


Micro-CT Evaluation of Different Root Canal Irrigation Protocols on the Removal of Accumulated Hard Tissue Debris: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
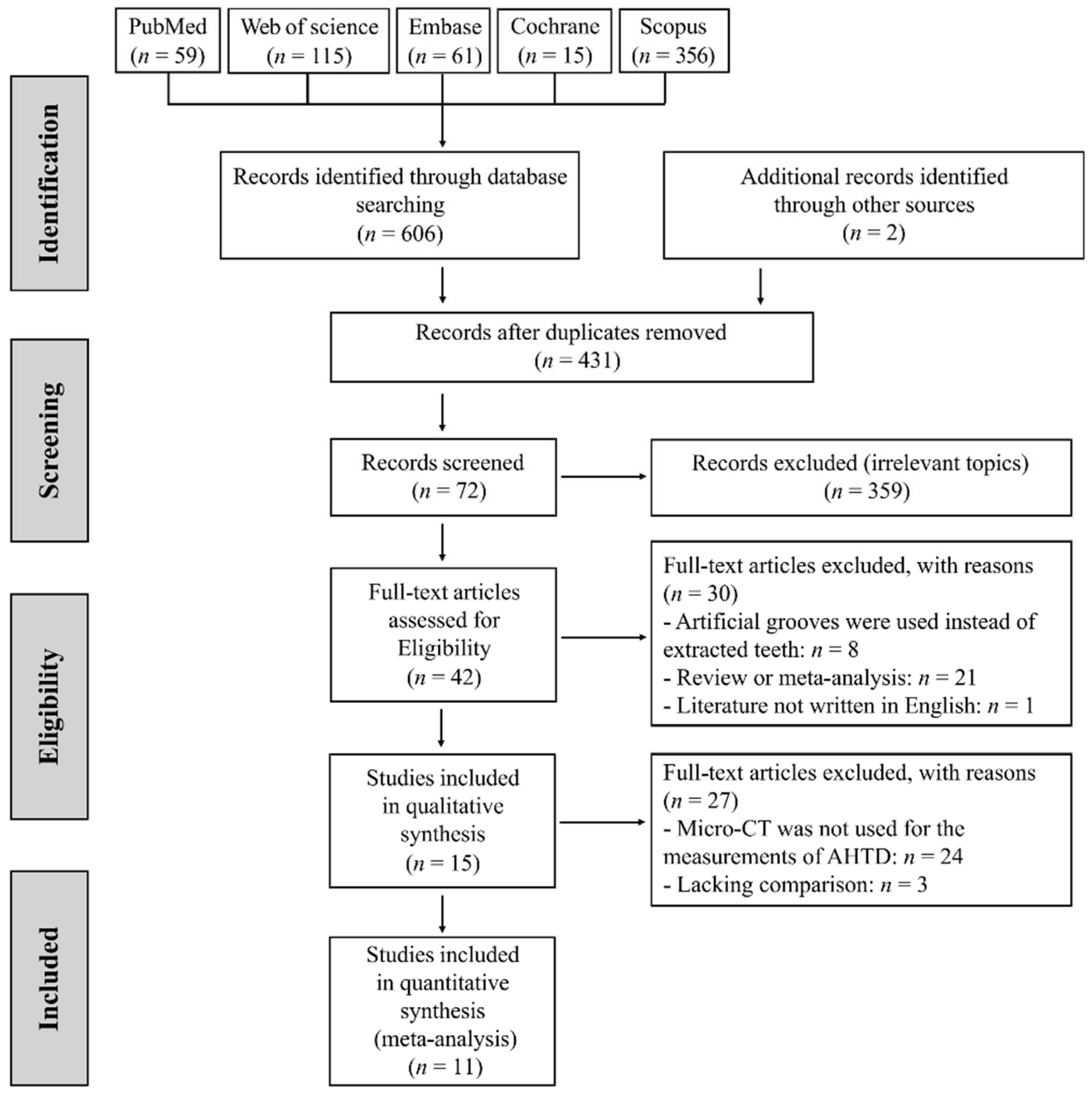
2.1. Search Strategy
2.2. Eligibility Criteria
- The subjects were extracted human teeth with complete root formation and no obvious root caries, root crack or root absorption.
- The root canal was cleaned with the irrigation protocols as described in the Introduction.
- AHTD in the root canal was evaluated by micro-CT before and after adjunctive root canal irrigation.
- The percentage reduction in AHTD after irrigation could be obtained directly or indirectly from the outcomes of interest.
- The study was an observational study.
- The study was published in English.
- Full-text article was not available.
- Artificial grooves or animal models were used as subjects.
- Lacking comparison with PUI in the study.
- Case reports, review articles and critical appraisal articles.
2.3. Study Selection and Data Collection
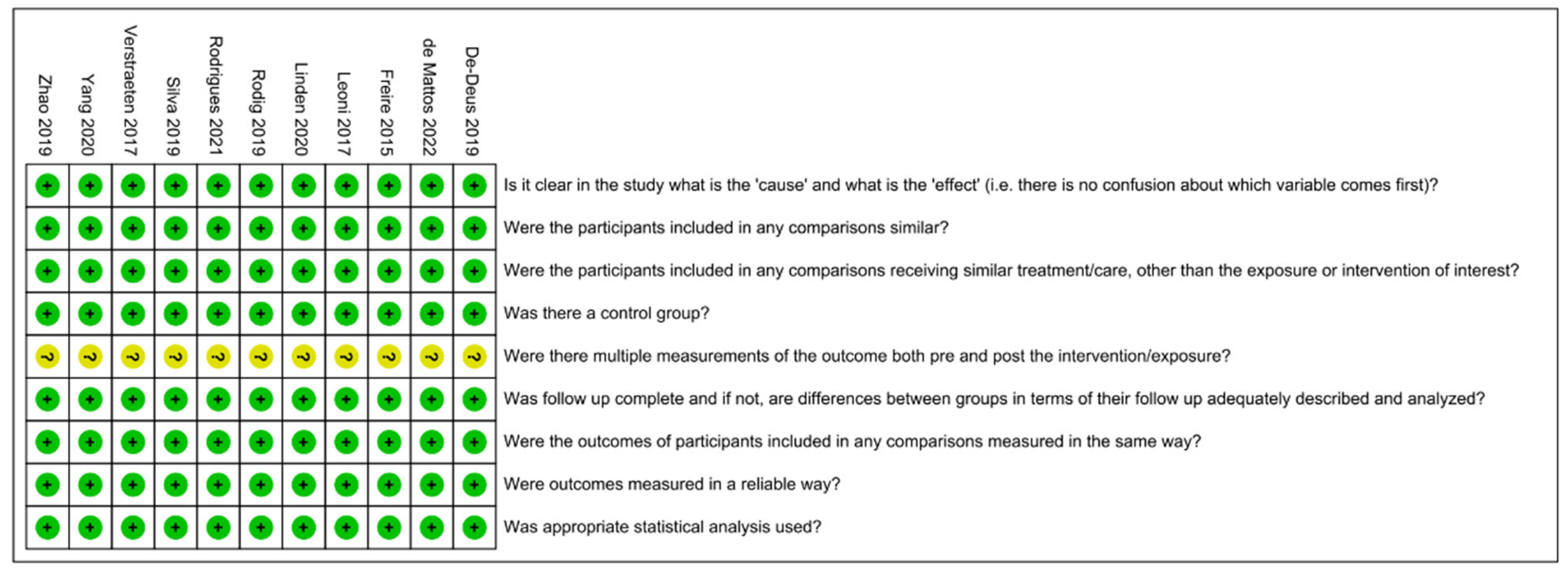
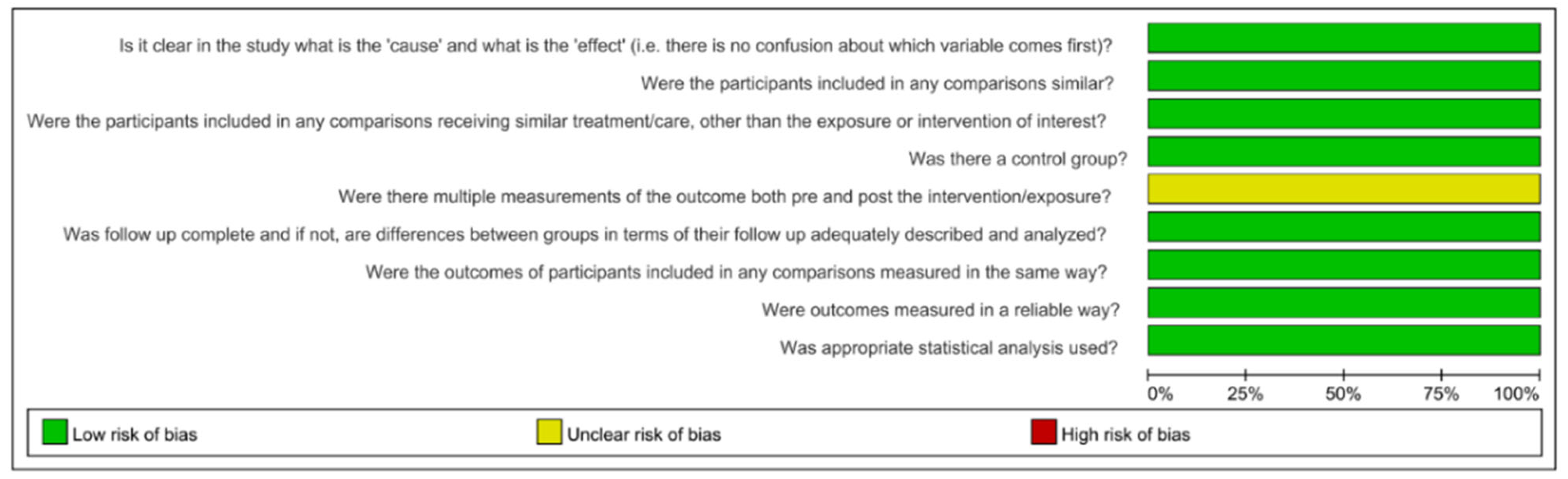
2.4. Quality Assessment
2.5. Statistical Analysis
2.6. Grading of the Evidence
3. Results
3.1. Characteristics of the Included Studies
3.2. Risk-of-Bias Judgement of Eligible Studies
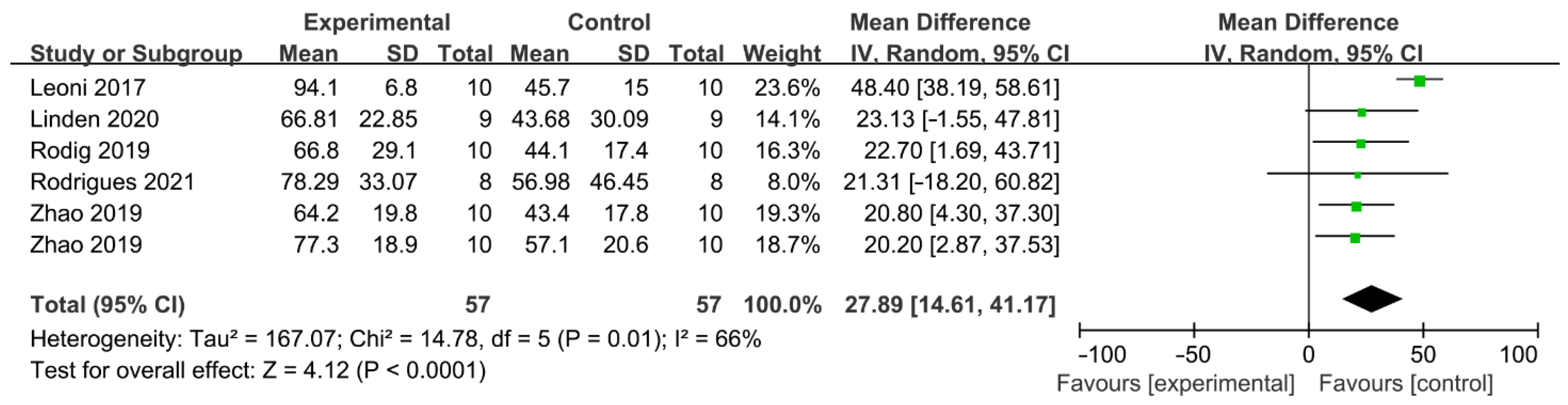
3.3. Outcomes of the Meta-Analysis and Publication Bias
3.3.1. Passive Ultrasonic Irrigation System
3.3.2. Negative Pressure Irrigation System
3.3.3. Sonically Activated Irrigation System
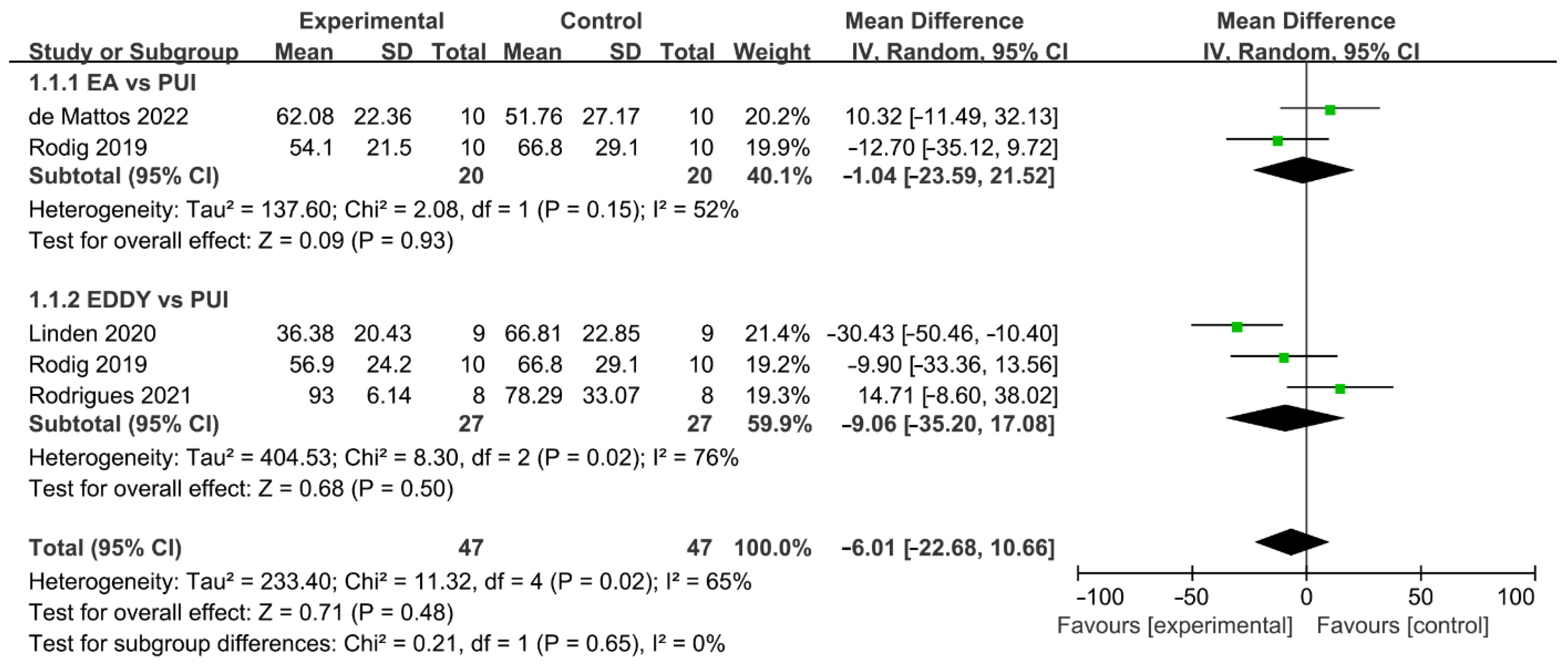
3.3.4. Mechanical-Activated Irrigation System
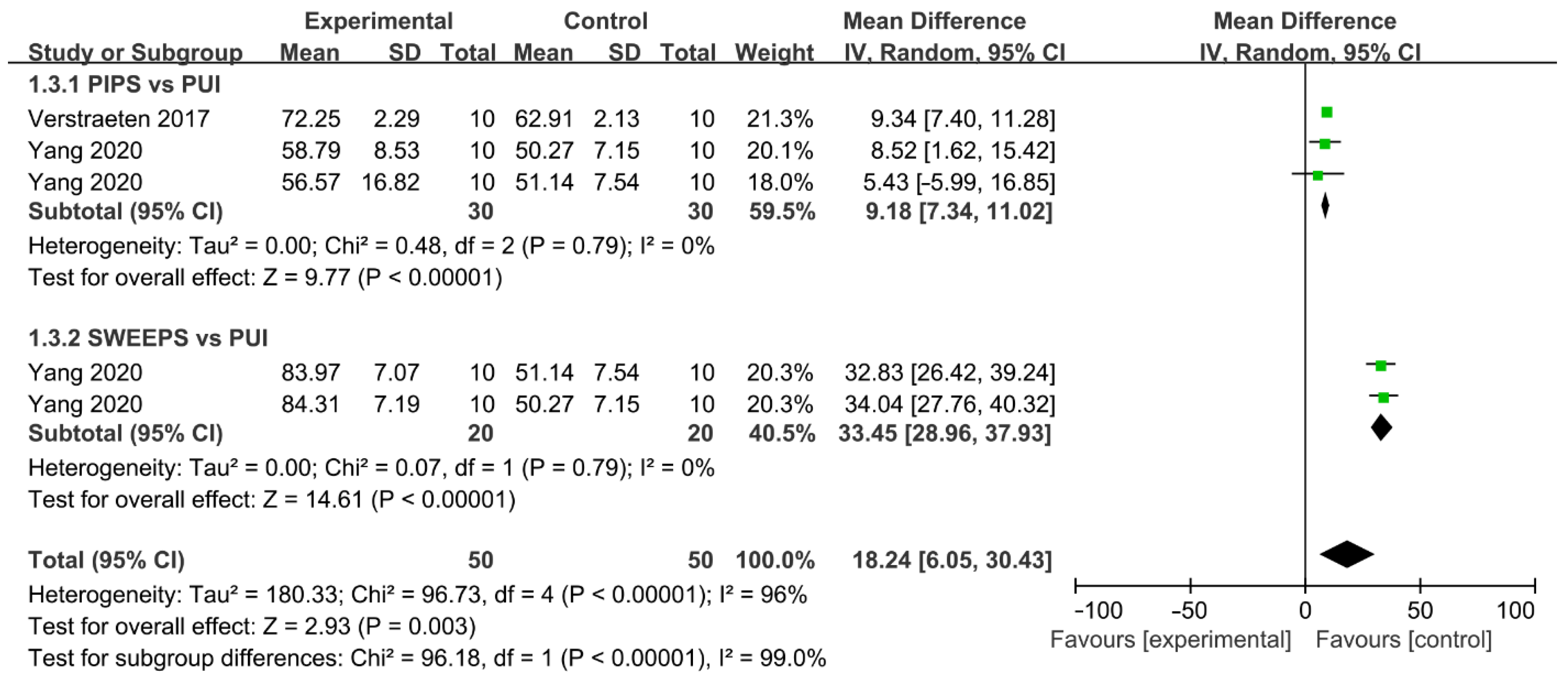
3.3.5. Laser-Activated Irrigation System
3.4. Grading of the Evidence
4. Discussion
4.1. Summary of the Main Results
4.2. Overall Completeness and Applicability of Evidence
4.3. Agreements and Disagreements with Other Studies or Reviews
4.3.1. Irrigation Protocols
- Passive ultrasonic irrigation (PUI)
- EndoVac
- Sonically Activated Irrigation (SAI)
- Self-adjusting File (SAF)
- XP-endo Finisher (XPF)
- PIPS
4.3.2. Complexity of Root Canal Anatomy
4.3.3. Application of Root Canal Irrigants
4.4. Strengths and Limitations
5. Prospective
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paqué, F.; Al-Jadaa, A.; Kfir, A. Hard-tissue debris accumulation created by conventional rotary versus self-adjusting file instrumentation in mesial root canal systems of mandibular molars. Int. Endod. J. 2012, 45, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Paqué, F.; Boessler, C.; Zehnder, M. Accumulated hard tissue debris levels in mesial roots of mandibular molars after sequential irrigation steps. Int. Endod. J. 2011, 44, 148–153. [Google Scholar] [CrossRef]
- Guerreiro, M.Y.R.; Belladonna, F.G.; Monteiro, L.P.B.; Lima, C.O.; Silva, E.; Brandão, J.M.S. The influence of the addition of surfactants to sodium hypochlorite on the removal of hard tissue debris. Int. Endod. J. 2020, 53, 1131–1139. [Google Scholar] [CrossRef]
- Faus-Llacer, V.; Luna-Roa, M.; Faus-Matoses, I.; Ruiz-Sanchez, C.; Zubizarreta-Macho, A.; Sauro, S.; Faus-Matoses, V. Comparative Analysis of the Smear Layer Removal Capability between EndoVac and Endoactivator Endodontic Irrigation Systems at the Root Canal System and Isthmus: A Micro-Computed Tomography Analysis. Appl. Sci. 2020, 10, 7033. [Google Scholar] [CrossRef]
- Xu, K.; Wang, J.; Wang, K.; Gen, N.; Li, J. Micro-computed tomographic evaluation of the effect of the final apical size prepared by rotary nickel-titanium files on the removal efficacy of hard-tissue debris. J. Int. Med. Res. 2018, 46, 2219–2229. [Google Scholar] [CrossRef] [Green Version]
- Aminoshariae, A.; Kulild, J.C. Master apical file size—Smaller or larger: A systematic review of healing outcomes. Int. Endod. J. 2015, 48, 639–647. [Google Scholar] [CrossRef]
- Perez, R.; Neves, A.A.; Belladonna, F.G.; Silva, E.; Souza, E.M.; Fidel, S.; Versiani, M.A.; Lima, I.; Carvalho, C.; De-Deus, G. Impact of needle insertion depth on the removal of hard-tissue debris. Int. Endod. J. 2017, 50, 560–568. [Google Scholar] [CrossRef]
- Huang, Q.; Barnes, J.B.; Schoeffel, G.J.; Fan, B.; Tay, C.; Bergeron, B.E.; Susin, L.F.; Ling, J.Q.; Niu, L.N.; Tay, F.R. Effect of Canal Anastomosis on Periapical Fluid Pressure Build-up during Needle Irrigation in Single Roots with Double Canals using a Polycarbonate Model. Sci. Rep. 2017, 7, 1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, R.N.; Brady, J.M.; Bernier, W.E. Efficacy of ultrasonic cleaning. J. Endod. 1980, 6, 740–743. [Google Scholar] [CrossRef]
- Ahmad, M.; Pitt Ford, T.R.; Crum, L.A. Ultrasonic debridement of root canals: An insight into the mechanisms involved. J. Endod. 1987, 13, 93–101. [Google Scholar] [CrossRef]
