
Trigeminal Nerve Affection in Patients with Neuro-Sjögren Detected by Corneal Confocal Microscopy

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Diagnosis of Sjögren’s Syndrome and Evaluation of Disease and Symptom Severity
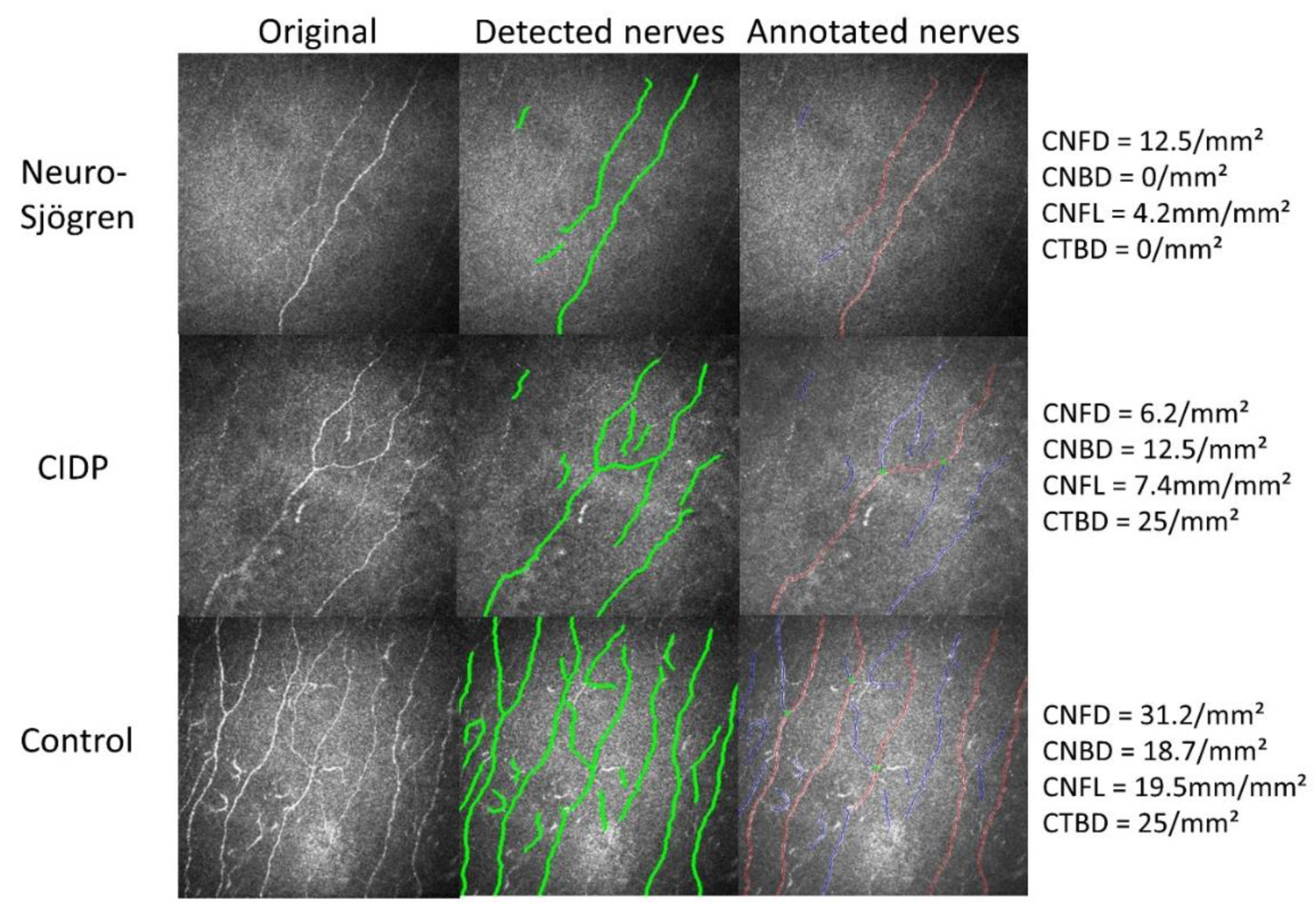
2.3. Corneal Confocal Microscopy
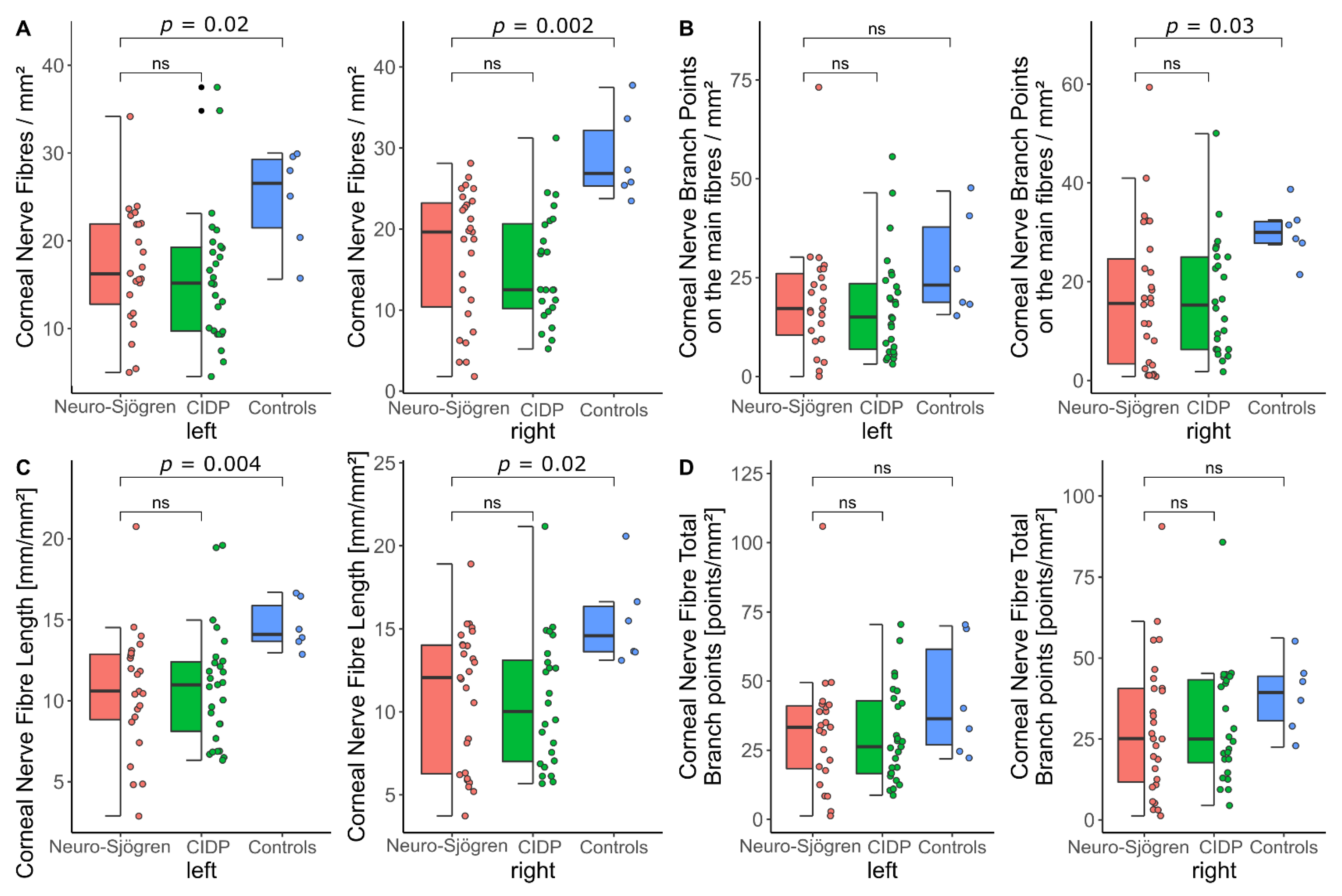
- Corneal Nerve Fibre Density (CNFD): The number of detected fibres per mm2
- Corneal Nerve Fibre Main Branch Density (CNBD): The number of detected branch points on the main fibres per mm2
- Corneal Nerve Fibre Length (CNFL): The total length of detected nerve fibres in mm per mm2
- Corneal Nerve Fibre Total Branch Density (CTBD): The total number of branch points per mm2
2.4. Clinical Evaluation of Dry Eye Symptoms and Signs
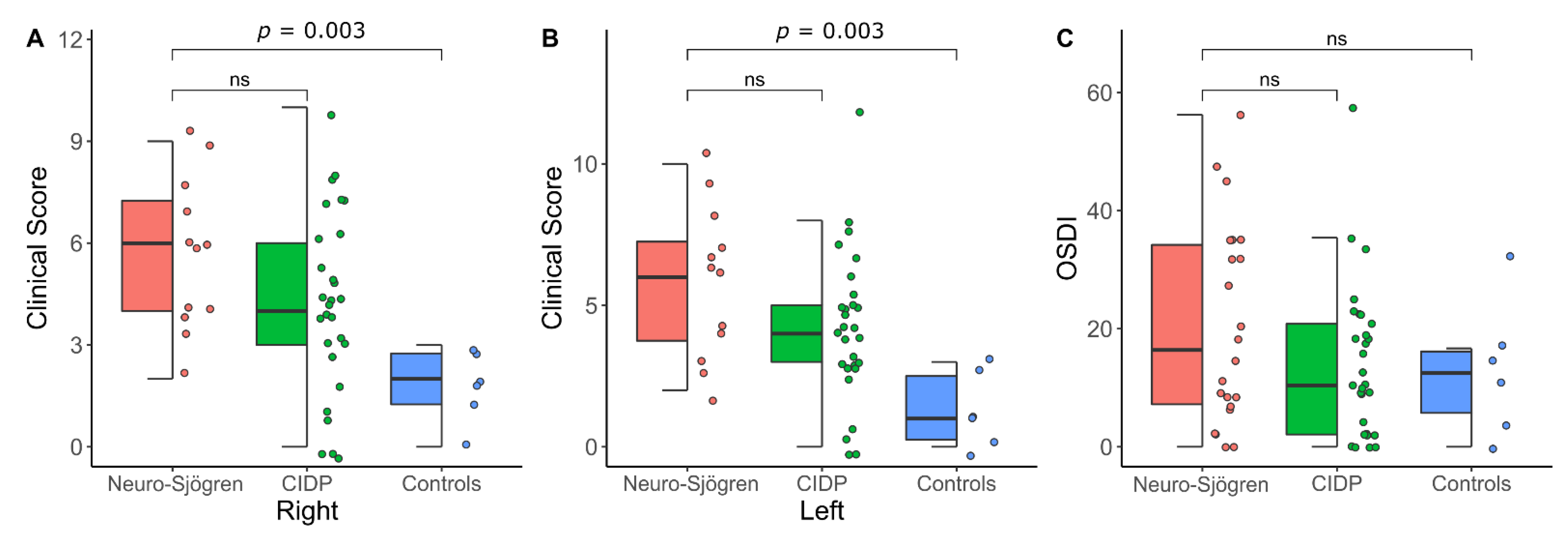
2.4.1. Clinical Score of the Dry Eye
2.4.2. Ocular Surface Disease Index (OSDI)
2.5. Statistical Analysis and Data Visualization
3. Results
3.1. Patients’ Characteristics
3.2. Confocal Microscopy of the Corneal Nerve Fibres
3.3. Clinical Evaluation of Dry Eye Symptoms and Signs
3.4. Correlation Analysis between Parameters of the Corneal Confocal Microscopy and the Clinical Evaluation of Dry Eye Symptoms and Signs
4. Discussion
4.1. Corneal Trigeminal Nerve Affection Is Similar in Neuro-Sjögren and CIDP
4.2. Dry eye Disease in Both Patient Groups
4.3. Notional Connection between Dry Eye Disease and Corneal Trigeminal Nerve Affection
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seeliger, T.; Bönig, L.; Witte, T.; Thiele, T.; Lesinski-Schiedat, A.; Stangel, M.; Lenarz, T.; Prenzler, N.C.; Skripuletz, T. Hearing dysfunction in patients with Neuro-Sjögren: A cross-sectional study. Ann. Transl. Med. 2020, 8, 1069. [Google Scholar] [CrossRef]
