Cases and Deaths. Vaccines. 2021; 9(5):474. https://doi.org/10.3390/vaccines9050474
Chicago/Turabian StyleRoot-Bernstein, Robert. 2021. "Pneumococcal and Influenza Vaccination Rates and Pneumococcal Invasive Disease Rates Set Geographical and Ethnic Population Susceptibility to Serious COVID-19 Cases and Deaths" Vaccines 9, no. 5: 474. https://doi.org/10.3390/vaccines9050474
APA StyleRoot-Bernstein, R. (2021). Pneumococcal and Influenza Vaccination Rates and Pneumococcal Invasive Disease Rates Set Geographical and Ethnic Population Susceptibility to Serious COVID-19 Cases and Deaths. Vaccines, 9(5), 474. https://doi.org/10.3390/vaccines9050474