- Agarwal, A.; Deore, R.B.; Rudagi, K.; Nanda, Z.; Baig, M.O.; Fareez, M.A. Evaluation of Apical Vapor Lock Formation and comparative Evaluation of its Elimination using Three different Techniques: An in vitro Study. Contemp. Dent. Pr. 2017, 18, 790–794. [Google Scholar] [CrossRef]
- Versiani, M.A.; Alves, F.R.; Andrade-Junior, C.V.; Marceliano-Alves, M.F.; Provenzano, J.C.; Rôças, I.N.; Sousa-Neto, M.D.; Siqueira, J.F., Jr. Micro-CT evaluation of the efficacy of hard-tissue removal from the root canal and isthmus area by positive and negative pressure irrigation systems. Int. Endod. J. 2016, 49, 1079–1087. [Google Scholar] [CrossRef]
- Amaral, R.R.; Oliveira, A.G.G.; Braga, T.; Reher, P.; Farias, L.D.M.; Magalhães, P.P.; Ferreira, P.G.; Côrtes, M.I.D.S. Quantitative Assessment of the Efficacy of Two Different Single-file Systems in Reducing the Bacterial load in Oval-Shaped Canals: A Clinical Study. J. Endod. 2020, 46, 1228–1234. [Google Scholar] [CrossRef]
- Galler, K.M.; Grubmüller, V.; Schlichting, R.; Widbiller, M.; Eidt, A.; Schuller, C.; Wölflick, M.; Hiller, K.A.; Buchalla, W. Penetration depth of irrigants into root dentine after sonic, ultrasonic and photoacoustic activation. Int. Endod. J. 2019, 52, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Liu, M.W.; Zhu, L.X.; Peng, B. Micro-CT study on the removal of accumulated hard-tissue debris from the root canal system of mandibular molars when using a novel laser-activated irrigation approach. Int. Endod. J. 2020, 53, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Kirmizi, D.; Aksoy, U.; Orhan, K. Efficacy of Laser-Activated Irrigation and Conventional Techniques in Calcium Hydroxide Removal from Simulated Internal Resorption Cavities: Micro-CT Study. Photobiomodul. Photo. Med. Laser Surg. 2021, 39, 674–681. [Google Scholar] [CrossRef]
- Mancini, M.; Cerroni, L.; Iorio, L.; Dall’Asta, L.; Cianconi, L. FESEM evaluation of smear layer removal using different irrigant activation methods (EndoActivator, EndoVac, PUI and LAI). An in vitro study. Clin. Oral Investig. 2018, 22, 993–999. [Google Scholar] [CrossRef]
- McKendry, D.J. Comparison of balanced forces, endosonic, and step-back filing instrumentation techniques: Quantification of extruded apical debris. J. Endod. 1990, 16, 24–27. [Google Scholar] [CrossRef]
- Vansan, L.P.; Pécora, J.D.; Costa, W.F.; Maia Campos, G. Effects of various irrigating solutions on the cleaning of the root canal with ultrasonic instrumentation. Braz. Dent. J. 1990, 1, 37–44. [Google Scholar]
- Vinhorte, M.C.; Suzuki, E.H.; de Carvalho, M.S.; Marques, A.A.F.; Júnior, E.C.S.; Garcia, L.d.F.R. Effect of passive ultrasonic agitation during final irrigation on cleaning capacity of hybrid instrumentation. Restor Dent. Endod. 2014, 39, 104–108. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, J.F.; Araújo, M.C.P.; Garcia, P.F.; Fraga, R.C.; Dantas, C.J.S. Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canals. J. Endod. 1997, 23, 499–502. [Google Scholar] [CrossRef]
- Merigo, E.; Bufflier, P.; Rocca, J.P.; Chevalier, M.; Medioni, E.; Meng, Z.; Fornaini, C. Bactericidal effect of Er,Cr:YSGG laser irradiation on endodontic biofilm: An ex vivo study. J. Photochem. Photobiol. B 2021, 218, 112185. [Google Scholar] [CrossRef] [PubMed]
- Caron, G.; Nham, K.; Bronnec, F.; Machtou, P. Effectiveness of Different Final lrrigant Activation Protocols on Smear Layer Removal in Curved Canals. J. Endod. 2010, 36, 1361–1366. [Google Scholar] [CrossRef] [PubMed]
- Dadresanfar, B.; Khalilak, Z.; Delvarani, A.; Mehrvarzfar, P.; Vatanpour, M.; Pourassadollah, M. Effect of ultrasonication with EDTA or MTAD on smear layer, debris and erosion scores. J. Oral Sci. 2011, 53, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De-Deus, G.; Reis, C.; Paciornik, S. Critical appraisal of published smear layer-removal studies: Methodological issues. Oral Surg Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 531–543. [Google Scholar] [CrossRef]
- Leonardi, D.P.; Sydney, G.B.; Tanomaru, M.F.; Baratto-Filho, F.; Baratto, S.S.; Cerri, P.S. Performance of RaCe instrumentation system in curved root canals: A comprehensive analysis by three study methods. Braz. Dent. J. 2013, 24, 230–234. [Google Scholar] [CrossRef] [Green Version]
- Andreani, Y.; Gad, B.T.; Cocks, T.C.; Harrison, J.; Keresztes, M.E.; Pomfret, J.K.; Rees, E.B.; Ma, D.; Baloun, B.L.; Rahimi, M. Comparison of irrigant activation devices and conventional needle irrigation on smear layer and debris removal in curved canals. (Smear layer removal from irrigant activation using SEM). Aust. Endod. J. 2021, 47, 143–149. [Google Scholar] [CrossRef]
- Jung, M.; Lommel, D.; Klimek, J. The imaging of root canal obturation using micro-CT. Int. Endod. J. 2005, 38, 617–626. [Google Scholar] [CrossRef]