- Seeliger, T.; Jacobsen, L.; Hendel, M.; Bönig, L.; Prenzler, N.K.K.; Thiele, T.; Ernst, D.; Witte, T.; Stangel, M.; Kopp, B.; et al. Cognitive impairment in patients with Neuro-Sjögren. Ann. Clin. Transl. Neurol. 2020, 7, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Butryn, M.; Neumann, J.; Rolfes, L.; Bartels, C.; Wattjes, M.P.; Mahmoudi, N.; Seeliger, T.; Konen, F.F.; Thiele, T.; Witte, T.; et al. Clinical, Radiological, and Laboratory Features of Spinal Cord Involvement in Primary Sjögren’s Syndrome. J. Clin. Med. 2020, 9, 1482. [Google Scholar] [CrossRef]
- Seeliger, T.; Prenzler, N.K.; Gingele, S.; Seeliger, B.; Körner, S.; Thiele, T.; Bönig, L.; Sühs, K.-W.; Witte, T.; Stangel, M.; et al. Neuro-Sjögren: Peripheral Neuropathy With Limb Weakness in Sjögren’s Syndrome. Front. Immunol. 2019, 10, 1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren’s syndrome. Ann. Rheum. Dis. 2017, 76, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Grant, I.A.; Hunder, G.G.; Homburger, H.A.; Dyck, P.J. Peripheral neuropathy associated with sicca complex. Neurology 1997, 48, 855–892. [Google Scholar] [CrossRef]
- Pavlakis, P.; Alexopoulos, H.; Kosmidis, M.; Mamali, I.; Moutsopoulos, H.; Tzioufas, A.; Dalakas, M. Peripheral neuropathies in Sjögren’s syndrome: A critical update on clinical features and pathogenetic mechanisms. J. Autoimmun. 2012, 39, 27–33. [Google Scholar] [CrossRef]
- Seeliger, T.; Bönig, L.; Gingele, S.; Prenzler, N.K.; Thiele, T.; Ernst, D.; Witte, T.; Stangel, M.; Skripuletz, T.; Körner, S. Nerve ultrasound findings in Sjögren’s syndrome-associated neuropathy. J. Neuroimaging 2021, 31, 1156–1165. [Google Scholar] [CrossRef]
- Seeliger, T.; Gingele, S.; Bönig, L.; Konen, F.F.; Körner, S.; Prenzler, N.; Thiele, T.; Ernst, D.; Witte, T.; Stangel, M.; et al. CIDP associated with Sjögren’s syndrome. J. Neurol. 2021, 268, 2908–2912. [Google Scholar] [CrossRef]
- Yang, A.Y.; Chow, J.; Liu, J. Corneal innervation and sensation: The eye and beyond. Yale J. Biol. Med. 2018, 91, 13–21. [Google Scholar]
- Petropoulos, I.N.; Alam, U.; Fadavi, H.; Marshall, A.; Asghar, O.; Dabbah, M.A.; Chen, X.; Graham, J.; Ponirakis, G.; Boulton, A.J.M.; et al. Rapid Automated Diagnosis of Diabetic Peripheral Neuropathy With In Vivo Corneal Confocal Microscopy. Investig. Opthalmology Vis. Sci. 2014, 55, 2071–2078. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Ferdousi, M.; Kalteniece, A.; Kass-Iliyya, L.; Petropoulos, I.N.; Malik, R.A.; Kobylecki, C.; Silverdale, M. Corneal confocal microscopy detects small fibre neurodegeneration in Parkinson’s disease using automated analysis. Sci. Rep. 2020, 10, 20147. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Dong, X.; Zhou, X.; Yan, L.; Wan, Q. Corneal subbasal nerve plexus changes in patients with episodic migraine: An in vivo confocal microscopy study. J. Pain Res. 2019, ume 12, 1489–1495. [Google Scholar] [CrossRef] [Green Version]
- Flockerzi, E.; Daas, L.; Seitz, B. Structural changes in the corneal subbasal nerve plexus in keratoconus. Acta Ophthalmol. 2020, 98, e928–e932. [Google Scholar] [CrossRef] [Green Version]
- Grossman, S.A.; Krabak, M.J. Leptomeningeal carcinomatosis. Cancer Treat. Rev. 1999, 25, 103–119. [Google Scholar] [CrossRef]
- Che, N.N.; Yang, H.Q. Potential use of corneal confocal microscopy in the diagnosis of Parkinson’s dis-ease associated neuropathy. Transl. Neurodegener. 2020, 9, 28. [Google Scholar] [CrossRef]
- Bohn, S.; Stahnke, T.; Sperlich, K.; Linke, S.J.; Farrokhi, S.; Klemm, M.; Allgeier, S.; Köhler, B.; Reichert, K.-M.; Witt, M.; et al. In Vivo Histology of the Cornea—From the “Rostock Cornea Module” to the “Rostock Electronic Slit Lamp”—A Clinical “Proof of Concept” Study. Klin. Mon. Augenheilkd. 2020, 237, 1442–1454. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.L.; Tepelus, T.C.; Huang, J.; Irvine, A.G.; Irvine, C.; Chiu, G.B.; Sadda, S.R. Evaluation of the corneal epithelium in non-Sjögren’s and Sjögren’s dry eyes: An in vivo confocal microscopy study using HRT III RCM. BMC Ophthalmol. 2018, 18, 309. [Google Scholar] [CrossRef] [PubMed]