- Freire, L.G.; Iglecias, E.F.; Cunha, R.S.; Dos Santos, M.; Gavini, G. Micro-Computed Tomographic Evaluation of Hard Tissue Debris Removal after Different Irrigation Methods and Its Influence on the Filling of Curved Canals. J. Endod. 2015, 41, 1660–1666. [Google Scholar] [CrossRef]
- Paqué, F.; Laib, A.; Gautschi, H.; Zehnder, M. Hard-Tissue Debris Accumulation Analysis by High-Resolution Computed Tomography Scans. J. Endod. 2009, 35, 1044–1047. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, J.F., Jr.; Pérez, A.R.; Marceliano-Alves, M.F.; Provenzano, J.C.; Silva, S.G.; Pires, F.R.; Vieira, G.C.S.; Rôças, I.N.; Alves, F.R.F. What happens to unprepared root canal walls: A correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int. Endod. J. 2018, 51, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Angerame, D.; De Biasi, M.; Pecci, R.; Bedini, R. Filling ability of three variants of the single-cone technique with bioceramic sealer: A micro-computed tomography study. J. Mater. Sci. Mater. Med. 2020, 31, 91. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. BMJ (Clin. Res. Ed.) 2009, 21, b2700. [Google Scholar] [CrossRef] [Green Version]
- Kirwan, J.R.; Bijlsma, J.W.; Boers, M.; Shea, B.J. Effects of glucocorticoids on radiological progression in rheumatoid arthritis. Cochrane Database Syst. Rev. 2007, 2007, Cd006356. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.T.; EzEldeen, M.; Jacobs, R.; Lambrechts, P.; Alcalde, M.P.; Duarte, M.A.H. Cleaning efficacy and uncontrolled removal of dentin of two methods of irrigant activation in curved canals connected by an isthmus. Aust. Endod. J. 2021, 47, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Linden, D.; Boone, M.; De Bruyne, M.; De Moor, R.; Versiani, M.A.; Meire, M. Adjunctive Steps for the Removal of Hard Tissue Debris from the Anatomic Complexities of the Mesial Root Canal System of Mandibular Molars: A Micro-Computed Tomographic Study. J. Endod. 2020, 46, 1508–1514. [Google Scholar] [CrossRef]
- Zhao, Y.; Fan, W.; Xu, T.; Tay, F.R.; Gutmann, J.L.; Fan, B. Evaluation of several instrumentation techniques and irrigation methods on the percentage of untouched canal wall and accumulated dentine debris in C-shaped canals. Int. Endod. J. 2019, 52, 1354–1365. [Google Scholar] [CrossRef]
- Silva, E.; Carvalho, C.R.; Belladonna, F.G.; Prado, M.C.; Lopes, R.T.; De-Deus, G.; Moreira, E.J.L. Micro-CT evaluation of different final irrigation protocols on the removal of hard-tissue debris from isthmus-containing mesial root of mandibular molars. Clin. Oral Investig. 2019, 23, 681–687. [Google Scholar] [CrossRef]
- Rödig, T.; Koberg, C.; Baxter, S.; Konietschke, F.; Wiegand, A.; Rizk, M. Micro-CT evaluation of sonically and ultrasonically activated irrigation on the removal of hard-tissue debris from isthmus-containing mesial root canal systems of mandibular molars. Int. Endod. J. 2019, 52, 1173–1181. [Google Scholar] [CrossRef]
- De-Deus, G.; Belladonna, F.G.; Zuolo, A.D.S.; Perez, R.; Carvalho, M.S.; Souza, E.M.; Lopes, R.T.; Silva, E. Micro-CT comparison of XP-endo Finisher and passive ultrasonic irrigation as final irrigation protocols on the removal of accumulated hard-tissue debris from oval shaped-canals. Clin. Oral Investig. 2019, 23, 3087–3093. [Google Scholar] [CrossRef]
- Verstraeten, J.; Jacquet, W.; De Moor, R.J.G.; Meire, M.A. Hard tissue debris removal from the mesial root canal system of mandibular molars with ultrasonically and laser-activated irrigation: A micro-computed tomography study. Lasers Med. Sci. 2017, 32, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Leoni, G.B.; Versiani, M.A.; Silva-Sousa, Y.T.; Bruniera, J.F.; Pécora, J.D.; Sousa-Neto, M.D. Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int. Endod. J. 2017, 50, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Araujo, B.M.D.M.d.; Cruz, A.T.G.; Piasecki, L.; Webber, M.; Carneiro, E.; Westphalen, V.P.D.; da Silva Neto, U.X. Micro-CT evaluation of four final irrigation protocols on hard-tissue debris removal from mesial roots of mandibular molars containing isthmus. Clin Oral Investig. 2022, 26, 6121–6128. [Google Scholar] [CrossRef] [PubMed]
- Mozo, S.; Llena, C.; Forner, L. Review of ultrasonic irrigation in endodontics: Increasing action of irrigating solutions. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e512–e516. [Google Scholar] [CrossRef] [Green Version]
- Cameron, J.A. The choice of irrigant during hand instrumentation and ultrasonic irrigation of the root canal: A scanning electron microscope study. Aust. Dent. J. 1995, 40, 85–90. [Google Scholar] [CrossRef]
- Huque, J.; Kota, K.; Yamaga, M.; Iwaku, M.; Hoshino, E. Bacterial eradication from root dentine by ultrasonic irrigation with sodium hypochlorite. Int. Endod. J. 1998, 31, 242–250. [Google Scholar] [CrossRef]
- Middha, M.; Sangwan, P.; Tewari, S.; Duhan, J. Effect of continuous ultrasonic irrigation on postoperative pain in mandibular molars with nonvital pulps: A randomized clinical trial. Int. Endod. J. 2017, 50, 522–530. [Google Scholar] [CrossRef]
- Susila, A.; Minu, J. Activated Irrigation vs. Conventional non-activated Irrigation in Endodontics—A Systematic Review. Eur. Endod. J. 2019, 4, 96–110. [Google Scholar] [CrossRef]
- Capar, I.D.; Aydinbelge, H.A. Effectiveness of Various Irrigation Activation Protocols and the Self-Adjusting File System on Smear Layer and Debris Removal. Scanning 2014, 36, 640–647. [Google Scholar] [CrossRef]
- Yilmaz, M.; Yilmaz, S.; Dumani, A.; Kuden, C.; Yoldas, O. Effects of Seven Different Irrigation Techniques on Debris and the Smear Layer: A Scanning Electron Microscopy Study. Niger. J. Clin. Pr. 2017, 20, 328–334. [Google Scholar] [CrossRef] [Green Version]
- Karade, P.; Chopade, R.; Patil, S.; Hoshing, U.; Rao, M.; Rane, N.; Chopade, A.; Kulkarni, A. Efficiency of Different Endodontic Irrigation and Activation Systems in Removal of the Smear Layer: A Scanning Electron Microscopy Study. Iran. Endod. J. 2017, 12, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Jamleh, A.; Suda, H.; Adorno, C.G. Irrigation effectiveness of continuous ultrasonic irrigation system: An ex vivo study. Dent. Mater. J. 2018, 37, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbosa-Ribeiro, M.; Arruda-Vasconcelos, R.; Fabretti, F.L.; Silva, E.; De-Deus, G.; Gomes, B. Evaluation of Apically Extruded Debris Using Positive and Negative Pressure Irrigation Systems in Association with Different Irrigants. Braz. Dent. J. 2018, 29, 184–188. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Wang, R.; Zhang, L.; Li, H.L.; Zheng, Q.H.; Zhou, X.D.; Huang, D.M. Apically extruded debris and irrigant with two Ni-Ti systems and hand files when removing root fillings: A laboratory study. Int. Endod. J. 2013, 46, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Azim, A.A.; Aksel, H.; Jefferson, M.M.; Huang, G.T. Comparison of sodium hypochlorite extrusion by five irrigation systems using an artificial root socket model and a quantitative chemical method. Clin. Oral Investig. 2018, 22, 1055–1061. [Google Scholar] [CrossRef]
- Jamleh, A.; Fukumoto, Y.; Takatomo, Y.; Kobayashi, C.; Suda, H.; Adorno, C.G. A comparison between two negative pressure irrigation techniques in simulated immature tooth: An ex vivo study. Clin. Oral Investig. 2016, 20, 125–131. [Google Scholar] [CrossRef]
- Gupta, J.; Nikhil, V.; Jha, P. Corelation between machines assisted endodontic irrigant agitation and apical extrusion of debris and irrigant: A laboratory study. Sci. World J. 2014, 2014, 346184. [Google Scholar] [CrossRef] [Green Version]
- Rödig, T.; Bozkurt, M.; Konietschke, F.; Hülsmann, M. Comparison of the Vibringe System with Syringe and Passive Ultrasonic Irrigation in Removing Debris from Simulated Root Canal Irregularities. J. Endod.J. Endod. 2010, 36, 1410–1413. [Google Scholar] [CrossRef]
- Desai, P.; Himel, V. Comparative safety of various intracanal irrigation systems. J. Endod. 2009, 35, 545–549. [Google Scholar] [CrossRef]
- Navjot, S.M.; Manpreet, K.; Ashu, J.; Manu, R.; Divya, B.; Aaron, S. Efficacy of Various Irrigants Used with Self-Adjusting File System on Smear Layer: An In Vitro Study. J. Pharm. Res. Int. 2021, 33, 52–61. [Google Scholar] [CrossRef]
- Karade, P.; Sharma, D.; Hoshing, U.A.; Medha, A.H.; Bhagat, A.R.; Chopade, R.V. Efficiency of Different Endodontic Irrigation and Activation Systems, Self-Adjusting File Instrumentation/Irrigation System, and XP-Endo Finisher in Removal of the Intracanal Smear Layer: An Ex vivo Scanning Electron Microscope Study. Pharm. Bioallied Sci. 2021, 13, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Neves, M.A.S.; Rocas, I.N.; Siqueira, J.F., Jr. Clinical antibacterial effectiveness of the self-adjusting file system. Int. Endod. J. 2014, 47, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Keleş, A.; Alçin, H.; Sousa-Neto, M.D.; Versiani, M.A. Supplementary Steps for Removing Hard Tissue Debris from Isthmus-containing Canal Systems. J. Endod. 2016, 42, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Teves, A.; Blanco, D.; Casaretto, M.; Torres, J.; Alvarado, D.E.; Coaguila-Llerena, H.; Faria, G.; Jaramillo, D.E. Multispecies biofilm removal by XP-endo Finisher and passive ultrasonic irrigation: A scanning electron microscopy study. Aust. Endod. J. 2022, 48, 91–97. [Google Scholar] [CrossRef]
- Ballal, N.V.; Gandhi, P.; Shenoy, P.A.; Dummer, P.M.H. Evaluation of various irrigation activation systems to eliminate bacteria from the root canal system: A randomized controlled single blinded trial. J. Dent. 2020, 99, 103412. [Google Scholar] [CrossRef]