- Stettner, M.; Hinrichs, L.; Guthoff, R.; Bairov, S.; Petropoulos, I.N.; Warnke, C.; Hartung, H.-P.; Malik, R.A.; Kieseier, B.C. Corneal confocal microscopy in chronic inflammatory demyelinating polyneuropathy. Ann. Clin. Transl. Neurol. 2015, 3, 88–100. [Google Scholar] [CrossRef]
- Schneider, C.; Bucher, F.; Cursiefen, C.; Fink, G.R.; Heindl, L.M.; Lehmann, H.C. Corneal confocal microscopy detects small fiber damage in chronic inflammatory demyelinating polyneuropathy (CIDP). J. Peripher. Nerv. Syst. 2014, 19, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Pitarokoili, K.; Sturm, D.; Labedi, A.; Greiner, T.; Eitner, L.; Kumowski, N.; Enax-Krumova, E.K.; Fisse, A.L.; Maier, C.; Gold, R.; et al. Neuroimaging markers of clinical progression in chronic inflammatory demyelinating polyradiculoneuropathy. Ther. Adv. Neurol. Disord. 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheum. 2017, 76, 9–16. [Google Scholar] [CrossRef]
- Chisholm, D.M.; Mason, D.K. Labial salivary gland biopsy in Sjogren’s disease. J. Clin. Pathol. 1968, 21, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Seror, R.; Theander, E.; Brun, J.G.; Ramos-Casals, M.; Valim, V.; Dörner, T.; Bootsma, H.; Tzioufas, A.; Solans-Laqué, R.; Mandl, T.; et al. Validation of EULAR primary Sjögren’s syndrome disease activity (ESSDAI) and patient indexes (ESSPRI). Ann. Rheum. Dis. 2015, 74, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, P.Y.K.; van Doorn, P.A.; Hadden, R.D.M.; Avau, B.; Vankrunkelsven, P.; Allen, J.A.; Attarian, S.; Blomkwist-Markens, P.H.; Cornblath, D.R.; Eftimov, F.; et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint Task Force—Second revision. Eur. J. Neurol. 2021, 28, 3556–3583. [Google Scholar] [CrossRef] [PubMed]