- Ulusoy, Ö.İ.; Savur, İ.G.; Alaçam, T.; Çelik, B. The effectiveness of various irrigation protocols on organic tissue removal from simulated internal resorption defects. Int. Endod. J. 2018, 51, 1030–1036. [Google Scholar] [CrossRef]
- Keskin, C.; Sariyilmaz, E.; Sariyilmaz, Ö. Efficacy of XP-endo Finisher File in Removing Calcium Hydroxide from Simulated Internal Resorption Cavity. J. Endod. 2017, 43, 126–130. [Google Scholar] [CrossRef]
- Arslan, H.; Capar, I.D.; Saygili, G.; Gok, T.; Akcay, M. Effect of photon-initiated photoacoustic streaming on removal of apically placed dentinal debris. Int. Endod. J. 2014, 47, 1072–1077. [Google Scholar] [CrossRef]
- De Moor, R.J.; Meire, M.; Goharkhay, K.; Moritz, A.; Vanobbergen, J. Efficacy of ultrasonic versus laser-activated irrigation to remove artificially placed dentin debris plugs. J. Endod. 2010, 36, 1580–1583. [Google Scholar] [CrossRef]
- Su, Z.; Li, Z.; Shen, Y.; Bai, Y.; Zheng, Y.; Pan, C.; Hou, B. Characteristics of the Irrigant Flow in a Simulated Lateral Canal Under Two Typical Laser-Activated Irrigation Regimens. Lasers Surg. Med. 2021, 53, 587–594. [Google Scholar] [CrossRef]
- Arıcıoğlu, B.; Çıkman, A.Ş.; Babacan, M. The comparison of cleaning efficacy and apical extrusion of advanced irrigation activation methods with a novel Er:YAG laser modality: Sweeps. Lasers Dent. Sci. 2021, 5, 43–52. [Google Scholar] [CrossRef]
- Fariniuk, L.F.; Baratto, F.; da Cruz, A.M.; de Sousa-Neto, M.D. Histologic analysis of the cleaning capacity of mechanical endodontic instruments activated by the ENDOflash system. J. Endod. 2003, 29, 651–653. [Google Scholar] [CrossRef]
- Rodig, T.; Hulsmann, M.; Muhge, M.; Schafers, F. Quality of preparation of oval distal root canals in mandibular molars using nickel-titanium instruments. Int. Endod. J. 2002, 35, 919–928. [Google Scholar] [CrossRef]
- Swimberghe, R.C.D.; Buyse, R.; Meire, M.A.; De Moor, R.J.G. Efficacy of different irrigation technique in simulated curved root canals. Lasers Med. Sci. 2021, 36, 1317–1322. [Google Scholar] [CrossRef] [PubMed]
- Vianna, M.E.; Gomes, B.; Berber, V.B.; Zaia, A.A.; Ferraz, C.C.R.; de Souza, F.J. In vitro evaluation of the antimicrobial activity of chlorhexidine and sodium hypochlorite. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 97, 79–84. [Google Scholar] [CrossRef]
- Portenier, I.; Waltimo, T.; Orstavik, D.; Haapasalo, M. The susceptibility of starved, stationary phase, and growing cells of Enterococcus faecalis to endodontic medicaments. J. Endod. 2005, 31, 380–386. [Google Scholar] [CrossRef]
- Metzger, Z. The self-adjusting file (SAF) system: An evidence-based update. J. Conserv. Dent. 2014, 17, 401–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haapasalo, M.; Shen, Y.; Qian, W.; Gao, Y. Irrigation in endodontics. Dent. Clin. North Am. 2010, 54, 291–312. [Google Scholar] [CrossRef]
- Gazzaneo, I.; Vieira, G.C.S.; Pérez, A.R.; Alves, F.R.F.; Gonçalves, L.S.; Mdala, I.; Siqueira, J.F., Jr.; Rôças, I.N. Root Canal Disinfection by Single- and Multiple-instrument Systems: Effects of Sodium Hypochlorite Volume, Concentration, and Retention Time. J. Endod. 2019, 45, 736–741. [Google Scholar] [CrossRef]
- Alves, F.R.F.; Almeida, B.M.; Neves, M.A.S.; Rôças, I.N.; Siqueira, J.F. Time-dependent Antibacterial Effects of the Self-Adjusting File Used with Two Sodium Hypochlorite Concentrations. J. Endod. 2011, 37, 1451–1455. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Kim, Y.K.; Cadenaro, M.; Bryan, T.E.; Sidow, S.J.; Loushine, R.J.; Ling, J.-q.; Pashley, D.H.; Tay, F.R. Effects of Different Exposure Times and Concentrations of Sodium Hypochlorite/Ethylenediaminetetraacetic Acid on the Structural Integrity of Mineralized Dentin. J. Endod. 2010, 36, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Mai, S.; Kim, Y.K.; Arola, D.D.; Gu, L.S.; Kim, J.R.; Pashley, D.H.; Tay, F.R. Differential aggressiveness of ethylenediamine tetraacetic acid in causing canal wall erosion in the presence of sodium hypochlorite. J. Dent. 2010, 38, 201–206. [Google Scholar] [CrossRef]
- Elnaggar, S.E.; El Backly, R.M.; Zaazou, A.M.; Elshabrawy, S.M.; Abdallah, A.A. Effect of different irrigation protocols for applications in regenerative endodontics on mechanical properties of root dentin. Aust. Endod. J. 2021, 47, 228–235. [Google Scholar] [CrossRef]
- Giardino, L.; Bidossi, A.; Del Fabbro, M.; Savadori, P.; Maddalone, M.; Ferrari, L.; Ballal, N.V.; Das, S.; Rao, B.S.S. Antimicrobial activity, toxicity and accumulated hard-tissue debris (AHTD) removal efficacy of several chelating agents. Int. Endod. J. 2020, 53, 1093–1110. [Google Scholar] [CrossRef] [PubMed]
- Sen, B.H.; Ertürk, O.; Pişkin, B. The effect of different concentrations of EDTA on instrumented root canal walls. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 622–627. [Google Scholar] [CrossRef]
- Grawehr, M.; Sener, B.; Waltimo, T.; Zehnder, M. Interactions of ethylenediamine tetraacetic acid with sodium hypochlorite in aqueous solutions. Int. Endod. J. 2003, 36, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Tay, F.R.; Kim, Y.K.; Mitchell, J.K.; Kim, J.R.; Carrilho, M.; Pashley, D.H.; Ling, J.Q. The effect of initial irrigation with two different sodium hypochlorite concentrations on the erosion of instrumented radicular dentin. Dent. Mater. 2010, 26, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Han, Y.; Liu, Z.; Xu, Z.; Liu, H.; Wei, X. Comparison of the efficacy of laser-activated and ultrasonic-activated techniques for the removal of tricalcium silicate-based sealers and gutta-percha in root canal retreatment: A microtomography and scanning electron microscopy study. BMC Oral Health 2021, 21, 275. [Google Scholar] [CrossRef]
- Tavella, E.S.N.C.; Gibin, J.T.; Rivera, I.; Rached Junior, F.J.A.; Leoni, G.B.; Raucci-Neto, W. Calcium hydroxide paste removal strategies and bond strengths of epoxy- and silicate-based sealers. Aust. Endod. J. 2021, 47, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, I.; Babo, P.S.; Braga, A.C.; Lopes, M.A.; Gomes, M.E.; Pina-Vaz, I. Supplementary solvent irrigation efficacy on filling remnants removal comparing XP-endo Finisher R vs IrriSafe. Sci. Rep. 2021, 11, 12659. [Google Scholar] [CrossRef] [PubMed]
- Bago, I.; Plotino, G.; Katić, M.; Ferenac, A.; Petričević, G.K.; Gabrić, D.; Anić, I. Effect of a novel laser-initiated photoacoustic activation of a solvent or sodium hypochlorite in the removal of filling remnants after retreatment of curved root canals. Photodiagnosis Photodyn. 2021, 36, 102535. [Google Scholar] [CrossRef] [PubMed]
- Volponi, A.; Pelegrine, R.A.; Kato, A.S.; Stringheta, C.P.; Lopes, R.T.; Silva, A.S.S.; Bueno, C. Micro-computed Tomographic Assessment of Supplementary Cleaning Techniques for Removing Bioceramic Sealer and Gutta-percha in Oval Canals. J. Endod. 2020, 46, 1901–1906. [Google Scholar] [CrossRef] [PubMed]
- Bago, I.; Plotino, G.; Katić, M.; Ročan, M.; Batinić, M.; Anić, I. Evaluation of filling material remnants after basic preparation, apical enlargement and final irrigation in retreatment of severely curved root canals in extracted teeth. Int. Endod. J. 2020, 53, 962–973. [Google Scholar] [CrossRef] [PubMed]
- Kaloustian, M.K.; Nehme, W.; El Hachem, C.; Zogheib, C.; Ghosn, N.; Mallet, J.P.; Diemer, F.; Naaman, A. Evaluation of two shaping systems and two sonic irrigation devices in removing root canal filling material from distal roots of mandibular molars assessed by micro CT. Int. Endod. J. 2019, 52, 1635–1644. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Subjects | Total Sample | Root Canal Irrigation | Outcome of Interest | ||
|---|---|---|---|---|---|---|
| Groups | Irrigation Protocols | Irrigation Solutions | ||||
| Freire 2015 | Mesial canals of mandibular molars, with a curvature of 25–35° | 24 | PUI (n = 12) | At power 5 (Suprasson P5, France), A #20 Irrisafe ultrasonic tip, with an in-and-out motion, 2 mm away from the WL | 2 mL 1% NaOCl (30 s) + 2 mL 17%EDTA (30 s) + 2 mL 1% NaOCl (30 s) | Reduction in debris (%) 55.55 ± 21.91 |
| EV (n = 12) | Each cycle repeating the movement of microcannula: 1 mm from the WL for 6 s, followed by withdrawal to 2 mm from the WL for 6 s | 2 mL 1% NaOCl (30 s) + 2 mL 17%EDTA (30 s) + 2 mL 1% NaOCl (30 s) | Reduction in debris (%) 53.65 ± 18.16 | |||
| Leoni 2017 | Mesial canals of mandibular first molars, with a curvature of 15–20° Two mesial canals connected by a single and continuous isthmus that joined together in the apical third to exit in a single foramen | 40 | PUI (n = 10) | 35 Hz (10% power of Piezon 150), A #20 Irrisonic ultrasonic tip, with an in-and-out motion, 2 mm away from the WL | 0.5 mL 2.5% NaOCl (20 s) + 1.67 mL 2.5% NaOCl (20 s) + 1.67 mL 2.5% NaOCl (20 s) + 1.67 mL 2.5% NaOCl (20 s) | Reduction in debris (%) 94.1 ± 6.8 |
| XPF (n = 10) | Instrument inserts without rotation, then turns on rotation. With an in-and-out motion, (800 rpm, 1 N·cm) Up to the WL. | 0.5 mL 2.5% NaOCl (60 s) + 5 mL 2.5% NaOCl (SNI, 60 s) | Reduction in debris (%) 89.7 ± 10.4 | |||
| SNI (n = 10) | 30-gauge NaviTip needle, 2 mm away from the WL | 0.5 mL 2.5% NaOCl (left still for 60 s) + 5 mL 2.5% NaOCl (60 s) | Reduction in debris (%) 45.7 ± 15 | |||
| SAF (n = 10) | A 1.5-mm diameter SAF file (ReDent-Nova). With an in-and-out motion, Up to the WL | 0.5 mL 2.5% NaOCl (left still for 60 s) + 5 mL 2.5% NaOCl (60 s) | Reduction in debris (%) 41.3 ± 9.4 | |||