- Delmont, E.; Manso, C.; Querol, L.; Cortese, A.; Berardinelli, A.; Lozza, A.; Belghazi, M.; Malissart, P.; Labauge, P.; Taieb, G.; et al. Autoantibodies to nodal isoforms of neurofascin in chronic inflammatory demyelinating polyneuropathy. Brain 2017, 140, 1851–1858. [Google Scholar] [CrossRef] [Green Version]
- Oliveira-Soto, L.; Efron, N. Morphology of Corneal Nerves Using Confocal Microscopy. Cornea 2001, 20, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Baudouin, C.; Aragona, P.; Van Setten, G.; Rolando, M.; Irkeç, M.; Del Castillo, J.B.; Geerling, G.; Labetoulle, M.; Bonini, S.; ODISSEY European Consensus Group members. Diagnosing the severity of dry eye: A clear and practical algorithm. Br. J. Ophthalmol. 2014, 98, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Sowmya, S.; Jayachander, D.; Kamath, V.; Rao, M.S.; Tonse, M.R.; Baliga, M.S. Evaluation of the prevalence and severity of xerophthalmia in head and neck cancers patients undergoing curative radiotherapy. Asian J. Ophthalmol. 2016, 14, 154–165. [Google Scholar] [CrossRef]
- Lemp, M.A.; Baudouin, C.; Baum, J. The definition and classification of dry eye disease: Report of the definition and classification subcommittee of the international Dry Eye WorkShop. Ocul. Surf. 2007, 5, 75–92. [Google Scholar]
- Abusharha, A.A. Changes in blink rate and ocular symptoms during different reading tasks. Clin. Optom. 2017, ume 9, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Doughty, M.J. Spontaneous eyeblink activity under different conditions of gaze (eye position) and visual glare. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- DIAGNOSIS—Clinical TESTS—Ocular Surface Center Berlin. Available online: https://oscb-berlin.org/e-diagnosis-overview#Conjunctival-Redness-Index. (accessed on 26 September 2021).