| Verstraeten 2017 | Mesial canals of mandibular molars. Two mesial canals connected by an isthmus | 30 | PUI (n = 10) | At power 4 (Suprasson Pmax), A #20 Irrisafe ultrasonic tip, 2–4 mm away from the WL | 1 mL 2.5% NaOCl (20 s) + 1 mL 2.5% NaOCl (20 s) + 1 mL 2.5% NaOCl (20 s) | Vol% debris after preparation (%) 8.44 ± 2.15 Vol% debris after irrigation (%) 3.13 ± 0.98 |
| LAI (n = 10) | A 2940 nm Er:YAG laser (AT Fidelis) (Energy:20 mJ; frequency:20 Hz; length:50 μs) A 300 μm diameter tip (PRECISO 300/14). With an in-and-out motion. 5 mm away from the WL. | 1 mL 2.5% NaOCl (20 s) + 1 mL 2.5% NaOCl (20 s) + 1 mL 2.5% NaOCl (20 s) | Vol% debris after preparation (%) 8.21 ± 1.77 Vol% debris after irrigation (%) 2.43 ± 0.91 | |||
| PIPS (n = 10) | A 2940 nm Er:YAG laser (AT Fidelis) (Energy:20 mJ; frequency:20 Hz; length:50 μs). A 300-μm tip (PRECISO 300/14). Held still at the canal entrance. 5 mm away from the WL. | 1 mL 2.5% NaOCl (20 s) + 1 mL 2.5% NaOCl (20 s) + 1 mL 2.5% NaOCl (20 s) | Vol% debris after preparation (%) 8.18 ± 2.11 Vol% debris after irrigation (%) 2.28 ± 1.05 | |||
| De-Deus 2019 | Mandibular incisors with a single oval-shaped canal | 20 | XPF (n = 10) | Instrument inserts without rotation, then turns on rotation. With an in-and-out motion. (800 rpm, 1 N·cm) Up to the WL. | 0.5 mL 5.25% NaOCl (60 s) + 4.5 mL 5.25% NaOCl (60 s, SNI at 1 mm from the WL) | Reduction in debris (%) 62.67 ± 22.78 |
| PUI (n = 10) | 35 Hz (10% power of Piezon 150), A #20 Irrisonic ultrasonic tip, With an in-and-out motion, 2 mm away from the WL | 0.5 mL 5.25% NaOCl (20 s) + 1.5 mL 5.25% NaOCl (20 s) + 1.5 mL 5.25% NaOCl (20 s) + 1.5 mL 5.25% NaOCl (20 s) | Reduction in debris (%) 62.66 ± 22.13 | |||
| Rödig 2019 | Mesial canals of mandibular molars, with a curvature of 15–20° and a radius between 5.5 and 16.5 mm. Two mesial canals connected by an isthmus | 40 | EA (n = 10) | 166 Hz, A # 15 EndoActivator tip, 2 mm away from the WL | 1 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 15% EDTA (20 s) | Reduction in debris (%) 54.1 ± 21.5 |
| ED (n = 10) | 6000 Hz, An EDDY tip (VDW), 2 mm away from the WL | 1 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 15% EDTA (20 s) | Reduction in debris (%) 56.9 ± 24.2 | |||
| PUI (n = 10) | 30% power of VDW Ultra, A #25 IRRI S ultrasonic tip, 2 mm away from the WL | 1 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 15% EDTA (20 s) | Reduction in debris (%) 66.80 ± 29.10 | |||
| SNI (n = 10) | A 30-gauge Endo-EZE needle (Ultradent), 2 mm away from the WL | 1 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 1% NaOCl (20 s) + 2 mL 15% EDTA (20 s) | Reduction in debris (%) 44.10 ± 17.40 | |||
| Silva 2019 | Mesial canals of mandibular molars, with a curvature of 10–20° and isthmuses type I or III | 40 | PUI (n = 10) | 10% power of Piezo, A #20/0.01 Irrisonic ultrasonic tip, 1 mm away from the WL | 4 mL 5.25% NaOCl (30 s) + 4 mL 5.25% NaOCl (30 s) + 4 mL 5.25% NaOCl (30 s) + 4 mL 17%EDTA (30 s) + 4 mL 5.25% NaOCl (30 s) | Vol% debris after preparation (%) 0.63 ± 1.56 Vol% debris after irrigation (%) 0.14 ± 0.38 |
| EV (n = 10) | First: EndoVac microcannula was inserted into the root canal until finding resistance and moved up and down. Then: EndoVac microcannula was inserted 1 mm short of the WL. | 6 mL 5.25% NaOCl (activation for 30 s with microcannula, then left still for 1 min) + 5 mL 5.25% NaOCl (activation for 60 s with microcannula, then left still for 1 min) + 4 mL 17%EDTA (ditto) + 5 mL 5.25% NaOCl (ditto) | Vol% debris after preparation (%) 0.46 ± 0.73 Vol% debris after irrigation (%) 0.14 ± 0.27 | |||
| SAF (n = 10) | A 2 mm-diameter SAF file (ReDent-Nova). With an in-and-out motion. 1 mm away from the WL. | 12 mL 5.25% NaOCl (3 min) + 4 mL 17%EDTA (1 min) + 4 mL 5.25% NaOCl (1 min) | Vol% debris after preparation (%) 0.32 ± 0.55 Vol% debris after irrigation (%) 0.20 ± 0.40 | |||
| Easy-Clean (n = 10) | 1 mm away from the WL. | Similar with PUI | Vol% debris after preparation (%) 0.30 ± 0.34 Vol% debris after irrigation (%) 0.17 ± 0.28 | |||
| Zhao 2019 | Mandibular molars with a C-shaped canal system | 60 | SNI (n = 20) | A 30-gauge needle. 1 mm away from the WL. | 2 mL 2% NaOCl × 3 (SNI at a rate of 5 mL/min, then left still for 20 s) + 2 mL 17% EDTA (5 mL/min) + 2 mL 2% NaOCl (5 mL/min) | Reduction in debris (%) Group1: 43.4 ± 17.8 Group2: 57.1 ± 20.6 |
| PUI (n = 20) | At power 6 (Suprasson P5, France). A #20 Irrisafe ultrasonic tip With an in-and-out motion. 1 mm away from the WL. | 2 mL 2% NaOCl (20 s) × 3 + 2 mL 17% EDTA (SNI, 5 mL/min) + 2 mL 2% NaOCl (SNI, 5 mL/min) | Reduction in debris (%) Group1: 64.2 ± 19.8 Group2: 77.3 ± 18.9 | |||
| XPF (n = 20) | A #25/.00 XPF file inserts without rotation, then turns on rotation. With an in-and-out motion. (800 rpm, 1 N·cm) Up to the WL. | 1 mL 2% NaOCl (SNI at 1 mm away from the WL, 5 mL/min) + 5 mL 2% NaOCl (XPF for 1 min) + 2 mL 17% EDTA (SNI, 5 mL/min) + 2 mL 2% NaOCl (SNI, 5 mL/min) | Reduction in debris (%) Group1: 68.4 ± 18.0 Group2: 63.1 ± 20.9 | |||