- Abelson, M.B.; Smith, L.M.; Hollander, D.A.; Usner, D. How Do You Quantify The Qualitative? Rev. Ophthalmol. 2016, 13, 48–51. [Google Scholar]
- Xiao, J.; Adil, M.Y.; Chen, X.; Utheim, A.; Ræder, S.; Tønseth, K.A.; Lagali, N.S.; Dartt, D.A.; Utheim, T.P. Functional and Morphological Evaluation of Meibomian Glands in the Assessment of Meibomian Gland Dysfunction Subtype and Severity. Am. J. Ophthalmol. 2020, 209, 160–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walt, J.G.; Rowe, M.; Stern, K. Evaluating the functional impact of dry eye: The Ocular Surface Disease Index. Drug Inf. J. 1997, 31, 1436. [Google Scholar]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Tavakoli, M.; Ferdousi, M.; Petropoulos, I.N.; Morris, J.; Pritchard, N.; Zhivov, A.; Ziegler, D.; Pacaud, D.; Romanchuk, K.; Perkins, B.A.; et al. Normative Values for Corneal Nerve Morphology Assessed Using Corneal Confocal Microscopy: A Multinational Normative Data Set. Diabetes Care 2015, 38, 838–843. [Google Scholar] [CrossRef] [Green Version]
- Bitirgen, G.; Turkmen, K.; Malik, R.A.; Ozkagnici, A.; Zengin, N. Corneal confocal microscopy detects corneal nerve damage and increased dendritic cells in Fabry disease. Sci. Rep. 2018, 8, 12244. [Google Scholar] [CrossRef]
- Labbé, A.; Liang, Q.; Wang, Z.; Zhang, Y.; Xu, L.; Baudouin, C.; Sun, X. Corneal Nerve Structure and Function in Patients With Non-Sjögren Dry Eye: Clinical Correlations. Investig. Opthalmology Vis. Sci. 2013, 54, 5144–5150. [Google Scholar] [CrossRef] [Green Version]
- Villani, E.; Galimberti, D.; Viola, F.; Mapelli, C.; Ratiglia, R. The Cornea in Sjögren’s Syndrome: An In Vivo Confocal Study. Investig. Opthalmology Vis. Sci. 2007, 48, 2017–2022. [Google Scholar] [CrossRef] [PubMed]
- McNamara, N.A.; Ge, S.; Lee, S.M.; Enghauser, A.M.; Kuehl, L.; Chen, F.Y.-T.; Gallup, M.; McKown, R.L. Reduced Levels of Tear Lacritin Are Associated With Corneal Neuropathy in Patients With the Ocular Component of Sjögren’s Syndrome. Investig. Opthalmology Vis. Sci. 2016, 57, 5237–5243. [Google Scholar] [CrossRef]
- Perkins, B.A.; Lovblom, L.E.; Bril, V.; Scarr, D.; Ostrovski, I.; Orszag, A.; Edwards, K.; Pritchard, N.; Russell, A.; Dehghani, C.; et al. Corneal confocal microscopy for identification of diabetic sensorimotor polyneuropathy: A pooled multinational consortium study. Diabetologia 2018, 61, 1856–1861. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Zhang, Q.; Ying, X.; He, J.; Jin, Y.; Xu, H.; Cheng, Y.; Zhao, M. Corneal nerve structure in patients with primary Sjögren’s syndrome in China. BMC Ophthalmol. 2021, 21, 211. [Google Scholar] [CrossRef] [PubMed]
- Tepelus, T.C.; Chiu, G.B.; Huang, J.; Huang, P.; Sadda, S.R.; Irvine, J.; Lee, O.L. Correlation between corneal innervation and inflammation evaluated with confocal microscopy and symptomatology in patients with dry eye syndromes: A preliminary study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 1771–1778. [Google Scholar] [CrossRef]
- Sturm, D.; Schmidt-Wilcke, T.; Greiner, T.; Maier, C.; Schargus, M.; Tegenthoff, M.; Vorgerd, M. Confocal Cornea Microscopy Detects Involvement of Corneal Nerve Fibers in a Patient with Light-Chain Amyloid Neuropathy Caused by Multiple Myeloma: A Case Report. Case Rep. Neurol. 2016, 8, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Bucher, F.; Schneider, C.; Blau, T.; Cursiefen, C.; Fink, G.R.; Lehmann, H.C.; Heindl, L.M. Small-Fiber Neuropathy Is Associated With Corneal Nerve and Dendritic Cell Alterations. Cornea 2015, 34, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Niederer, R.L.; Perumal, D.; Sherwin, T.; McGhee, C.N.J. Age-related differences in the normal human cornea: A laser scanning in vivo confocal microscopy study. Br. J. Ophthalmol. 2007, 91, 1165–1169. [Google Scholar] [CrossRef] [Green Version]
- Cardigos, J.; Barcelos, F.; Carvalho, H.; Hipólito, D.; Crisóstomo, S.; Vaz-Patto, J.; Alves, N. Tear Meniscus and Corneal Sub-basal Nerve Plexus Assessment in Primary Sjögren Syndrome and Sicca Syndrome Patients. Cornea 2019, 38, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.; Bunya, V.; Maguire, M.; Asbell, P.; Ying, G.-S. Systemic Conditions Associated with Severity of Dry Eye Signs and Symptoms in the Dry Eye Assessment and Management Study. Ophthalmology 2021, 128, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Ismail, O.M.; Poole, Z.B.; Bierly, S.L.; Van Buren, E.D.; Lin, F.-C.; Meyer, J.J.; Davis, R.M. Association Between Dry Eye Disease and Migraine Headaches in a Large Population-Based Study. JAMA Ophthalmol. 2019, 137, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Delalande, S.; de Seze, J.; Fauchais, A.-L.; Hachulla, E.; Stojkovic, T.; Ferriby, D.; Dubucquoi, S.; Pruvo, J.-P.; Vermersch, P.; Hatron, P.-Y. Neurologic manifestations in primary Sjögren syndrome: A study of 82 pa-tients. Medicine 2004, 83, 280–291. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, F.; Moreira, I.; Silva, A.M.; Vasconcelos, C.; Farinha, F.; Santos, E. Neurological involvement in Primary Sjögren Syndrome. Acta Reum. Port. 2013, 38, 29–36. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 0 | 1 | 2 | 3 | |
|---|---|---|---|---|
| Conjunctival Injection [33] | none | mild | moderate | severe |
| Tear Film Breakup Time | >10 s | ≤10 s | ≤5 s | immediate |
| Blink Frequency | ≤21/min | >21/min | ||
| Schirmer’s test (mm/5 min) | >10 | ≤10 | ≤5 | ≤2 |
| Superficial Punctate Keratitis (National Eye Institute Score) [34] | Grade 0 | Grade 1 | Grade 2 | Grade 3 |
| Meibomian Gland Dysfunction [35] | none | mild | moderate | severe |
| Neuro-Sjögren | CIDP | Controls | |
|---|---|---|---|
| n | 26 | 29 | 6 |
| Age at evaluation, median (IQR) (years) | 64 (56–72) | 67 (60–74) | 61 (60–64) |
| Female, n (%) | 15 (58%) | 6 (21%) | 5 (83%) |
| Disease duration, median (IQR) (years) | 7 (2–18) | 9 (4–10) | n/a |
| ACR/ EULAR classification criteria | |||
| Objective xerophthalmia, n (%) | 20 (77%) | 7 (24%) | n/a |
| Objective xerostomia, n (%) | 12 (46%) | 8 (28%) | n/a |
| SSA(Ro) antibody positivity, n (%) | 11 (42%) | 0 (0%) | n/a |
| Sialadenitis grade 3/4 by Chisholm and Mason, n (%) | 21/22 (95%) | 0/10 (0%) | n/a |
| Focus Score, median (IQR) | 4 (4–5) | 0 (0–1) | n/a |
| ESSDAI, median (IQR) | 17 (11–22) | n/a | n/a |
| ESSPRI, median (IQR) | 3.2 (2.3–4.8) | n/a | n/a |
| n (%) | |
|---|---|
| Clinical feature of peripheral nerve affection | |
| Cranial nerve impairment | 9 (35%) |
| Small Fibre Neuropathy | 2 (8%) |
| Motor impairment | 21 (81%) |
| Sensory deficits | 21 (81%) |
| ● Pain | 4 (19%) |
| ● Paresthesia | 12 (57%) |
| ● Sensory ataxia | 13 (62%) |
| Autonomic dysfunction | 4 (16%) |
| Nerve damage pattern on pathological nerve conduction studies (n = 24) | |
| SSB(La)-antibody positivity | 3 (12%) |
| Cryoglobulins | 0 (0%) |
| Additional serological parameters | |
| SSB(La)-antibody positivity | 3 (12%) |
| Cryoglobulins | 0 (0%) |