| Linden 2020 | Mesial canals of mandibular molars with a moderate curvature. Two mesial canals connected by an isthmus. | 27 | SNI (n = 9) | A 30-G notched needle. 2 mm away from the WL. | 3 mL 2.5% NaOCl (0.14 mL/s) | Reduction in debris (%) 43.68 ± 30.09 |
| ED (n = 9) | 6000 Hz. A #25/.04 EDDY tip. 2 mm away from the WL. | 1 mL 2.5% NaOCl (20 s) × 3 | Reduction in debris (%) 36.38 ± 20.43 | |||
| PUI (n = 9) | At power 9 (Suprasson P5, France). A #20 Irrisafe ultrasonic tip. Without an in-and-out motion. 2 mm away from the WL. | 1 mL 2.5% NaOCl (20 s) × 3 | Reduction in debris (%) 66.81 ± 22.85 | |||
| Yang 2020 | Mandibular molars, with a single canal in the distal root and two mesial canals connected by an isthmus and have a curvature of 25–35° | 30 | PUI (n = 10) | At power 5 (Suprasson P5, France). A #15/.02 Irrisafe ultrasonic tip. With an in-and-out motion. 2 mm away from the WL. | 0.5 mL 1% NaOCl (SNI) + 5 mL 1% NaOCl (activation for 30 s, then left still for 30 s) × 3 | Reduction in debris (%) Group1: 50.27 ± 7.15 Group2: 51.14 ± 7.54 |
| PIPS (n = 10) | A 2940 nm Er:YAG laser (LightWalker AT) (Energy:20 mJ; frequency:15 Hz; length:50μs). A 600 μm diameter tip (PIPS 600/9). Held still at the canal entrance | 0.5 mL 1% NaOCl (SNI) + 5 mL 1% NaOCl (activation for 30 s, then left still for 30 s) × 3 | Reduction in debris (%) Group1: 58.79 ± 8.53 Group2: 56.57 ± 16.82 | |||
| SWEEPS (n = 10) | A 2940 nm Er:YAG laser (LightWalker AT) (Energy:20 mJ; frequency:15 Hz; length:50 μs). A special fibre tip (SWEEPS 600). | 0.5 mL 1% NaOCl (SNI) + 5 mL 1% NaOCl (activation for 30 s, then left still for 30 s) × 3 | Reduction in debris (%) Group1: 84.31 ± 7.19 Group2: 83.97 ± 7.07 | |||
| Rodrigues 2021 | Mesial canals of mandibular molars, with a curvature of 20–46° (mean 32.5°) and isthmuses type I | 24 | PUI (n = 8) | At medium power of ultrasonic unit (SEM). An ultrasonic ESI Tip (SEM). 2 mm away from the WL. | 5 mL 3% NaOCl (20 s) + 5 mL 17% EDTA (20 s) + 5 mL 3% NaOCl (20 s) + 5 mL saline solution (SNI) | Reduction in debris (%) 78.29 ± 33.07 |
| SNI (n = 8) | A 30-G Navitip needle 1 mm away from the WL. | 5 mL 3% NaOCl (20 s) + 5 mL 17% EDTA (20 s) + 5 mL 3% NaOCl (20 s) + 5 mL saline solution | Reduction in debris (%) 56.98 ± 46.45 | |||
| ED (n = 8) | An EDDY tip. 1 mm away from the WL. | 5 mL 3% NaOCl (20 s) + 5 mL 17% EDTA (20 s) + 5 mL 3% NaOCl (20 s) + 5 mL saline solution (SNI) | Reduction in debris (%) 93 ± 6.14 | |||
| de Mattos 2022 | mesial roots of mandibular molars, with a curvature of 10–20° and isthmuses type II | 40 | PUI (n = 10) | 15% power of Jet Sonic (Brazil). A #20 Irrisafe ultrasonic tip. 1 mm away from the WL. | 2 mL 2.5% NaOCl (1 min) + 2 mL 17% EDTA (1 min) | Reduction in debris (%): 51.76 ± 27.17 |
| XPF (n = 10) | An XPF file inserts without rotation, then turns on rotation. (800 rpm, 1 N·cm) 1 mm away from the WL. | 0.5 mL 5.25% NaOCl (1 min) +4.5 mL 5.25% NaOCl (SNI) | Reduction in debris (%): 79.86 ± 19.38 | |||
| EA (n = 10) | A #25/04 EndoActivator tip, 1 mm away from the WL, activated at 10,000 cycles per minute. | 2 mL 2.5% NaOCl (1 min) + 2 mL 17% EDTA (1 min) 5 mL 2.5% NaOCl (1 min) × 2 + 5 mL 17% EDTA (1 min) + 5 mL 2.5% NaOCl (1 min) 5 mL 2.5% NaOCl (microcannula) + 5 mL 2.5% NaOCl (microcannula) × 3 | Reduction in debris (%): 62.08 ± 22.36 | |||
| EasyClean (n = 10) | 1 mm away from the WL | Reduction in debris (%): 31.30 ± 19.21 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, A.; Huang, L.; Li, B.; Huang, Y.; Zhou, X.; Zhang, X.; Gong, Q. Micro-CT Evaluation of Different Root Canal Irrigation Protocols on the Removal of Accumulated Hard Tissue Debris: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6053. https://doi.org/10.3390/jcm11206053
Liang A, Huang L, Li B, Huang Y, Zhou X, Zhang X, Gong Q. Micro-CT Evaluation of Different Root Canal Irrigation Protocols on the Removal of Accumulated Hard Tissue Debris: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(20):6053. https://doi.org/10.3390/jcm11206053
Chicago/Turabian StyleLiang, Ailin, Luo Huang, Baoyu Li, Yihua Huang, Xiaoyan Zhou, Xufang Zhang, and Qimei Gong. 2022. "Micro-CT Evaluation of Different Root Canal Irrigation Protocols on the Removal of Accumulated Hard Tissue Debris: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 20: 6053. https://doi.org/10.3390/jcm11206053
APA StyleLiang, A., Huang, L., Li, B., Huang, Y., Zhou, X., Zhang, X., & Gong, Q. (2022). Micro-CT Evaluation of Different Root Canal Irrigation Protocols on the Removal of Accumulated Hard Tissue Debris: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(20), 6053. https://doi.org/10.3390/jcm11206053