| Free Kappa Light Chains, median (IQR) (mg/L) | 19 (21.1–21.5) |
| Free Lambda Light Chains, median (IQR) (mg/L) | 19.7 (11.4–22.3) |
| Kappa/Lambda ratio, median (IQR) | (0.81–1.21) |
| Analysis without Subgroup Division | Left | Right |
|---|---|---|
| Clinical score, mean ± standard deviation | 4 (3–6.5) | 4 (3–6.5) |
| OSDI | 12.5 (4.2–25) | |
| Correlation analysis | p-values (left) | p-values (right) |
| Clinical Score vs. OSDI | 0.005 | 0.002 |
| Clinical Score vs. | ||
| Corneal Nerve Fibre Density | 0.34 | 0.6 |
| Corneal Nerve Fibre Main Branch Density | 0.44 | 0.88 |
| Corneal Nerve Fibre Length (total length of nerves) | 0.13 | 0.41 |
| Corneal Nerve Fibre Total Branch Density | 0.66 | 0.74 |
| OSDI vs. | ||
| Corneal Nerve Fibre Density | 0.50 | 0.68 |
| Corneal Nerve Fibre Main Branch Density | 0.40 | 0.48 |
| Corneal Nerve Fibre Length (total length of nerves) | 0.14 | 0.42 |
| Corneal Nerve Fibre Total Branch Density | 0.08 | 0.30 |
| Reference | Patients | Controls | ||||||
|---|---|---|---|---|---|---|---|---|
| Patients’ Condition, n | Median Age | Corneal Nerve Fibre Density, Mean ± SD (fibres/mm2) | Corneal Nerve Fibre Length, Mean ± SD (mm/mm2) | n | Median Age | Corneal Nerve Fibre Density, Mean ± SD (fibres/mm2) | Corneal Nerve Fibre Length, Mean ± SD (mm/mm2) | |
| [39] | Behçet’s disease, 49 | 39.9 | 27.7 ± 8.6 | 16.3 ± 4.6 | 30 | 41.2 | 35.6 ± 10 | 18.5 ± 4.1 |
| [40] | Dry eye disease, 43 | 46.2 | 34.9 ± 8.1 | 16.26 ± 3.5 | 14 | 45.4 | 45.9 ± 4.2 | 21.86 ± 2.1 |
| [42] | Sjögren’s syndrome, 10 | 58.2 | 21.7 ± 18.9 | 4.18 ± 3.4 | 10 | 56.5 | 31.8 ± 9.3 | 6.54 ± 2.47 |
| [49] | Sjögren’s syndrome with dry eye disease, 54 | 57.8 | 28.1 ± 12.2 | 10.3 ± 6.6 | 20 | 50.9 | 43.9 ± 12.9 | 15.4 ± 5.1 |
| [43] | Diabetes, 998 | 52 | 20.6 ± 9.8 | 12.5 ± 4.6 | - | - | - | - |
| [19] | CIDP, 88 | n/a | 19 ± 7 | 12 ± 3 | 85 | n/a | 29 ± 6 | 17 ± 3 |
| MMN, 6 | n/a | 18 ± 11 | 11 ± 5 | |||||
| MGUSN, 12 | n/a | 20 ± 5 | 12 ± 2 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seeliger, T.; Gehlhaar, M.A.; Oluwatoba-Popoola, I.; Konen, F.F.; Haar, M.; Donicova, E.; Wachsmann, M.; Pielen, A.; Gingele, S.; Prenzler, N.K.; et al. Trigeminal Nerve Affection in Patients with Neuro-Sjögren Detected by Corneal Confocal Microscopy. J. Clin. Med. 2022, 11, 4484. https://doi.org/10.3390/jcm11154484
Seeliger T, Gehlhaar MA, Oluwatoba-Popoola I, Konen FF, Haar M, Donicova E, Wachsmann M, Pielen A, Gingele S, Prenzler NK, et al. Trigeminal Nerve Affection in Patients with Neuro-Sjögren Detected by Corneal Confocal Microscopy. Journal of Clinical Medicine. 2022; 11(15):4484. https://doi.org/10.3390/jcm11154484
Chicago/Turabian StyleSeeliger, Tabea, Marten A. Gehlhaar, Irene Oluwatoba-Popoola, Franz F. Konen, Melanie Haar, Emilia Donicova, Marija Wachsmann, Amelie Pielen, Stefan Gingele, Nils K. Prenzler, and et al. 2022. "Trigeminal Nerve Affection in Patients with Neuro-Sjögren Detected by Corneal Confocal Microscopy" Journal of Clinical Medicine 11, no. 15: 4484. https://doi.org/10.3390/jcm11154484
APA StyleSeeliger, T., Gehlhaar, M. A., Oluwatoba-Popoola, I., Konen, F. F., Haar, M., Donicova, E., Wachsmann, M., Pielen, A., Gingele, S., Prenzler, N. K., Ernst, D., Witte, T., Framme, C., Bajor, A., & Skripuletz, T. (2022). Trigeminal Nerve Affection in Patients with Neuro-Sjögren Detected by Corneal Confocal Microscopy. Journal of Clinical Medicine, 11(15), 4484. https://doi.org/10.3390/jcm11154484